Assessing Sensory Processing Dysfunction in Adults and Adolescents with Autism Spectrum Disorder: A Scoping Review

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Phase 1–Empirical Literature Search
2.2. Phase 2–Grey Literature Search
3. Results
3.1. Empircal Literature Search
3.2. Grey Literature Search
3.3. Empirical Studies
3.4. Summary of Assessment Types
- (1)
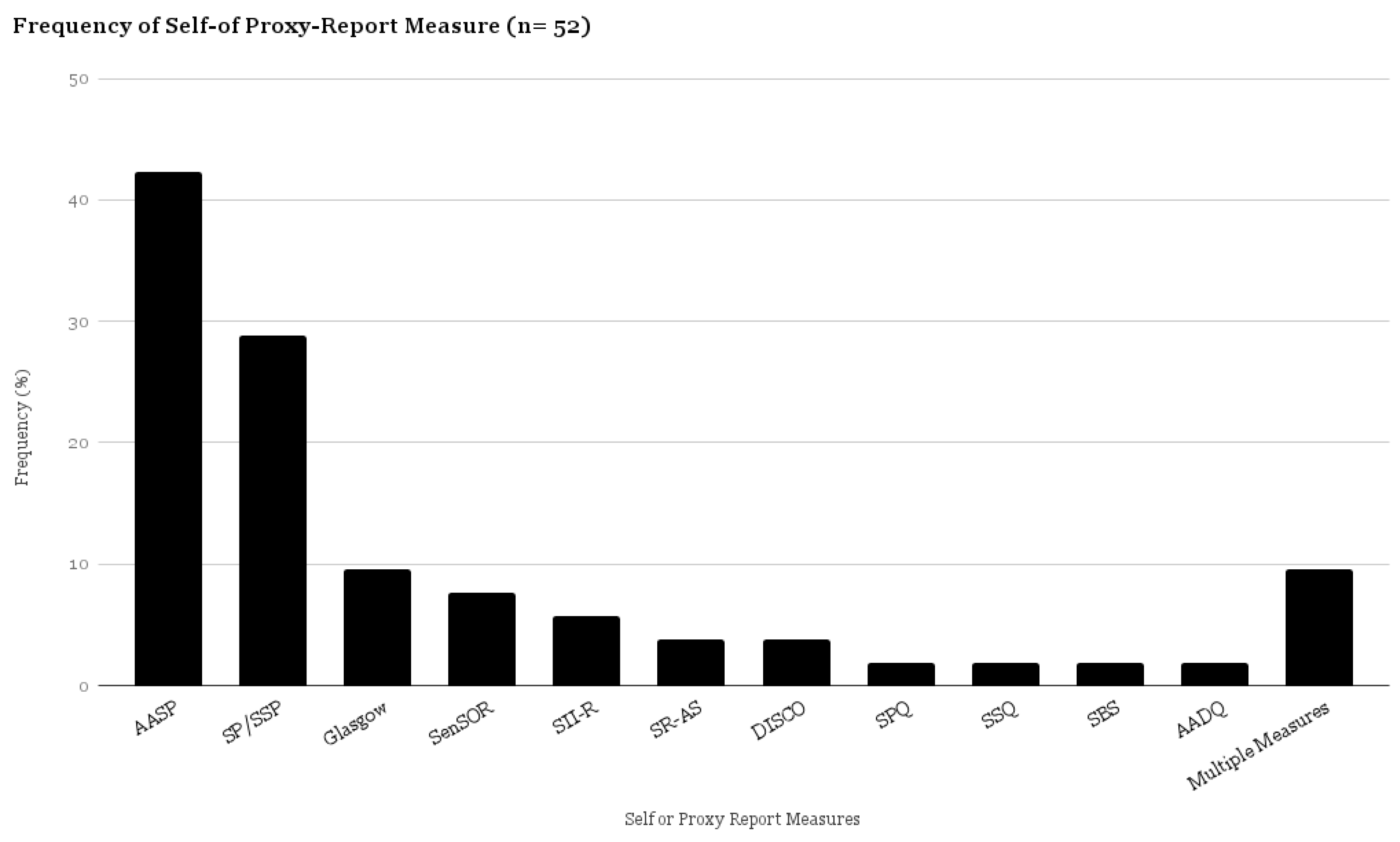
- Self- and Proxy-Report Measures: These are questionnaires requiring respondents to either read the items and select responses, or verbally respond to a list of questions read to them by an interviewer. Questions ask respondents to rate the kinds of difficulties they experience related to sensory processing. Proxy respondents may be caregivers or others, such as a clinician or significant other. Proxy respondents provide responses based on their perceptions of sensory processing behaviors and how frequently these behaviors occur.
