
Surgical Protocols before and after COVID-19—A Narrative Review


 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Focused Question
2.2. Literature Search
2.3. Exclusion Criteria
- -
- Case reports and case series were excluded.
- -
- Articles which did not describe in detail about surgical interventions were excluded.
2.4. Selection of Studies
2.5. Data Extraction
2.6. Methodological Quality Appraisal
3. Results and Discussion
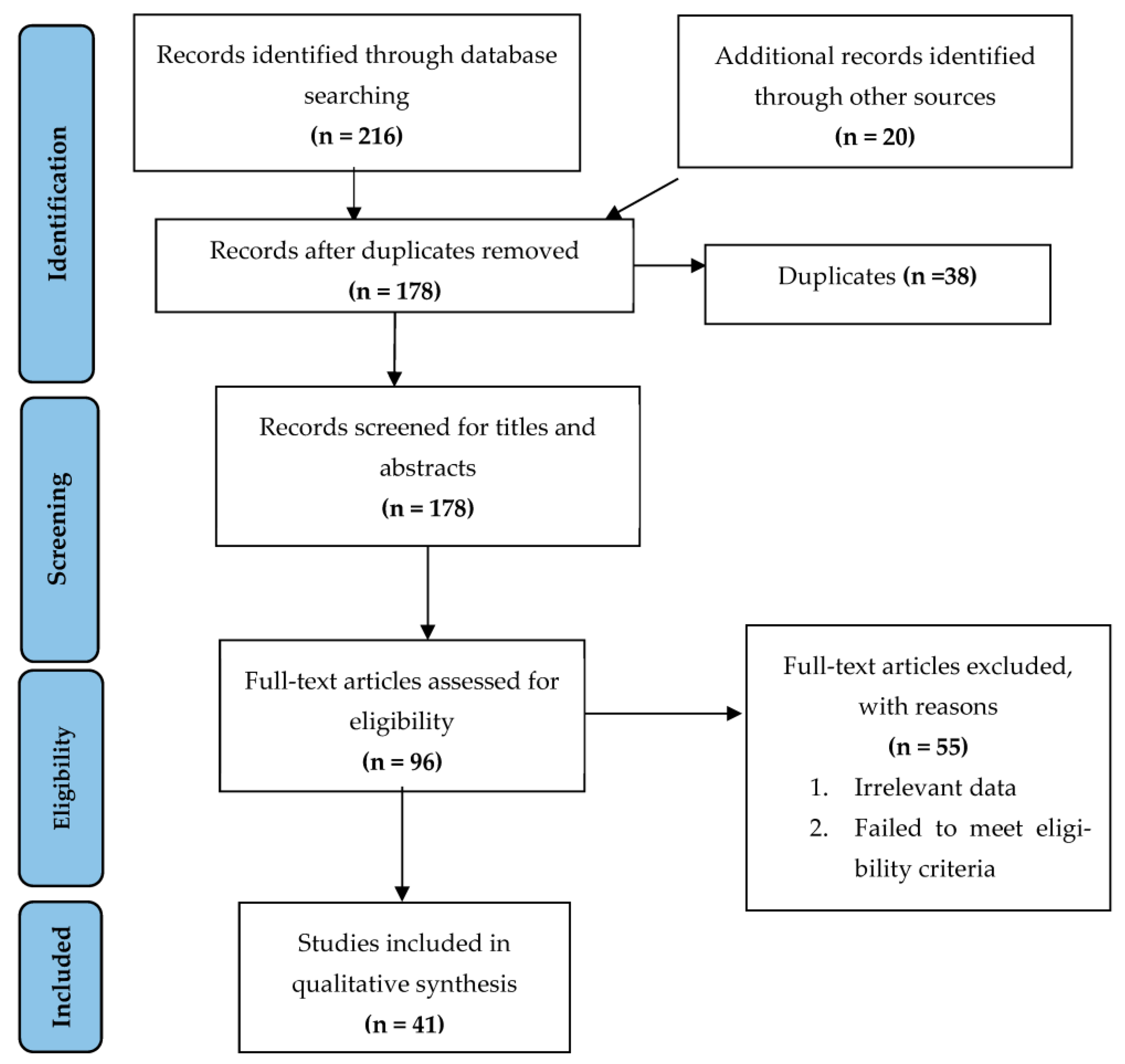
3.1. Literature Search
3.2. Changes in Ocular/Ophthalmic Surgeries
3.3. Changes in Urological Surgeries
3.4. Changes in Neurological Surgeries
3.5. Changes in Oncological Surgeries
3.6. Changes in Obstetrics/Gynaecological Surgeries
3.7. Changes in Orthopaedic Surgeries
3.8. Changes in Plastic Surgery Practices
3.9. Changes in Pre- and Post-Operative Complications
3.10. Changes in General Surgical Practices
3.11. Changes in Elective Surgeries
4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. 2020. Available online: https://www.who.int/dg/speeches/detail/whodirector-general-s-opening-remarks-at-the-media-briefing-on-covid-19—11-march-2020 (accessed on 29 March 2020).
