1. Introduction
Liver regeneration has been known for centuries and has been subject to many myths. The regenerative capacity of the liver determines the success of many surgical procedures such as anatomic and non-anatomic or living donor hepatectomy (LDH), which is an important part of living donor liver transplantation (LDLT) [
1]. Furthermore, this ability of the liver protects organisms from many injurious effects [
2]. There are two main liver regeneration mechanisms: typical and progenitor cell-dependent regeneration. Both mechanisms are triggered during any injury to the liver, however, the dominance of either mechanism depends on the amount of liver tissue that is affected by the injurious event. The studies on experimental models have shown that the regeneration of the liver has several stages including priming, proliferation, and termination, all providing hepatocyte proliferation and hypertrophy [
3,
4,
5].
The process of regeneration has been studied extensively in preclinical models and factors such as the hepatocyte growth factor (HGF), interleukin-6 (IL-6), tumor necrosis factor-α (TNF- α), and signal transducer and activator of transcription 3 (STAT3), whilst Notch and Yap pathways have been found to be important in the regenerative process. During the era of COVID-19, the role of angiotensin-converting enzyme II receptors (ACEII) has been emphasized [
6,
7,
8,
9]. Studies have shown that ACEII is over-expressed early after partial hepatectomy and is sustained until the termination of the regenerative process [
6,
7,
8,
9]. Studies regarding the ACEII levels following liver resection in humans are lacking. Retinol binding protein (RBP) and especially RBP4 have been shown to play a role in glucose homeostasis in the liver in various pathological processes such as non-alcoholic fatty liver disease [
10]. However, its role in the regenerating liver where hypoglycemia is prevalent has not been studied. Ornithine decarboxylase (ODC) is an important enzyme in the catabolism of ornithine to polyamines which is very important in the stabilization of the deoxyribonucleic acid (DNA) structure. ODC can be considered as an indirect marker for DNA synthesis [
11]. There is a lack of literature analyzing the role of ODC in liver regeneration in liver transplantation. Alfa Feto Protein (AFP) is mainly involved in hepatoblasts and embryonic hepatic progenitor cells [
12]. These cells are shown to be conditionally activated following various injurious effects in preclinical models [
12]. Therefore, it can be stated that AFP is associated with hepatic progenitor cell-dependent liver regeneration such as those seen in massive hepatic resections and toxic liver injury [
12]. The association of changes in AFP levels needs to be analyzed with the regenerative process in LDLT. Des-gamma-carboxy prothrombin (DCP) is a known marker for the prognostication and diagnosis of hepatocellular carcinoma [
13]. However, changes in the levels of DCP in hepatic regeneration have not been analyzed before.
As can be seen clearly, there is a lack of comprehensive studies regarding the regenerative process following living donor hepatectomy (LDH) and in the recipients following the transplantation of the partial liver graft. Furthermore, the majority of our knowledge regarding liver regeneration following partial hepatectomy originates from preclinical experimental models [
14].
We are a center of excellence in LDLT and we perform an average of 300 cases of LDLT annually. Therefore, in the present study, we aimed to evaluate the process of liver regeneration in living liver donors (LLDs), who underwent LDH by evaluating serum biomarkers of regeneration including AFP, DCP, ACEII, ODC, and RBP4.
2. Materials and Methods
2.1. Study Population and Design
This is a prospective cohort study. We performed a power analysis to determine the minimum number of subjects that should be included in the present study. Power analyses showed that, with the study power being 0.95, the alpha coefficient being 0.05, and the effect size being (d) = 0.5, the minimum number of subjects required for the study was calculated to be 44. The power analysis was performed using G*Power 3.1.9.7 (Düsseldorf, Germany). We prospectively analyzed and followed up with 63 LLDs who received LDH between 2020 and 2022 in Inonu University Liver Transplant Institute and included in our study. Our LLDs evaluation algorithm, LDH technique, and postoperative follow-up protocol have been previously defined [
15]. Verbal and written informed consent were obtained from all LLDs.