- (2)
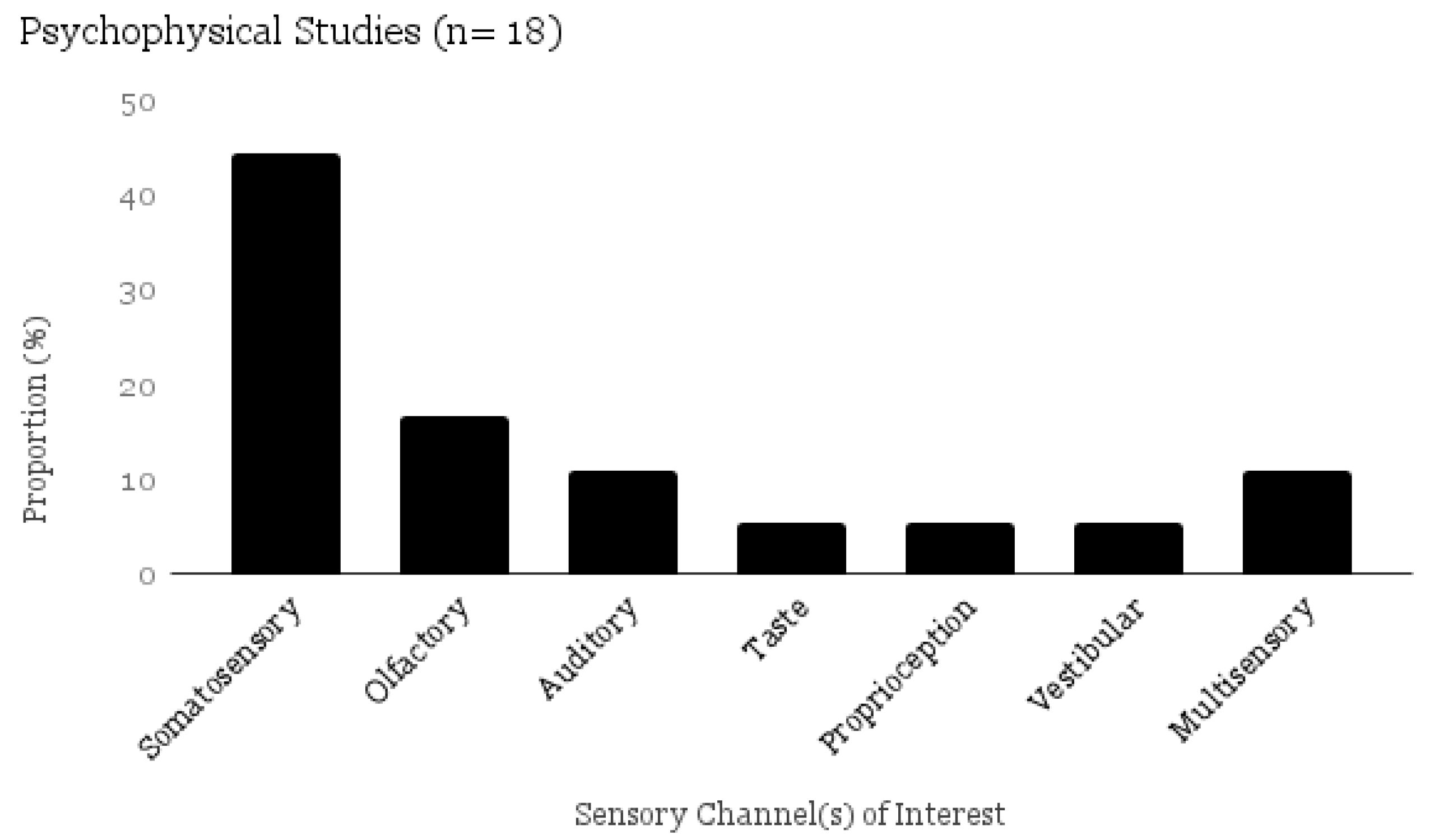
- Psychophysical Methods: This assessment method quantitatively measures the relationship between a controlled sensory stimulus and an individual’s physiological or self-reported response (e.g., detection, discrimination, and/or comfort thresholds).
- (3)
- Direct Observation: refers to a wide range of techniques (i.e., measure of frequency/intensity of specific behavior pattern, initiation and task completion, motivation and sensory preference assessments, timing, habits/routines, environmental factors) that may be used by clinicians and researchers to capture behaviors indicative of underlying sensory symptoms or preferences in either a controlled laboratory or real-world setting.
- (4)
- Qualitative Interview Methods: These methods involve having individuals describe their sensory experiences in an open-ended or semi-structured interview format, and then the responses are grouped and summarized by a researcher.
- (5)
- Neuroimaging/EEG: Functional neuroimaging measures brain responses through electroencephalogram (EEG) or functional magnetic resonance imaging (fMRI) with the aim to understand the relationship between a brain signal and certain clinical symptoms or observable behaviors.
