
The Effect of Antioxidant Supplementation on Operated or Non-Operated Varicocele-Associated Infertility: A Systematic Review and Meta-Analysis

 , , ,
, , ,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Acquisition and Risk of Bias
2.4. Data Synthesis and Statistical Analysis
3. Results
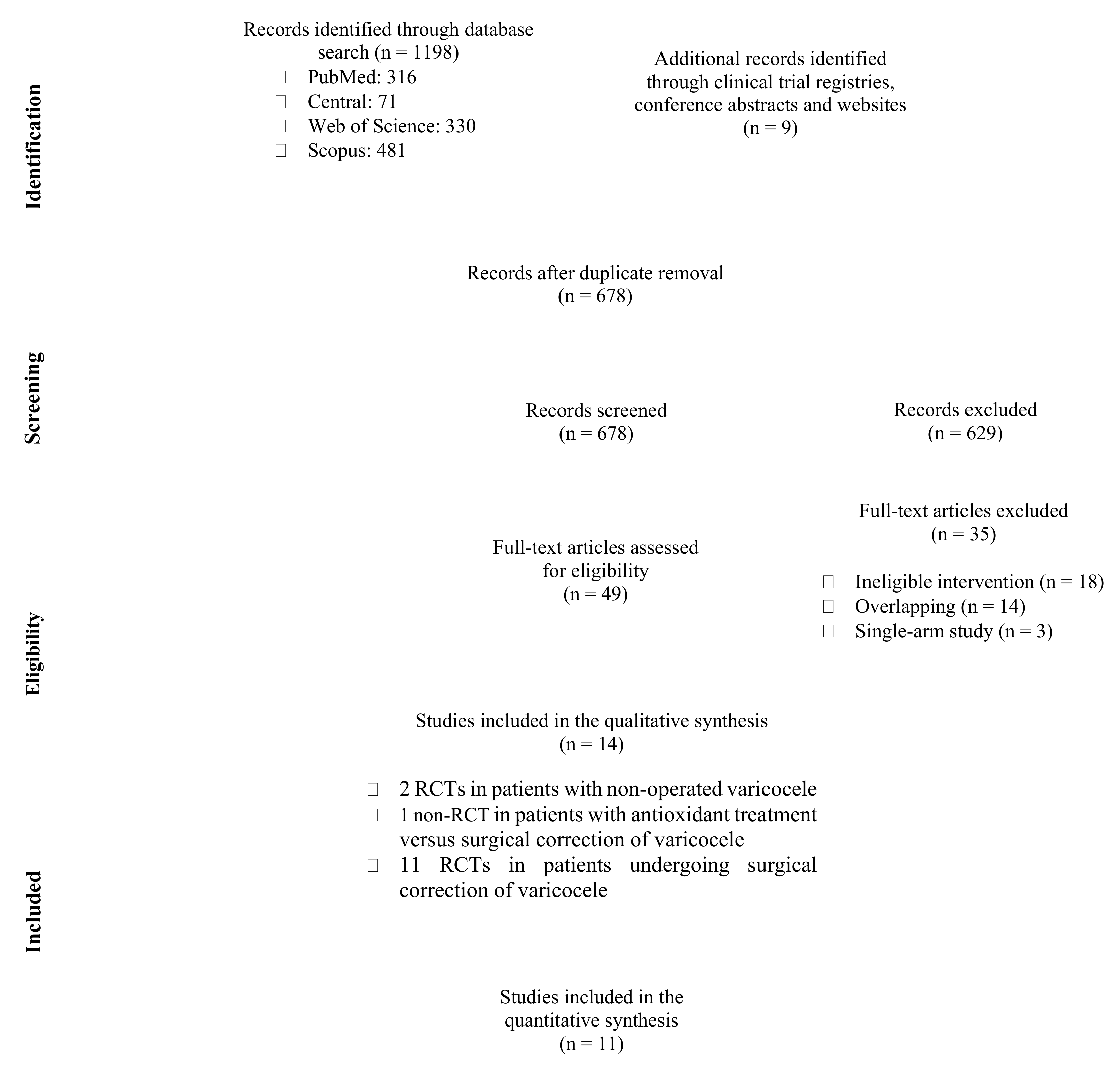
3.1. Study Selection, Study Characteristics, and Quality Assessment
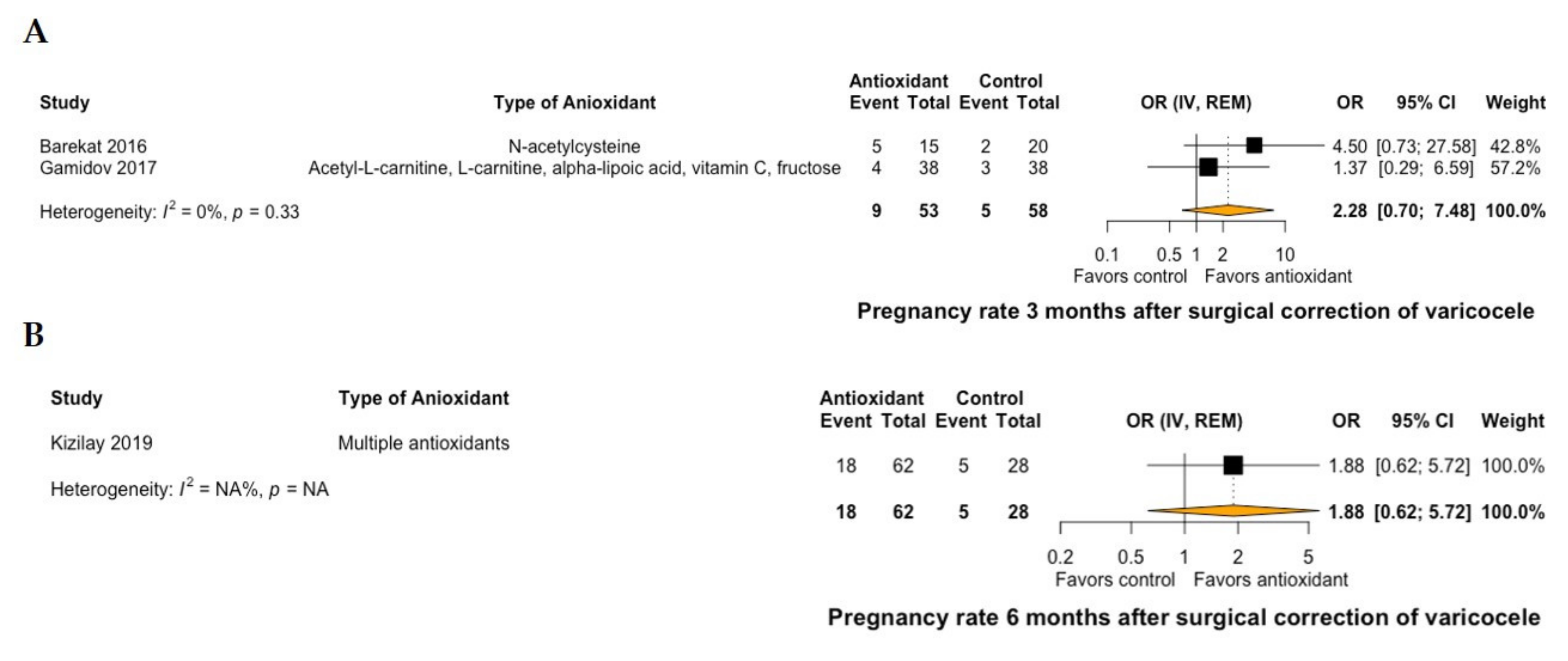
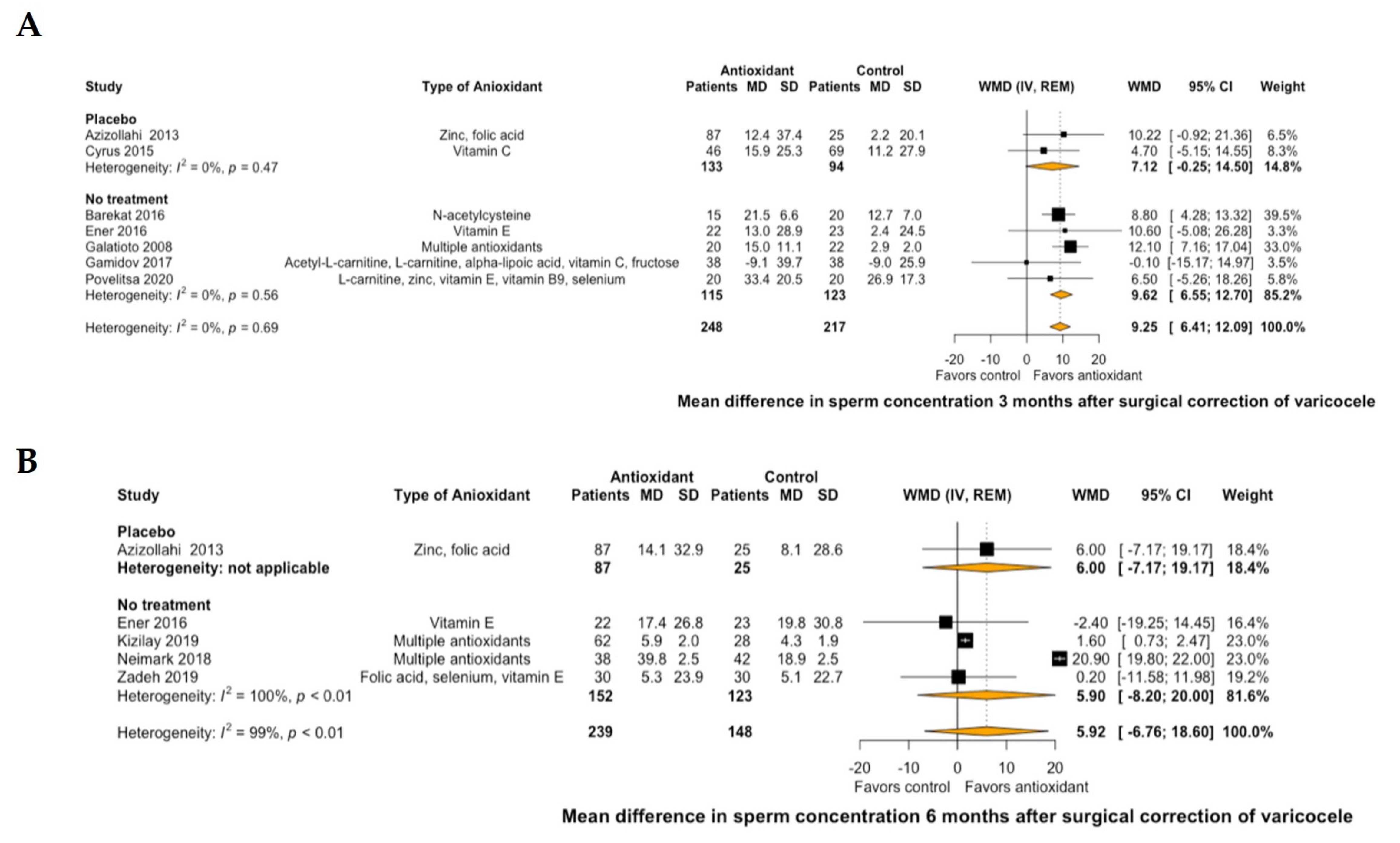
3.2. Effect of Antioxidant Treatment on Fertility in Patients Undergoing Surgical Repair of Varicocele
3.3. Effect of Antioxidant Treatment on Fertility in Patients with Non-Operated Varicocele
3.4. Antioxidant Treatment Versus Surgical Repair in Patients with Varicocele
3.5. Grading of Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Dubin, L.; Amelar, R.D. Etiologic factors in 1294 consecutive cases of male infertility. Fertil. Steril. 1971, 22, 469–474. [Google Scholar] [CrossRef]
- Damsgaard, J.; Joensen, U.N.; Carlsen, E.; Erenpreiss, J.; Jensen, M.B.; Matulevicius, V.; Zilaitiene, B.; Olesen, I.A.; Perheentupa, A.; Punab, M.; et al. Varicocele is associated with impaired semen quality and reproductive hormone levels: A study of 7035 healthy young men from six European countries. Eur. Urol. 2016, 70, 1019–1029. [Google Scholar] [CrossRef]
- Omar, M.I.; Pal, R.P.; Kelly, B.D.; Bruins, H.M.; Yuan, Y.; Diemer, T.; Krausz, C.; Tournaye, H.; Kopa, Z.; Jungwirth, A.; et al. Benefits of empiric nutritional and medical therapy for semen parameters and pregnancy and live birth rates in couples with idiopathic infertility: A systematic review and meta-analysis. Eur. Urol. 2019, 75, 615–625. [Google Scholar] [CrossRef] [Green Version]
- Sofikitis, N.; Stavrou, S.; Skouros, S.; Dimitriadis, F.; Tsounapi, P.; Takenaka, A. Mysteries, facts, and fiction in varicocele pathophysiology and treatment. Eur. Urol. Suppl. 2014, 13, 89–99. [Google Scholar] [CrossRef]
- Jensen, C.F.S.; Østergren, P.; DuPree, J.M.; Ohl, J.M.D.D.A.; Sønksen, J.; Fode, C.F.S.J.P. Varicocele and male infertility. Nat. Rev. Urol. 2017, 14, 523–533. [Google Scholar] [CrossRef]
- Ghaleno, L.R.; Alizadeh, A.; Drevet, J.R.; Shahverdi, A.; Valojerdi, M.R. Oxidation of sperm DNA and male infertility. Antioxidants 2021, 10, 97. [Google Scholar] [CrossRef] [PubMed]
