
Oxidative Stress Biomarkers in Chronic Obstructive Pulmonary Disease Exacerbations: A Systematic Review

 ,
,  , ,
, ,  and
and
Abstract
1. Introduction
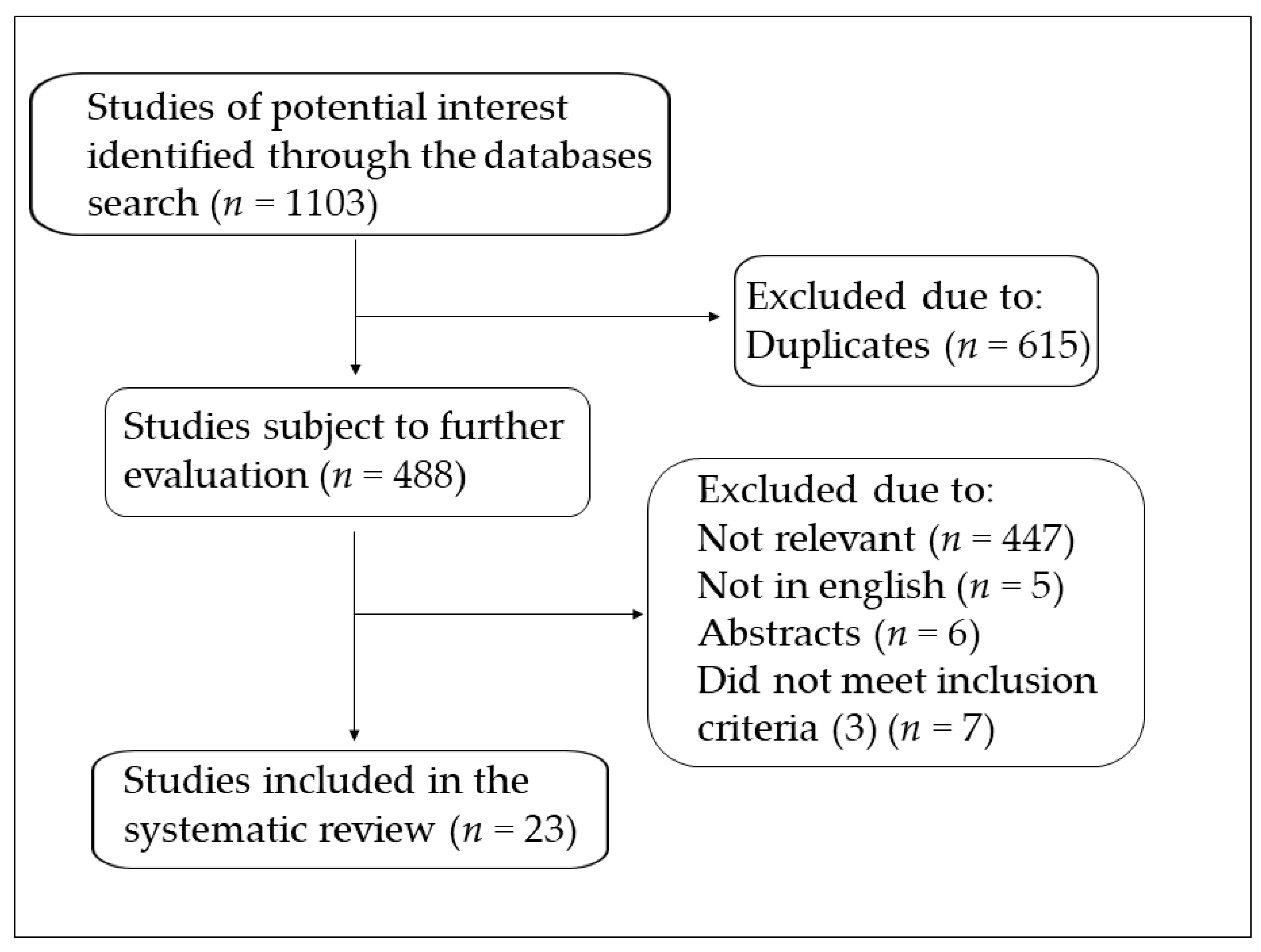
2. Search Strategy and Study Selection
3. Oxidative Stress Biomarkers in Exacerbated COPD
3.1. Brief Overview
3.2. Blood Biomarkers
3.3. Sputum Biomarkers
3.4. EBC and BALF Biomarkers
4. Discussion
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report. GOLD Executive Summary. Am. J. Respir. Crit. Care Med. 2017, 195, 557–582. [Google Scholar] [CrossRef] [PubMed]
- Barnes, P.J. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J. Allergy Clin. Immunol. 2016, 138, 16–27. [Google Scholar] [CrossRef]
- Lamprecht, B.; McBurnie, M.A.; Vollmer, W.M.; Gudmundsson, G.; Welte, T.; Nizankowska-Mogilnicka, E.; Studnicka, M.; Bateman, E.; Anto, J.M.; Burney, P.; et al. COPD in never smokers: Results from the population-based burden of obstructive lung disease study. Chest 2011, 139, 752–763. [Google Scholar] [CrossRef] [PubMed]
- Agustí, A.; Hogg, J.C. Update on the Pathogenesis of Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2019, 381, 1248–1256. [Google Scholar] [CrossRef] [PubMed]
- Brusselle, G.G.; Joos, G.F.; Bracke, K.R. New insights into the immunology of chronic obstructive pulmonary disease. Lancet 2011, 378, 1015–1026. [Google Scholar] [CrossRef]
- Fischer, B.M.; Voynow, J.A.; Ghio, A.J. COPD: Balancing oxidants and antioxidants. Int. J. Chron. Obs. Pulmon. Dis. 2015, 10, 261–276. [Google Scholar] [CrossRef]
- Kirkham, P.A.; Barnes, P.J. Oxidative stress in COPD. Chest 2013, 144, 266–273. [Google Scholar] [CrossRef]
- Marrocco, I.; Altieri, F.; Peluso, I. Measurement and Clinical Significance of Biomarkers of Oxidative Stress in Humans. Oxid. Med. Cell. Longev. 2017, 2017, 6501046. [Google Scholar] [CrossRef]
- de Groot, L.; van der Veen, T.A.; Martinez, F.O.; Hamann, J.; Lutter, R.; Melgert, B.N. Oxidative stress and macrophages: Driving forces behind exacerbations of asthma and chronic obstructive pulmonary disease? Am. J. Physiol. Lung Cell. Mol. Physiol. 2019, 316, L369–L384. [Google Scholar] [CrossRef]
- Ritchie, A.I.; Wedzicha, J.A. Definition, Causes, Pathogenesis, and Consequences of Chronic Obstructive Pulmonary Disease Exacerbations. Clin. Chest Med. 2020, 41, 421–438. [Google Scholar] [CrossRef]
- Halpin, D.M.; Miravitlles, M.; Metzdorf, N.; Celli, B. Impact and prevention of severe exacerbations of COPD: A review of the evidence. Int. J. Chron. Obs. Pulmon. Dis. 2017, 12, 2891–2908. [Google Scholar] [CrossRef]