3.4.1. Self- and Proxy-Report Measures
3.4.2. Psychophysical Methods
3.4.3. Direct Behavioral Observation
3.4.4. Qualitative Interview Techniques
3.4.5. Neuroimaging/EEG
4. Discussion
4.1. Use of Multiple Methods
4.2. Implications and Future Directions
4.3. Future Methodological Considerations
4.4. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Lord, C.; Risi, S.; Linda, L.; Cook, E.H., Jr.; Leventhal, B.L.; DiLavore, P.C.; Pickles, A.; Rutter, M. The Autism Diagnostic Observation Schedule—Generic: A standard mesure of social and communication deficits associated with the spectrum of autism. J. Autism Dev. Disord. 2000, 30, 205–223. [Google Scholar] [CrossRef] [PubMed]
- Leung, R.C.; Vogan, V.M.; Powell, T.L.; Anagnostou, E.; Taylor, M.J. The role of executive functions in social impairment in Autism Spectrum Disorder. Child Neuropsychol. 2015, 7049, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Schaaf, R.C.; Lane, A.E. Toward a Best-Practice Protocol for Assessment of Sensory Features in ASD. J. Autism Dev. Disord. 2015, 45, 1380–1395. [Google Scholar] [CrossRef] [PubMed]
- Cascio, C.J.; Woynaroski, T.; Baranek, G.T.; Wallace, M.T. Toward an interdisciplinary approach to understanding sensory function in autism spectrum disorder. Autism Res. 2016, 9, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Lillywhite, A.; Haines, D. Occupational Therapy and People with Learning Disabilities; College of Occupational Therapists: London, UK, 2010. [Google Scholar]
- Schauder, K.B.; Bennetto, L. Toward an interdisciplinary understanding of sensory dysfunction in autism spectrum disorder: An integration of the neural and symptom literatures. Front. Neurosci. 2016, 10, 268. [Google Scholar] [CrossRef] [PubMed]
- Marr, D. Fostering Full Implementation of Evidence-Based Practice. Am. J. Occup. Ther. 2017, 71, 1–5. [Google Scholar] [CrossRef] [PubMed]
- McKibbon, K.A. Evidence-Based Practice. Bull. Med. Libr. Assoc. 1998, 86, 396–401. [Google Scholar] [PubMed]
- Pilling, S.; Baron-Cohen, S.; Odette, M.-V.; Lee, R.; Taylor, C. Recognition, referral, diagnosis, and management of adults with autism: Summary of NICE guidance. Br. Med. J. 2012, 345, 43–45. [Google Scholar] [CrossRef] [PubMed]
- Dillenburger, K.; Dounavi, H.R.; Sparkman, K.; Keenan, C. Multidisciplinary Teamwork in Autism: Can One Size Fit All? Aust. Educ. Dev. Psychol. 2014, 31, 97–112. [Google Scholar] [CrossRef]
- Kuhaneck, H.M.; Henry, D.A.; Glennon, T.J. Sensory Processing Measure; Western Psychological Services: Los Angeles, CA, USA, 2007. [Google Scholar]
- Dunn, W. Sensory Profile; Psychological Coorporation: San Antonio, TE, USA, 1999. [Google Scholar]
- Ayres, A.J. Sensory Integration and Praxis Test; Western Psychological Services: Los Angeles, CA, USA, 1989. [Google Scholar]
- DeGangi, G.A.; Greenspan, S.I. Test of Sensory Functions in Infants (TSFI); Western Psychological Services: Philadelphia, PE, USA, 1989. [Google Scholar]
- Crane, L.; Goddard, L.; Pring, L. Sensory processing in adults with autism spectrum disorders. Autism 2009, 13, 215–228. [Google Scholar] [CrossRef] [PubMed]
- DuBois, D.; Ameis, S.H.; Desarkar, P.; Service, A.N.; Health, M.; Health, M.; Program, F.; Health, M. Interoception in Autism Spectrum Disorder : A Systematic Review. Int. J. Dev. Neurosci. 2016, 52, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.; Colquhoun, H.; Kastner, M.; Levac, D.; Ng, C.; Sharpe, J.P.; Wilson, K.; et al. A scoping review on the conduct and reporting of scoping reviews. BMC Med. Res. Methodol. 2016, 16, 15. [Google Scholar] [CrossRef] [PubMed]
- Colquhoun, H.L.; Levac, D.; O’brien, K.K.; Straus, S.; Tricco, A.C.; Perrier, L.; Kastner, M.; Moher, D. Scoping reviews: Time for clarity in definition, methods, and reporting. J. Clin. Epidemiol. 2014, 67, 1291–1294. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, K.; Colquhoun, H.; Levac, D.; Straus, S.; Baxter, L.; Moher, D.; O’Malley, L.; Parker, G.; Tattle, S.; Ya, T. Advancing the Field of Scoping Study Methodology Meeting Final Report; Unviersity of Toronto: Toronto, ON, Canada, 2015. [Google Scholar]
- Colquhoun, H.L.; Jesus, T.S.; O’Brien, K.K.; Tricco, A.C.; Chui, A.; Zarin, W.; Lillie, E.; Hitzig, S.L.; Straus, S. Study protocol for a scoping review on rehabilitation scoping reviews. Clin. Rehabil. 2017, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L.; Baldwin, S.; Harris, J.; Mason, A. Services to Support Carers of People with Mental Health Problems; National Health Service Delivery and Organization: London, UK, 2002. [Google Scholar]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 19–32. [Google Scholar] [CrossRef]
- Addo, R.N.; Wiens, S.; Nord, M.; Larsson, M. Olfactory Functions in Adults With Autism Spectrum Disorders. Perception 2017, 46, 530–537. [Google Scholar] [CrossRef] [PubMed]
