

Changing Patterns of SARS-CoV-2 Seroprevalence: A Snapshot among the General Population in Kuwait

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. Study Design and Population
2.3. Data Collection
2.4. Biological Sample Collection, Handling, Transport, and Testing
2.5. Detection of SARS-CoV-2 Antibodies
2.6. Statistical Analysis
3. Results
3.1. Seroprevalence in the General Population during the Pre-Vaccination Period Due to Natural Infection
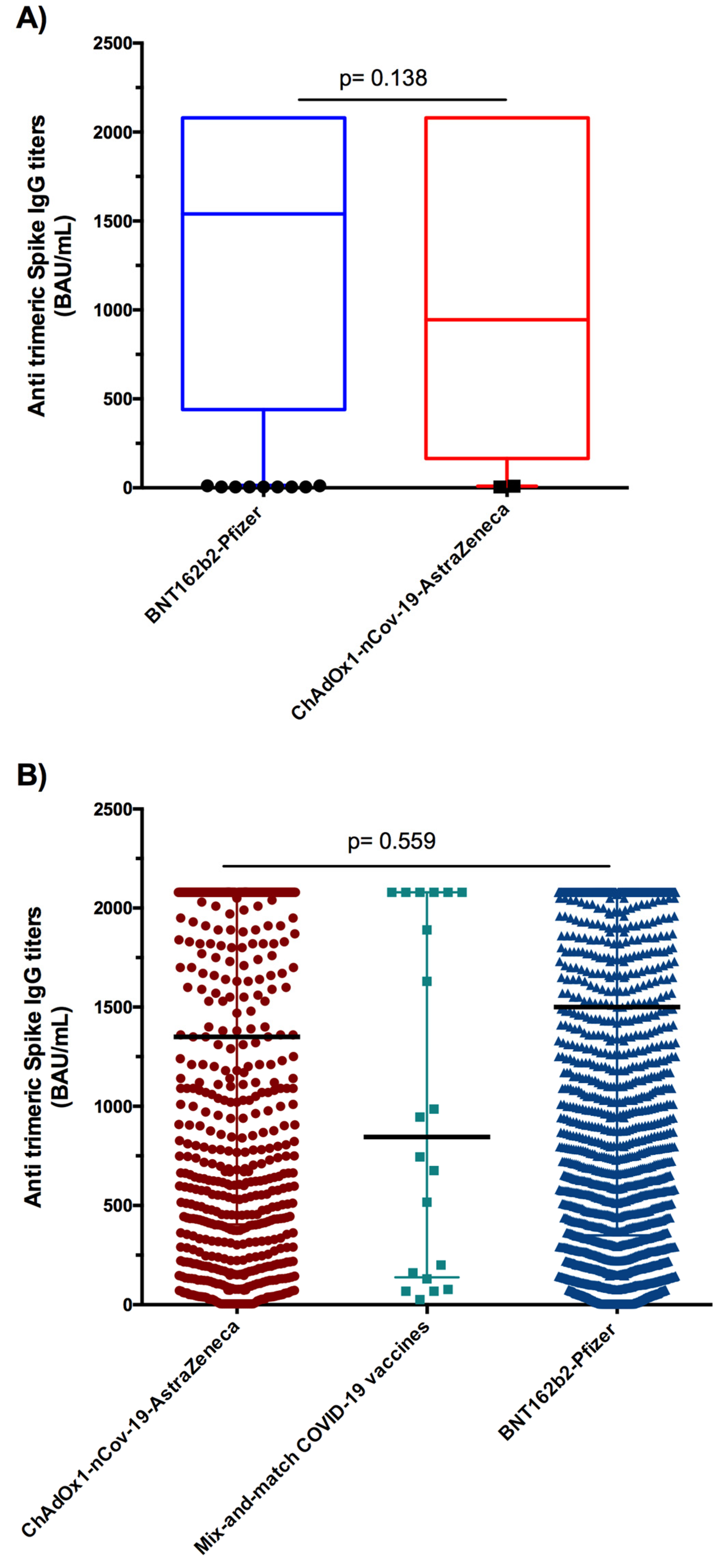
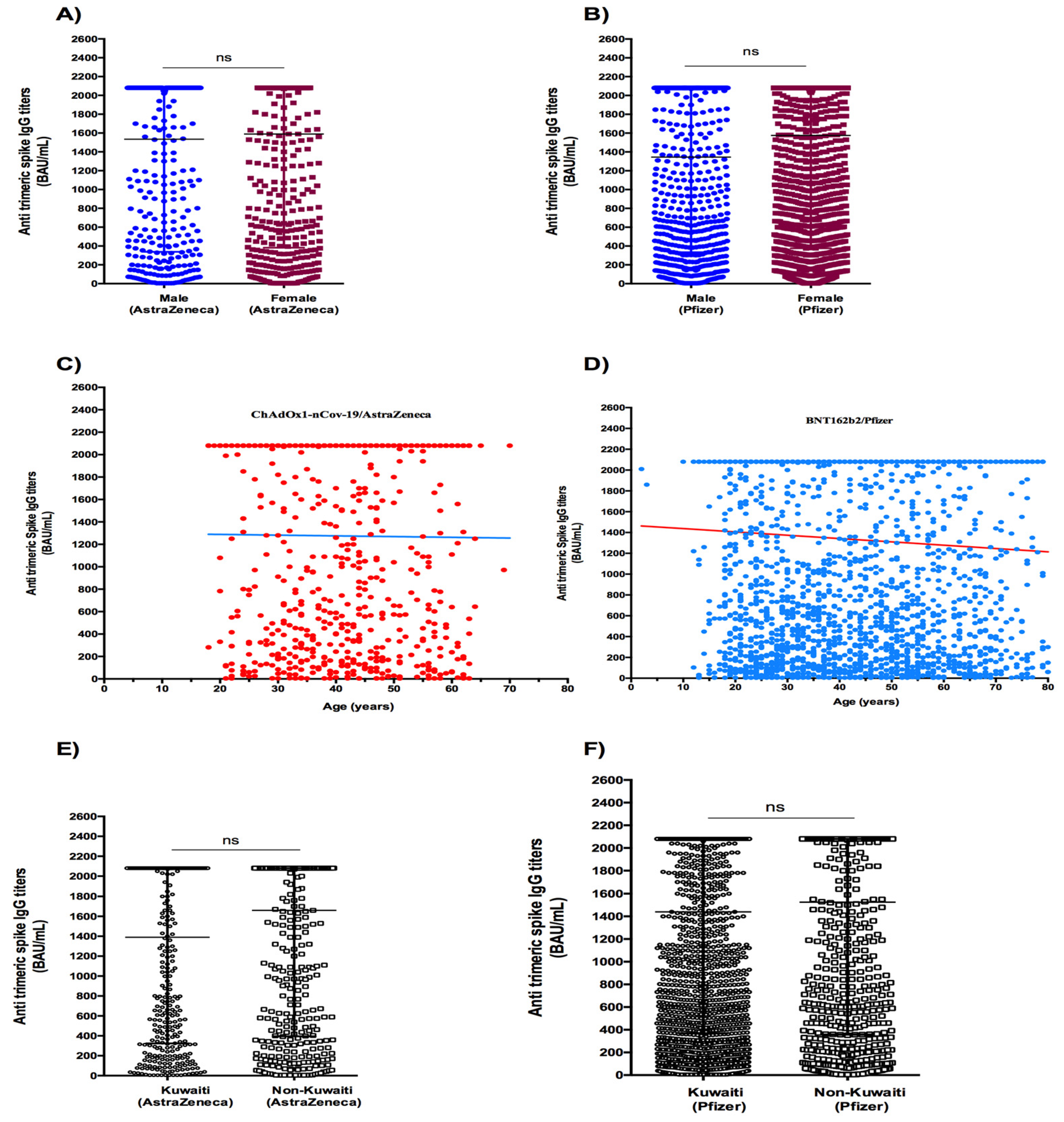
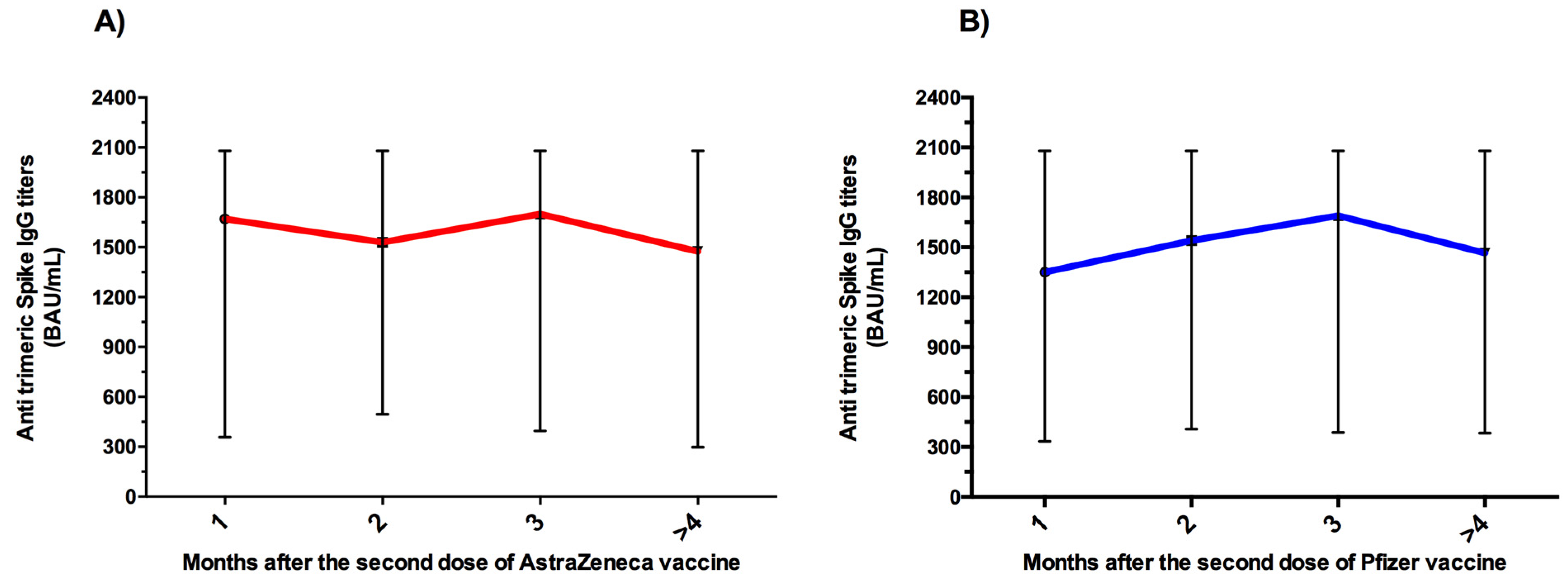
3.2. Seroprevalence in the General Population during the Post-Vaccination Period
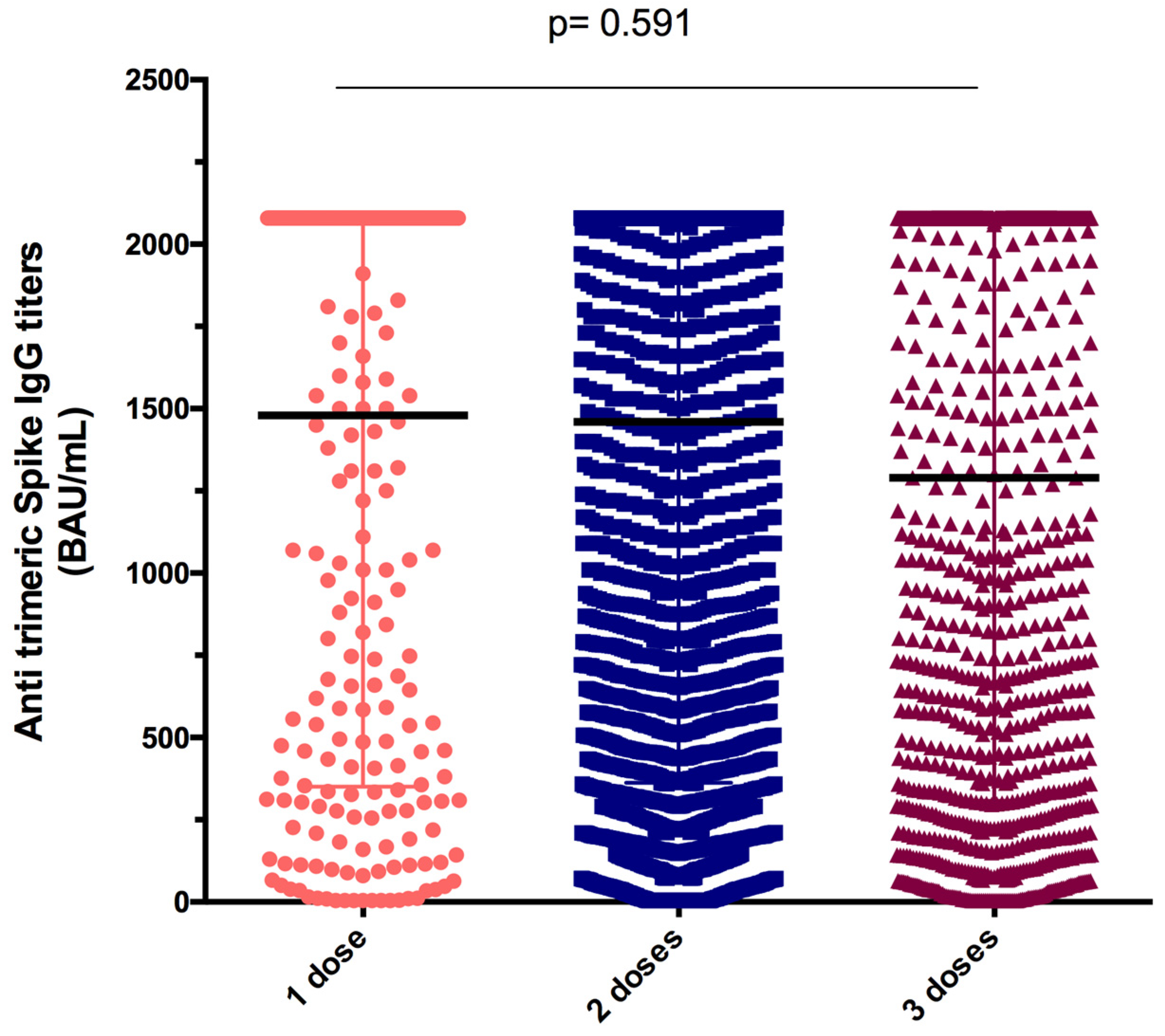
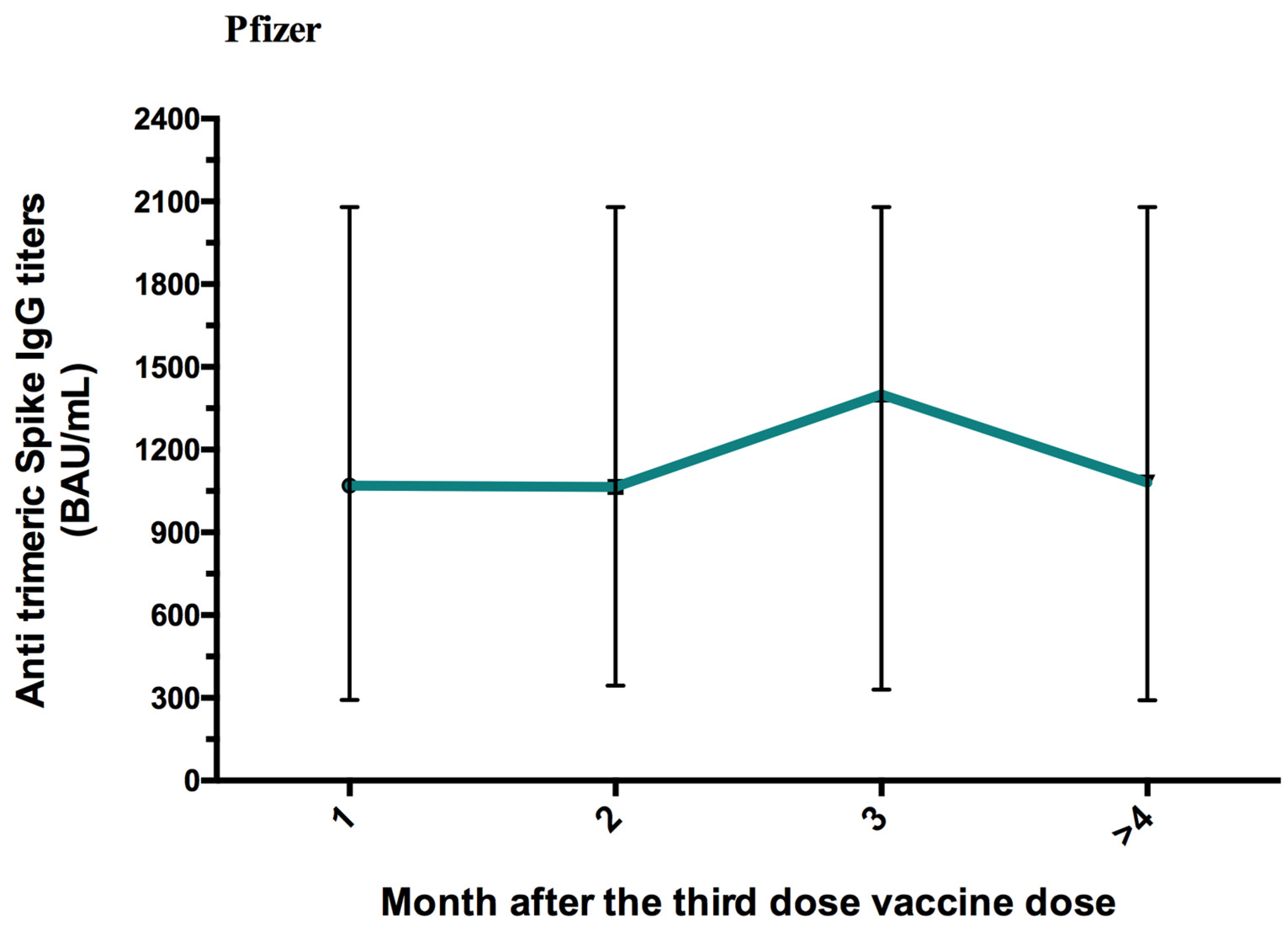
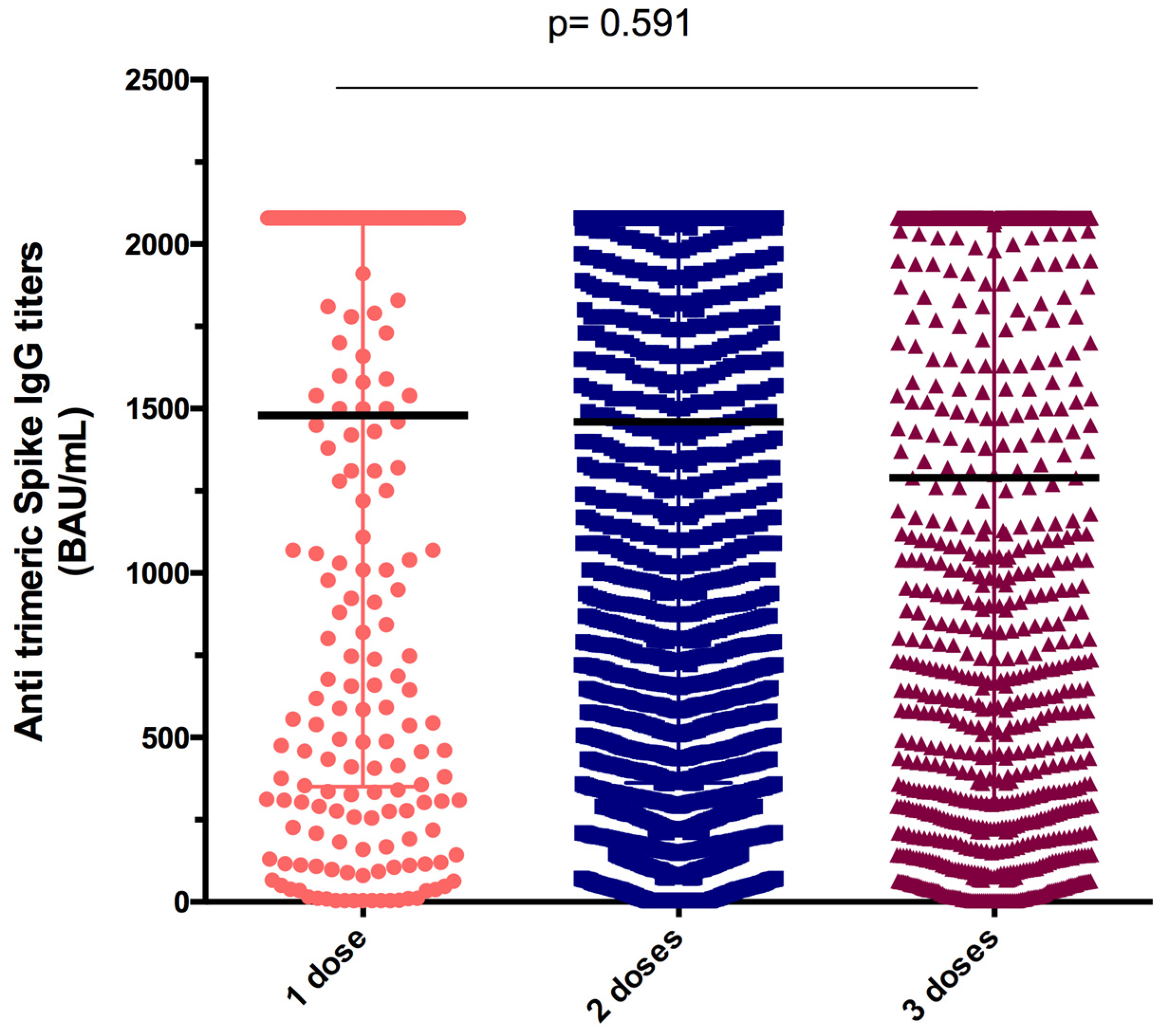
3.3. Antibody Response to One, Two, and Three Doses of SARS-CoV-2 Vaccine in the General Population of Kuwait
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.; Shi, Z.L. SARS-CoV-2 spillover events. Science 2021, 371, 120–122. [Google Scholar] [CrossRef] [PubMed]
- Kwok, K.O.; Lai, F.; Wei, W.I.; Wong, S.Y.S.; Tang, J.W.T. Herd immunity—Estimating the level required to halt the COVID-19 epidemics in affected countries. J. Infect. 2020, 80, e32–e33. [Google Scholar] [CrossRef] [PubMed]
- Altawalah, H. Antibody Responses to Natural SARS-CoV-2 Infection or after COVID-19 Vaccination. Vaccines 2021, 9, 910. [Google Scholar] [CrossRef] [PubMed]
- Arora, R.K.; Joseph, A.; Van Wyk, J.; Rocco, S.; Atmaja, A.; May, E.; Yan, T.; Bobrovitz, N.; Chevrier, J.; Cheng, M.P.; et al. SeroTracker: A global SARS-CoV-2 seroprevalence dashboard. Lancet Infect. Dis. 2021, 21, e75–e76. [Google Scholar] [CrossRef]
- Altawalah, H.; Alfouzan, W.; Dhar, R.; Alali, W.; Bastaki, H.; Al-Fadalah, T.; Al-Ghimlas, F.; Rabaan, A.A.; Ezzikouri, S. Severe acute respiratory syndrome coronavirus 2 seroprevalence survey among 10,256 workers in Kuwait. J. Clin. Virol. Plus 2021, 1, 100017. [Google Scholar] [CrossRef]
- Nasreen, S.; Chung, H.; He, S.; Brown, K.A.; Gubbay, J.B.; Buchan, S.A.; Fell, D.B.; Austin, P.C.; Schwartz, K.L.; Sundaram, M.E.; et al. Effectiveness of COVID-19 vaccines against symptomatic SARS-CoV-2 infection and severe outcomes with variants of concern in Ontario. Nat. Microbiol. 2022, 7, 379–385. [Google Scholar] [CrossRef]