- Ding, H.; Tian, J.; Du, W.; Zhang, L.; Wang, H.; Wang, Z. Open non-microsurgical, laparoscopic or open microsurgical varicocelectomy for male infertility: A meta-analysis of randomized controlled trials. BJU Int. 2012, 110, 1536–1542. [Google Scholar] [CrossRef] [PubMed]
- Amorini, A.; Listorti, I.; Bilotta, G.; Pallisco, R.; Saab, M.; Mangione, R.; Manca, B.; Lazzarino, G.; Tavazzi, B.; Lazzarino, G.; et al. Antioxidant-based therapies in male infertility: Do we have sufficient evidence supporting their effectiveness? Antioxidants 2021, 10, 220. [Google Scholar] [CrossRef]
- Gharagozloo, P.; Aitken, R.J. The role of sperm oxidative stress in male infertility and the significance of oral antioxidant therapy. Hum. Reprod. 2011, 26, 1628–1640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smits, R.M.; Mackenzie-Proctor, R.; Yazdani, A.; Stankiewicz, M.T.; Jordan, V.; Showell, M.G. Antioxidants for male subfertility. Cochrane Database Syst. Rev. 2019, 2019, CD007411. [Google Scholar] [CrossRef]
- Steiner, A.Z.; Hansen, K.R.; Barnhart, K.T.; Cedars, M.I.; Legro, R.S.; Diamond, M.P.; Krawetz, S.A.; Usadi, R.; Baker, V.L.; Coward, R.M.; et al. The effect of antioxidants on male factor infertility: The Males, antioxidants, and infertility (MOXI) randomized clinical trial. Fertil. Steril. 2020, 113, 552–560.e3. [Google Scholar] [CrossRef] [PubMed]
- Balercia, G.; Regoli, F.; Armeni, T.; Koverech, A.; Mantero, F.; Boscaro, M. Placebo-controlled double-blind randomized trial on the use of l-carnitine, l-acetylcarnitine, or combined l-carnitine and l-acetylcarnitine in men with idiopathic asthenozoospermia. Fertil. Steril. 2005, 84, 662–671. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.B.; Lawaetz, J.G.; Petersen, J.H.; Juul, A.; Jørgensen, N. Effects of vitamin D supplementation on semen quality, reproductive hormones, and live birth rate: A randomized clinical trial. J. Clin. Endocrinol. Metab. 2017, 103, 870–881. [Google Scholar] [CrossRef]
- Chen, Y.-W.; Niu, Y.-H.; Wang, D.-Q.; Li, H.; Pokhrel, G.; Xu, H.; Wang, T.; Wang, S.-G.; Liu, J.-H. Effect of adjuvant drug therapy after varicocelectomy on fertility outcome in males with varicocele-associated infertility: Systematic review and meta-analysis. Andrologia 2018, 50, e13070. [Google Scholar] [CrossRef]