- Ashburner, J.; Bennett, L.; Rodger, S.; Ziviani, J. Understanding the sensory experiences of young people with autism spectrum disorder: A preliminary investigation. Aust. Occup. Ther. J. 2013, 60, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Ashwin, C.; Chapman, E.; Howells, J.; Rhydderch, D.; Walker, I.; Baron-Cohen, S. Enhanced olfactory sensitivity in autism spectrum conditions. Mol. Autism 2014, 5, 53. [Google Scholar] [CrossRef] [PubMed]
- Billstedt, E.; Gillberg, C.; Gillberg, C. Autism in adults: Symptom patterns and early childhood predictors. Use of the DISCO in a community sample followed from childhood. J. Child Psychol. Psychiatry Allied Discip. 2007. [Google Scholar] [CrossRef] [PubMed]
- Brandwein, A.B.; Foxe, J.J.; Butler, J.S.; Frey, H.-P.; Bates, J.C.; Shulman, L.H.; Molholm, S. Neurophysiological Indices of Atypical Auditory Processing and Multisensory Integration are Associated with Symptom Severity in Autism. J. Autism Dev. Disord. 2015, 45, 230–244. [Google Scholar] [CrossRef] [PubMed]
- Cascio, C.; McGlone, F.; Folger, S.; Tannan, V.; Baranek, G.; Pelphrey, K.A.; Essick, G. Tactile perception in adults with autism: A multidimensional psychophysical study. J. Autism Dev. Disord. 2008, 38, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Cavalari, R.N.S.; Dubard, M.; Luiselli, J.K. Simplified Habit Reversal and Treatment Fading for Chronic Skin Picking in an Adolescent With Autism. Clin. Case Stud. 2014, 13, 190–198. [Google Scholar] [CrossRef]
- Chen, C.; Hung, A.-Y.; Fan, Y.-T.; Tan, S.; Hong, H.; Cheng, Y. Linkage between pain sensitivity and empathic response in adolescents with autism spectrum conditions and conduct disorder symptoms. Autism Res. 2017, 10, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Clince, M.; Connolly, L.; Nolan, C. Comparing and Exploring the Sensory Processing Patterns of Higher Education Students With Attention Deficit Hyperactivity Disorder and Autism Spectrum Disorder. Am. J. Occup. Ther. 2016. [Google Scholar] [CrossRef] [PubMed]
- Damiano, C.R.; Aloi, J.; Burrus, C.; Garbutt, J.C.; Kampov-Polevoy, A.B.; Dichter, G.S. Intact hedonic responses to sweet tastes in autism spectrum disorder. Res. Autism Spectr. Disord. 2014, 8, 230–236. [Google Scholar] [CrossRef] [PubMed]
- De La Marche, W.; Steyaert, J.; Noens, I. Atypical sensory processing in adolescents with an autism spectrum disorder and their non-affected siblings. Res. Autism Spectr. Disord. 2012, 6, 639–645. [Google Scholar] [CrossRef]
- Doumas, M.; Roisin McKenna, B.; Blain Murphy, B. Postural Control Deficits in Autism Spectrum Disorder: The Role of Sensory Integration. J. Autism Dev. Disord. 2016, 46, 853–861. [Google Scholar] [CrossRef] [PubMed]
- Duerden, E.G.; Taylor, M.J.; Lee, M.; McGrath, P.A.; Davis, K.D.; Roberts, S.W. Decreased sensitivity to thermal stimuli in adolescents with autism spectrum disorder: Relation to symptomatology and cognitive ability. J. Pain 2015, 16, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Dunlop, W.A.; Enticott, P.G.; Rajan, R. Speech Discrimination Difficulties in High-Functioning Autism Spectrum Disorder Are Likely Independent of Auditory Hypersensitivity. Front. Hum. Neurosci. 2016, 10, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Edgington, L.; Hill, V.; Pellicano, E. The design and implementation of a CBT-based intervention for sensory processing difficulties in adolescents on the autism spectrum. Res. Dev. Disabil. 2016, 59, 221–233. [Google Scholar] [CrossRef] [PubMed]
- Elwin, M.; Ek, L.; Kjellin, L.; Schröder, A. Too much or too little: Hyper-and hypo-reactivity in high-functioning autism spectrum conditions. J. Intellectural Dev. Disabil. 2013, 38, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Elwin, M.; Schroder, A.; Ek, L.; Kjellin, L. Development and pilot validation of a sensory reactivity scale for adults with high functioning autism spectrum conditions Sensory Reactivity in. Nord. J. Psychiatry 2016, 70, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Elwin, M.; Schröder, A.; Ek, L.; Wallsten, T.; Kjellin, L. Sensory Clusters of Adults With and Without Autism Spectrum Conditions. J. Autism Dev. Disord. 2017, 47, 579–589. [Google Scholar] [CrossRef] [PubMed]
- Fründt, O.; Grashorn, W.; Schöttle, D.; Peiker, I.; David, N.; Engel, A.K.; Forkmann, K.; Wrobel, N.; Münchau, A.; Bingel, U. Quantitative Sensory Testing in adults with Autism Spectrum Disorders. J. Autism Dev. Disord. 2017, 47, 1183–1192. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, C.T.; Mostofsky, S.H.; Bastian, A.J. No proprioceptive deficits in autism despite movement-related sensory and execution impairments. J. Autism Dev. Disord. 2011, 41, 1352–1361. [Google Scholar] [CrossRef] [PubMed]
