
Cost-Effectiveness of Influenza Vaccination Strategies in Adults: Older Adults Aged ≥65 Years, Adults Aged 50–64 Years, and At-Risk Adults Aged 19–64 Years

 , , , , , , and
, , , , , , and
Abstract
1. Introduction
2. Methods
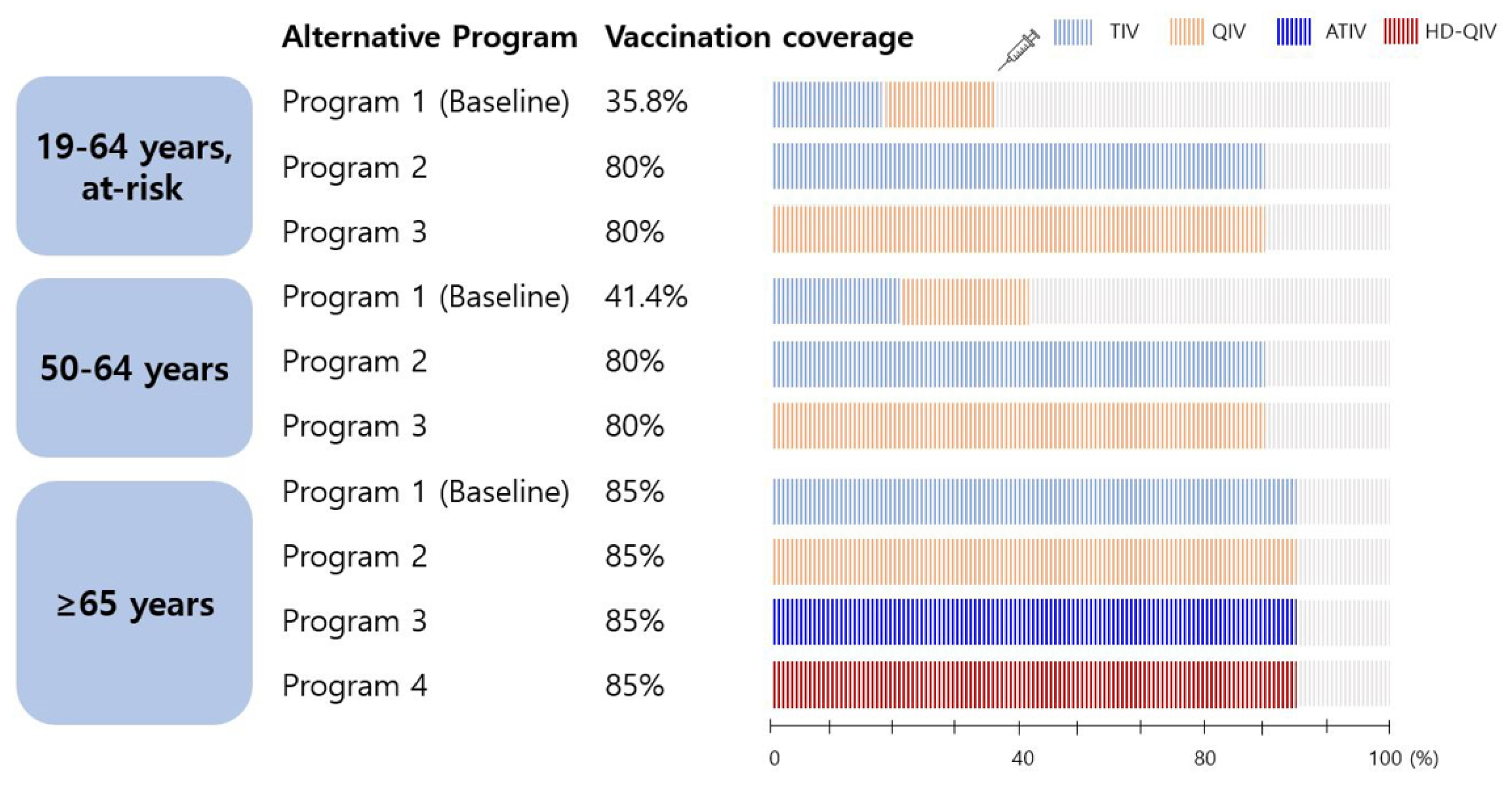
2.1. Vaccination Programs Evaluated
2.1.1. Older Adults Aged ≥65 Years
- -
- Program 1 (baseline): all older adults received the trivalent influenza vaccine (TIV) according to the current Korean NIP.
- -
- Programs 2, 3, and 4: assume the introduction of a quadrivalent influenza vaccine (QIV), adjuvanted trivalent vaccine (ATIV), or high-dose QIV (HD-QIV) to the NIP instead of the TIV, and target a vaccination rate of 85%.
2.1.2. Adults Aged 50–64 Years and at-Risk Adults Aged 19–64 Years
- -
- Program 1 (baseline): individuals receiving influenza vaccination with out-of-pocket expenses (TIV or QIV).