- Paliogiannis, P.; Fois, A.G.; Sotgia, S.; Mangoni, A.A.; Zinellu, E.; Pirina, P.; Carru, C.; Zinellu, A. Circulating malondialdehyde concentrations in patients with stable chronic obstructive pulmonary disease: A systematic review and meta-analysis. Biomark. Med. 2018, 12, 771–781. [Google Scholar] [CrossRef]
- Zinellu, E.; Zinellu, A.; Fois, A.G.; Fois, S.S.; Piras, B.; Carru, C.; Pirina, P. Reliability and Usefulness of Different Biomarkers of Oxidative Stress in Chronic Obstructive Pulmonary Disease. Oxid. Med. Cell. Longev. 2020, 2020, 4982324. [Google Scholar] [CrossRef]
- Rahman, I.; Morrison, D.; Donaldson, K.; MacNee, W. Systemic oxidative stress in asthma, COPD, and smokers. Am. J. Respir. Crit. Care Med. 1996, 154, 1055–1060. [Google Scholar] [CrossRef]
- Calikoğlu, M.; Unlü, A.; Tamer, L.; Ercan, B.; Buğdayci, R.; Atik, U. The levels of serum vitamin C, malonyldialdehyde and erythrocyte reduced glutathione in chronic obstructive pulmonary disease and in healthy smokers. Clin. Chem. Lab. Med. 2002, 40, 1028–1031. [Google Scholar] [CrossRef]
- Tug, T.; Karatas, F.; Terzi, S.M. Antioxidant vitamins (A, C and E) and malondialdehyde levels in acute exacerbation and stable periods of patients with chronic obstructive pulmonary disease. Clin. Investig. Med. 2004, 27, 123–128. [Google Scholar]
- Tug, T.; Karatas, F.; Terzi, S.M.; Ozdemir, N. Comparison of serum malondialdehyde levels determined by two different methods in patients with COPD: HPLC or TBARS methods. Lab. Med. 2004, 36, 41–44. [Google Scholar] [CrossRef]
- Hanta, I.; Kocabas, A.; Canacankatan, N.; Kuleci, S.; Seydaoglu, G. Oxidant-antioxidant balance in patients with COPD. Lung 2006, 184, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Sadowska, A.M.; Luyten, C.; Vints, A.M.; Verbraecken, J.; van Ranst, D.; de Backer, W.A. Systemic antioxidant defences during acute exacerbation of chronic obstructive pulmonary disease. Respirology 2006, 11, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Koutsokera, A.; Kiropoulos, T.S.; Nikoulis, D.J.; Daniil, Z.D.; Tsolaki, V.; Tanou, K.; Papaioannou, A.I.; Germenis, A.; Gourgoulianis, K.I.; Kostikas, K. Clinical, functional and biochemical changes during recovery from COPD exacerbations. Respir. Med. 2009, 103, 919–926. [Google Scholar] [CrossRef] [PubMed]
- Zeng, M.; Li, Y.; Jiang, Y.; Lu, G.; Huang, X.; Guan, K. Local and systemic oxidative stress status in chronic obstructive pulmonary disease patients. Can. Respir. J. 2013, 20, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Stanojkovic, I.; Kotur-Stevuljevic, J.; Spasic, S.; Milenkovic, B.; Vujic, T.; Stefanovic, A.; Ivanisevic, J. Relationship between bone resorption, oxidative stress and inflammation in severe COPD exacerbation. Clin. Biochem. 2013, 46, 1678–1682. [Google Scholar] [CrossRef]