- Fung, L.K.; Libove, R.A.; Phillips, J.; Haddad, F.; Hardan, A.Y. Brief report: An open-label study of the neurosteroid pregnenolone in adults with autism spectrum disorder. J. Autism Dev. Disord. 2015, 44, 1689–1699. [Google Scholar] [CrossRef]
- Gonthier, C.; Longuépée, L.; Bouvard, M. Sensory Processing in Low-Functioning Adults with Autism Spectrum Disorder: Distinct Sensory Profiles and Their Relationships with Behavioral Dysfunction. J. Autism Dev. Disord. 2016. [Google Scholar] [CrossRef] [PubMed]
- Green, S.A.; Rudie, J.D.; Colich, N.L.; Wood, J.J.; Shirinyan, D.; Hernandez, L.; Tottenham, N.; Dapretto, M.; Bookheimer, S.Y. Overreactive Brain Responses to Sensory Stimuli in Youth With Autism Spectrum Disorders. J. Am. Acad. Child Adolesc. Psychiatry 2013, 52, 1158–1172. [Google Scholar] [CrossRef] [PubMed]
- Green, S.A.; Hernandez, L.; Tottenham, N.; Krasileva, K.; Bookheimer, S.Y.; Dapretto, M. Neurobiology of Sensory Overresponsivity in Youth With Autism Spectrum Disorders. JAMA Psychiatry 2015, 72, 778. [Google Scholar] [CrossRef] [PubMed]
- Green, S.A.; Hernandez, L.; Bookheimer, S.Y.; Dapretto, M. Salience Network Connectivity in Autism Is Related to Brain and Behavioral Markers of Sensory Overresponsivity. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 618–626. [Google Scholar] [CrossRef] [PubMed]
- Green, D.; Beaton, L.; Moore, D.; Warren, L.; Wick, V.; Sanford, J.E.; Santosh, P. Clinical incidence of sensory integration difficulties in adults with learning disabilities and illustration of management. Br. J. Occup. Ther. 2003, 66, 454–463. [Google Scholar] [CrossRef]
- Haigh, S.M.; Heeger, D.J.; Dinstein, I.; Minshew, N.; Behrmann, M. Cortical Variability in the Sensory-Evoked Response in Autism. J. Autism Dev. Disord. 2014. [Google Scholar] [CrossRef] [PubMed]
- Haigh, S.M.; Minshew, N.; Heeger, D.J.; Dinstein, I.; Behrmann, M. Over-Responsiveness and Greater Variability in Roughness Perception in Autism. Autism Res. 2016, 9, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Hannant, P.; Cassidy, S.; Tavassoli, T.; Mann, F. Sensorimotor difficulties are associated with the severity of autism spectrum conditions. Front. Integr. Neurosci. 2016, 10, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Harrison, J.; Hare, D.J. Brief report: Assessment of sensory abnormalities in people with autistic spectrum disorders. J. Autism Dev. Disord. 2004, 34, 727–730. [Google Scholar] [CrossRef] [PubMed]
- Healey, J.J.; Ahearn, W.H.; Graff, R.B.; Libby, M.E. Extended analysis and treatment of self-injurious behavior. Behav. Interv. 2001, 16, 181–195. [Google Scholar] [CrossRef]
- Horder, J.; Wilson, C.E.; Mendez, M.A.; Murphy, D.G. Autistic traits and abnormal sensory experiences in adults. J. Autism Dev. Disord. 2014, 44, 1461–1469. [Google Scholar] [CrossRef] [PubMed]
- Howe, F.E.J.; Stagg, S.D. How Sensory Experiences Affect Adolescents with an Autistic Spectrum Condition within the Classroom. J. Autism Dev. Disord. 2016. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.R.G.; Happé, F.; Baird, G.; Simonoff, E.; Marsden, A.J.S.; Tregay, J.; Phillips, R.J.; Goswami, U.; Thomson, J.M.; Charman, T. Auditory discrimination and auditory sensory behaviours in autism spectrum disorders. Neuropsychologia 2009, 47, 2850–2858. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, M.D.; Yang, D.Y.J.; Voos, A.C.; Bennett, R.H.; Gordon, I.; Pretzsch, C.; Beam, D.; Keifer, C.; Eilbott, J.; McGlone, F.; et al. Brain Mechanisms for Processing Affective (and Nonaffective) Touch Are Atypical in Autism. Cereb. Cortex 2016, 26, 2705–2714. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, M.; Clopton, M.; Khazanova, O.; Kitaichik, T. The effects of Snoezelen use in adult developmental delay. Dev. Disabil. Spec. Interes. Sect. Q. 2007, 30, 1–4. [Google Scholar]
- Karhson, D.S.; Golob, E.J. Atypical Sensory Reactivity Influences Auditory Attentional Control in Adults with Autism Spectrum Disorders. Autism Res. 2016, 9, 1079–1092. [Google Scholar] [CrossRef] [PubMed]
- Kern, J.K.; Garver, C.R.; Grannemann, B.D.; Trivedi, M.H.; Carmody, T.; Andrews, A.A.; Mehta, J.A. Response to vestibular sensory events in autism. Res. Autism Spectr. Disord. 2007, 1, 67–74. [Google Scholar] [CrossRef]
- Kern, J.K.; Trivedi, M.H.; Grannemann, B.D.; Garver, C.R.; Johnson, D.G.; Andrews, A.A.; Savla, J.S.; Mehta, J.A.; Schroeder, J.L. Sensory correlations in autism. Autism 2007. [Google Scholar] [CrossRef] [PubMed]
- Kern, J.K.; Garver, C.R.; Carmody, T.; Andrews, A.A.; Mehta, J.A.; Trivedi, M.H. Examining sensory modulation in individuals with autism as compared to community controls. Res. Autism Spectr. Disord. 2008, 2, 85–94. [Google Scholar] [CrossRef]