- -
- Programs 2 and 3: assume the introduction of a TIV and QIV, respectively, into the NIP with a target vaccination rate of 80%.
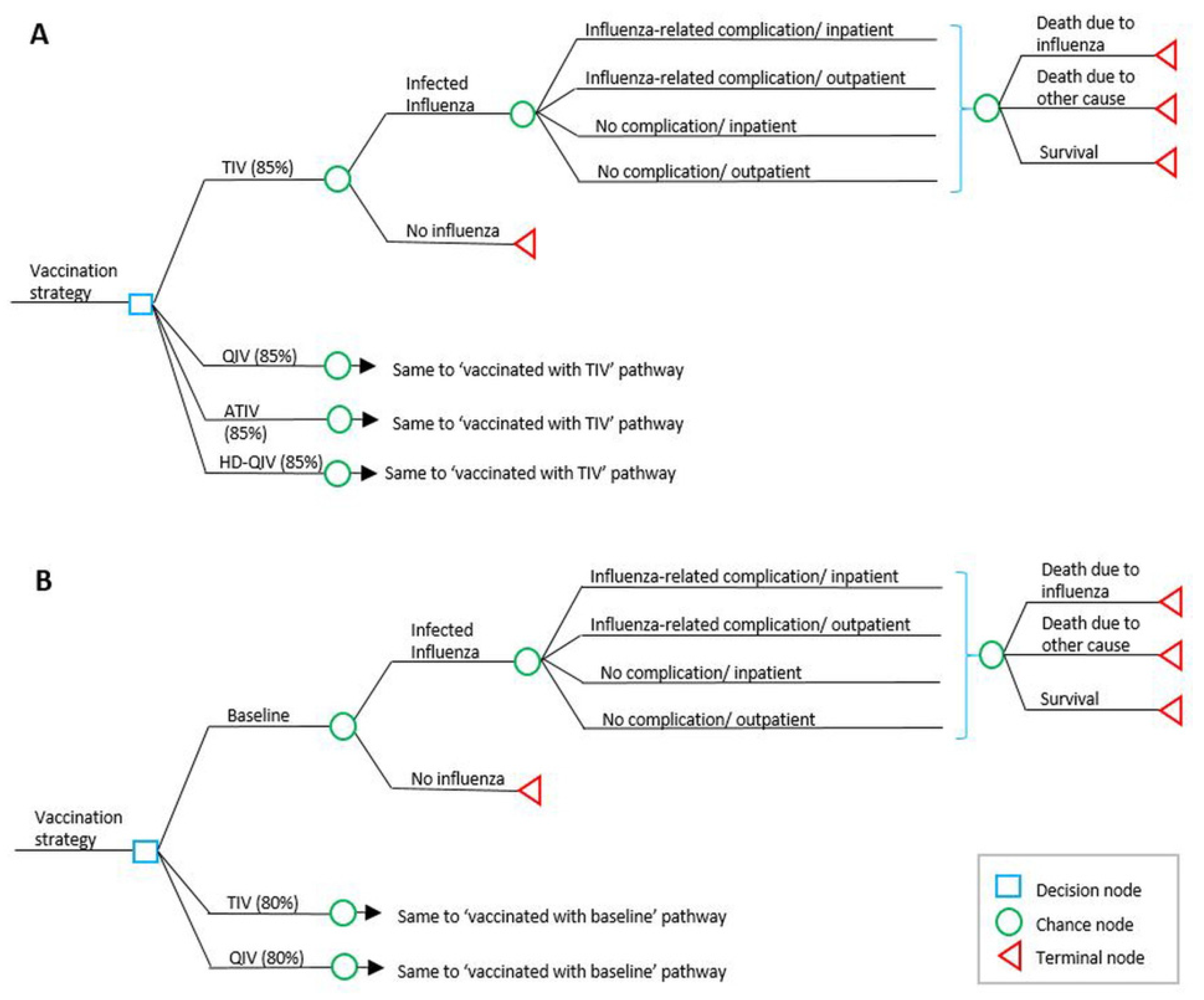
2.2. Model Design and Structure
2.3. Input Data
2.3.1. Population Data
2.3.2. Disease Burden (Probability and Vaccine Data)
2.3.3. Cost Data
2.3.4. Influenza Type or Subtype Circulation Data
2.3.5. Utility Data
2.3.6. Vaccine Characteristics (Efficacy and Cost of Vaccines)
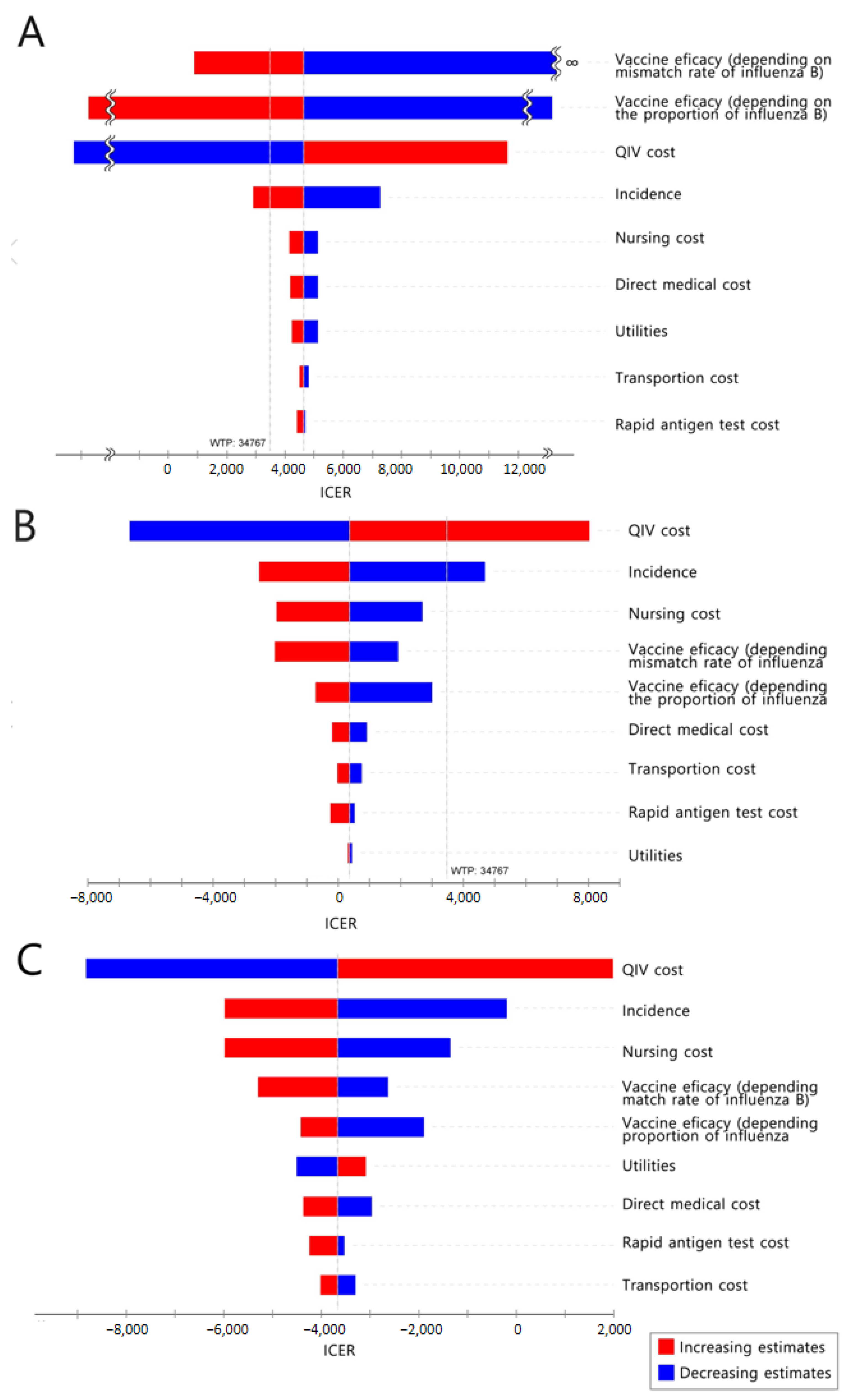
2.4. Sensitivity Analysis
2.5. Consideration of Herd Effect
3. Results
3.1. Older Adults Aged ≥65 Years
3.1.1. Base Case Analysis
3.1.2. Sensitivity Analysis
3.2. Adults Aged 50–64 Years
3.2.1. Base Case Analysis
3.2.2. Sensitivity Analysis
3.3. At-risk Adults Aged 19–64 Years
3.3.1. Base Case Analysis
3.3.2. Sensitivity Analysis
4. Discussion
- 1.
- An “age-based” strategy might be a more efficient option considering the wide range of comorbidities, uncertainty of diagnosis, and implementation issues with influenza vaccine administration within a short period (1–2 months).
- 2.
- The cost of the government’s investment in the vaccine program ranged from $242 million (TIV 80%) to $297 million (QIV 80%) for 50–64-year-old adults and from $114 million (TIV 80%) to $140 million (QIV 80%) for at-risk 19–64-year-old adults. Therefore, the total cost to be invested is expected to be lower for the at-risk adult group than for the 50-to-64-year-old group, but implementation issues should be considered.
- 3.
- From a societal perspective, introducing the influenza vaccine into the NIP (TIV or QIV) appears to be a cost-effective or even cost-saving strategy for both adult age groups. However, after excluding productivity loss, the ICER of introducing QIV into the NIP was $86,463/QALY for 50–64-year-old adults and $53,050/QALY for at-risk 19–64-year-old adults, which is no longer cost-effective for both groups with respect to GDP per capita. Considering that the ICER of at-risk 19–64-year-old adults was lower than that of the comparison group, it might be appropriate to expand the immunization program to the at-risk population first. Of course, it would be difficult to directly determine the dominance between the target groups with an ICER only derived from different analyses; however, it might be meaningful because the analytic results were derived from the same data source and analytic methods.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Influenza (Seasonal). Available online: https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal (accessed on 28 March 2020).