- Nicola, M.; O’Neill, N.; Sohrabi, C.; Khan, M.; Agha, M.; Agha, R. Evidence based management guideline for the COVID-19 pandemic—Review article. Int. J. Surg. 2020, 77, 206–216. [Google Scholar] [CrossRef] [PubMed]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Kurihara, H.; Bisagni, P.; Faccincani, R.; Zago, M. COVID-19 outbreak in Northern Italy: Viewpoint of the Milan area surgical community. J. Trauma: Inj. Infect. Crit. Care 2020, 88, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Qu, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Monaghesh, E.; Hajizadeh, A. The role of telehealth during COVID-19 outbreak: A systematic review based on current evidence. BMC Public Health 2020, 20, 1193. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control (ECDC). Infection Prevention and Control and Preparedness for COVID-19 in Healthcare Settings. 2020. Available online: https://www.ecdc.europa.eu/en/publications-data/infection-prevention-and-control-andpreparedness-covid-19-healthcare-settings (accessed on 1 January 2022).
- Brindle, M.E.; Gawande, A. Managing COVID-19 in Surgical Systems. Ann. Surg. 2020, 272, e1–e2. [Google Scholar] [CrossRef]
- COVIDSurg Collaborative. Global guidance for surgical care during the COVID-19 pandemic: Surgical care during the COVID-19 pandemic. Br. J. Surg. 2020, 107, 1097–1103. [Google Scholar] [CrossRef]
- Monitor, International Comparisons of Selected Service Lines in Seven Health Systems. Annex 3—Review of Service Lines: Critical Care. 2014. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/382845/Annex_3_Critical_Care1.pdf (accessed on 1 January 2022).
- Cetinkaya, Y.F. Ophthalmic surgeries before and during the covid-19 outbreak in a tertiary hospital. Int. Ophthalmol. 2022, 1–6. [Google Scholar] [CrossRef]
- Shabto, J.M.; Faaborg-Andersen, C.; O’Keefe, G.A. The impact of COVID-19: Variations in volumes and characteristics of retina surgeries. BMC Surg. 2022, 22, 41. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Ophthalmology. New Recommendations for Urgent and Nonurgent Patient Care. Available online: https://www.aao.org/headline/new-recom%20mendations-urgent-nonurgent-patient-care (accessed on 20 November 2022).
- American Society of Retina Specialists. ASRS Releases Guidelines to Help Retina Practices Navigate COVID-19 Pandemic. Available online: https://www.asrs.org/clinical/clinical-updates/1962/asrs-releases-guidelines-to-help-retina-practices-navigate-covid-19-pandemic (accessed on 20 November 2022).