- Kern, J.K.; Trivedi, M.H.; Garver, C.R.; Grannemann, B.D.; Andrews, A.A.; Savla, J.S.; Johnson, D.G.; Mehta, J.A.; Schroeder, J.L. The pattern of sensory processing abnormalities in autism. Autism 2006, 10, 480–494. [Google Scholar] [CrossRef] [PubMed]
- Kern, J.K.; Garver, C.R.; Carmody, T.; Andrews, A.A.; Trivedi, M.H.; Mehta, J.A. Examining sensory quadrants in autism. Res. Autism Spectr. Disord. 2007. [Google Scholar] [CrossRef]
- Kerns, C.; Kendall, P.; Berry, L.; Souders, M.; Franklin, M.E.; Schultz, R.T.; Miller, J.; Herrington, J.D. Traditional and Atypical Presentations of Anxiety in Youth with Autism Spectrum Disorder. J. Autism Dev. Disord. 2014, 44, 2851–2861. [Google Scholar] [CrossRef] [PubMed]
- Kuschner, E.S.; Eisenberg, I.W.; Orionzi, B.; Simmons, W.K.; Kenworthy, L.; Martin, A.; Wallace, G.L. A preliminary study of self-reported food selectivity in adolescents and young adults with autism spectrum disorder. Res. Autism Spectr. Disord. 2015. [Google Scholar] [CrossRef] [PubMed]
- Landon, J.; Shepherd, D.; Lodhia, V. A qualitative study of noise sensitivity in adults with autism spectrum disorder. Res. Autism Spectr. Disord. 2016. [Google Scholar] [CrossRef]
- Leekam, S.R.; Nieto, C.; Libby, S.J.; Wing, L.; Gould, J. Describing the sensory abnormalities of children and adults with autism. J. Autism Dev. Disord. 2007, 37, 894–910. [Google Scholar] [CrossRef] [PubMed]
- Mayer, J.L. The Relationship Between Autistic Traits and Atypical Sensory Functioning in Neurotypical and ASD Adults: A Spectrum Approach. J. Autism Dev. Disord. 2016. [Google Scholar] [CrossRef] [PubMed]
- Mayer, J.L.; Heaton, P.F. Age and Sensory Processing Abnormalities Predict Declines in Encoding and Recall of Temporally Manipulated Speech in High-Functioning Adults with ASD. Autism Res. 2014, 7, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Milosavljevic, B.; Carter Leno, V.; Simonoff, E.; Baird, G.; Pickles, A.; Jones, C.R.G.; Erskine, C.; Charman, T.; Happé, F. Alexithymia in Adolescents with Autism Spectrum Disorder: Its Relationship to Internalising Difficulties, Sensory Modulation and Social Cognition. J. Autism Dev. Disord. 2016. [Google Scholar] [CrossRef] [PubMed]
- Minshew, N.J.; Hobson, J.A. Sensory sensitivities and performance on sensory perceptual tasks in high-functioning individuals with autism. J. Autism Dev. Disord. 2008, 38, 1485–1498. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.; Cividini-Motta, C.; Clark, K.M.; Ahearn, W.H. Sensory Integration as a treatment for automatically maintained stereotypy. Behav. Interv. 2015, 30, 95–111. [Google Scholar] [CrossRef]
- Poole, D.; Gowen, E.; Warren, P.A.; Poliakoff, E. Brief Report: Which Came First? Exploring Crossmodal Temporal Order Judgements and Their Relationship with Sensory Reactivity in Autism and Neurotypicals. J. Autism Dev. Disord. 2017, 47, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Robertson, A.E.; Simmons, D.R. The sensory experiences of adults with autism spectrum disorder: A qualitative analysis. Perception 2015, 44, 569–586. [Google Scholar] [CrossRef] [PubMed]
- Smith-Myles, B.; Lee, H.J.; Smith, S.M.; Tien, K.; Chou, Y.; Swanson, T.C.; Hudson, J. A Large-Scale Study of the Characteristics of Asperger Syndrome. Educ. Train. 2007, 42, 448–459. [Google Scholar]
- Takayama, Y.; Hashimoto, R.; Tani, M.; Kanai, C.; Yamada, T.; Watanabe, H.; Ono, T.; Kato, N.; Iwanami, A. Standardization of the Japanese version of the Glasgow Sensory Questionnaire (GSQ). Res. Autism Spectr. Disord. 2014, 8, 347–353. [Google Scholar] [CrossRef]
- Tavassoli, T.; Baron-Cohen, S. Olfactory detection thresholds and adaptation in adults with autism spectrum condition. J. Autism Dev. Disord. 2012, 42, 905–909. [Google Scholar] [CrossRef] [PubMed]
- Tavassoli, T.; Baron-Cohen, S. Taste identification in adults with autism spectrum conditions. J. Autism Dev. Disord. 2012, 42, 1419–1424. [Google Scholar] [CrossRef] [PubMed]
- Tavassoli, T.; Miller, L.J.; Schoen, S.A.; Nielsen, D.M.; Baron-Cohen, S. Sensory over-responsivity in adults with autism spectrum conditions. Autism 2014, 18, 428–432. [Google Scholar] [CrossRef] [PubMed]
- Tavassoli, T.; Hoekstra, R.; Baron-Cohen, S. The Sensory Perception Quotient (SPQ): Development and validation of a new sensory questionnaire for adults with and without autism. Mol. Autism 2014, 5, 29. [Google Scholar] [CrossRef] [PubMed]
- Uljarevic, M.; Lane, A.; Kelly, A.; Leekam, S. Sensory subtypes and anxiety in older children and adolescents with autism spectrum disorder. Autism Res. 2016, 9, 1073–1078. [Google Scholar] [CrossRef] [PubMed]
- Urwin, R.; Ballinger, C. The effectiveness of sensory integration therapy to improve functional behaviour in adults with learning disabilities: Five single-case experimental designs. Br. J. Occup. Ther. 2005, 68, 56–66. [Google Scholar] [CrossRef]