- Feikin, D.R.; Higdon, M.M.; Abu-Raddad, L.J.; Andrews, N.; Araos, R.; Goldberg, Y.; Groome, M.J.; Huppert, A.; O’Brien, K.L.; Smith, P.G.; et al. Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: Results of a systematic review and meta-regression. Lancet 2022, 399, 924–944. [Google Scholar] [CrossRef]
- Favresse, J.; Bayart, J.L.; Mullier, F.; Elsen, M.; Eucher, C.; Van Eeckhoudt, S.; Roy, T.; Wieers, G.; Laurent, C.; Dogné, J.M.; et al. Antibody titres decline 3-month post-vaccination with BNT162b2. Emerg. Microbes Infect. 2021, 10, 1495–1498. [Google Scholar] [CrossRef]
- Jalkanen, P.; Kolehmainen, P.; Häkkinen, H.K.; Huttunen, M.; Tähtinen, P.A.; Lundberg, R.; Maljanen, S.; Reinholm, A.; Tauriainen, S.; Pakkanen, S.H.; et al. COVID-19 mRNA vaccine induced antibody responses against three SARS-CoV-2 variants. Nat. Commun. 2021, 12, 3991. [Google Scholar] [CrossRef]
- Ebinger, J.E.; Fert-Bober, J.; Printsev, I.; Wu, M.; Sun, N.; Prostko, J.C.; Frias, E.C.; Stewart, J.L.; Van Eyk, J.E.; Braun, J.G.; et al. Antibody responses to the BNT162b2 mRNA vaccine in individuals previously infected with SARS-CoV-2. Nat. Med. 2021, 27, 981–984. [Google Scholar] [CrossRef]
- Lombardi, A.; Consonni, D.; Oggioni, M.; Bono, P.; Renteria, S.U.; Piatti, A.; Pesatori, A.C.; Castaldi, S.; Muscatello, A.; Riboldi, L.; et al. SARS-CoV-2 anti-spike antibody titres after vaccination with BNT162b2 in naïve and previously infected individuals. J. Infect. Public Health 2021, 14, 1120–1122. [Google Scholar] [CrossRef]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.M.; et al. COVID-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef]
- Stringhini, S.; Zaballa, M.E.; Pullen, N.; Perez-Saez, J.; de Mestral, C.; Loizeau, A.J.; Lamour, J.; Pennacchio, F.; Wisniak, A.; Dumont, R.; et al. Seroprevalence of anti-SARS-CoV-2 antibodies 6 months into the vaccination campaign in Geneva, Switzerland, 1 June to 7 July 2021. Eurosurveillance 2021, 26, 2100830. [Google Scholar] [CrossRef]