- Ermis, H.; Celik, M.R.; Gulbas, G.; Tavli, D.; Aytemur, Z.A. Relationship between serum gamma-glutamyltransferase levels and acute exacerbation of chronic obstructive pulmonary disease. Pol. Arch. Med. Wewn. 2013, 123, 85–90. [Google Scholar]
- Antus, B.; Paska, C.; Simon, B.; Barta, I. Monitoring Antioxidant Enzyme Activity during Exacerbations of Chronic Obstructive Pulmonary Disease. COPD 2018, 15, 496–502. [Google Scholar] [CrossRef]
- Lıu, X.; Deng, K.; Chen, S.; Zhang, Y.; Yao, J.; Weng, X.; Zhang, Y.; Gao, T.; Feng, G. 8-Hydroxy-2’-deoxyguanosine as a biomarker of oxidative stress in acute exacerbation of chronic obstructive pulmonary disease. Turk. J. Med. Sci. 2019, 49, 93–100. [Google Scholar] [CrossRef]
- Sun, D.; Liu, H.; Ouyang, Y.; Liu, X.; Xu, Y. Serum Levels of Gamma-Glutamyltransferase During Stable and Acute Exacerbations of Chronic Obstructive Pulmonary Disease. Med. Sci. Monit. 2020, 26, e927771. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.; Wang, S.; Qiu, Y.; Jiang, E.; Du, G.; Wang, W.; Xu, P.; Yang, H.; Hu, M.; Xiao, W. Screening for and combining serum intestinal barrier-related biomarkers to predict the disease severity of AECOPD. Ann. Palliat. Med. 2021, 10, 1548–1559. [Google Scholar] [CrossRef]
- Kersul, A.L.; Iglesias, A.; Ríos, Á.; Noguera, A.; Forteza, A.; Serra, E.; Agustí, A.; Cosío, B.G. Molecular mechanisms of inflammation during exacerbations of chronic obstructive pulmonary disease. Arch. Bronconeumol. 2011, 47, 176–183. [Google Scholar] [CrossRef]
- Tufvesson, E.; Ekberg, M.; Bjermer, L. Inflammatory biomarkers in sputum predict COPD exacerbations. Lung 2013, 191, 413–416. [Google Scholar] [CrossRef]
- Turgut, T.; Ilhan, N.; Deveci, F.; Akpolat, N.; Erden, E.Ş.; Muz, M.H. Glutathione and nitrite levels in induced sputum at COPD patients and healthy smokers. J. Thorac. Dis. 2014, 6, 765–771. [Google Scholar] [PubMed]
- Antus, B.; Harnasi, G.; Drozdovszky, O.; Barta, I. Monitoring oxidative stress during chronic obstructive pulmonary disease exacerbations using malondialdehyde. Respirology 2014, 19, 74–79. [Google Scholar] [CrossRef]
- Drozdovszky, O.; Barta, I.; Antus, B. Sputum eicosanoid profiling in exacerbations of chronic obstructive pulmonary disease. Respiration 2014, 87, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Dekhuijzen, P.N.; Aben, K.K.; Dekker, I.; Aarts, L.P.; Wielders, P.L.; van Herwaarden, C.L.; Bast, A. Increased exhalation of hydrogen peroxide in patients with stable and unstable chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 1996, 154, 813–816. [Google Scholar] [CrossRef] [PubMed]