- Putri, W.C.W.S.; Muscatello, D.J.; Stockwell, M.S.; Newall, A.T. Economic burden of seasonal influenza in the United States. Vaccine 2018, 36, 3960–3966. [Google Scholar] [CrossRef]
- Grohskopf, L.A.; Alyanak, E.; Broder, K.R.; Blanton, L.H.; Fry, A.M.; Jernigan, D.B.; Atmar, R.L. Prevention and control of seasonal influenza with vaccines: Recommendations of the Advisory Committee on Immunization Practices—United States, 2020–2021 influenza season. M.M.W.R. Recomm. Rep. 2020, 69, 1–24. [Google Scholar] [CrossRef]
- Public Health England. Annual Flu Programme. Available online: https://www.gov.uk/government/collections/annual-flu-programme (accessed on 28 March 2021).
- Centre for Health Protection. Government Vaccination Program 2020/2021. Eligible Groups for Free Seasonal Influenza Vaccination. Available online: https://www.chp.gov.hk/files/pdf/eligible_groups_202021_siv_en.pdf (accessed on 28 March 2021).
- ECDC. Influenza: Recommended Vaccinations. Available online: https://vaccine-schedule.ecdc.europa.eu/Scheduler/ByDisease?SelectedDiseaseId=15&SelectedCountryIdByDisease=-1 (accessed on 28 March 2021).
- Taiwan Centers for Disease Control [Press Release], 3 October 2016. Available online: https://www.cdc.gov.tw/En/Bulletin/Detail/xBgOvV41MbSoq0YxkG3ezQ?typeid=158 (accessed on 28 March 2021).
- Korea Disease Control and Prevention Agency. Influenza National Immunization Program Management Guideline. Available online: https://nip.cdc.go.kr/irgd/reference.do?MnLv1=2 (accessed on 28 March 2021).
- Park, M.; Wu, P.; Goldstein, E.; Joo Kim, W.J.; Cowling, B.J. Influenza-associated excess mortality in South Korea. Am. J. Prev. Med. 2016, 50, e111–e119. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, K.; Viboud, C.; Simonsen, L. Antibody response to influenza vaccination in the elderly: A quantitative review. Vaccine 2006, 24, 1159–1169. [Google Scholar] [CrossRef] [PubMed]
- DiazGranados, C.A.; Dunning, A.J.; Kimmel, M.; Kirby, D.; Treanor, J.; Collins, A.; Pollak, R.; Christoff, J.; Earl, J.; Landolfi, V.; et al. Efficacy of high-dose versus standard-dose influenza vaccine in older adults. N. Engl. J. Med. 2014, 371, 635–645. [Google Scholar] [CrossRef]
- Wilkinson, K.; Wei, Y.; Szwajcer, A.; Rabbani, R.; Zarychanski, R.; Abou-Setta, A.M.; Mahmud, S.M. Efficacy and safety of high-dose influenza vaccine in elderly adults: A systematic review and meta-analysis. Vaccine 2017, 35, 2775–2780. [Google Scholar] [CrossRef]
- Mannino, S.; Villa, M.; Apolone, G.; Weiss, N.S.; Groth, N.; Aquino, I.; Boldori, L.; Caramaschi, F.; Gattinoni, A.; Malchiodi, G.; et al. Effectiveness of adjuvanted influenza vaccination in elderly subjects in northern Italy. Am. J. Epidemiol. 2012, 176, 527–533. [Google Scholar] [CrossRef]
- McConeghy, K.W.; Davidson, H.E.; Canaday, D.H.; Han, L.; Saade, E.; Mor, V.; Gravenstein, S. Cluster-randomized trial of adjuvanted versus nonadjuvanted trivalent influenza vaccine in 823 US nursing home. Clin. Infect. Dis. 2021, 73, 4237–4243. [Google Scholar] [CrossRef]
- Pelton, S.I.; Divino, V.; Shah, D.; Mould-Quevedo, J.; DeKoven, M.; Krishnarajah, G.; Postma, M.J. Evaluating the relative vaccine effectiveness of adjuvanted trivalent influenza vaccine compared to high-dose trivalent and other egg-based influenza vaccine among older adults in the US during the 2017–2018 influenza season. Vaccines 2020, 8, 446. [Google Scholar] [CrossRef]
- Doyle, J.D.; Beacham, L.; Martin, E.T.; Talbot, H.K.; Monto, A.; Gaglani, M.; Middleton, D.B.; Silveira, F.P.; Zimmerman, R.K.; Alyanak, E.; et al. Relative and absolute effectiveness of high-dose and standard-dose influenza vaccine against influenze-related hospitalization among older adults-United States, 2015–2017. Clin. Infect. Dis. 2021, 72, 995–1003. [Google Scholar] [CrossRef]
- Byeon, G.R.; Hur, Y.I.; Kang, J.H.; Park, H.A.; Kim, K.W.; Cho, Y.G.; Shin, K.; Kang, B. Influenza vaccination status in Korean adult population in relation with socioeconomic and medical factors. Korean J. Health Promot. 2016, 16, 20–31. [Google Scholar] [CrossRef]
- Korean Statistical Information Service. Available online: https://kosis.kr (accessed on 28 March 2021).