- Wang, J.; Wang, T.; Ding, W.; Wu, J.; Wu, G.; Wang, Y.; Zhou, Z.; Xu, L.; Cui, Y. Efficacy of antioxidant therapy on sperm quality measurements after varicocelectomy: A systematic review and meta-analysis. Andrologia 2019, 51, e13396. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rucker, G.; Harbord, R.; Schmid, C.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busetto, G.M.; Agarwal, A.; Virmani, A.; Antonini, G.; Ragonesi, G.; Del Giudice, F.; Micic, S.; Gentile, V.; De Berardinis, E. Effect of metabolic and antioxidant supplementation on sperm parameters in oligo-astheno-teratozoospermia, with and without varicocele: A double-blind placebo-controlled study. Andrologia 2018, 50, e12927. [Google Scholar] [CrossRef] [Green Version]
- Cavallini, G.; Ferraretti, A.P.; Gianaroli, L.; Biagiotti, G.; Vitali, G. Cinnoxicam andl-carnitine/acetyl-l-carnitine treatment for idiopathic and varicocele-associated oligoasthenospermia. J. Androl. 2004, 25, 761–770. [Google Scholar] [CrossRef] [PubMed]
- Sofimajidpour, H.; Ghaderi, E.; Ganji, O. Comparison of the effects of varicocelectomy and oral L-carnitine on sperm parameters in infertile men with varicocele. J. Clin. Diagn. Res. 2016, 10, PC07–PC10. [Google Scholar] [CrossRef] [PubMed]
- Azizollahi, G.; Azizollahi, S.; Babaei, H.; Kianinejad, M.; Baneshi, M.R.; Nematollahi-Mahani, S.N. Effects of supplement therapy on sperm parameters, protamine content and acrosomal integrity of varicocelectomized subjects. J. Assist. Reprod. Genet. 2013, 30, 593–599. [Google Scholar] [CrossRef]
- Barekat, F.; Tavalaee, M.; Deemeh, M.R.; Bahreinian, M.; Azadi, L.; Abbasi, H.; Rozbahani, S.; Nasr-Esfahani, M.H. A preliminary study: N-acetyl-L-cysteine improves semen quality following varicocelectomy. Int. J. Fertil. Steril. 2016, 10, 120–126. [Google Scholar] [PubMed]
- Cyrus, A.; Kabir, A.; Goodarzi, D.; Moghimi, M. The effect of adjuvant vitamin C after varicocele surgery on sperm quality and quantity in infertile men: A double blind placebo controlled clinical trial. Int. Braz. J. Urol. 2015, 41, 230–238. [Google Scholar] [CrossRef] [Green Version]