- Soytas, M.; Boz, M.Y.; Guzelburc, V.; Calik, G.; Horuz, R.; Akbulut, Z.; Albayrak, S. Comparison of before and after COVID-19 urology practices of a pandemic hospital. Turk. J. Urol. 2020, 46, 474–480. [Google Scholar] [CrossRef] [PubMed]
- Nabil, M.; Dorrah, M.; Sharfeldin, A.; Abaza, H. Impact of COVID-19 pandemic on the neurosurgical practice in Egypt. Egypt. J. Neurosurg. 2022, 37, 23. [Google Scholar] [CrossRef]
- Grani, G.; Ciotti, L.; Del Gatto, V.; Montesano, T.; Biffoni, M.; Giacomelli, L.; Sponziello, M.; Pecce, V.; Lucia, P.; Verrienti, A.; et al. The COVID-19 outbreak and de-escalation of thyroid cancer diagnosis and treatment. Endocrine 2022, 78, 387–391. [Google Scholar] [CrossRef]
- Puig-Domingo, M.; Marazuela, M.; Giustina, A. COVID-19 and endocrine diseases. A statement from the European Society of Endocrinology. Endocrine 2020, 68, 2–5. [Google Scholar] [CrossRef] [PubMed]
- Medas, F.; Ansaldo, G.L.; Avenia, N.; Basili, G.; Boniardi, M.; Bononi, M.; Bove, A.; Carcoforo, P.; Casaril, A.; Cavallaro, G.; et al. The THYCOVIT (Thyroid Surgery during COVID-19 pandemic in Italy) study: Results from a nationwide, multicentric, case-controlled study. Updat. Surg. 2021, 73, 1467–1475. [Google Scholar] [CrossRef] [PubMed]
- Vigliar, E.; Pisapia, P.; Iacovo, F.D.; Alcaraz-Mateos, E.; Alì, G.; Ali, S.Z.; Baloch, Z.W.; Bellevicine, C.; Bongiovanni, M.; Botsun, P.; et al. COVID-19 pandemic impact on cytopathology practice in the post-lockdown period: An international, multicenter study. Cancer Cytopathol. 2022, 130, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Spurlin, E.E.; Han, E.S.; Silver, E.R.; May, B.L.; Tatonetti, N.P.; Ingram, M.A.; Jin, Z.; Hur, C.; Advincula, A.P.; Hur, H.-C. Where Have All the Emergencies Gone? The Impact of the COVID-19 Pandemic on Obstetric and Gynecologic Procedures and Consults at a New York City Hospital. J. Minim. Invasive Gynecol. 2020, 28, 1411–1419.e1. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. Joint Statement on Elective Surgeries. Available online: https://www.acog.org/news/newsreleases/2020/03/joint-statement-on-elective-surgeries (accessed on 1 January 2022).
- Cengiz, B. The impact of COVID-19-related social restriction and containment measures on admissions for orthopedic surgery in a private hospital: Cross-sectional data from a secondary healthcare provider in Turkey. Med. Sci. | Int. Med. J. 2022, 11, 180. [Google Scholar] [CrossRef]
- Hernigou, J.; Morel, X.; Callewier, A.; Bath, O.; Hernigou, P. Staying home during “COVID-19” decreased fractures, but trauma did not quarantine in one hundred and twelve adults and twenty-eight children and the “tsunami of recommendations” could not lockdown twelve elective operations. Int. Orthop. 2020, 44, 1473–1480. [Google Scholar] [CrossRef]
- Kalem, M.; Kocaoglu, H.; Merter, A.; Karaca, M.O.; Özbek, E.A.; Kinik, H.H. Effects of COVID-19 pandemic curfew on orthopedic trauma in a tertiary care hospital in Turkey. Acta Orthop. Traumatol. Turc. 2021, 55, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Mortada, H.; Alawaji, Z.H.; Aldihan, R.A.; Alkuwaiz, L.A.; Alshaalan, S.F.; Kattan, A.E. Impact of the Coronavirus Disease 2019 Pandemic on the Patterns and Characteristics of Plastic Surgery Practice: A Retrospective Comparative Study of Before and During the Pandemic. Cureus 2022, 14, e29722. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Hormozi, A.; Habibzadeh, Z.; Yavari, M.; Mousavizadeh, S.M.; Hassanpour, S.E.; Motamed, S.; Rouientan, A.; Mozafari, N.; Shahrokh, S.; Mohammadsadeghi, S.; et al. Impact of COVID-19 pandemic on plastic surgery activities and residency programs in a tertiary referral centre in Iran. Eur. J. Plast. Surg. 2021, 44, 817–823. [Google Scholar] [CrossRef] [PubMed]