- Biernacki, W.A.; Kharitonov, S.A.; Barnes, P.J. Increased leukotriene B4 and 8-isoprostane in exhaled breath condensate of patients with exacerbations of COPD. Thorax 2003, 58, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Carpagnano, G.E.; Resta, O.; Foschino-Barbaro, M.P.; Spanevello, A.; Stefano, A.; Di Gioia, G.; Serviddio, G.; Gramiccioni, E. Exhaled Interleukine-6 and 8-isoprostane in chronic obstructive pulmonary disease: Effect of carbocysteine lysine salt monohydrate (SCMC-Lys). Eur. J. Pharm. 2004, 505, 169–175. [Google Scholar] [CrossRef]
- Drost, E.M.; Skwarski, K.M.; Sauleda, J.; Soler, N.; Roca, J.; Agusti, A.; MacNee, W. Oxidative stress and airway inflammation in severe exacerbations of COPD. Thorax 2005, 60, 293–300. [Google Scholar] [CrossRef]
- GBD Chronic Respiratory Disease Collaborators. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir. Med. 2020, 8, 585–596. [Google Scholar]
- Hurst, J.R.; Vestbo, J.; Anzueto, A.; Locantore, N.; Müllerova, H.; Tal-Singer, R.; Miller, B.; Lomas, D.A.; Agusti, A.; Macnee, W.; et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N. Engl. J. Med. 2010, 363, 1128–1138. [Google Scholar] [CrossRef]
- Footitt, J.; Mallia, P.; Durham, A.L.; Ho, W.E.; Trujillo-Torralbo, M.B.; Telcian, A.G.; Del Rosario, A.; Chang, C.; Peh, H.Y.; Kebadze, T.; et al. Oxidative and nitrosative stress and histone deacetylase-2 activity in exacerbations of COPD. Chest 2016, 149, 62–73. [Google Scholar] [CrossRef]
- Zinellu, E.; Zinellu, A.; Fois, A.G.; Carru, C.; Pirina, P. Circulating biomarkers of oxidative stress in chronic obstructive pulmonary disease: A systematic review. Respir. Res. 2016, 17, 150. [Google Scholar] [CrossRef]
- Barnes, P.J. Oxidative stress-based therapeutics in COPD. Redox Biol. 2020, 33, 101544. [Google Scholar] [CrossRef]
- Cazzola, M.; Calzetta, L.; Page, C.; Jardim, J.; Chuchalin, A.G.; Rogliani, P.; Matera, M.G. Influence of N-acetylcysteine on chronic bronchitis or COPD exacerbations: A meta-analysis. Eur. Respir. Rev. 2015, 24, 451–461. [Google Scholar] [CrossRef] [PubMed]
- Calverley, P.M.; Page, C.; Dal Negro, R.W.; Fontana, G.; Cazzola, M.; Cicero, A.F.; Pozzi, E.; Wedzicha, J.A. Effect of Erdosteine on COPD Exacerbations in COPD Patients with Moderate Airflow Limitation. Int. J. Chron. Obs. Pulmon. Dis. 2019, 14, 2733–2744. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Yang, D.; Huang, X.; Xiao, Z. Effect of carbocisteine on patients with COPD: A systematic review and meta-analysis. Int. J. Chron. Obs. Pulmon. Dis. 2017, 12, 2277–2283. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Oxidative Stress Biomarkers | Biological Specimen | AE (n) | ST (n) | Ref |