- Ener, K.; Aldemir, M.; Işık, E.; Okulu, E.; Özcan, M.F.; Uğurlu, M.; Tangal, S.; Özayar, A. The impact of vitamin E supplementation on semen parameters and pregnancy rates after varicocelectomy: A randomised controlled study. Andrologia 2016, 48, 829–834. [Google Scholar] [CrossRef]
- Galatioto, G.P.; Gravina, G.L.; Angelozzi, G.; Sacchetti, A.; Innominato, P.F.; Pace, G.; Ranieri, G.; Vicentini, C. May antioxidant therapy improve sperm parameters of men with persistent oligospermia after retrograde embolization for varicocele? World J. Urol. 2007, 26, 97–102. [Google Scholar] [CrossRef]
- Gamidov, S.I.; Ovchinnikov, R.I.; Popova, A.Y.; Avakyan, A.Y.; Sukhikh, G.T. Adjuvant antioxidant therapy in varicocele infertility. Urologiia 2017, 2017, 64–72. [Google Scholar] [CrossRef]
- Kızılay, F.; Altay, B. Evaluation of the effects of antioxidant treatment on sperm parameters and pregnancy rates in infertile patients after varicocelectomy: A randomized controlled trial. Int. J. Impot. Res. 2019, 31, 424–431. [Google Scholar] [CrossRef]
- Neimark, A.; Neimark, B.; Davydov, A.; Saldan, I.; Nozdrachev, N. Rehabilitation of patients with male infertility after varicocelectomy. Eff. Pharmacother. 2018, 8–12. [Google Scholar]
- Pourmand, G.; Movahedin, M.; Dehghani, S.; Mehrsai, A.; Ahmadi, A.; Pourhosein, M. Does anti-oxidant therapy add any extra benefit to standard inguinal varicocelectomy in terms of DNA damage or sperm quality factor indices? A randomized study. Int. J. Reprod. Biomed. 2014, 12, 40. [Google Scholar]
- Povelitsa, E.A.; Leanovich, V.E.; Dosta, N.I.; Parhomenko, O.V.; Shesternya, A.M. Combined treatment of oligoasthenospermia by postoperative Speroton therapy in patients with varicocele. Androl. Genit. Surg. 2020, 21, 64–69. [Google Scholar] [CrossRef]
- Zadeh, A.A.; Arab, D.; Kia, N.S.; Heshmati, S.; Amirkhalili, S.N. The role of vitamin E-selenium-folic acid supplementation in improving sperm parameters after varicocelectomy: A randomized clinical trial. Urol. J. 2019, 16, 495–500. [Google Scholar] [CrossRef]
- Kumar, R.; Garg, H. An update on the role of medical treatment including antioxidant therapy in varicocele. Asian J. Androl. 2016, 18, 222–228. [Google Scholar] [CrossRef]
- Boeri, L.; Belladelli, F.; Capogrosso, P.; Cazzaniga, W.; Candela, L.; Pozzi, E.; Valsecchi, L.; Papaleo, E.; Viganò, P.; Abbate, C.; et al. Normal sperm parameters per se do not reliably account for fertility: A case-control study in the real-life setting. Andrologia 2021, 53, e13861. [Google Scholar] [CrossRef]
