

Overview of the Current Knowledge and Conventional MRI Characteristics of Peri- and Para-Vascular Spaces

 ,
,  , , ,
, , ,  and
and 
Abstract
1. Introduction
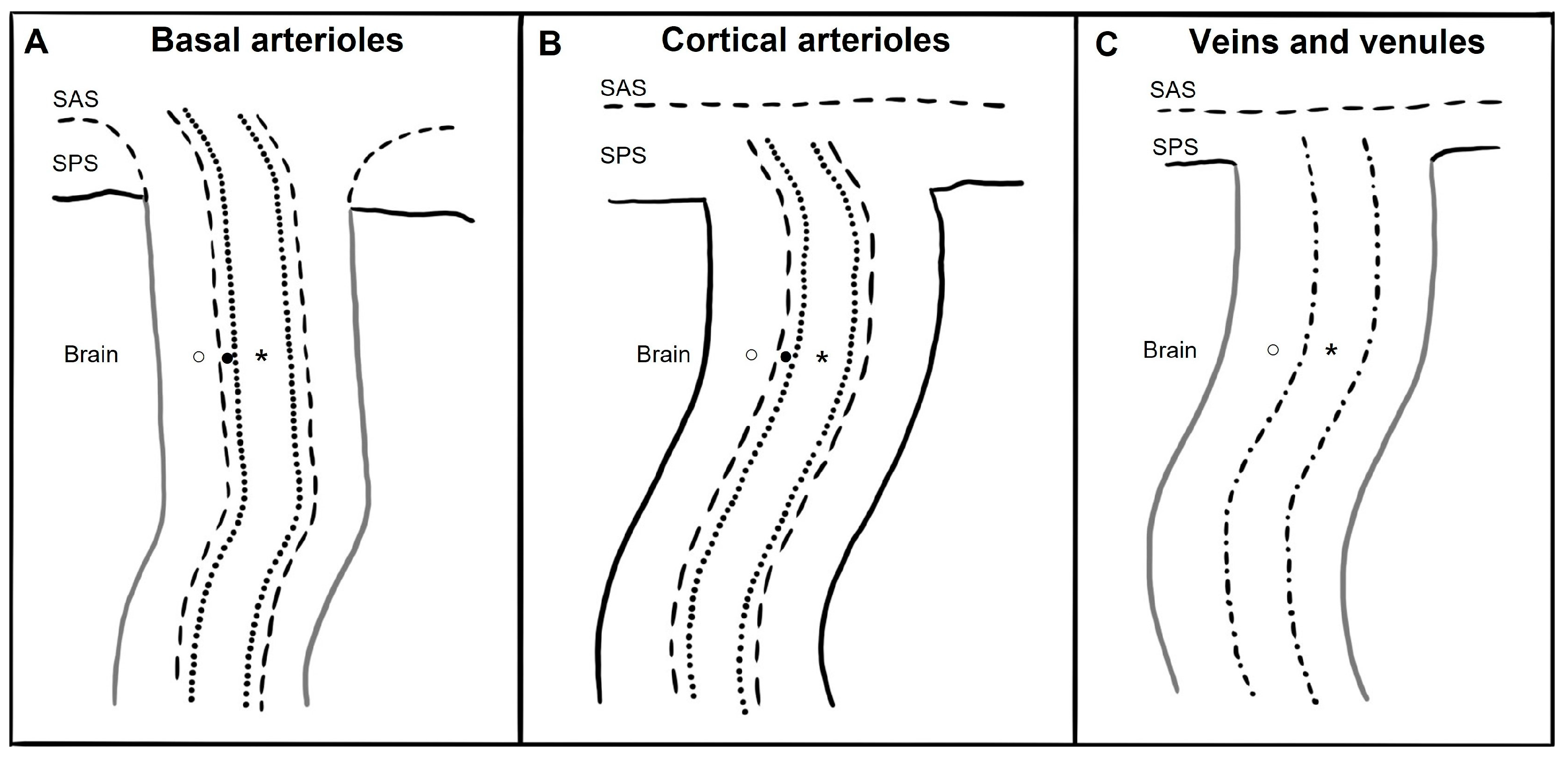
2. Anatomy
3. Imaging
4. Quantification
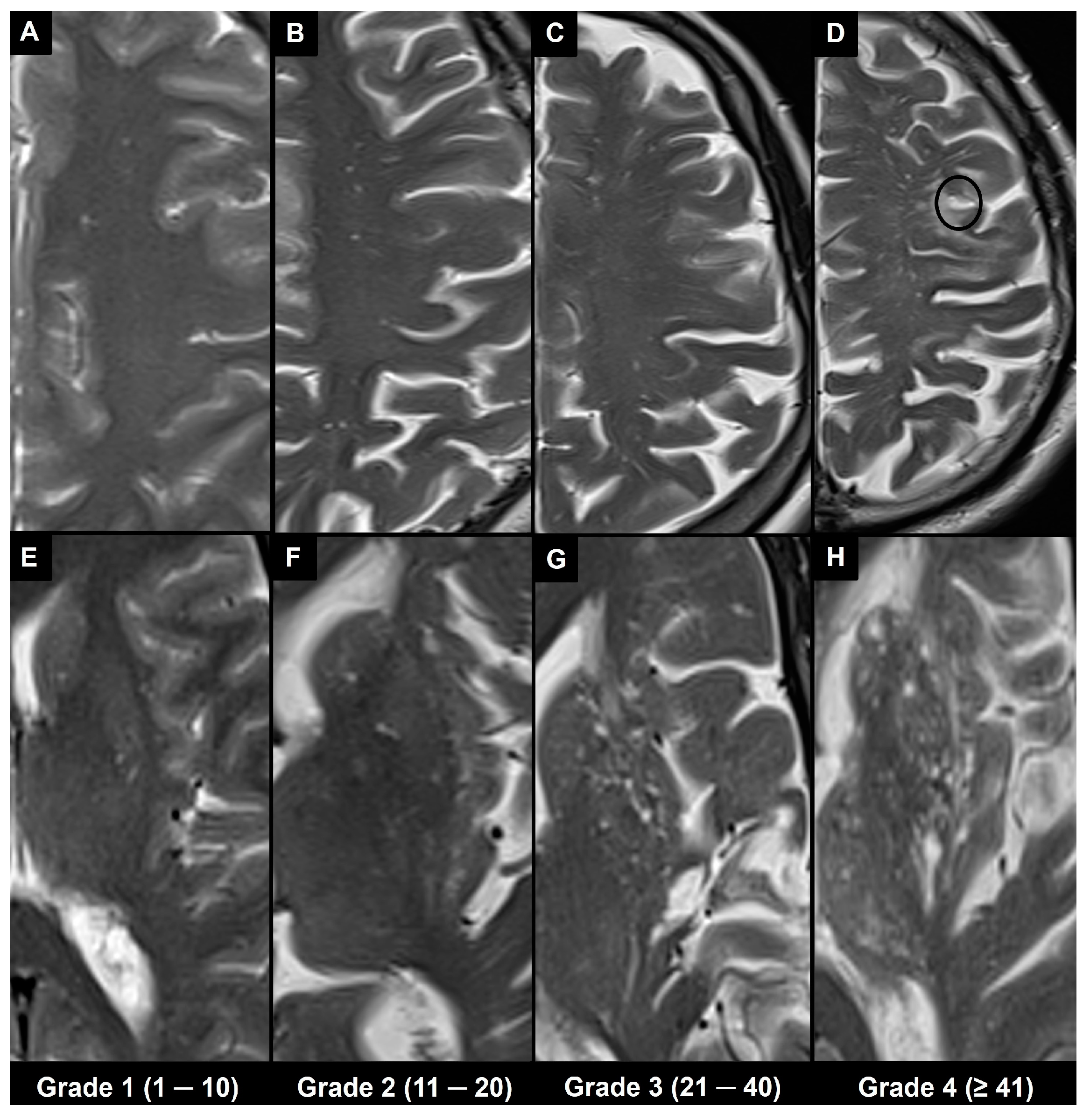
4.1. Visual Scoring
4.2. Automatic and Semi-Automatic Segmentation and Morphometry
5. Associations
5.1. Physiological
5.2. Pathological
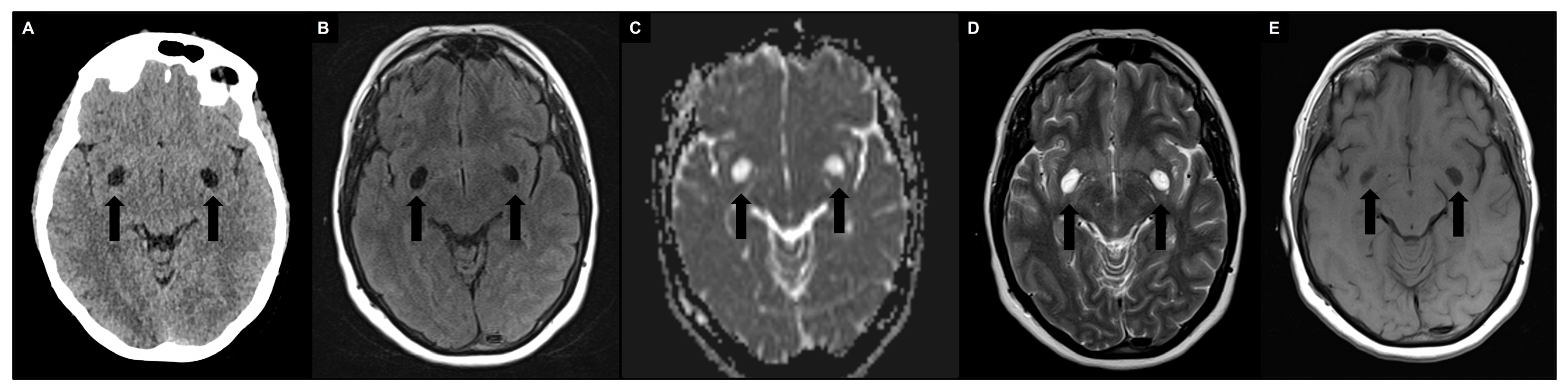
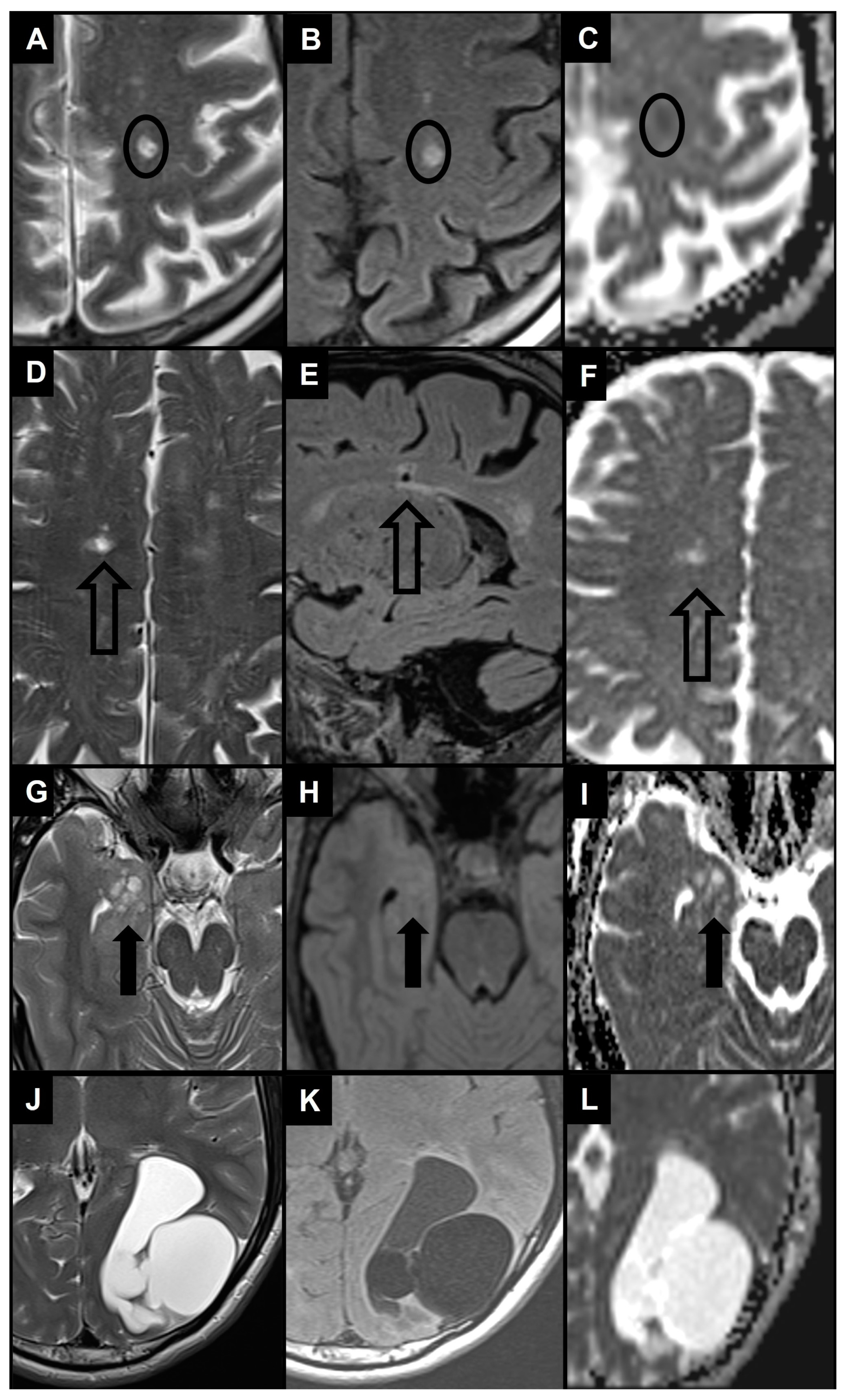
6. Differential Diagnosis
6.1. Recent Small Subcortical Infarct
6.2. Lacune of Presumed Vascular Origin
6.3. WMH
6.4. Benign Intracranial Cysts
6.5. Neoplastic Intracranial Cysts
6.6. Vascular and Inflammatory Cysts
6.7. Infectious Cysts
6.8. Inherited Cysts
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wardlaw, J.M.; Benveniste, H.; Nedergaard, M.; Zlokovic, B.V.; Mestre, H.; Lee, H.; Doubal, F.N.; Brown, R.; Ramirez, J.; MacIntosh, B.J.; et al. Perivascular Spaces in the Brain: Anatomy, Physiology and Pathology. Nat. Rev. Neurol. 2020, 16, 137–153. [Google Scholar] [CrossRef] [PubMed]
- Robin, C. Recherches Sur Quelques Particularites de La Structure Des Capillaires de l’encephale. J. Physiol. Homme Anim. 1859, 2, 537–548. [Google Scholar]
- Virchow, R. Ueber die Erweiterung kleinerer Gefäfse. Arch. Für Pathol. Anat. Physiol. Für Klin. Med. 1851, 3, 427–462. [Google Scholar] [CrossRef]
- Iliff, J.J.; Wang, M.; Liao, Y.; Plogg, B.A.; Peng, W.; Gundersen, G.A.; Benveniste, H.; Vates, G.E.; Deane, R.; Goldman, S.A.; et al. A Paravascular Pathway Facilitates CSF Flow through the Brain Parenchyma and the Clearance of Interstitial Solutes, Including Amyloid β. Sci. Transl. Med. 2012, 4, 147ra111. [Google Scholar] [CrossRef] [PubMed]
- Gouveia-Freitas, K.; Bastos-Leite, A.J. Perivascular Spaces and Brain Waste Clearance Systems: Relevance for Neurodegenerative and Cerebrovascular Pathology. Neuroradiology 2021, 63, 1581–1597. [Google Scholar] [CrossRef]
- Jessen, N.A.; Munk, A.S.F.; Lundgaard, I.; Nedergaard, M. The Glymphatic System: A Beginner’s Guide. Neurochem. Res. 2015, 40, 2583–2599. [Google Scholar] [CrossRef]
- Barua, N.U.; Gill, S.S.; Love, S. Convection-Enhanced Drug Delivery to the Brain: Therapeutic Potential and Neuropathological Considerations. Brain Pathol. Zur. Switz. 2014, 24, 117–127. [Google Scholar] [CrossRef]