- Byeon, K.H.; Kim, J.; Choi, B.; Choi, B.Y. The coverage rates for influenza vaccination and related factors in Korean adults aged 50 and older with chronic disease: Based on 2016 Community Health Survey data. Epidemiol. Health 2018, 40, e2018034. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.J.; Bae, E.Y.; Kang, E.J.; Bae, S.J.; Ahn, H.G.; Jo, M.W.; Han, S.K.; Hong, J.H.; Lee, Y.S. Guideline for Economic Evaluation of Pharmaceuticals in Korea. Available online: http://www.hira.or.kr/rc/icenter/study/getReportInfo.do?pgmid=HIRAA030095000000 (accessed on 4 April 2021).
- Kim, L.Y. Health Insurance Review and Assessment Service National Patient Samples (HIRA-NPS). Available online: https://repository.hira.or.kr/bitstream/2019.oak/894/2/%EA%B1%B4%EA%B0%95%EB%B3%B4%ED%97%98%EC%8B%AC%EC%82%AC%ED%8F%89%EA%B0%80%EC%9B%90%20%ED%99%98%EC%9E%90%ED%91%9C%EB%B3%B8%EC%9E%90%EB%A3%8C(HIRA-NPS)%EC%9D%98%20%EC%86%8C%EA%B0%9C.pdf (accessed on 10 October 2021).
- Korea Disease Control and Prevention Agency. Adult Immunization Guide 2018. Available online: https://www.cdc.go.kr/board/board.es?mid=a20507020000&bid=0019 (accessed on 4 April 2021).
- Yun, J.W.; Choi, M.J.; Shin, G.S.; Lim, J.O.; Noh, J.Y.; Kim, Y.K.; Song, J.Y.; Kim, W.J.; Choi, S.E.; Cheong, H.J. Cost-effectiveness of influenza vaccine strategies for the elderly in South Korea. PLoS ONE 2019, 14, e0209643. [Google Scholar] [CrossRef] [PubMed]
- Korean Ministry of Health and Welfare. Korea Health Statistics 2014: Korean National Health and Nutrition Examination Survey (KNHANES VI-2) [Research Report]; Korea Centers for Disease Control & Prevention (KCDC): Cheongju, Korea, 2015. [Google Scholar]
- Korea Disease Control and Prevention Agency. Infectious Disease Portal. Laboratory Newsletter. Available online: http://www.kdca.go.kr/npt/biz/npp/portal/nppPblctDtaMain.do (accessed on 4 April 2021).
- Korea Institute for Health and Social Affairs. Korea Health Panel Survey of 2017. Available online: https://www.khp.re.kr:444/web/research/board/view.do?bbsid=13&seq=2251 (accessed on 19 April 2021).
- Ministry of Employment and Labor. Employment and Labor Statistics. Available online: http://laborstat.moel.go.kr/ (accessed on 18 August 2021).
- Centers for Medicare & Medicaid Services. Seasonal Influenza Vaccine Pricing. Available online: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Part-B-Drugs/McrPartBDrugAvgSalesPrice/VaccinesPricing (accessed on 18 August 2021).