- Andrews, B.T.; Garg, R.; Przylecki, W.; Habal, M. COVID-19 Pandemic and its Impact on Craniofacial Surgery. J. Craniofacial Surg. 2020, 31, e620–e622. [Google Scholar] [CrossRef] [PubMed]
- Paiva, M.M.; Rao, V.M.; Spake, C.S.M.; King, V.A.; Crozier, J.W.M.; Liu, P.Y.; Woo, A.S.; Schmidt, S.T.M.; Kalliainen, L.K.M. The Impact of the COVID-19 Pandemic on Plastic Surgery Consultations in the Emergency Department. Plast. Reconstr. Surg.—Glob. Open 2020, 8, e3371. [Google Scholar] [CrossRef] [PubMed]
- Farsi, Y.; Shojaeian, F.; Ahmad Safavi-Naini, S.A.; Honarvar, M.; Mohammadzadeh, B.; Nasiri, M.J. The comparison of Post-Operative Complications pre Covid era versus during Covid-Era based on Clavien-Dindo-classification: A Systematic Review and Meta-Analysis. medRxiv 2022. [Google Scholar] [CrossRef]
- Collaborative COVID. COVID Surg Collaborative. Mortality and pulmonary complications in patients undergoing surgery with perioperative SARS-CoV-2 infection: An international cohort study. Lancet 2020, 396, 27–38. [Google Scholar] [CrossRef]
- Abbott, T.E.; Fowler, A.J.; Dobbs, T.D.; Gibson, J.; Shahid, T.; Dias, P.; Akbari, A.; Whitaker, I.S.; Pearse, R.M. Mortality after surgery with SARS-CoV-2 infection in England: A population-wide epidemiological study. Br. J. Anaesth. 2021, 127, 205–214. [Google Scholar] [CrossRef]
- Knisely, A.; Ni Zhou, Z.; Wu, J.; Huang, Y.; Holcomb, K.; Melamed, A.; Advincula, A.P.; Lalwani, A.; Khoury-Collado, F.; Tergas, A.I.; et al. Perioperative Morbidity and Mortality of Patients With COVID-19 Who Undergo Urgent and Emergent Surgical Procedures. Ann. Surg. 2020, 273, 34–40. [Google Scholar] [CrossRef]
- Kaufman, E.J.M.; Ong, A.W.; Cipolle, M.D.M.; Whitehorn, G.B.; Ratnasekera, A.D.; Stawicki, S.P.M.; Martin, N.D. The impact of COVID-19 infection on outcomes after injury in a state trauma system. J. Trauma Inj. Infect. Crit. Care 2021, 91, 559–565. [Google Scholar] [CrossRef]
- Kumaira Fonseca, M.; Trindade, E.N.; Costa Filho, O.P.; Nácul, M.P.; Seabra, A.P. Impact of COVID -19 Outbreak on the Emergency Presentation of Acute Appendicitis. Am. Surg. 2020, 86, 1508–1512. [Google Scholar] [CrossRef]
- Tartaglia, N.; Pavone, G.; Lizzi, V.; Vovola, F.; Tricarico, F.; Pacilli, M.; Ambrosi, A. How emergency surgery has changed during the COVID-19 pandemic: A cohort study. Ann. Med. Surg. 2020, 60, 686–689. [Google Scholar] [CrossRef]
- Sartori, A.; Podda, M.; Botteri, E.; Passera, R.; Agresta, F.; Arezzo, A.; CRAC Study Collaboration Group. Appendectomy during the COVID-19 pandemic in Italy: A multicenter ambispective cohort study by the Italian Society of Endoscopic Surgery and new technologies (the CRAC study). Updates Surg. 2021, 73, 2205–2213. [Google Scholar] [CrossRef] [PubMed]
- Vusirikala, A.; Saleh, M.; Laurent, E.; del Castillo, T.; Kuzhupilly, R.R.; Fahmy, A.; Tsekes, D. Restarting Elective Orthopaedic Surgery During the COVID-19 Pandemic: Lessons Learned. Cureus 2021, 13, e16343. [Google Scholar] [CrossRef] [PubMed]
- Panda, S.; Vig, S.; Singh, C.A.; Konkimalla, A.; Thakar, A.; Sakthivel, P.; Sikka, K.; Kumar, R.; Bhatnagar, S.; Mohan, A.; et al. Head and Neck Surgery During COVID-19 Pandemic: Experience from a Tertiary Care in India. Indian J. Surg. Oncol. 2021, 12, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Al-Jabir, A.; Kerwan, A.; Nicola, M.; Alsafi, Z.; Khan, M.; Sohrabi, C.; O’Neill, N.; Iosifidis, C.; Griffin, M.; Mathew, G.; et al. Impact of the Coronavirus (COVID-19) pandemic on surgical practice—Part 1. Int. J. Surg. 2020, 79, 168–179. [Google Scholar] [CrossRef] [PubMed]
- Al-Jabir, A.; Kerwan, A.; Nicola, M.; Alsafi, Z.; Khan, M.; Sohrabi, C.; O’Neill, N.; Iosifidis, C.; Griffin, M.; Mathew, G.; et al. Impact of the Coronavirus (COVID-19) pandemic on surgical practice—Part 2 (surgical prioritisation). Int. J. Surg. 2020, 79, 233–248. [Google Scholar] [CrossRef]