2.2. Study Parameters
The demographic characteristics including age, sex, body mass index (BMI), habits (smoking and alcohol consumption), blood type (ABO and Rh), operative parameters including the type of liver graft resected, graft weight, remnant liver volume, postoperative complications requiring relaparotomy (such as bleeding and biliary peritonitis) and clinical variables including the routine laboratory parameters on preoperative and postoperative days (PODs) 1, 3, 5, 7, 10 and 21 were collected. Specific laboratory values including alfa-fetoprotein (AFP), des carboxy prothrombin (DCP), ornithine decarboxylase (ODC), retinol binding protein 4 (RBP4), and angiotensin converting enzyme isotype II (ACEII) levels were measured in the same time intervals.
All routine laboratory evaluations including liver function tests, complete blood count, and coagulation studies were obtained from the hospital database. The demographic and operative parameters were obtained from the electronic patient registry. Five milliliters of extra blood was drawn from the subjects and transferred to Inonu University Liver Transplant Institute Hepatology Research Laboratories and all the samples were centrifuged at 2000 rpm at 4 °C for 10 min and serum obtained from the blood samples were divided into four aliquots and stored at −80 °C until the experiments were performed. The comparison of these variables was performed according to different study subgroups; (i) the routine and specific laboratory variables were compared according to sex (male versus females); (ii) according to LDH type (right-lobe LDH versus left-lobe LDH (including left-lobe lateral segment)); and (iii) according to the presence or absence of complications requiring relaparotomy.
2.3. Measurement of the Specific Laboratory parameters
All routine and specific biochemical analysis were performed at Inonu University Liver Transplant Institute Hepatology Research Laboratories. All specific measurements including AFP, DCP, ACEII, ODC, and RBP4 were performed using enzyme-linked immunosorbent assay (ELISA). The measurements were performed by using Human AFP ELISA Kit (BT-LAB, Cat No: E1630Hu), Human DCP ELISA Kit (BT-LAB, Cat No: E4012Hu), Human ACEII ELISA Kit (BT-LAB, Cat No: E3169Hu), Human ODC ELISA Kit (BT-LAB, Cat No: E0845Hu), and Human RBP4 ELISA Kit (BT-LAB, Cat No: E1206Hu) according to manufacturer’s instructions. For all ELISA measurements, after pipetting 40 µL of serum samples to the wells of the precoated ELISA plate, 10 µL of the biotinylated antibody of AFP, DCP, ACEII, ODC, and RBP4 were added to sample wells, respectively. Then, 50 µL of Streptavidin-HRP was added and incubated for 1 h at 37 °C. At the end of the incubation period, the wells were washed thoroughly, 50 µL of both Solution A and B were added and incubated for 10 min at 37 °C in the dark. Then, 50 µL of Stop Solution was pipetted and the color of the solution turned yellow. Absorbance was determined by using Biotek Synergy H1m™ microplate reader (BioTek Instruments Inc., Winooski, VT, USA) at 450 nm within 10 min.
2.4. Ethics Committee Approval and Financial Support
The ethics committee approval was obtained from the Malatya Clinical Research Ethics Committee (Approval no: 2020/170). All stages of the study were carried out according to the guidelines of the Declaration of Helsinki. The financial support was received from the Inonu University Scientific Research Projects Coordination Unit (Project ID: TSA-2021-2382).
2.5. Statistical Analysis
The categorical variables were expressed as the number of individuals and percentage of the study population. Continuous variables are expressed as mean ± standard deviation or median (95% lower CL for median; 95% upper CL for median). The normality of continuous variables was tested using the Kolmogorov–Smirnov and Shapiro–Wilk tests. The Friedman, Mann–Whitney U, and Kruskal–Wallis tests were used to compare the dependent variables among the study groups. Any p-value less than 0.05 was considered statistically significant. All analyses were performed using the Statistical Software Package for Social Sciences version 26.0 (IBM, SPSSv26.0, Armonk, NY, USA).