- Jiang, C.; Wang, Y.; Hu, M.; Wen, L.; Wen, C.; Wang, Y.; Zhu, W.; Tai, S.; Jiang, Z.; Xiao, K.; et al. Antibody seroconversion in asymptomatic and symptomatic patients infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Clin. Transl. Immunol. 2020, 9, e1182. [Google Scholar] [CrossRef]
- Long, Q.X.; Tang, X.J.; Shi, Q.L.; Li, Q.; Deng, H.J.; Yuan, J.; Hu, J.L.; Xu, W.; Zhang, Y.; Lv, F.J.; et al. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat. Med. 2020, 26, 1200–1204. [Google Scholar] [CrossRef]
- Heydarifard, Z.; Zadheidar, S.; Yavarian, J.; Kalantari, S.; Nejati, A.; Mokhtari-Azad, T.; Shafiei-Jandaghi, N.Z. SARS-CoV-2 Seroprevalence in People Referred to Private Medical Laboratories in Different Districts of Tehran, Iran from May 2020 to April 2021. Virol. Sin. 2021, 36, 1236–1240. [Google Scholar] [CrossRef]
- Almaghrabi, R.S.; Alsagheir, O.I.; Alquaiz, R.M.; Alhekail, O.Z.; Abaalkhail, A.M.; Alduaij, A.A.; Algwaiz, G.F.; Alkaff, M.A.; Althawadi, S.I. Seroprevalence of SARS-CoV-2 antibodies in healthcare workers at a tertiary care hospital in Riyadh, Saudi Arabia. IJID Reg. 2022, 2, 51–54. [Google Scholar] [CrossRef]
- Al-Abri, S.S.; Al-Wahaibi, A.; Al-Kindi, H.; Kurup, P.J.; Al-Maqbali, A.; Al-Mayahi, Z.; Al-Tobi, M.H.; Al-Katheri, S.H.; Albusaidi, S.; Al-Sukaiti, M.H.; et al. Seroprevalence of SARS-CoV-2 antibodies in the general population of Oman: Results from four successive nationwide sero-epidemiological surveys. Int. J. Infect. Dis. 2021, 112, 269–277. [Google Scholar] [CrossRef]
- Zamani, M.; Poustchi, H.; Mohammadi, Z.; Dalvand, S.; Sharafkhah, M.; Motevalian, S.A.; Eslami, S.; Emami, A.; Somi, M.H.; Yazdani-Charati, J.; et al. Seroprevalence of SARS-CoV-2 antibody among urban Iranian population: Findings from the second large population-based cross-sectional study. BMC Public Health 2022, 22, 1031. [Google Scholar] [CrossRef]
- Jeremijenko, A.; Chemaitelly, H.; Ayoub, H.H.; Alishaq, M.; Abou-Samra, A.B.; Al Ajmi, J.A.A.A.; Al Ansari, N.A.A.; Al Kanaani, Z.; Al Khal, A.; Al Kuwari, E.; et al. Herd Immunity against Severe Acute Respiratory Syndrome Coronavirus 2 Infection in 10 Communities, Qatar. Emerg. Infect. Dis. 2021, 27, 1343–1352. [Google Scholar] [CrossRef] [PubMed]