|---|---|---|---|---|
| MDA ↑; protein carbonyls ↔; TEAC ↓; protein thiols ↓ | plasma | 11 | 9 | [14] |
| MDA ↑; vitamin C ↓ | serum | |||
| reduced GSH ↓ | erythrocytes | 21 | 41 | [15] |
| MDA ↑; vitamin C ↔; vitamin A and E ↓ | serum | 24 | 24 | [16] |
| MDA ↑; | serum | 22 | 22 | [17] |
| MDA ↔ | plasma | |||
| SOD ↔ | erythrocytes | 31 | 71 | [18] |
| TEAC ↓; Vitamin A and E ↓ | plasma | |||
| GSH-Px ↑; SOD ↔ | whole blood | 12 | 17 | [19] |
| dROM ↔ | serum | 30 | 30 | [20] |
| MDA ↑; SOD ↓; GSH-Px ↓; reduced GSH ↓ | plasma | |||
| MDA ↑; SOD ↓; GSH-Px ↓; reduced GSH ↓ | sputum | 43 | 35 | [21] |
| TOS ↑ns; PON↑ns | serum | 85 | 85 | [22] |
| GGT ↑ | serum | 132 | 147 | [23] |
| SOD ↓ns; catalase ↓ns | serum | |||
| MDA ↑; SOD ↑; catalase ↑ | sputum | 36 | 24 | [24] |
| 8-OHdG ↑ | plasma | 110 | 24 | [25] |
| GGT ↑ | serum | 117 | 107 | [26] |
| GST ↔ | serum | 40 | 10 | [27] |
| TAC ↓ | sputum | 17 | 17 | [28] |
| 8-isoprostane ↑ ns; MPO ↑ ns | sputum | 25 | 43 | [29] |
| total GSH ↑ ns | sputum | 11 | 10 | [30] |
| MDA ↑ | Sputum | |||
| MDA ↔ | EBC | 34 | 21 | [31] |
| 8-isoprostane | sputum | 25 | 37 | [32] |
| H2O2 ↑ | EBC | 19 | 12 | [33] |
| 8-isoprostane ↑ | EBC | 21 | 12 | [34] |
| 8-isoprostane ↑ | EBC | 30 | 10 | [35] |
| reduced GSH ↓ | BALF | 14 | 7 | [36] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zinellu, E.; Zinellu, A.; Fois, A.G.; Pau, M.C.; Scano, V.; Piras, B.; Carru, C.; Pirina, P. Oxidative Stress Biomarkers in Chronic Obstructive Pulmonary Disease Exacerbations: A Systematic Review. Antioxidants 2021, 10, 710. https://doi.org/10.3390/antiox10050710
Zinellu E, Zinellu A, Fois AG, Pau MC, Scano V, Piras B, Carru C, Pirina P. Oxidative Stress Biomarkers in Chronic Obstructive Pulmonary Disease Exacerbations: A Systematic Review. Antioxidants. 2021; 10(5):710. https://doi.org/10.3390/antiox10050710
Chicago/Turabian StyleZinellu, Elisabetta, Angelo Zinellu, Alessandro G. Fois, Maria Carmina Pau, Valentina Scano, Barbara Piras, Ciriaco Carru, and Pietro Pirina. 2021. "Oxidative Stress Biomarkers in Chronic Obstructive Pulmonary Disease Exacerbations: A Systematic Review" Antioxidants 10, no. 5: 710. https://doi.org/10.3390/antiox10050710
APA StyleZinellu, E., Zinellu, A., Fois, A. G., Pau, M. C., Scano, V., Piras, B., Carru, C., & Pirina, P. (2021). Oxidative Stress Biomarkers in Chronic Obstructive Pulmonary Disease Exacerbations: A Systematic Review. Antioxidants, 10(5), 710. https://doi.org/10.3390/antiox10050710