- Guzick, D.S.; Overstreet, J.W.; Factor-Litvak, P.; Brazil, C.K.; Nakajima, S.T.; Coutifaris, C.; Carson, S.A.; Cisneros, P.; Steinkampf, M.P.; Hill, J.A.; et al. Sperm morphology, motility, and concentration in fertile and infertile men. N. Engl. J. Med. 2001, 345, 1388–1393. [Google Scholar] [CrossRef]
- WHO. WHO Laboratory Manual for the Examination and Processing of Human Semen, 5th ed.; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Agarwal, A.; Sharma, R.; Roychoudhury, S.; Du Plessis, S.; Sabanegh, E. MiOXSYS: A novel method of measuring oxidation reduction potential in semen and seminal plasma. Fertil. Steril. 2016, 106, 566–573.e10. [Google Scholar] [CrossRef] [Green Version]
- Dimitriadis, F.; Tsounapi, P.; Zachariou, A.; Kaltsas, A.; Sokolakis, I.; Hatzichristodoulou, G.; Symeonidis, E.N.; Kotsiris, D.; Gabales, M.R.; Vlachopoulou, E.; et al. Therapeutic effects of micronutrient supplements on sperm parameters: Fact or fiction? Curr. Pharm. Des. 2020, 26, 1–24. [Google Scholar] [CrossRef]
- Baazeem, A.; Belzile, E.; Ciampi, A.; Dohle, G.; Jarvi, K.; Salonia, A.; Weidner, W.; Zini, A. Varicocele and male factor infertility treatment: A new meta-analysis and review of the role of varicocele repair. Eur. Urol. 2011, 60, 796–808. [Google Scholar] [CrossRef]
- Salonia, A.; Bettocchi, C.; Boeri, L.; Capogrosso, P.; Carvalho, J.; Cilesiz, N.C.; Cocci, A.; Corona, G.; Dimitropolous, K.; Gül, M.; et al. European association of urology guidelines on sexual and reproductive health—2021 update: Male sexual dysfunction. Eur. Urol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Silay, M.S.; Hoen, L.; Quadackaers, J.; Undre, S.; Bogaert, G.; Dogan, H.S.; Kocvara, R.; Nijman, R.J.; Radmayr, C.; Tekgul, S.; et al. Treatment of varicocele in children and adolescents: A systematic review and meta-analysis from the European association of urology/European society for paediatric urology guidelines panel. Eur. Urol. 2019, 75, 448–461. [Google Scholar] [CrossRef] [PubMed]