- Parillo, M.; Vertulli, D.; Mallio, C.A.; Quattrocchi, C.C. Imaging Findings in Carcinomatous Encephalitis Secondary to Malignant Melanoma. Egypt. J. Neurol. Psychiatry Neurosurg. 2023, 59, 76. [Google Scholar] [CrossRef]
- Weller, R.O.; Hawkes, C.A.; Kalaria, R.N.; Werring, D.J.; Carare, R.O. White Matter Changes in Dementia: Role of Impaired Drainage of Interstitial Fluid. Brain Pathol. Zur. Switz. 2015, 25, 63–78. [Google Scholar] [CrossRef]
- Absinta, M.; Ha, S.-K.; Nair, G.; Sati, P.; Luciano, N.J.; Palisoc, M.; Louveau, A.; Zaghloul, K.A.; Pittaluga, S.; Kipnis, J.; et al. Human and Nonhuman Primate Meninges Harbor Lymphatic Vessels That Can Be Visualized Noninvasively by MRI. eLife 2017, 6, e29738. [Google Scholar] [CrossRef]
- Bouvy, W.H.; Biessels, G.J.; Kuijf, H.J.; Kappelle, L.J.; Luijten, P.R.; Zwanenburg, J.J.M. Visualization of Perivascular Spaces and Perforating Arteries with 7 T Magnetic Resonance Imaging. Investig. Radiol. 2014, 49, 307–313. [Google Scholar] [CrossRef]
- Weller, R.O.; Djuanda, E.; Yow, H.-Y.; Carare, R.O. Lymphatic Drainage of the Brain and the Pathophysiology of Neurological Disease. Acta Neuropathol. 2009, 117, 1–14. [Google Scholar] [CrossRef]
- Ringstad, G.; Valnes, L.M.; Dale, A.M.; Pripp, A.H.; Vatnehol, S.-A.S.; Emblem, K.E.; Mardal, K.-A.; Eide, P.K. Brain-Wide Glymphatic Enhancement and Clearance in Humans Assessed with MRI. JCI Insight 2018, 3, e121537. [Google Scholar] [CrossRef]
- Eide, P.K.; Vatnehol, S.A.S.; Emblem, K.E.; Ringstad, G. Magnetic Resonance Imaging Provides Evidence of Glymphatic Drainage from Human Brain to Cervical Lymph Nodes. Sci. Rep. 2018, 8, 7194. [Google Scholar] [CrossRef] [PubMed]
- Roher, A.E.; Kuo, Y.-M.; Esh, C.; Knebel, C.; Weiss, N.; Kalback, W.; Luehrs, D.C.; Childress, J.L.; Beach, T.G.; Weller, R.O.; et al. Cortical and Leptomeningeal Cerebrovascular Amyloid and White Matter Pathology in Alzheimer’s Disease. Mol. Med. Camb. Mass. 2003, 9, 112–122. [Google Scholar] [CrossRef]
- Bakker, E.N.T.P.; Bacskai, B.J.; Arbel-Ornath, M.; Aldea, R.; Bedussi, B.; Morris, A.W.J.; Weller, R.O.; Carare, R.O. Lymphatic Clearance of the Brain: Perivascular, Paravascular and Significance for Neurodegenerative Diseases. Cell. Mol. Neurobiol. 2016, 36, 181–194. [Google Scholar] [CrossRef]
- Bacyinski, A.; Xu, M.; Wang, W.; Hu, J. The Paravascular Pathway for Brain Waste Clearance: Current Understanding, Significance and Controversy. Front. Neuroanat. 2017, 11, 101. [Google Scholar] [CrossRef]