- Korean Society of Infectious Disease. Vaccinations for Adults, 3rd ed.; Koonja Publishing: Paju, Korea, 2019. [Google Scholar]
- Demicheli, V.; Jefferson, T.; Ferroni, E.; Rivetti, A.; Di Pietrantonj, C. Vaccines for preventing influenza in healthy adults. Cochrane Database Syst. Rev. 2018, 2, CD001269. [Google Scholar] [CrossRef] [PubMed]
- Demicheli, V.; Jefferson, T.; Di Pietrantonj, C.; Ferroni, E.; Thorning, S.; Thomas, R.E.; Rivetti, A. Vaccines for preventing influenza in the elderly. Cochrane Database Syst. Rev. 2018, 2, CD004876. [Google Scholar] [CrossRef]
- Capri, S.; Barbieri, M.; De Waure, C.; Boccalini, S.; Panatto, D. Cost-effectiveness analysis of different seasonal influenza vaccines in the elderly Italian population. Hum. Vaccin Immunother 2018, 14, 1331–1341. [Google Scholar] [CrossRef]
- Tricco, A.C.; Chit, A.; Soobiah, C.; Hallett, D.; Meier, G.; Chen, M.H.; Tashkandi, M.; Bauch, C.T.; Loeb, M. Comparing influenza vaccine efficacy against mismatched and matched strains: A systematic review and meta-analysis. BMC Med. 2013, 11, 153. [Google Scholar] [CrossRef]
- DiazGranados, C.A.; Denis, M.; Plotkin, S. Seasonal influenza vaccine efficacy and its determinants in children and non-elderly adults: A systematic review with meta-analyses of controlled trials. Vaccine 2012, 31, 49–57. [Google Scholar] [CrossRef]
- Blommaert, A.; Bilcke, J.; Vandendijck, Y.; Hanquet, G.; Hens, N.; Beutels, P. Cost-effectiveness of seasonal influenza vaccination in pregnant women, health care workers and persons with underlying illnesses in Belgium. Vaccine 2014, 32, 6075–6083. [Google Scholar] [CrossRef]
- Englund, H.; Campe, H.; Hautmann, W. Effectiveness of trivalent and monovalent influenza vaccines against laboratory-confirmed influenza infection in persons with medically attended influenza-like illness in Bavaria, Germany, 2010/2011 Season. Epidemiol. Infect. 2013, 141, 1807–1815. [Google Scholar] [CrossRef]
- Hutubessy, R.; Chisholm, D.; Edejer, T.T.-T. Generalized cost-effectiveness analysis for national-level priority-setting in the health sector. Cost Eff. Resour. Alloc. 2003, 1, 8. [Google Scholar] [CrossRef] [PubMed]
- Bauch, C.T.; Anonychuk, A.M.; Van Effelterre, T.; Pham, B.Z.; Merid, M.F. Incorporating herd immunity effects into cohort models of vaccine cost-effectiveness. Med. Decis. Making 2009, 29, 557–569. [Google Scholar] [CrossRef] [PubMed]
- Van Vlaenderen, I.; Van Bellinghen, L.A.; Meier, G.; Nautrup, B.P. An approximation of herd effect due to vaccinating children against seasonal influenza–a potential solution to the incorporation of indirect effects into static models. BMC Infect. Dis. 2013, 13, 25. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.G. Immunization Rates of Vaccines Not Supported by the Nation (Influenza, Rotavirus) and Affecting Factors. KDCA. 2019. Available online: https://nip.kdca.go.kr/irgd/index.html (accessed on 25 April 2021).
- Cheong, H.J. Cost-Effectiveness Analysis of Extension of Influenza Immunization Program. KDCA. 2020. Available online: http://27.101.205.56/homepage/entire/retrieveEntireDetail.do?pageIndex=1&research_id=1351000-201800432&leftMenuLevel=160&cond_research_name=%EC%9D%B8%ED%94%8C%EB%A3%A8%EC%97%94%EC%9E%90&cond_research_start_date=&pageUnit=10&cond_order=3 (accessed on 25 April 2021).
- Ali, S.T.; Cowling, B.J.; Lau, E.H.Y.; Fang, V.J.; Leung, G.M. Mitigation of influenza B epidemic with school closures, Hong Kong, 2018. Emerg. Infect. Dis. 2018, 24, 2071–2073. [Google Scholar] [CrossRef]
- Avritscher, E.B.; Cooksley, C.D.; Geraci, J.M.; Bekele, B.N.; Cantor, S.B.; Rolston, K.V.; Elting, L.S. Cost-effectiveness of influenza vaccination in working-age cancer patients. Cancer 2007, 109, 2357–2364. [Google Scholar] [CrossRef]
- Meier, G.; Gregg, M.; Poulsen Nautrup, B. Cost-effectiveness analysis of quadrivalent influenza vaccination in at-risk adults and the elderly: An updated analysis in the U. K. J. Med. Econ. 2015, 18, 746–761. [Google Scholar] [CrossRef]