- Dimitriadis, F.; Symeonidis, E.N.; Tsounapi, P.; Kaltsas, A.; Hatzichristodoulou, G.; Sokolakis, I.; Zachariou, A.; Takenaka, A.; Sofikitis, N. Administration of antioxidants in the infertile male: When may it have a detrimental effect? Curr. Pharm. Des. 2021, 27, 1. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year of Publication | Type of Study | Population | Type of Antioxidant Supplementation | Duration of Treatment | Participants (n) | Adverse Events |
|---|---|---|---|---|---|---|
| Azizollahi 2013 [26] | RCT | Patients with surgically corrected clinical grade III varicocele and infertility receiving antioxidants × 1/day vs. placebo | 66 mg zinc 5 mg folic acid 66 mg zinc and 5mg folic acid | 6 months | 32 vs. 25 26 vs. 25 29 vs. 25 | No AEs or AE-related dropouts were reported in both groups |
| Barekat 2016 [27] | RCT | Patients with surgically corrected clinical grade II or III varicocele and infertility receiving antioxidants × 1/day vs. no treatment | 200 mg N-acetylcysteine | 3 months | 15 vs. 20 | No AEs or AE-related dropouts were reported in both groups |
| Busetto 2018 [23] | RCT | Patients with non-operated clinical grade I–III varicocele and infertility receiving antioxidants × 2/day vs. placebo | 1 g L-carnitine, 725 mg fumarate, 0.5 g acetyl-L-carnitine, 1 g fructose, 20 mg CoQ10, 90 mg vitamin C, 10 mg zinc, 200 μg folic acid and 1.5 μg vitamin B12 | 6 months | 21 vs. 24 | Nausea, vertigo, or headache in patients receiving antioxidants |
| Cavallini 2004 [24] | RCT | Patients with non-operated sonographical grade IΙΙ–V varicocele and infertility receiving antioxidants × 2/day vs. placebo | 2 g L-carnitine and 0.5 g acetyl-L-carnitine | 6 months | 62 vs. 71 | No AEs or AE-related dropouts were reported in both groups |
| Cyrus 2015 [28] | RCT | Patients with surgically corrected clinical grade II or III varicocele and infertility receiving antioxidants × 2/day vs. placebo | 250 mg vitamin C | 3 months | 46 vs. 69 | No AEs or AE-related dropouts were reported in both groups |
| Ener 2016 [29] | RCT | Patients with surgically corrected clinical grade III varicocele and infertility receiving antioxidants × 2/day vs. no treatment | 300 mg vitamin E | 12 months | 22 vs. 23 | No AEs or AE-related dropouts were reported in both groups |