- Tarasoff-Conway, J.M.; Carare, R.O.; Osorio, R.S.; Glodzik, L.; Butler, T.; Fieremans, E.; Axel, L.; Rusinek, H.; Nicholson, C.; Zlokovic, B.V.; et al. Clearance Systems in the Brain-Implications for Alzheimer Disease. Nat. Rev. Neurol. 2015, 11, 457–470. [Google Scholar] [CrossRef]
- Carare, R.O.; Bernardes-Silva, M.; Newman, T.A.; Page, A.M.; Nicoll, J.A.R.; Perry, V.H.; Weller, R.O. Solutes, but Not Cells, Drain from the Brain Parenchyma along Basement Membranes of Capillaries and Arteries: Significance for Cerebral Amyloid Angiopathy and Neuroimmunology. Neuropathol. Appl. Neurobiol. 2008, 34, 131–144. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, N.; Carare, R.O. Cerebral Vessels: An Overview of Anatomy, Physiology, and Role in the Drainage of Fluids and Solutes. Front. Neurol. 2020, 11, 611485. [Google Scholar] [CrossRef] [PubMed]
- George, I.C.; Arrighi-Allisan, A.; Delman, B.N.; Balchandani, P.; Horng, S.; Feldman, R. A Novel Method to Measure Venular Perivascular Spaces in Patients with MS on 7T MRI. AJNR Am. J. Neuroradiol. 2021, 42, 1069–1072. [Google Scholar] [CrossRef] [PubMed]
- Jochems, A.C.C.; Blair, G.W.; Stringer, M.S.; Thrippleton, M.J.; Clancy, U.; Chappell, F.M.; Brown, R.; Jaime Garcia, D.; Hamilton, O.K.L.; Morgan, A.G.; et al. Relationship Between Venules and Perivascular Spaces in Sporadic Small Vessel Diseases. Stroke 2020, 51, 1503–1506. [Google Scholar] [CrossRef] [PubMed]
- Brown, W.R.; Moody, D.M.; Challa, V.R.; Thore, C.R.; Anstrom, J.A. Venous Collagenosis and Arteriolar Tortuosity in Leukoaraiosis. J. Neurol. Sci. 2002, 203–204, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Barisano, G.; Lynch, K.M.; Sibilia, F.; Lan, H.; Shih, N.-C.; Sepehrband, F.; Choupan, J. Imaging Perivascular Space Structure and Function Using Brain MRI. NeuroImage 2022, 257, 119329. [Google Scholar] [CrossRef] [PubMed]
- Montagne, A.; Nikolakopoulou, A.M.; Zhao, Z.; Sagare, A.P.; Si, G.; Lazic, D.; Barnes, S.R.; Daianu, M.; Ramanathan, A.; Go, A.; et al. Pericyte Degeneration Causes White Matter Dysfunction in the Mouse Central Nervous System. Nat. Med. 2018, 24, 326–337. [Google Scholar] [CrossRef] [PubMed]
- Perosa, V.; Oltmer, J.; Munting, L.P.; Freeze, W.M.; Auger, C.A.; Scherlek, A.A.; van der Kouwe, A.J.; Iglesias, J.E.; Atzeni, A.; Bacskai, B.J.; et al. Perivascular Space Dilation Is Associated with Vascular Amyloid-β Accumulation in the Overlying Cortex. Acta Neuropathol. 2022, 143, 331–348. [Google Scholar] [CrossRef] [PubMed]