- Gornyk, D.; Harries, M.; Glöckner, S.; Strengert, M.; Kerrinnes, T.; Heise, J.K.; Maaß, H.; Ortmann, J.; Kessel, B.; Kemmling, Y.; et al. SARS-CoV-2 Seroprevalence in Germany. Dtsch. Ärzteblatt Int. 2021, 118, 824–831. [Google Scholar] [CrossRef] [PubMed]
- Poustchi, H.; Darvishian, M.; Mohammadi, Z.; Shayanrad, A.; Delavari, A.; Bahadorimonfared, A.; Eslami, S.; Javanmard, S.H.; Shakiba, E.; Somi, M.H.; et al. SARS-CoV-2 antibody seroprevalence in the general population and high-risk occupational groups across 18 cities in Iran: A population-based cross-sectional study. Lancet Infect. Dis. 2021, 21, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Adam, M.H.; Mohamoud, J.H.; Mohamood, A.S.; Mohamed, A.A.; Garba, B.; Dirie, N.I. Seroprevalence of Anti-SARS-CoV-2 Antibodies in Benadir Region, Somalia. Vaccines 2022, 10, 220. [Google Scholar] [CrossRef]
- Silva, A.V.F.G.; Menezes, D.; Moreira, F.R.R.; Torres, O.A.; Fonseca, P.L.C.; Moreira, R.G.; Alves, H.J.; Alves, V.R.; Amaral, T.M.R.; Coelho, A.N.; et al. Seroprevalence, Prevalence, and Genomic Surveillance: Monitoring the Initial Phases of the SARS-CoV-2 Pandemic in Betim, Brazil. Front. Microbiol. 2022, 13, 799713. [Google Scholar] [CrossRef]
- Prakash, O.; Solanki, B.; Sheth, J.; Makwana, G.; Kadam, M.; Vyas, S.; Shukla, A.; Pethani, J.; Tiwari, H. SARS-CoV2 IgG antibody: Seroprevalence among health care workers. Clin. Epidemiol. Glob. Health 2021, 11, 100766. [Google Scholar] [CrossRef]
- Pollán, M.; Pérez-Gómez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernán, M.A.; Pérez-Olmeda, M.; Sanmartín, J.L.; Fernández-García, A.; Cruz, I.; de Larrea, N.F.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A nationwide, population-based seroepidemiological study. Lancet 2020, 396, 535–544. [Google Scholar] [CrossRef]
- Alsuwaidi, A.R.; Al Hosani, F.I.; Al Memari, S.; Narchi, H.; Abdel Wareth, L.; Kamal, H.; Al Ketbi, M.; Al Baloushi, D.; Elfateh, A.; Khudair, A.; et al. Seroprevalence of COVID-19 infection in the Emirate of Abu Dhabi, United Arab Emirates: A population-based cross-sectional study. Int. J. Epidemiol. 2021, 50, 1077–1090. [Google Scholar] [CrossRef]
