
Increased EBV DNAemia after Anti-SARS-CoV-2 Vaccination in Solid Organ Transplants


{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Patients and Methods
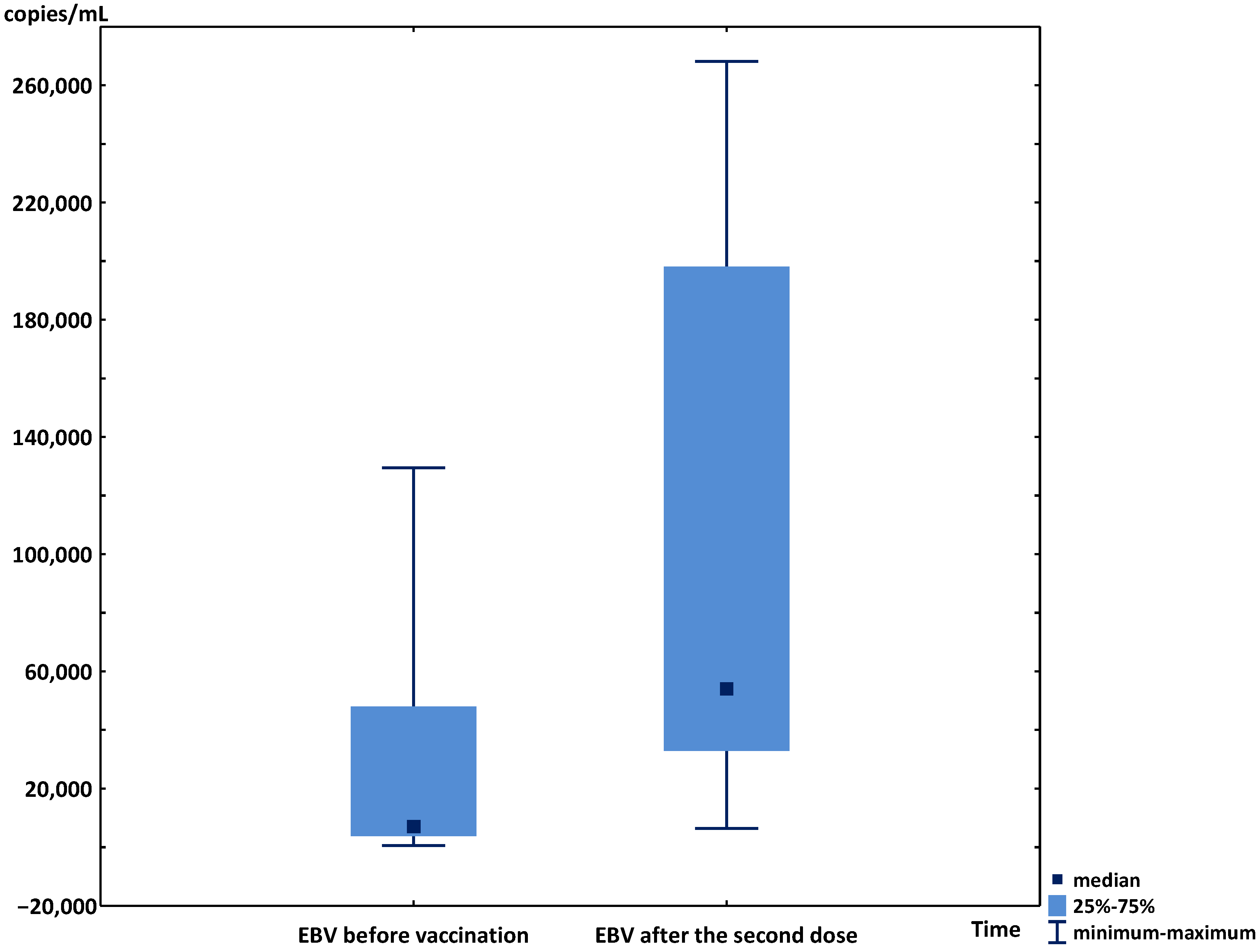
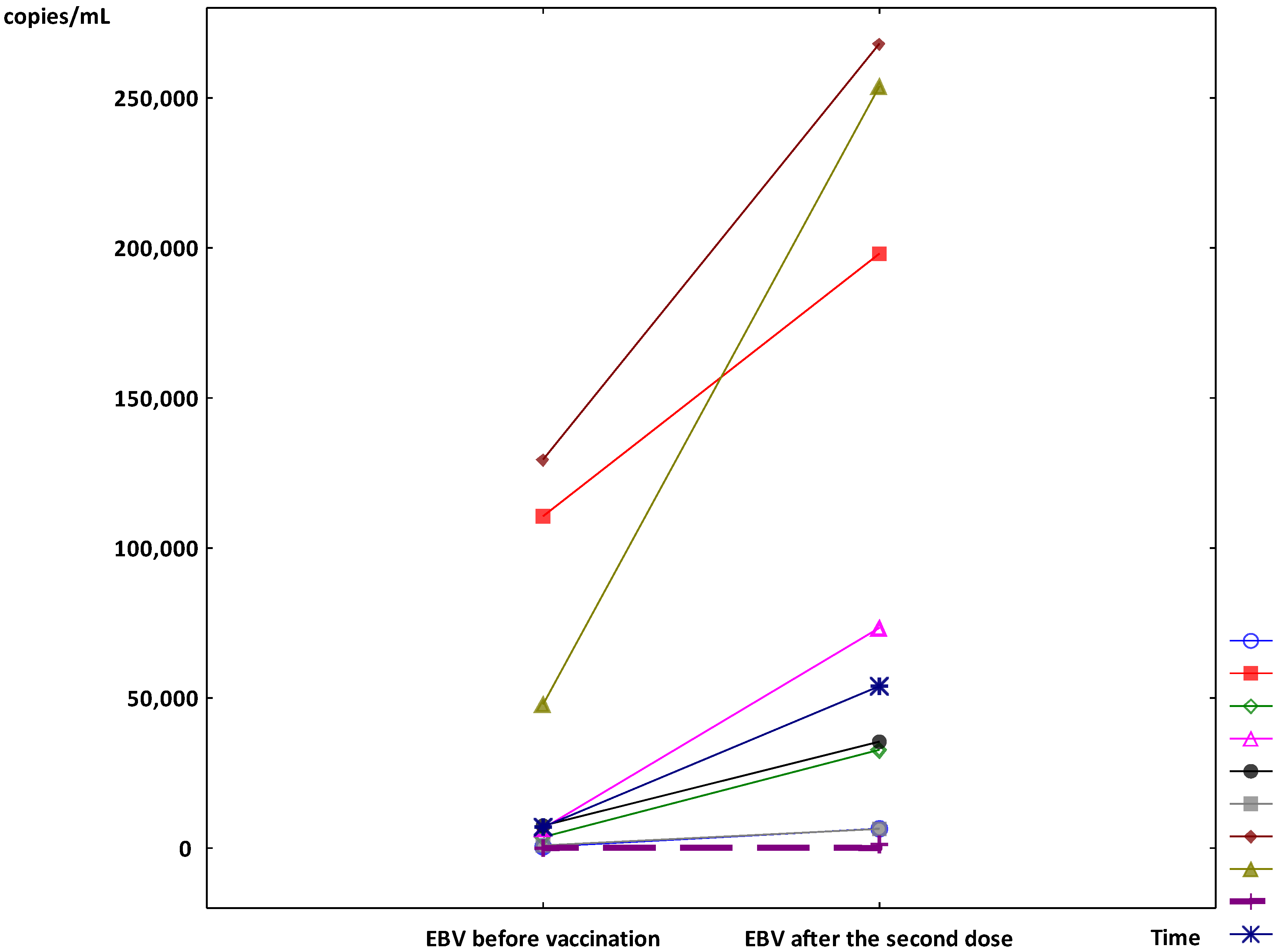
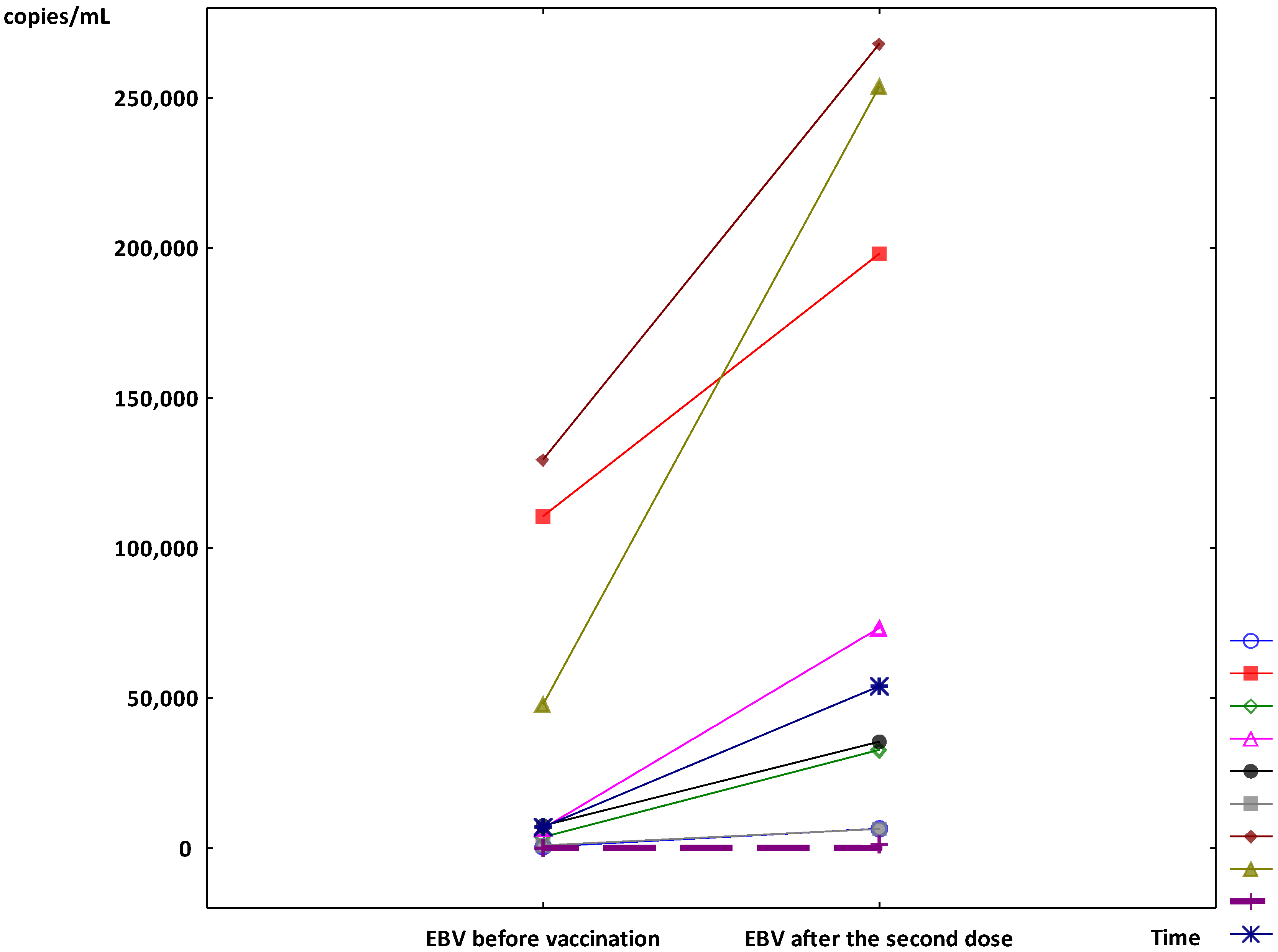
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shahid, Z.; Kalayanamitra, R.; McClafferty, B.; Kepko, D.; Ramgobin, D.; Patel, R.; Jones, K.; Bhatt, D.; Golamari, R.; Jain, R.; et al. COVID-19 and older adults: What we know. J. Am. Geriatr. Soc. 2020, 68, 926–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallo Marin, B.; Aghagoli, G.; Lavine, K.; Yang, L.; Siff, E.J.; Chiang, S.S.; Salazar-Mater, T.P.; Dumenco, L.; Savaria, M.C.; Aung, S.N.; et al. Predictors of COVID-19 severity: A literature review. Rev. Med. Virol. 2021, 31, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kadali, R.A.K.; Janagama, R.; Peruru, S.; Malayala, S.V. Side effects of BNT162b2 mRNA COVID-19 vaccine: A randomized, cross-sectional study with detailed self-reported symptoms from healthcare workers. Int. J. Infect. Dis. 2021, 106, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Hall, V.G.; Ferreira, V.H.; Ierullo, M.; Ku, T.; Marinelli, T.; Majchrzak-Kita, B.; Yousuf, A.; Kulasingam, V.; Humar, A.; Kumar, D. Humoral and cellular immune response and safety of two-dose SARS-CoV-2 mRNA-1273 vaccine in solid organ transplant recipients. Am. J. Transplant. 2021, 21, 3980–3989. [Google Scholar] [CrossRef]