- Oztürk, M.H.; Aydingöz, U. Comparison of MR Signal Intensities of Cerebral Perivascular (Virchow-Robin) and Subarachnoid Spaces. J. Comput. Assist. Tomogr. 2002, 26, 902–904. [Google Scholar] [CrossRef]
- Naganawa, S.; Nakane, T.; Kawai, H.; Taoka, T. Differences in Signal Intensity and Enhancement on MR Images of the Perivascular Spaces in the Basal Ganglia versus Those in White Matter. Magn. Reson. Med. Sci. MRMS Off. J. Jpn. Soc. Magn. Reson. Med. 2018, 17, 301–307. [Google Scholar] [CrossRef]
- Wardlaw, J.M.; Smith, E.E.; Biessels, G.J.; Cordonnier, C.; Fazekas, F.; Frayne, R.; Lindley, R.I.; O’Brien, J.T.; Barkhof, F.; Benavente, O.R.; et al. Neuroimaging Standards for Research into Small Vessel Disease and Its Contribution to Ageing and Neurodegeneration. Lancet Neurol. 2013, 12, 822–838. [Google Scholar] [CrossRef]
- Yu, L.; Hu, X.; Li, H.; Zhao, Y. Perivascular Spaces, Glymphatic System and MR. Front. Neurol. 2022, 13, 844938. [Google Scholar] [CrossRef]
- Mallio, C.A.; Quattrocchi, C.C.; Rovira, À.; Parizel, P.M. Gadolinium Deposition Safety: Seeking the Patient’s Perspective. AJNR Am. J. Neuroradiol. 2020, 41, 944–946. [Google Scholar] [CrossRef] [PubMed]
- Parillo, M.; Mallio, C.A.; Van der Molen, A.J.; Rovira, À.; Ramalho, J.; Ramalho, M.; Gianolio, E.; Karst, U.; Radbruch, A.; Stroomberg, G.; et al. Skin Toxicity after Exposure to Gadolinium-Based Contrast Agents in Normal Renal Function, Using Clinical Approved Doses: Current Status of Preclinical and Clinical Studies. Investig. Radiol. 2023, 58, 530–538. [Google Scholar] [CrossRef] [PubMed]
- Barisano, G.; Sheikh-Bahaei, N.; Law, M.; Toga, A.W.; Sepehrband, F. Body Mass Index, Time of Day and Genetics Affect Perivascular Spaces in the White Matter. J. Cereb. Blood Flow. Metab. Off. J. Int. Soc. Cereb. Blood Flow. Metab. 2021, 41, 1563–1578. [Google Scholar] [CrossRef] [PubMed]
- Heier, L.A.; Bauer, C.J.; Schwartz, L.; Zimmerman, R.D.; Morgello, S.; Deck, M.D. Large Virchow-Robin Spaces: MR-Clinical Correlation. AJNR Am. J. Neuroradiol. 1989, 10, 929–936. [Google Scholar]
- Kwee, R.M.; Kwee, T.C. Virchow-Robin Spaces at MR Imaging. Radiogr. Rev. Publ. Radiol. Soc. N. Am. Inc. 2007, 27, 1071–1086. [Google Scholar] [CrossRef]
- Salzman, K.L.; Osborn, A.G.; House, P.; Jinkins, J.R.; Ditchfield, A.; Cooper, J.A.; Weller, R.O. Giant Tumefactive Perivascular Spaces. AJNR Am. J. Neuroradiol. 2005, 26, 298–305. [Google Scholar]