- Raviotta, J.M.; Smith, K.J.; DePasse, J.; Brown, S.T.; Shim, E.; Nowalk, M.P.; Zimmerman, R.K. Cost-effectiveness and public health effect of influenza vaccine strategies for US elderly adults. J. Am. Geriatr. Soc. 2016, 64, 2126–2131. [Google Scholar] [CrossRef]
- García, A.; Ortiz de Lejarazu, R.; Reina, J.; Callejo, D.; Cuervo, J.; Morano Larragueta, R. Cost–effectiveness analysis of quadrivalent influenza vaccine in Spain. Hum. Vaccin Immunother. 2016, 12, 2269–2277. [Google Scholar] [CrossRef]
- Hong, K.W.; Cheong, H.J.; Choi, W.S.; Lee, J.; Wie, S.H.; Baek, J.H.; Kim, H.Y.; Jeong, H.W.; Kim, W.J. Clinical courses and outcomes of hospitalized adult patients with seasonal influenza in Korea, 2011–2012: Hospital-based influenza morbidity & mortality (HIMM) surveillance. J. Infect. Chemother. 2014, 20, 9–14. [Google Scholar] [CrossRef]
- Kim, Y.K.; Song, J.Y.; Jang, H.; Kim, T.H.; Koo, H.; Varghese, L.; Han, E. Cost effectiveness of quadrivalent influenza vaccines compared with trivalent influenza vaccines in young children and older adults in Korea. Pharmacoeconomics 2018, 36, 1475–1490. [Google Scholar] [CrossRef]
- Turner, D.A.; Wailoo, A.J.; Cooper, N.J.; Sutton, A.J.; Abrams, K.R.; Nicholson, K.G. The cost-effectiveness of influenza vaccination of healthy adults 50-64 years of age. Vaccines 2006, 24, 1035–1043. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Target Groups | Reference | ||
|---|---|---|---|---|
| 19–64 Years, At-Risk | 50–64 Years | ≥65 Years | ||
| Population | 5,636,765 | 11,998,063 | 7,455,149 | [18], assumption |
| Probability of disease burden | Extracted from NHIS database | |||
| Influenza case | 0.0549 | 0.0454 | 0.0531 | |
| Complication/Influenza case | 0.0675 | 0.0515 | 0.1417 | |
| Hospitalization/Influenza case | 0.0638 | 0.0553 | 0.1046 | |
| Death/Influenza case | 0.000349% | 0.000232 | 0.005740 | |
| Costs (USD) * | ||||
| Vaccination | ||||
| TIV | 25.22 | 25.22 | 22.86 | Government data |
| QIV | 30.95 | 30.95 | 28.24 | Assumption |
| ATIV | - | - | 30.55 (26.70–38.25) | Assumption |
| HD-QIV | - | - | ||
| Out-of-pocket a | 31.36 | 31.36 | - | Assumption |
| Direct medical cost | ||||
| Uncomplicated outpatient | 61.01 | 59.90 | 60.69 | Extracted from NHIS database |
| Complicated outpatient | 129.04 | 118.78 | 119.60 | |
| Uncomplicated hospitalization | 934.17 | 870.72 | 1361.41 | |
| Complicated hospitalization | 1948.93 | 1700.13 | 2278.45 | |
| Direct non-medical cost | ||||
| Nursing cost | 41.90 | 41.90 | 51.18 | |
| Transportation cost | 21.64 per episode | |||
| Length of stay (or number of visits) | ||||
| Uncomplicated outpatient | 3.59 | 3.66 | 3.69 | Extracted from NHIS database |
| Complicated outpatient | 4.96 | 5.12 | 4.36 | |
| Uncomplicated hospitalization | 7.66 | 7.74 | 8.60 | |
| Complicated hospitalization | 11.34 | 11.00 | 12.42 | |
| Utility | [18,23,24] | |||
| Baseline utility | 0.819 | 0.938 | 0.867 | |
| Uncomplicated outpatient | −0.35 | −0.35 | −0.35 | |
| Complicated outpatient | −0.4 | −0.4 | −0.4 | |
| Uncomplicated hospitalization | −0.4 | −0.4 | −0.4 | |
| Complicated hospitalization | −0.5 | −0.5 | −0.5 | |
| Target Groups | |||||
|---|---|---|---|---|---|
| At-Risk | 50–64 Years | ≥65 Years | |||
| 19–49 Years | 50–64 Years | ||||
| Vaccine efficacy | TIV | 59% | 59% | 59% | 58% |
| QIV | 64.2% (59–70.3%) | 64.2% (59–70.3%) | 64.2% (59–70.3%) | 63.2% (58–69.3%) | |
| ATIV | 66.4% (62.2–74.8%) | ||||
| HD-QIV | 72.0% (68.1–76.7%) | ||||
| Vaccination coverage rates | 35.8% | 35.8% | 41.4% | 84.3% | |
| ≥65 Years | |||||
|---|---|---|---|---|---|
| TIV (85%) | QIV (85%) | ATIV (85%) | HD-QIV (85%) | ||
| Number of | Vaccinated | 6,336,877 | 6,336,877 | 6,336,877 | 6,336,877 |
| Influenza cases | 392,724 | 358,486 | 300,546 | 337,417 | |
| Complications | 55,649 | 50,797 | 42,587 | 47,812 | |
| Hospitalizations | 41,079 | 37,498 | 31,437 | 35,294 | |
| Deaths | 2254 | 2058 | 1725 | 1937 | |
| Total life-year (QALY) | 6,457,913 | 6,458,238 | 6,458,437 | 6,458,786 | |