- Neves, M.; Marinho-Dias, J.; Ribeiro, J.; Sousa, H. Epstein-Barr virus strains and variations: Geographic or disease-specific variants? J. Med. Virol. 2017, 89, 373–387. [Google Scholar] [CrossRef]
- Ambinder, R.F. Epstein-Barr virus-associated post-transplant lymphoproliferative disease. Recent. Results Cancer Res. 2021, 217, 197–207. [Google Scholar]
- Kaden, J.; Petersen, S.; Kaden, K.; May, G. Epstein-Barr virus infection after kidney transplantation. Transpl. Int. 1998, 11 (Suppl. S1), S119–S124. [Google Scholar] [CrossRef]
- Sprangers, B.; Riella, L.V.; Dierickx, D. Posttransplant lymphoproliferative disorder following kidney transplantation: A review. Am. J. Kidney Dis. 2021, 78, 272–281. [Google Scholar] [CrossRef]
- Pluss, M.; Mese, K.; Kowallick, J.T.; Schuster, A.; Tampe, D.; Tampe, B. Case report: Cytomegalovirus reactivation and pericarditis following ChAdOx1 nCov-19 vaccination against SARS-CoV-2. Front. Immunol. 2022, 12, 784145. [Google Scholar] [CrossRef]
- Psichogiou, M.; Samarkos, M.; Mikos, N.; Hatzakis, A. Reactivation of varicella zoster virus after vaccination for SARS-CoV-2. Vaccines 2021, 9, 572. [Google Scholar] [CrossRef]
- Maldonado, M.D.; Romero-Aibar, J. The Pfizer-BNT162b2 mRNA-based vaccine against SARS-CoV-2 may be responsible for awakening the latency of herpes varicella-zoster virus. Brain Behav. Immun. Health 2021, 18, 100381. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.-R.; Hsu, C.-W.; Lee, C.-C.; Huang, W.-L.; Lin, C.-Y.; Hsu, Y.-T.; Chang, C.; Tsai, M.-T.; Hu, Y.-N.; Hsu, C.-H.; et al. A case report of posttransplant lymphoproliferative disorder after AstraZeneca coronavirus disease 2019 vaccine in a heart transplant recipient. Transplant. Proc. 2021, 8, 3347–3352. [Google Scholar] [CrossRef] [PubMed]