4. Discussion
Liver regeneration is a crucial component that determines the success of major hepatic resections such as formal hepatectomy, informal hepatectomy, and LDH. The regenerative capacity of the liver enables us to perform major liver resections and if this regenerative process is disturbed in either way, post-hepatectomy liver failure or a small-for-size syndrome is observed [
16]. After major hepatectomy series, the incidence of post-hepatectomy liver failure is reported as high as 32% [
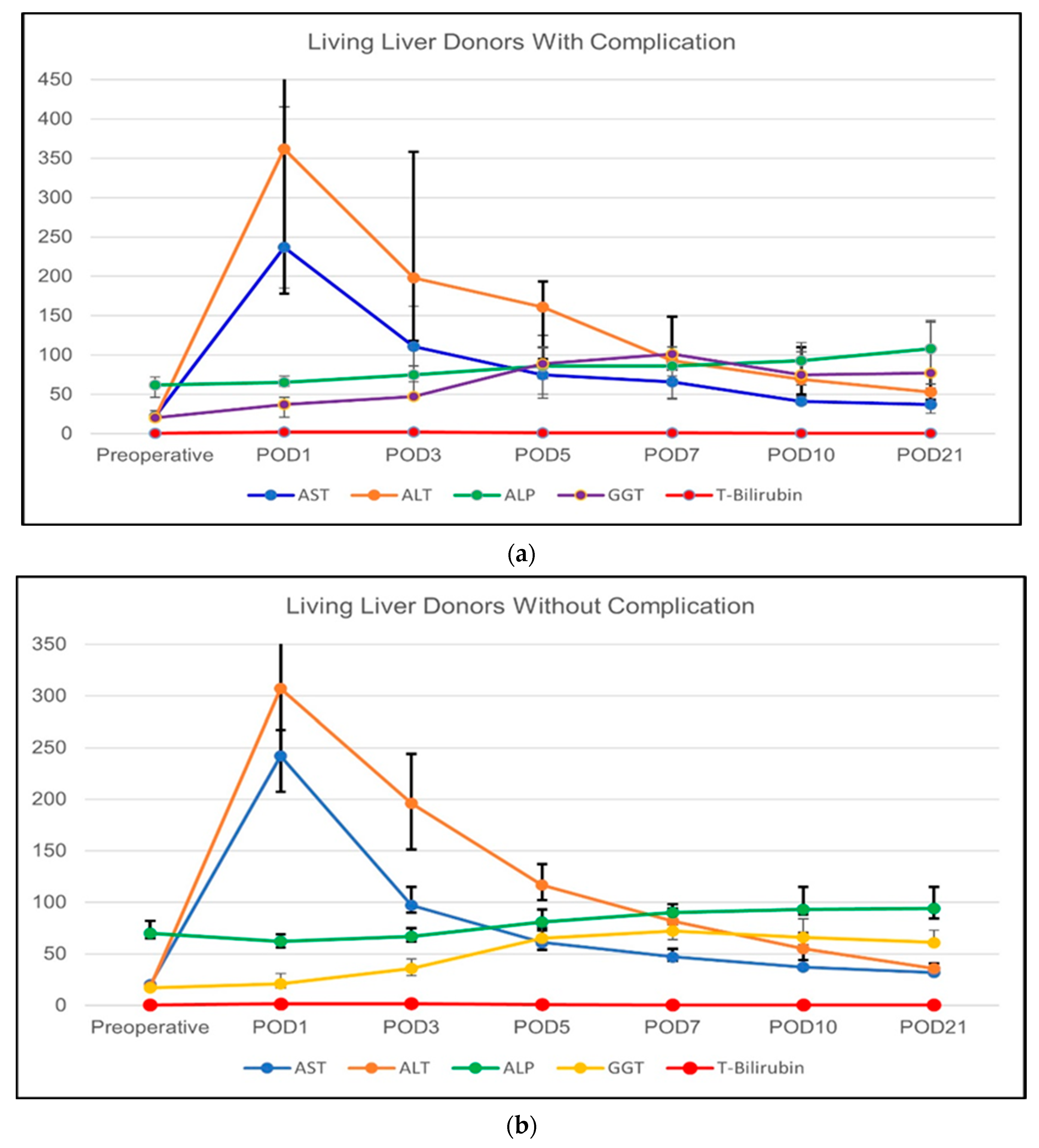
17]. In the present study, we have found that markers of regeneration change significantly after LDH in LLDs. This phenomenon is more prominent in right-lobe liver grafts. The change in the serum levels of the markers is not prominently observed in LLDs with complication who require re-laparotomy. To our knowledge, this is the only study analyzing the markers of regeneration in LLDs.