- Chen, X.; Chen, Z.; Azman, A.S.; Deng, X.; Sun, R.; Zhao, Z.; Zheng, N.; Chen, X.; Lu, W.; Zhuang, T.; et al. Serological evidence of human infection with SARS-CoV-2: A systematic review and meta-analysis. Lancet Glob. Health 2021, 9, e598–e609. [Google Scholar] [CrossRef]
- Rostami, A.; Sepidarkish, M.; Leeflang, M.M.G.; Riahi, S.M.; Shiadeh, M.N.; Esfandyari, S.; Mokdad, A.H.; Hotez, P.J.; Gasser, R.B. SARS-CoV-2 seroprevalence worldwide: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 331–340. [Google Scholar] [CrossRef]
- Hallal, P.C.; Hartwig, F.P.; Horta, B.L.; Silveira, M.F.; Struchiner, C.J.; Vidaletti, L.P.; Neumann, N.A.; Pellanda, L.C.; Dellagostin, O.A.; Burattini, M.N.; et al. SARS-CoV-2 antibody prevalence in Brazil: Results from two successive nationwide serological household surveys. Lancet Glob. Health 2020, 8, e1390–e1398. [Google Scholar] [CrossRef]
- González, F.; Vielot, N.A.; Sciaudone, M.; Toval-Ruíz, C.; Premkumar, L.; Gutierrez, L.; Cuadra, E.C.; Munguia, N.; Blandón, P.; de Silva, A.M.; et al. Seroepidemiology of SARS-CoV-2 infections in an urban population-based cohort in León, Nicaragua. Epidemiol. Infect. 2021, 149, e247. [Google Scholar] [CrossRef]
- Percivalle, E.; Cambiè, G.; Cassaniti, I.; Nepita, E.V.; Maserati, R.; Ferrari, A.; Di Martino, R.; Isernia, P.; Mojoli, F.; Bruno, R.; et al. SARS-CoV-2 specific neutralising antibodies in blood donors from the Lodi Red Zone in Lombardy, Italy, as at 06 April 2020. Eurosurveillance 2020, 25, 2001031. [Google Scholar] [CrossRef]
- Silva, A.A.M.D.; Lima-Neto, L.G.; Azevedo, C.M.P.E.S.; Costa, L.M.M.D.; Bragança, M.L.B.M.; Filho, A.K.D.B.; Wittlin, B.B.; Souza, B.F.; Oliveira, B.L.C.A.; Carvalho, C.A.; et al. Population-based seroprevalence of SARS-CoV-2 and the herd immunity threshold in Maranhão. Rev. Saude Publica 2020, 54, 131. [Google Scholar] [CrossRef]
- Canto-Osorio, F.; Stern, D.; Pérez-Ferrer, C.; Arias-de la Garza, E.; Danon, L.; Barrientos-Gutiérrez, T.; Lajous, M. Seroprevalencia de SARS-CoV-2 en niños y adolescentes mexicanos en edad escolar. Salud Pública México 2021, 63, 803–806. [Google Scholar] [CrossRef]