- Ward, J.; Hoadley, C.; Hughes, J.E.A.; Smith, P.; Allison, C.; Baron-Cohen, S.; Simner, J. Atypical sensory sensitivity as a shared feature between synaesthesia and autism. Sci. Rep. 2017, 7, 41155. [Google Scholar] [CrossRef] [PubMed]
- Wicker, B.; Monfardini, E.; Royet, J.-P. Olfactory processing in adults with autism spectrum disorders. Mol. Autism 2016, 4. [Google Scholar] [CrossRef] [PubMed]
- Wigham, S.; Rodgers, J.; South, M.; McConachie, H.; Freeston, M. The interplay between sensory processing abnormalities, intolerance of uncertainty, anxiety and restricted and repetitive behaviours in autism spectrum disorder. J. Autism Dev. Disord. 2015, 45, 943–952. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, Y.; Hashimoto, R.; Nakae, A.; Kang, H.; Ohi, K.; Yamamori, H.; Fujimoto, M.; Hagihira, S.; Takeda, M. Sensory cognitive abnormalities of pain in autism spectrum disorder: A case–control study. Ann. Gen. Psychiatry 2016, 15, 8. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.; Tollefson, N.; Dunn, W.; Cromwell, R.; Filion, D. The adult sensory profile: Measuring patterns of sensory processing. Am. J. Occup. Ther. 2001, 55, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Schoen, S.A.; Miller, L.J.; Green, K.E. Pilot study of the sensory over-responsivity scales: Assessment and inventory. Am. J. Occup. Ther. 2008, 62, 393–406. [Google Scholar] [CrossRef] [PubMed]
- Wing, L.; Leekam, S.R.; Libby, S.J.; Gould, J.; Larcombe, M. The Diagnostic Interview for Social and Communication Disorders: Background, inter-rater reliability and clinical use. J. Child Psychol. Psychiatry 2002, 43, 307–325. [Google Scholar] [CrossRef] [PubMed]
- Elwin, M.; Ek, L.; Schröder, A.; Kjellin, L. Autobiographical accounts of sensing in Asperger syndrome and high-functioning autism. Arch. Psychiatr. Nurs. 2012, 26, 420–429. [Google Scholar] [CrossRef] [PubMed]
- Garfinkel, S.N.; Tiley, C.; O’Keeffe, S.; Harrison, N.A.; Seth, A.K. Discrepancies between dimensions of interoception in Autism: Implications for emotion and anxiety. Biol. Psychol. 2016, 114, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Schoen, S.A.; Miller, L.J.; Sullivan, J.C. Measurement in Sensory Modulation: The Sensory Processing Scale Assessment. Am. J. Occup. Ther. 2014, 68, 522–530. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| -Original research published in peer-reviewed journals | -Non-peer-reviewed |
| -Available electronically through CAMH or University of Toronto Libraries | -Did not focus directly on sensory processing (e.g., ASD diagnostic tools with limited sensory processing questions) |
| -Diagnosis of ASD with or without an IDD. | -Non-English language |
| -Use of a clearly defined sensory processing measure or technique | -Theses and conference abstracts |
| -Publication date before 1988 | |
| -Age 16+ included in study sample | -Reviews and Meta-analyses (used for cross-reference) |
| Organization | Country | Title | Year |
|---|---|---|---|
| National Institute of Health Care and Excellence | United Kingdom | Recognition, referral, diagnosis, and management of adults with autism | 2012 |
| Australian Psychological Association | Australia | Clinical Assessment Resource: An overview of best practice tools and approaches to conducting biopsychosocial and developmental assessment of child, young people, and adults with a disability who display behaviors of concern | 2011 |
| Canadian Association of Occupational Therapists (CAOT) | Canada | Position Statement on Autism Spectrum Disorders and Occupational Therapy | 2015 |
| American Occupational Therapy Association (AOTA) | United States | Scope of Occupational Therapy Services for Individuals with ASD across the Life Course | 2015 |
| College of Occupational Therapy | United Kingdom | Occupational Therapy and Learning Disabilities | 2012 |
| Self- or Proxy-Report Measures | Creators | Subscales/Items | Terminology | Age Group | Scoring | Clinically Available (Y/N) | Published Psycho-metric Prop-erties (Y/N) | Development | Discipline | Self- or Proxy-Report | ASD Specific (Y/N) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| AASP | Dunn, 2001 | Low Registration, Sensory Sensitivity, Sensory Avoidance, Sensory Seeking; taste/smell, movement, visual, touch, multisensory, activity level, and auditory | Four Quadrant Model of Sensory Processing; Neurological and Behavioral Thresholds | 11+ | 60 items; 4 point scale | Y | Y | Expert panel, factor analysis, construct validity–physiological measure | Occupation-al Therapy (OT) | Self-Report | N |
| SP/SSP | Dunn, 1997 | Sensory processing, modulation, and behavioral and emotional responses; taste/smell, movement, visual, touch, multisensory, activity level, and auditory | Four Quadrant Model of Sensory Processing; Neurological and Behavioral Thresholds | 3–10 | 125 items; 38 items (short); 4 point scale | Y | Y | Expert panel, factor analysis, construct validity–physiological measure | OT | Proxy-Report | N |