- Paolucci, S.; Cassaniti, I.; Novazzi, F.; Fiorina, L.; Piralla, A.; Comolli, G.; Bruno, R.; Maserati, R.; Gulminetti, R.; Novati, S.; et al. EBV DNA increase in COVID-19 patients with impaired lymphocyte subpopulation count. Int. J. Infect. Dis. 2021, 104, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Simonnet, A.; Engelmann, I.; Moreau, A.-S.; Garcia, B.; Six, S.; El Kalioubie, A.; Robriquet, L.; Hober, D.; Jourdain, M. High incidence of Epstein-Barr virus, cytomegalovirus, and human-herpes virus-6 reactivations in critically ill patients with COVID-19. Infect. Dis. Now 2021, 51, 296–299. [Google Scholar] [CrossRef]
- Chen, T.; Song, J.; Liu, H.; Zheng, H.; Chen, C. Positive Epstein-Barr virus detection in coronavirus disease 2019 (COVID-19) patients. Sci. Rep. 2021, 11, 10902. [Google Scholar] [CrossRef]
- Sausen, D.G.; Bhutta, M.S.; Gallo, E.S.; Dahari, H.; Borenstein, R. Stress-induced Epstein-Barr virus reactivation. Biomolecules 2021, 11, 1380. [Google Scholar] [CrossRef]
- Rodríguez-Jiménez, P.; Chicharro, P.; Cabrera, L.M.; Seguí, M.; Morales-Caballero, Á.; Llamas-Velasco, M.; Sánchez-Pérez, J. Varicella-zoster virus reactivation after SARS-CoV-2 BNT162b2 mRNA vaccination: Report of 5 cases. JAAD Case Rep. 2021, 12, 58–59. [Google Scholar] [CrossRef]
- Gringeri, M.; Battini, V.; Cammarata, G.; Mosini, G.; Guarnieri, G.; Leoni, C.; Pozzi, M.; Radice, S.; Clementi, E.; Carnovale, C. Herpes zoster and simplex reactivation following COVID-19 vaccination: New insights from a vaccine adverse event reporting system (VAERS) database analysis. Expert Rev. Vaccines 2022, 21, 675–684. [Google Scholar] [CrossRef]