- Barisano, G. Neuroimaging Aspects and Clinical Significance of Giant Perivascular Spaces in the Brain. Precis. Cancer Med. 2022, 5, 31. [Google Scholar] [CrossRef]
- Poirier, J.; Barbizet, J.; Gaston, A.; Meyrignac, C. [Thalamic dementia. Expansive lacunae of the thalamo-paramedian mesencephalic area. Hydrocephalus caused by stenosis of the aqueduct of Sylvius]. Rev. Neurol. 1983, 139, 349–358. [Google Scholar]
- Kanamalla, U.S.; Calabrò, F.; Jinkins, J.R. Cavernous Dilatation of Mesencephalic Virchow-Robin Spaces with Obstructive Hydrocephalus. Neuroradiology 2000, 42, 881–884. [Google Scholar] [CrossRef] [PubMed]
- Rudie, J.D.; Rauschecker, A.M.; Nabavizadeh, S.A.; Mohan, S. Neuroimaging of Dilated Perivascular Spaces: From Benign and Pathologic Causes to Mimics. J. Neuroimaging Off. J. Am. Soc. Neuroimaging 2018, 28, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Papayannis, C.E.; Saidon, P.; Rugilo, C.A.; Hess, D.; Rodriguez, G.; Sica, R.E.P.; Rey, R.C. Expanding Virchow Robin Spaces in the Midbrain Causing Hydrocephalus. AJNR Am. J. Neuroradiol. 2003, 24, 1399–1403. [Google Scholar]
- Loh, D.D.L.; Swaminathan, S.K. Tumefactive Perivascular Spaces Causing Obstructive Hydrocephalus. Radiology 2023, 307, e221724. [Google Scholar] [CrossRef] [PubMed]
- Kwee, R.M.; Kwee, T.C. Tumefactive Virchow-Robin Spaces. Eur. J. Radiol. 2019, 111, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Cheraya, G.; Bajaj, S.; Sharma, S.; Gandhi, D.; Shah, J.; Parikh, N.; Gupta, N. Giant Perivascular Spaces in Brain: Case Report with a Comprehensive Literature Review. Precis. Cancer Med. 2022, 5, 29. [Google Scholar] [CrossRef]
- Lakhani, D.A.; Joseph, J. Giant Tumefactive Perivascular Spaces. Radiology 2023, 307, 222559. [Google Scholar] [CrossRef]
- Rawal, S.; Croul, S.E.; Willinsky, R.A.; Tymianski, M.; Krings, T. Subcortical Cystic Lesions within the Anterior Superior Temporal Gyrus: A Newly Recognized Characteristic Location for Dilated Perivascular Spaces. AJNR Am. J. Neuroradiol. 2014, 35, 317–322. [Google Scholar] [CrossRef]
- Lim, A.T.; Chandra, R.V.; Trost, N.M.; McKelvie, P.A.; Stuckey, S.L. Large Anterior Temporal Virchow-Robin Spaces: Unique MR Imaging Features. Neuroradiology 2015, 57, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Drenthen, G.S.; Elschot, E.P.; van der Knaap, N.; Uher, D.; Voorter, P.H.M.; Backes, W.H.; Jansen, J.F.A.; van der Thiel, M.M. Imaging Interstitial Fluid with MRI: A Narrative Review on the Associations of Altered Interstitial Fluid with Vascular and Neurodegenerative Abnormalities. J. Magn. Reson. Imaging JMRI, 2023; epub ahead of print. [Google Scholar] [CrossRef]