| Total cost (USD) | 363,530,403 | 378,601,928 | 381,051,836 | 360,969,390 | |
| 50–64 years | |||||
| Current | TIV (80%) | QIV (80%) | |||
| Number of | Vaccinated | 4,967,198 | 9,598,450 | 9,598,450 | |
| Influenza cases | 544,712 | 380,565 | 350,581 | ||
| Complications | 28,053 | 19,599 | 18,055 | ||
| Hospitalizations | 30,123 | 21,045 | 19,387 | ||
| Deaths | 126 | 88 | 81 | ||
| Total life-year (QALY) | 11,251,489 | 11,252,146 | 11,252,271 | ||
| Total cost (USD), societal perspective | 554,543,223 | 524,733,031 | 557,407,544 | ||
| Total cost (USD), healthcare sector perspective | 367,995,027 | 392,517,433 | 435,608,932 | ||
| 19–64 years, at-risk | |||||
| Current | TIV (80%) | QIV (80%) | |||
| Number of | Vaccinated | 2,017,962 | 4,509,412 | 4,509,412 | |
| Influenza cases | 309,564 | 207,218 | 190,892 | ||
| Complications | 20,896 | 13,987 | 12,885 | ||
| Hospitalizations | 19,750 | 13,221 | 12,179 | ||
| Deaths | 108 | 72 | 67 | ||
| Total life-year (QALY) | 3,982,199 | 3,982,569 | 3,982,630 | ||
| Total cost (USD), societal perspective | 306,667,009 | 278,606,389 | 288,380,562 | ||
| Total cost (USD), healthcare sector perspective | 189,104,801 | 198,971,911 | 215,629,718 | ||
| Cost (USD) | Incremental Cost (ΔUSD) | Effectiveness (QALY) | Incremental Effectiveness (ΔQALY) | ICER (ΔUSD/ QALY) | ||
|---|---|---|---|---|---|---|
| ≥65 years | TIV | 363,530,403 | 6,457,913 | (reference) | ||
| QIV | 378,601,928 | 15,071,525 | 6,458,238 | 324 | 46,486 | |
| ATIV | 381,501,836 | 17,971,433 | 6,458,437 | 524 | 34,314 | |
| HD-QIV | 360,969,390 | −2,561,013 | 6,458,786 | 873 | Cost-saving | |
| 50–64 years | Current | 554,543,223 | 11,251,489 | (reference) | ||
| TIV | 524,733,031 | −29,810,192 | 11,252,146 | 657 | Cost-saving | |
| QIV | 557,407,544 | 2,864,321 | 11,252,271 | 782 | 3661 | |
| 19–64 years, at–risk | Current | 306,667,009 | 4,614,862 | (reference) | ||
| TIV | 278,606,389 | −28,060,620 | 4,615,290 | 429 | Cost-saving | |
| QIV | 288,380,562 | −18,286,447 | 4,615,361 | 500 | Cost-saving | |
| From healthcare sector perspective | ||||||
| 50–64 years | Current | 367,995,027 | 11,251,489 | (reference) | ||
| TIV | 392,517,433 | 24,522,405 | 11,252,146 | 657 | 37,352 | |
| QIV | 435,608,932 | 67,613,905 | 11,252,271 | 782 | 86,463 | |
| 19–64 years, at–risk | Current | 189,104,801 | 4,614,862 | (reference) | ||
| TIV | 198,971,911 | 9,867,110 | 4,615,290 | 429 | 23,020 | |
| QIV | 215,629,718 | 26,524,917 | 4,615,361 | 500 | 53,050 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, M.J.; Shin, G.; Kang, D.; Lim, J.-O.; Kim, Y.-K.; Choi, W.S.; Yun, J.-W.; Noh, J.Y.; Song, J.Y.; Kim, W.J.; et al. Cost-Effectiveness of Influenza Vaccination Strategies in Adults: Older Adults Aged ≥65 Years, Adults Aged 50–64 Years, and At-Risk Adults Aged 19–64 Years. Vaccines 2022, 10, 445. https://doi.org/10.3390/vaccines10030445
Choi MJ, Shin G, Kang D, Lim J-O, Kim Y-K, Choi WS, Yun J-W, Noh JY, Song JY, Kim WJ, et al. Cost-Effectiveness of Influenza Vaccination Strategies in Adults: Older Adults Aged ≥65 Years, Adults Aged 50–64 Years, and At-Risk Adults Aged 19–64 Years. Vaccines. 2022; 10(3):445. https://doi.org/10.3390/vaccines10030445
Chicago/Turabian StyleChoi, Min Joo, Gyeongseon Shin, Daewon Kang, Jae-Ok Lim, Yun-Kyung Kim, Won Suk Choi, Jae-Won Yun, Ji Yun Noh, Joon Young Song, Woo Joo Kim, and et al. 2022. "Cost-Effectiveness of Influenza Vaccination Strategies in Adults: Older Adults Aged ≥65 Years, Adults Aged 50–64 Years, and At-Risk Adults Aged 19–64 Years" Vaccines 10, no. 3: 445. https://doi.org/10.3390/vaccines10030445
APA StyleChoi, M. J., Shin, G., Kang, D., Lim, J.-O., Kim, Y.-K., Choi, W. S., Yun, J.-W., Noh, J. Y., Song, J. Y., Kim, W. J., Choi, S.-E., & Cheong, H. J. (2022). Cost-Effectiveness of Influenza Vaccination Strategies in Adults: Older Adults Aged ≥65 Years, Adults Aged 50–64 Years, and At-Risk Adults Aged 19–64 Years. Vaccines, 10(3), 445. https://doi.org/10.3390/vaccines10030445