- Alkwikbi, H.; Alenazi, M.; Alanazi, W.; Alruwaili, S. Herpetic keratitis and corneal endothelitis following COVID-19 vaccination: A case series. Cureus 2022, 14, e20967. [Google Scholar] [CrossRef]
- Brosh-Nissimov, T.; Sorek, N.; Yeshayahu, M.; Zherebovich, I.; Elmaliach, M.; Cahan, A.; Amit, S.; Rotlevi, E. Oropharyngeal shedding of herpesviruses before and after BNT162b2 mRNA vaccination against COVID-19. Vaccine 2021, 39, 5729–5731. [Google Scholar] [CrossRef]
- Dong, S.W.; Blair, B.M.; Alonso, C.D. Epidemiology and outcomes of Epstein-Barr virus DNAemia in adult solid organ transplant recipients (abstract 934). Open Forum Infect Dis. 2021, 8 (Suppl. S1), S559–S560. [Google Scholar] [CrossRef]
- Holman, C.J.; Krger, A.B.; Mullan, B.D.; Brundage, R.C.; Balfou, H.H., Jr. Quantitative Epstein-Barr virus shedding nand its correlation with the risk of post-transplant lymphoproliferative disease. Clin. Transplant. 2012, 26, 741–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rowe, D.T.; Webber, S.; Schauer, E.M.; Reyes, J.; Green, M. Epstein-Barr virus load monitoring: Its role in the prevention and management of post-transplant lymphoproliferative disease. Transpl. Infect. Dis. 2001, 3, 79–87. [Google Scholar] [CrossRef]