- Alali, W.Q.; Bastaki, H.; Longenecker, J.C.; Aljunid, S.M.; AlSeaidan, M.; Chehadeh, W.; Vainio, H. Seroprevalence of SARS-CoV-2 in migrant workers in Kuwait. J. Travel Med. 2021, 28, taaa223. [Google Scholar] [CrossRef]
- Shields, A.M.; Faustini, S.E.; Hill, H.J.; Al-Taei, S.; Tanner, C.; Ashford, F.; Workman, S.; Moreira, F.; Verma, N.; Wagg, H.; et al. Increased Seroprevalence and Improved Antibody Responses Following Third Primary SARS-CoV-2 Immunisation: An Update From the COV-AD Study. Front. Immunol. 2022, 13, 912571. [Google Scholar] [CrossRef]
- Rose, R.; Neumann, F.; Grobe, O.; Lorentz, T.; Fickenscher, H.; Krumbholz, A. Humoral immune response after different SARS-CoV-2 vaccination regimens. BMC Med. 2022, 20, 31. [Google Scholar] [CrossRef]
- Heinz, F.X.; Stiasny, K. Distinguishing features of current COVID-19 vaccines: Knowns and unknowns of antigen presentation and modes of action. NPJ Vaccines 2021, 6, 104. [Google Scholar] [CrossRef]
- Lewis, D. Mix-and-match COVID vaccines: The case is growing, but questions remain. Nature 2021, 595, 344–345. [Google Scholar] [CrossRef]
- Hamaya, T.; Hatakeyama, S.; Yoneyama, T.; Tobisawa, Y.; Kodama, H.; Fujita, T.; Murakami, R.; Fujita, N.; Okamoto, T.; Yamamoto, H.; et al. Seroprevalence of SARS-CoV-2 spike IgG antibodies after the second BNT162b2 mRNA vaccine in Japanese kidney transplant recipients. Sci. Rep. 2022, 12, 5876. [Google Scholar] [CrossRef] [PubMed]
- Madhi, S.A.; Kwatra, G.; Myers, J.E.; Jassat, W.; Dhar, N.; Mukendi, C.K.; Nana, A.J.; Blumberg, L.; Welch, R.; Ngorima-Mabhena, N.; et al. Population Immunity and COVID-19 Severity with Omicron Variant in South Africa. N. Engl. J. Med. 2022, 386, 1314–1326. [Google Scholar] [CrossRef] [PubMed]
- Sendi, P.; Thierstein, M.; Widmer, N.; Babongo Bosombo, F.; Büchi, A.E.; Güntensperger, D.; Blum, M.R.; Baldan, R.; Tinguely, C.; Gahl, B.; et al. Serosurveillance after a COVID-19 vaccine campaign in a Swiss police cohort. Immun. Inflamm. Dis. 2022, 10, e640. [Google Scholar] [CrossRef]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 COVID-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef] [PubMed]