| SenSOR | Schoen et al., 2008 | Sensory over-responsivity (sensory sensitivity or sensory avoiding); touch, vision, hearing, smell, taste, and proprioception | Sensory Modulation | All ages | Unclear | N | Y | Factor analysis (discriminant validity, internal reliability/consistency); ongoing development; expert and lit review; correlated to examiner-scored behavior analysis and AASP | OT | Self/Care giver- Report | N |
| SII-R | Reisman & Hanschu, 1992 | tactile, vestibular and proprioceptive processing; “general reactions” section | Sensory Integration | Adult | Checklist | Y | N | Based on sensory integration theory | OT | Proxy-Report | N (IDD Specific) |
| GSQ | Horder et al., 2014 | visual, auditory, gustatory, olfactory, tactile, vestibular, and proprioceptive | Hypo and Hypersensitivities | Adults with ASD | 42 items; 4 point scale; total score | N | Y | Factor analysis across cultures; reports in the literature of sensory signs and symptoms commonly associated with ASD and b signs and symptoms reported by parents of children with ASD; correlated to AASP | OT | Self-Report | Y |
| SR-AS | Elwin et al., 2016 | hyper- and hypo-reactivity, strong sensory interest, and sensory/motor; visual, auditory, gustatory, olfactory, tactile, vestibular, proprioceptive and interoceptive | High and low awareness | Adults with ASD | 38 items; 4 point scale | N | Y | Qualitative interviews; factor/cluster analysis | Psychiatry | Self-Report | Y |
| DISCO | Wing, Leekam, Libby, Gould, & Larcombe, 2002 | touch, taste, smell, kinesthetic, auditory, and visual. Items relating to atypical taste/oral, movement, touch responsiveness, and self-injurious behavior | “proximal” (e.g., smell, taste, touch, kinesthetic and mixed) | Mixed Age Group–Autism | 25 items (sensory); 300 total for diagnostic tool | Y | Y | Chosen based on clinical observation; developed as part of diagnostic tool; factor analysis | Psychology | Proxy-Report/Inter-view | Y |
| SPQ | Tavassoli et al., 2014 | touch, hearing, vision, smell, and taste | basic detection and discrimination to sensory input measured across hyper-and hyposensitivity | Adults | 35 item; 4 point scale | N | Y | Factor analysis; correlated to SenSOR; developed to study basic detection and discrimination–based on ‘main sensory modalities’ (Goldstein, 2002) | Psychiatry | Self-Report | N |
| SBS | Harrison & Hare, 2004 | visual, auditory, gustatory, olfactory, tactile, vestibular, movement, proprioception, temperature and sensory processes | sensory symptoms (ongoing, past, none) | Adults with ASD | 17 items; ongoing, past, none | Y | N | Literature review, discussion with experts, and based on O'Neill (1995) | Psychology | Proxy-Report | Y |
| SSQ | Minshew & Hobson, 2008 | sound, light, tactile and temperature sensitivities, pain tolerance, awareness of smell or taste, and sensitivity to environmental events or conditions | sensory sensitivity | Mixed Age Group | 13 item; Yes/No | N | N | Based on items from the highly sensitive person self-report checklist (Aron and Aron 1997), common reactions to sensory stimuli reported by individuals with ASD, classic behavioral descriptions, and clinical reports | Psychiatry | Self-/Proxy-Report | Y |
| AADQ | Dunlop et al., 2016 | Auditory | auditory hypersensitivity; difficulty hearing in noisy environments | Adults | 33 items; 7 point Likert scale | Y | N | Based on validated inventories for specific adult clinical populations that experience abnormal auditory processing | Speech Language | Self-Report | N |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
DuBois, D.; Lymer, E.; Gibson, B.E.; Desarkar, P.; Nalder, E. Assessing Sensory Processing Dysfunction in Adults and Adolescents with Autism Spectrum Disorder: A Scoping Review. Brain Sci. 2017, 7, 108. https://doi.org/10.3390/brainsci7080108
DuBois D, Lymer E, Gibson BE, Desarkar P, Nalder E. Assessing Sensory Processing Dysfunction in Adults and Adolescents with Autism Spectrum Disorder: A Scoping Review. Brain Sciences. 2017; 7(8):108. https://doi.org/10.3390/brainsci7080108
Chicago/Turabian StyleDuBois, Denise, Erin Lymer, Barbara E. Gibson, Pushpal Desarkar, and Emily Nalder. 2017. "Assessing Sensory Processing Dysfunction in Adults and Adolescents with Autism Spectrum Disorder: A Scoping Review" Brain Sciences 7, no. 8: 108. https://doi.org/10.3390/brainsci7080108
APA StyleDuBois, D., Lymer, E., Gibson, B. E., Desarkar, P., & Nalder, E. (2017). Assessing Sensory Processing Dysfunction in Adults and Adolescents with Autism Spectrum Disorder: A Scoping Review. Brain Sciences, 7(8), 108. https://doi.org/10.3390/brainsci7080108