- Potter, G.M.; Chappell, F.M.; Morris, Z.; Wardlaw, J.M. Cerebral Perivascular Spaces Visible on Magnetic Resonance Imaging: Development of a Qualitative Rating Scale and Its Observer Reliability. Cerebrovasc. Dis. Basel Switz. 2015, 39, 224–231. [Google Scholar] [CrossRef]
- Zhang, C.; Chen, Q.; Wang, Y.; Zhao, X.; Wang, C.; Liu, L.; Pu, Y.; Zou, X.; Du, W.; Pan, Y.; et al. Risk Factors of Dilated Virchow-Robin Spaces Are Different in Various Brain Regions. PLoS ONE 2014, 9, e105505. [Google Scholar] [CrossRef]
- Ding, J.; Sigurðsson, S.; Jónsson, P.V.; Eiriksdottir, G.; Charidimou, A.; Lopez, O.L.; van Buchem, M.A.; Guðnason, V.; Launer, L.J. Large Perivascular Spaces Visible on Magnetic Resonance Imaging, Cerebral Small Vessel Disease Progression, and Risk of Dementia: The Age, Gene/Environment Susceptibility-Reykjavik Study. JAMA Neurol. 2017, 74, 1105–1112. [Google Scholar] [CrossRef]
- Moses, J.; Sinclair, B.; Law, M.; O’Brien, T.J.; Vivash, L. Automated Methods for Detecting and Quantitation of Enlarged Perivascular Spaces on MRI. J. Magn. Reson. Imaging JMRI 2023, 57, 11–24. [Google Scholar] [CrossRef]
- Zong, X.; Park, S.H.; Shen, D.; Lin, W. Visualization of Perivascular Spaces in the Human Brain at 7T: Sequence Optimization and Morphology Characterization. NeuroImage 2016, 125, 895–902. [Google Scholar] [CrossRef]
- Boespflug, E.L.; Schwartz, D.L.; Lahna, D.; Pollock, J.; Iliff, J.J.; Kaye, J.A.; Rooney, W.; Silbert, L.C. MR Imaging-Based Multimodal Autoidentification of Perivascular Spaces (mMAPS): Automated Morphologic Segmentation of Enlarged Perivascular Spaces at Clinical Field Strength. Radiology 2018, 286, 632–642. [Google Scholar] [CrossRef] [PubMed]
- Ballerini, L.; Lovreglio, R.; Valdés Hernández, M.D.C.; Ramirez, J.; MacIntosh, B.J.; Black, S.E.; Wardlaw, J.M. Perivascular Spaces Segmentation in Brain MRI Using Optimal 3D Filtering. Sci. Rep. 2018, 8, 2132. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Gao, Y.; Park, S.H.; Zong, X.; Lin, W.; Shen, D. Structured Learning for 3-D Perivascular Space Segmentation Using Vascular Features. IEEE Trans. Biomed. Eng. 2017, 64, 2803–2812. [Google Scholar] [CrossRef] [PubMed]