Conventional markers for liver and hepatocyte damage are ALT, AST, and ALP [
18]. However, these are not sufficient to evaluate the regenerative process of the liver [
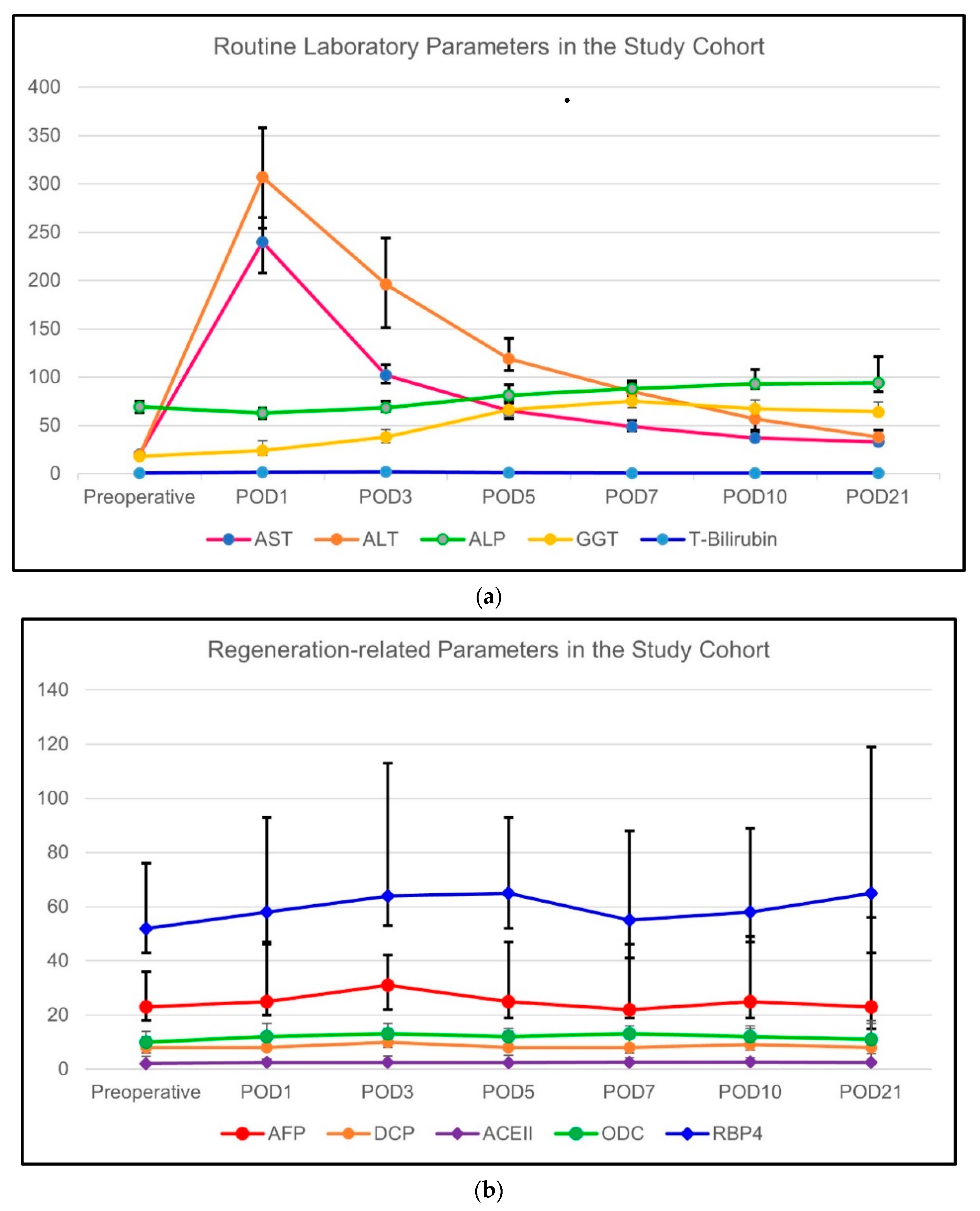
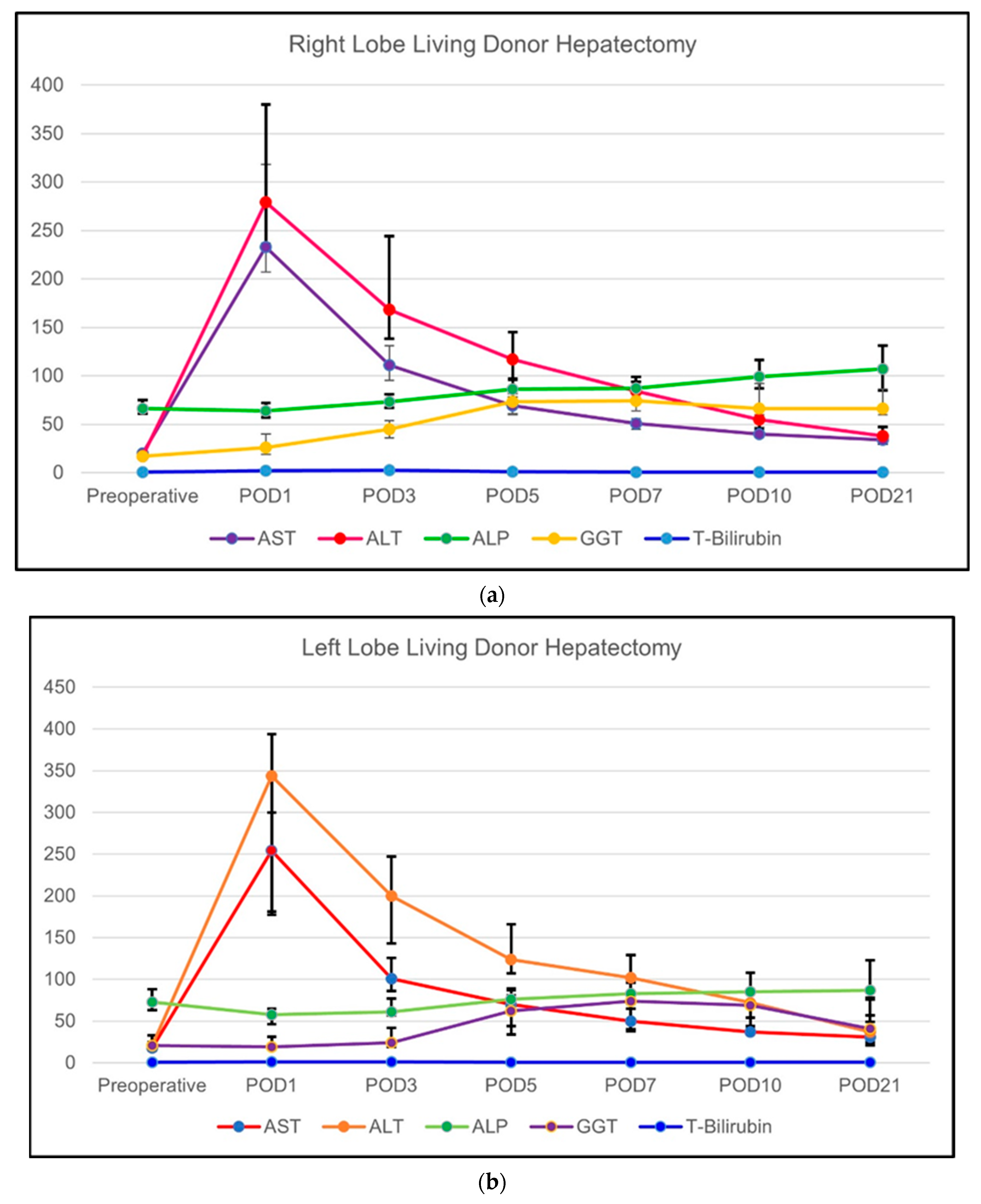
19]. There is clearly a need for additional markers to evaluate the regenerative capacity of the liver. Furthermore, there is a need for the evaluation of the normal postoperative course of these markers so that the deviation from the normal course can be evaluated under complicated conditions. In the present study, the markers of hepatocellular markers such as AST, ALT, ALP, and GGT have been elevated towards the POD3 and POD5. Thereafter, a decline in the levels of these enzymes has been observed. This pattern of change was observed in both right, left, and left lateral liver grafts. However, in terms of remnant liver volume, right-lobe liver grafts are associated with lower remnant liver volumes when compared to [
20]. This has been reflected in the postoperative course of the enzymes and AST, ALT, ALP, and GGT have been significantly higher in the right-lobe grafts in various postoperative time intervals when compared to left- and left-lateral-liver grafts. Similarly, ALT and AST levels of the male LLDs were higher than the female in postoperative periods. This may be related with the liver mass and the amount of liver tissue resected from the male patients. However, we could not find any data in the literature to explain the differences in liver function tests in LLDs according to sex.