| Galatioto 2008 [30] | RCT | Patients with embolization of sonographical grade III–V varicocele and infertility receiving antioxidants × 1/day vs. no treatment | 10 mg/kg N-acetyl-cysteine, 3 mg/kg vitamin C, 0.2 mg/kg vitamin E, 0.06 IU/kg vitamin A, 0.4 mg/kg thiamine, 0.1 mg/kg riboxavin, 0.2 mg/kg piridoxin, 1 mg/kg nicotinamide, 0.2 mg/kg pantothenate, 0.04 mg/kg biotin, 0.1 mg/kg cyanocobalamin, 8IU/kg ergocalciferol, 1 mg/kg calcium, 0.35 mg/kg magnesium, 0.45 mg/kg phosphate, 0.2 mg/kg iron, 0.01 mg/kg manganese, 0.02 mg/kg copper, and 0.01 mg/kg zinc | 3 months | 20 vs. 22 | No AEs or AE-related dropouts were reported in both groups |
| Gamidov 2017 [31] | RCT | Patients with surgically corrected clinical grade II or III varicocele and infertility receiving antioxidants × 1/day vs. no treatment | 1 g acetyl-L-carnitine, 2 g L-carnitine, 100 mg alpha-lipoic acid, 100 mg vitamin D and 4 g fructose | 3 months | 38 vs. 38 | No AEs or AE-related dropouts were reported in both groups |
| Kizilay 2019 [32] | RCT | Patients with surgically corrected clinical grade I–III varicocele and infertility receiving antioxidants × 2/day vs. no treatment | 1 g L-carnitine, 0.5 g acetyl-L carnitine, 1 g fructose, 50 mg citric acid, 90 mg vitamin C, 10mg zinc, 200 μg folic acid, 50 μg selenium, 20 mg CoQ10, and 1.5 μg vitamin B12 | 6 months | 62 vs. 28 | Nausea in 5 patients and gastroesophageal reflux in 4 patients receiving antioxidants |
| Neimark 2018 [33] | RCT | Patients with surgically corrected clinical grade III varicocele and infertility receiving antioxidants × 4/day vs. no treatment | 180 mg L-arginine, 60 mg L-carnitine, 23 mg L-carnosine, 2.5 mg CoQ10, 1.5 mg glycyrrhizic acid, 1.2 mg zinc, 0.8 mg vitamin E, 0.09 mg vitamin A, and 8.5 μg selenium | 6 months | 38 vs. 42 | No AEs or AE-related dropouts were reported in both groups |
| Pourmand 2014 [34] | RCT | Patients with surgically corrected clinical grade I–III varicocele and infertility receiving antioxidants × 3/day vs. no treatment | 250 mg L-carnitine | 6 months | 50 vs. 50 | Gastrointestinal reflux in patients receiving antioxidants |
| Povelitsa 2020 [35] | RCT | Patients with surgically corrected clinical grade III varicocele and infertility receiving antioxidants × 1/day vs. no treatment | 750 mg L-carnitine, 21 mg zinc, 30 mg vitamin E, 400 μg vitamin B9, and 70 μg selenium | 3 months | 20 vs. 20 | No AEs or AE-related dropouts were reported in both groups |