- Shrotri, M.; Navaratnam, A.M.D.; Nguyen, V.; Byrne, T.; Geismar, C.; Fragaszy, E.; Beale, S.; Fong, W.L.E.; Patel, P.; Kovar, J.; et al. Spike-antibody waning after second dose of BNT162b2 or ChAdOx1. Lancet 2021, 398, 385–387. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, H.R.; Parai, D.; Dash, G.C.; Kshatri, J.S.; Mishra, N.; Choudhary, P.K.; Pattnaik, D.; Panigrahi, K.; Behera, S.; Sahoo, N.R.; et al. Persistence of Antibodies Against Spike Glycoprotein of SARS-CoV-2 in Healthcare Workers Post Double Dose of BBV-152 and AZD1222 Vaccines. Front. Med. 2021, 8, 778129. [Google Scholar] [CrossRef]
- Parai, D.; Choudhary, H.R.; Dash, G.C.; Behera, S.; Mishra, N.; Pattnaik, D.; Raghav, S.K.; Mishra, S.K.; Sahoo, S.K.; Swain, A.; et al. Dynamicity and persistence of severe acute respiratory syndrome coronavirus-2 antibody response after double dose and the third dose with BBV-152 and AZD1222 vaccines: A prospective, longitudinal cohort study. Front. Microbiol. 2022, 13, 942659. [Google Scholar] [CrossRef]
- Lee, N.; Jeong, S.; Lee, S.K.; Cho, E.J.; Hyun, J.; Park, M.J.; Song, W.; Kim, H.S. Quantitative Analysis of Anti-N and Anti-S Antibody Titers of SARS-CoV-2 Infection after the Third Dose of COVID-19 Vaccination. Vaccines 2022, 10, 1143. [Google Scholar] [CrossRef]
- Paramithiotis, E.; Sugden, S.; Papp, E.; Bonhomme, M.; Chermak, T.; Crawford, S.Y.; Demetriades, S.Z.; Galdos, G.; Lambert, B.L.; Mattison, J.; et al. Cellular Immunity Is Critical for Assessing COVID-19 Vaccine Effectiveness in Immunocompromised Individuals. Front. Immunol. 2022, 13, 880784. [Google Scholar] [CrossRef]
- Sadarangani, M.; Marchant, A.; Kollmann, T.R. Immunological mechanisms of vaccine-induced protection against COVID-19 in humans. Nat. Rev. Immunol. 2021, 21, 475–484. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. Participants | Seroprevalence (%) (95% CI) | p-Value | Adjusted OR (95% CI) | p-Value |
|---|---|---|---|---|---|
| Sex * | |||||
| Male | 2189 | 28.4 (27.4–29.5) | <0.0001 | 1.00 | |
| Female | 2769 | 31.1 (30.1–32.0) | 1.3 (1.2–1.4) | <0.0001 | |
| Age group (years) * | <0.0001 | ||||
| <15 | 328 | 23.0 (20.9–25.3) | 1.00 | ||
| 15–24 | 530 | 20.5 (19.0–22.1) | 1.1 (1–1.3) | 0.06 | |