- Lian, C.; Zhang, J.; Liu, M.; Zong, X.; Hung, S.-C.; Lin, W.; Shen, D. Multi-Channel Multi-Scale Fully Convolutional Network for 3D Perivascular Spaces Segmentation in 7T MR Images. Med. Image Anal. 2018, 46, 106–117. [Google Scholar] [CrossRef] [PubMed]
- Sudre, C.H.; Anson, B.G.; Ingala, S.; Lane, C.D.; Jimenez, D.; Haider, L.; Varsavsky, T.; Smith, L.; Ourselin, S.; Jäger, R.H.; et al. 3D Multirater RCNN for Multimodal Multiclass Detection and Characterisation of Extremely Small Objects. In Proceedings of the 2nd International Conference on Medical Imaging with Deep Learning, PMLR, London, UK, 8–10 July 2019; pp. 447–456. [Google Scholar]
- Sepehrband, F.; Barisano, G.; Sheikh-Bahaei, N.; Cabeen, R.P.; Choupan, J.; Law, M.; Toga, A.W. Image Processing Approaches to Enhance Perivascular Space Visibility and Quantification Using MRI. Sci. Rep. 2019, 9, 12351. [Google Scholar] [CrossRef] [PubMed]
- González-Castro, V.; Valdés Hernández, M.D.C.; Chappell, F.M.; Armitage, P.A.; Makin, S.; Wardlaw, J.M. Reliability of an Automatic Classifier for Brain Enlarged Perivascular Spaces Burden and Comparison with Human Performance. Clin. Sci. 2017, 131, 1465–1481. [Google Scholar] [CrossRef] [PubMed]
- Dubost, F.; Yilmaz, P.; Adams, H.; Bortsova, G.; Ikram, M.A.; Niessen, W.; Vernooij, M.; de Bruijne, M. Enlarged Perivascular Spaces in Brain MRI: Automated Quantification in Four Regions. NeuroImage 2019, 185, 534–544. [Google Scholar] [CrossRef] [PubMed]
- Dubost, F.; Adams, H.; Bortsova, G.; Ikram, M.A.; Niessen, W.; Vernooij, M.; de Bruijne, M. 3D Regression Neural Network for the Quantification of Enlarged Perivascular Spaces in Brain MRI. Med. Image Anal. 2019, 51, 89–100. [Google Scholar] [CrossRef]
- Dubost, F.; Adams, H.; Yilmaz, P.; Bortsova, G.; Tulder, G.; van Ikram, M.A.; Niessen, W.; Vernooij, M.W.; Bruijne, M. de Weakly Supervised Object Detection with 2D and 3D Regression Neural Networks. Med. Image Anal. 2020, 65, 101767. [Google Scholar] [CrossRef]
- Williamson, B.J.; Khandwala, V.; Wang, D.; Maloney, T.; Sucharew, H.; Horn, P.; Haverbusch, M.; Alwell, K.; Gangatirkar, S.; Mahammedi, A.; et al. Automated Grading of Enlarged Perivascular Spaces in Clinical Imaging Data of an Acute Stroke Cohort Using an Interpretable, 3D Deep Learning Framework. Sci. Rep. 2022, 12, 788. [Google Scholar] [CrossRef]