We previously found that the total bilirubin was an important factor in determining the prognosis of the patient’s acute liver failure who has undergone liver transplantation [
21]. Studies have shown that the bilirubin levels are indicative of the function of the liver and it is correlated with the severity of liver dysfunction [
22,
23]. In the present study, we found that the total bilirubin levels of the right-lobe liver grafts have been significantly higher than the other liver grafts which may be related with the larger mass of the liver removed and the associated decrease in the function initially observed in LLDs. Furthermore, in complicated patients, the postoperative bilirubin levels tended to be higher during the postoperative period, although this was not statistically significant. However, this finding shows the impact of any postoperative period on the function of the liver.
Historically, Rao et al. [
24] showed that, in chloroform poisoning, serum markers such as GGT, DCP, and AFP were elevated and their combined analysis with the markers of hepatocellular damage would give accurate prognostic information for the affected patients. Later on, the same team evaluated the prognostic significance of these markers in mushroom poisoning [
18]. Both studies have shown that, in patients who survived, regenerative markers increased gradually while the markers of liver damage decreased. Living donor hepatectomy and especially harvesting right-lobe grafts has a risk of post-hepatectomy liver failure [
25]. Furthermore, there is a certain level of liver dysfunction in the early postoperative period following living donor hepatectomy [
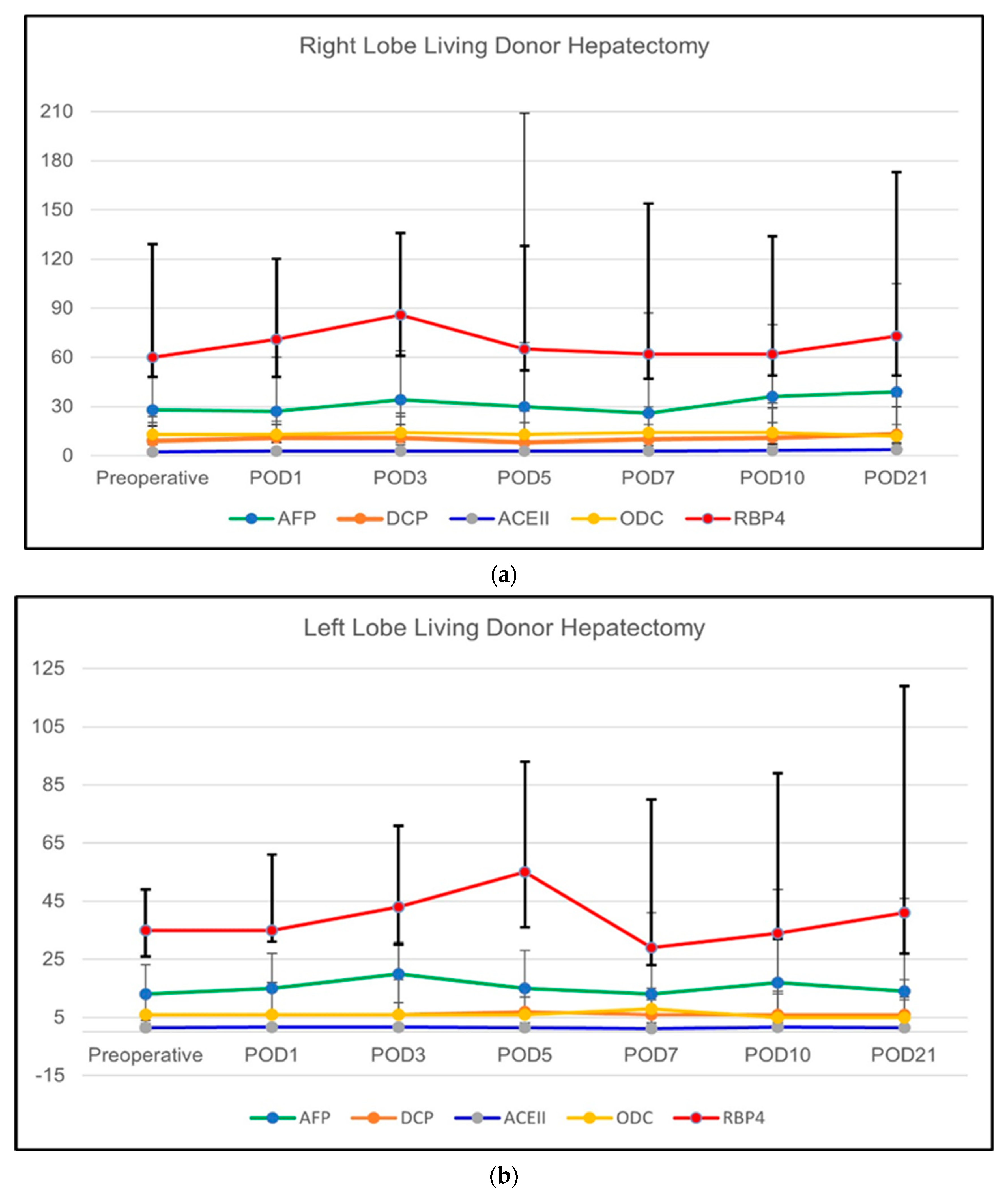
26]. For this reason, we wanted to evaluate the course of regenerative markers and the markers of hepatocellular damage in LLDs. We found that the markers of hepatocellular damage have gradually increased towards the POD3 and POD5 and gradually decreased thereafter. On the other hand, we observed a sustained elevation of AFP, DCP, ACEII, ODC, and GGT. Furthermore, this trend in the levels of regeneration markers did not occur in left-lobe liver grafts (except for DCP elevation); however, the right-lobe liver grafts showed a pattern of sustained AFP, DCP, ACEII, and ODC elevation. This proves that, after the removal of right-lobe liver grafts, progenitor oval cells actively take part in the regeneration of the remnant liver. The data regarding the serum ACEII levels following the living donor hepatectomy is lacking. Our study is the first study to emphasize the regeneration-related role of ACEII and it is mainly enhanced in right-lobe liver grafts. Furthermore, our study showed a sex difference between the serum levels of ACEII, which was previously studied in patients with hypertension and cardiac failure [
27,
28]; however, not in a liver transplant setting. The results of the present study show that there is a difference between the regenerative capacity of the female and male LLDs. It has been emphasized in a limited number of studies that the livers of female patients have a higher regenerative potential [