- Franceschini, E.; Plessi, J.; Zona, S.; Santoro, A.; Digaetano, M.; Fontana, F.; Alfano, G.; Guaraldi, G.; Comoli, P.; Facchini, F.; et al. Clinical utility of Epstein-Barr virus viral load monitoring and risk factors for posttransplant lymphoproliferative disorders after kidney transplantation: A single center, 10-yr observational cohort study. Transplant. Direct 2017, 3, e182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yong, S.J. Long COVID or post-COVID syndrome: Putative pathophysiology, risk factors, and treatment. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef]
- Gold, J.E.; Okyay, R.A.; Licht, W.E.; Hurley, D.J. Investigation of long COVID prevalence and its relationship to Epstein-Barr virus reactivation. Pathogens 2021, 10, 763. [Google Scholar] [CrossRef] [PubMed]
- Walter, R.; Hartmann, K.; Fleisch, F.; Reinhart, W.H.; Kuhn, M. Reactivation of herpesvirus infections after vaccinations? Lancet 1999, 353, 810. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Musialik, J.; Kolonko, A.; Więcek, A. Increased EBV DNAemia after Anti-SARS-CoV-2 Vaccination in Solid Organ Transplants. Vaccines 2022, 10, 992. https://doi.org/10.3390/vaccines10070992
Musialik J, Kolonko A, Więcek A. Increased EBV DNAemia after Anti-SARS-CoV-2 Vaccination in Solid Organ Transplants. Vaccines. 2022; 10(7):992. https://doi.org/10.3390/vaccines10070992
Chicago/Turabian StyleMusialik, Joanna, Aureliusz Kolonko, and Andrzej Więcek. 2022. "Increased EBV DNAemia after Anti-SARS-CoV-2 Vaccination in Solid Organ Transplants" Vaccines 10, no. 7: 992. https://doi.org/10.3390/vaccines10070992
APA StyleMusialik, J., Kolonko, A., & Więcek, A. (2022). Increased EBV DNAemia after Anti-SARS-CoV-2 Vaccination in Solid Organ Transplants. Vaccines, 10(7), 992. https://doi.org/10.3390/vaccines10070992