- Iacobucci, G. COVID-19: All non-urgent elective surgery is suspended for at least three months in England. BMJ 2020, 368, m1106. [Google Scholar] [CrossRef]
- Tao, K.X.; Zhang, B.X.; Zhang, P.; Zhu, P.; Wang, G.B.; Chen, X.P.; General Surgery Branch of Hubei Medical Association, General Surgery Branch of Wuhan Medical Association. Recommendations for general surgery clinical practice in 2019 coronavirus disease situation. Zhonghua Wai Ke Za Zhi 2020, 58, 170–177. [Google Scholar]
- Zheng, M.H.; Boni, L.; Fingerhut, A. Minimally Invasive Surgery and the Novel Coronavirus Outbreak: Lessons Learned in China and Italy. Ann. Surg. 2020, 272, e5–e6. [Google Scholar] [CrossRef]
- Demir, H.B.; Korucuk, E.; Miftari, A.; Turk, Y. Have General Surgery Practices Decreased During the COVID-19 Pandemic? Cureus 2022, 14, e27270. [Google Scholar] [CrossRef] [PubMed]
- Nasta, A.M.; Goel, R.; Kanagavel, M.; Easwaramoorthy, S. Impact of COVID-19 on General Surgical Practice in India. Indian J. Surg. 2020, 82, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.; Awuah, W.A.; Ng, J.C.; Kundu, M.; Yarlagadda, R.; Sen, M.; Nansubuga, E.P.; Abdul-Rahman, T.; Hasan, M.M. Elective surgeries during and after the COVID-19 pandemic: Case burden and physician shortage concerns. Ann. Med. Surg. 2022, 81, 104395. [Google Scholar] [CrossRef]
- Farr, S.; Berry, J.A.; Berry, D.K.; Marotta, D.A.; Buckley, S.E.; Javaid, R.; Jacqueline, D.M.; Magargee, C.E.; Ferrouge, L.M.; Rogalska, A.M.; et al. The Impact of the COVID-19 Pandemic on Resident Physicians Well-Being in the Surgical and Primary Care Specialties in the United States and Canada. Cureus 2021, 13, e19677. [Google Scholar] [CrossRef] [PubMed]
- Salenger, R.; Etchill, E.; Ad, N.; Matthew, T.; Alejo, D.; Whitman, G.; Lawton, J.; Lau, C.L.; Gammie, C.; Gammie, J. The surge after the surge: Cardiac surgery post-COVID-19. Ann. Thorac. Surg. 2020, 110, 2020–2025. [Google Scholar] [CrossRef]
- Cisternas, A.F.; Ramachandran, R.; Yaksh, T.L.; Nahama, A. Unintended consequences of COVID-19 safety measures on patients with chronic knee pain forced to defer joint replacement surgery. PAIN Rep. 2020, 5, e855. [Google Scholar] [CrossRef]
- Larson, D.W.; El Aziz, M.A.A.; Mandrekar, J.N. How Many Lives Will Delay of Colon Cancer Surgery Cost During the COVID-19 Pandemic? An Analysis Based on the US National Cancer Database. Mayo Clin. Proc. 2020, 95, 1805–1807. [Google Scholar] [CrossRef]
- Association of Surgeons of Great Britain & Ireland, Association of coloproctology of Great Britain & Ireland, Association of Upper Gastrointestinal Surgeons, Royal College of Surgeons of Edinburgh, Royal College of Surgeons of England, Royal College of Physicians and Surgeons of Glasgow, Royal College of Surgeons in Ireland. Updated General Surgery Guidance on COVID-19, 2nd Revision. 2020. Available online: https://www.rcsed.ac.uk/news-public-affairs/news/2020/april/updated-general-surgeryguidance-on-covid-19-2nd-revision-7th-april-2020 (accessed on 1 January 2022).
- NHS England, Royal College of Surgeons of England, Royal College of Surgeons in Ireland, Royal college of surgeons of Edinburgh, Royal College of Physicians and Surgeons of Glasgow, Clinical Guide to Surgical Prioritisation during the Coronavirus Pandemic. 2020. Available online: https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/03/C0221-specialty-guide-surgical-prioritisation-v1.pdf (accessed on 1 January 2022).
- American College of Surgeons. COVID-19 Guidelines for Triage of Emergency General Surgery Patients. 2020. Available online: https://www.facs.org/covid-19/clinicalguidance/elective-case/emergency-surgery (accessed on 1 January 2022).