29,
30,
31]. Unfortunately, our data are limited in terms of their ability to explain this observation, however, we can clearly state that it is not related to the type of graft because the frequency of the right- and left-lobe liver grafts were similar among the groups. The evaluation of the regeneration-related biomarkers and their changes according to the sex of the LLDs requires further studies with higher patient numbers.
However, in left and left lateral liver grafts, the changes in the levels of the enzymes AST, ALT, ALP, and GGT were like the general population. Therefore, evaluating the regenerative process according to elevated liver enzymes may be misleading. The DCP levels in left-lobe liver grafts changed mildly but it was statistically significant. Although our literature search did not yield any relationship between DCP and progenitor cells, our results also suggest that DCP may be indicative of the hepatocyte activity after partial hepatectomy rather than a progenitor cell marker. AFP, ACEII, and ODC seem to be better markers for progenitor-assisted liver regeneration.
We only had eight patients with early postoperative complications requiring relaparotomy. The regenerative markers tend to be elevated in these patients and the fluctuations in the level of the liver enzymes were similar to the general population. We believe that we did not observe any significant changes in the serum levels of the regenerative markers because there was a small group of complicated LLDs.
Our study is the first study to address liver regeneration in LLDs. Furthermore, it gives valuable information regarding the changes in the levels of these biomarkers and the transaminases. However, the current study has some limitations. The first one is the low number of patients. Although we reached the minimum number of patients calculated in a power analysis, the regenerative markers showed wide variation. Therefore, we believe that studies with a larger number of patients will reduce the margin of error. Furthermore, we tried to perform CT volumetry as a part of the follow-up of these LLDs; however, the compliance of the LLDs was low and there were a lot of missing data. Performing volumetric analysis and correlating the results with the levels of the regenerative markers would yield valuable information.
In conclusion, there is dual hepatic regeneration and the dominant mechanism depends on the volume of the resected liver. In right-lobe liver grafts, the remnant is small and this triggers progenitor cell-mediated regeneration. However, in left-lobe and left-lateral-lobe grafts, progenitor-related regenerative markers are not elevated. AFP, ACEII, and ODC are good markers for the surveillance of regeneration following living donor hepatectomy.



 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}