| Sofimajidpour 2016 [25] | Non-RCT | Patients with clinical grade II or III varicocele and infertility receiving antioxidants × 4/day vs. undergoing surgery | 250 mg L-carnitine | 6 months | 31 vs. 31 | No AEs or AE-related dropouts were reported in both groups |
| Zadeh 2019 [36] | RCT | Patients with surgically corrected clinical grade I–III varicocele and infertility receiving antioxidants × 1/day vs. no treatment | 5 mg folic acid, 200 mg selenium, and 400 IU vitamin E | 6 months | 30 vs. 30 | No AEs or AE-related dropouts were reported in both groups |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pyrgidis, N.; Sokolakis, I.; Palapelas, V.; Tishukov, M.; Mykoniatis, I.; Symeonidis, E.N.; Zachariou, A.; Kaltsas, A.; Sofikitis, N.; Hatzichristodoulou, G.; et al. The Effect of Antioxidant Supplementation on Operated or Non-Operated Varicocele-Associated Infertility: A Systematic Review and Meta-Analysis. Antioxidants 2021, 10, 1067. https://doi.org/10.3390/antiox10071067
Pyrgidis N, Sokolakis I, Palapelas V, Tishukov M, Mykoniatis I, Symeonidis EN, Zachariou A, Kaltsas A, Sofikitis N, Hatzichristodoulou G, et al. The Effect of Antioxidant Supplementation on Operated or Non-Operated Varicocele-Associated Infertility: A Systematic Review and Meta-Analysis. Antioxidants. 2021; 10(7):1067. https://doi.org/10.3390/antiox10071067
Chicago/Turabian StylePyrgidis, Nikolaos, Ioannis Sokolakis, Vasileios Palapelas, Maksim Tishukov, Ioannis Mykoniatis, Evangelos N. Symeonidis, Athanasios Zachariou, Aris Kaltsas, Nikolaos Sofikitis, Georgios Hatzichristodoulou, and et al. 2021. "The Effect of Antioxidant Supplementation on Operated or Non-Operated Varicocele-Associated Infertility: A Systematic Review and Meta-Analysis" Antioxidants 10, no. 7: 1067. https://doi.org/10.3390/antiox10071067
APA StylePyrgidis, N., Sokolakis, I., Palapelas, V., Tishukov, M., Mykoniatis, I., Symeonidis, E. N., Zachariou, A., Kaltsas, A., Sofikitis, N., Hatzichristodoulou, G., Tsiampali, C., & Dimitriadis, F. (2021). The Effect of Antioxidant Supplementation on Operated or Non-Operated Varicocele-Associated Infertility: A Systematic Review and Meta-Analysis. Antioxidants, 10(7), 1067. https://doi.org/10.3390/antiox10071067