| 25–44 | 1736 | 26.0 (24.9–27.0) | 1.2 (1.0–1.3) | 0.02 | |
| 45–64 | 1619 | 30.0 (28.4–30.8) | 1.4 (1.2–1.6) | <0.0001 | |
| ≥65 | 742 | 23.1 (21.7–24.6) | 1.0 (0.9–1.2) | 0.940 | |
| Nationality * | <0.0001 | ||||
| Kuwaiti | 2305 | 20.8% (20.0–21.6) | 1.00 | ||
| Non-Kuwaiti | 2629 | 32.2% (31.2–33.2) | 1.8 (1.7–1.9) | <0.0001 |
| COVID-19 Vaccination Status | General Population |
|---|---|
| 1 dose BNT162b2 Pfizer -IgG positive, (%) (95% CI) ChAdOx1-nCov-19 AstraZeneca-IgG positive, (%) (95% CI) 2 doses BNT162b2 Pfizer -IgG positive, (%) (95% CI) ChAdOx1-nCov-19 AstraZeneca-IgG positive, (%) (95% CI) Mix-and-match AstraZeneca- Pfizer IgG positive, (%) (95% CI) 3 doses IgG positive, (%) (95% CI) | 95.21 (91.15–97.46) 92.86 (80.99–97.54) 94.93 (94.06–95.68) 96.25 (94.67–97.38) 95.86 (76.39–99.11) 94.67 (93.18–95.85) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alfouzan, W.; Altawalah, H.; AlSarraf, A.; Alali, W.; Al-Fadalah, T.; Al-Ghimlas, F.; Alajmi, S.; Alajmi, M.; AlRoomi, E.; Jeragh, A.; et al. Changing Patterns of SARS-CoV-2 Seroprevalence: A Snapshot among the General Population in Kuwait. Vaccines 2023, 11, 336. https://doi.org/10.3390/vaccines11020336
Alfouzan W, Altawalah H, AlSarraf A, Alali W, Al-Fadalah T, Al-Ghimlas F, Alajmi S, Alajmi M, AlRoomi E, Jeragh A, et al. Changing Patterns of SARS-CoV-2 Seroprevalence: A Snapshot among the General Population in Kuwait. Vaccines. 2023; 11(2):336. https://doi.org/10.3390/vaccines11020336
Chicago/Turabian StyleAlfouzan, Wadha, Haya Altawalah, Ahmad AlSarraf, Walid Alali, Talal Al-Fadalah, Fahad Al-Ghimlas, Saud Alajmi, Mubarak Alajmi, Ebtehal AlRoomi, Ahlam Jeragh, and et al. 2023. "Changing Patterns of SARS-CoV-2 Seroprevalence: A Snapshot among the General Population in Kuwait" Vaccines 11, no. 2: 336. https://doi.org/10.3390/vaccines11020336
APA StyleAlfouzan, W., Altawalah, H., AlSarraf, A., Alali, W., Al-Fadalah, T., Al-Ghimlas, F., Alajmi, S., Alajmi, M., AlRoomi, E., Jeragh, A., & Dhar, R. (2023). Changing Patterns of SARS-CoV-2 Seroprevalence: A Snapshot among the General Population in Kuwait. Vaccines, 11(2), 336. https://doi.org/10.3390/vaccines11020336