{kind=link}
| Surgical Field | Articles Included |
|---|---|
| Ocular/Ophthalmic | Cetinkaya et al. [13], Shabto J.M. [14], AA of Opthalmology [15], American Society of Retina Specialists [16] |
| Urology | Soytas M. et al. [17] |
| Neurology | Nabil M. et al. [18] |
| Oncology | Grani G. et al. [19], Puig-Domingo M. et al. [20], Medas F. et al. [21], Vigiliar E. [22] |
| OBG | Spurlin E.E. et al. [23], American College of Obstetricians and Gynecolgists [24] |
| Orthopaedic | Cengiz and Bertam [25], Hernigou J. et al. [26], Kalem et al. [27] |
| Plastic surgery | Mortada H. et al. [28], Kalantar et al. [29], Hormozi A. et al. [30], Andrews et al. [31] |
| Surgical complications | Yeganeh Farsi [32], Surgery Colloborative [33], Abbott T.E.F. [34], Knisely A. et al [35], Kaufmen E.J. et al. [36], Kumaira Fonseca [37], Tartaglia N. [38], Sartori A. [39], Yusirikala A. et al. [40], Panda [41] |
| General surgery | Al-Jabir A. [42], Al-Jabir. [43], Jacobucci G. [44], Tao K.X. et al. [45], Zheng MH et al. [46], Demir HB et al. [47], Nasta et al. [48] |
| Elective surgery | Mehta A. et al. [49], Farr S. et al. [50], Salenger R. et al. [51], Cisternas A.F. et al. [52], Larson D.W. et al. [53] |
| Intervals | Studies |
|---|---|
| After [32/41] (75.6%) | AA of Opthalmology [15], American Society of Retina Specialists [16], Grani G. et al. [19], Puig-Domingo M. et al. [20], Medas F. et al. [21], Vigiliar E. [22], Spurlin E.E. et al. [23], American College of Obstetricians and Gynecolgists [24], Cengiz and Bertam [25], Hernigou J. et al. [26], Kalem et al. [27], Hormozi A. et al. [30], Surgery Colloborative [33], Abbott T.E.F. [34], Kaufmen E.J. et al. [36], Kumaira Fonseca [37], Tartaglia N. [38], Sartori A. [39], Yusirikala A. et al. [40], Panda [41], Al-Jabir A. [42], Al-Jabir [43], Jacobucci G. [44], Tao K.X. et al. [45], Zheng M.H. et al. [46], Demir H.B. et al. [47], Nasta et al. [48], Mehta A. et al. [49], Farr S. et al. [50], Salenger R. et al. [51], Cisternas A.F. et al. [52], Larson D.W. et al. [53] |
| Before and after [10/41] (24.4%) | Cetinkaya et al. [13], Shabto J.M. [14], Soytas M. et al. [17], Nabil M. et al. [18], Mortada H. et al. [28], Kalantar et al. [29], Hormozi A. et al. [30], Andrews et al. [31], Yeganeh Farsi [32], Knisely A. et al. [35], |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shivkumar, S.; Mehta, V.; Vaddamanu, S.K.; Shetty, U.A.; Alhamoudi, F.H.; Alwadi, M.A.M.; Aldosari, L.I.N.; Alshadidi, A.A.F.; Minervini, G. Surgical Protocols before and after COVID-19—A Narrative Review. Vaccines 2023, 11, 439. https://doi.org/10.3390/vaccines11020439
Shivkumar S, Mehta V, Vaddamanu SK, Shetty UA, Alhamoudi FH, Alwadi MAM, Aldosari LIN, Alshadidi AAF, Minervini G. Surgical Protocols before and after COVID-19—A Narrative Review. Vaccines. 2023; 11(2):439. https://doi.org/10.3390/vaccines11020439
Chicago/Turabian StyleShivkumar, Sahana, Vini Mehta, Sunil Kumar Vaddamanu, Urvashi A. Shetty, Fahad Hussain Alhamoudi, Maram Ali M. Alwadi, Lujain Ibrahim N. Aldosari, Abdulkhaliq Ali F. Alshadidi, and Giuseppe Minervini. 2023. "Surgical Protocols before and after COVID-19—A Narrative Review" Vaccines 11, no. 2: 439. https://doi.org/10.3390/vaccines11020439
APA StyleShivkumar, S., Mehta, V., Vaddamanu, S. K., Shetty, U. A., Alhamoudi, F. H., Alwadi, M. A. M., Aldosari, L. I. N., Alshadidi, A. A. F., & Minervini, G. (2023). Surgical Protocols before and after COVID-19—A Narrative Review. Vaccines, 11(2), 439. https://doi.org/10.3390/vaccines11020439