- Piantino, J.; Boespflug, E.L.; Schwartz, D.L.; Luther, M.; Morales, A.M.; Lin, A.; Fossen, R.V.; Silbert, L.; Nagel, B.J. Characterization of MR Imaging-Visible Perivascular Spaces in the White Matter of Healthy Adolescents at 3T. AJNR Am. J. Neuroradiol. 2020, 41, 2139–2145. [Google Scholar] [CrossRef] [PubMed]
- Francis, F.; Ballerini, L.; Wardlaw, J.M. Perivascular Spaces and Their Associations with Risk Factors, Clinical Disorders and Neuroimaging Features: A Systematic Review and Meta-Analysis. Int. J. Stroke Off. J. Int. Stroke Soc. 2019, 14, 359–371. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.G.; Shin, N.-Y.; Nam, Y.; Yun, E.; Yoon, U.; Lee, H.S.; Ahn, K.J. MRI-Visible Dilated Perivascular Space in the Brain by Age: The Human Connectome Project. Radiology 2023, 306, e213254. [Google Scholar] [CrossRef] [PubMed]
- Barisano, G.; Sepehrband, F.; Collins, H.R.; Jillings, S.; Jeurissen, B.; Taylor, J.A.; Schoenmaekers, C.; De Laet, C.; Rukavishnikov, I.; Nosikova, I.; et al. The Effect of Prolonged Spaceflight on Cerebrospinal Fluid and Perivascular Spaces of Astronauts and Cosmonauts. Proc. Natl. Acad. Sci. USA 2022, 119, e2120439119. [Google Scholar] [CrossRef] [PubMed]
- Okar, S.V.; Hu, F.; Shinohara, R.T.; Beck, E.S.; Reich, D.S.; Ineichen, B.V. The Etiology and Evolution of Magnetic Resonance Imaging-Visible Perivascular Spaces: Systematic Review and Meta-Analysis. Front. Neurosci. 2023, 17, 1038011. [Google Scholar] [CrossRef] [PubMed]
- Kikuta, J.; Kamagata, K.; Takabayashi, K.; Taoka, T.; Yokota, H.; Andica, C.; Wada, A.; Someya, Y.; Tamura, Y.; Kawamori, R.; et al. An Investigation of Water Diffusivity Changes along the Perivascular Space in Elderly Subjects with Hypertension. AJNR Am. J. Neuroradiol. 2022, 43, 48–55. [Google Scholar] [CrossRef]
- Lau, K.-K.; Li, L.; Lovelock, C.E.; Zamboni, G.; Chan, T.-T.; Chiang, M.-F.; Lo, K.-T.; Küker, W.; Mak, H.K.-F.; Rothwell, P.M. Clinical Correlates, Ethnic Differences, and Prognostic Implications of Perivascular Spaces in Transient Ischemic Attack and Ischemic Stroke. Stroke 2017, 48, 1470–1477. [Google Scholar] [CrossRef]
- Toh, C.H.; Siow, T.Y. Glymphatic Dysfunction in Patients With Ischemic Stroke. Front. Aging Neurosci. 2021, 13, 756249. [Google Scholar] [CrossRef]
- Zhang, C.; Sha, J.; Cai, L.; Xia, Y.; Li, D.; Zhao, H.; Meng, C.; Xu, K. Evaluation of the Glymphatic System Using the DTI-ALPS Index in Patients with Spontaneous Intracerebral Haemorrhage. Oxid. Med. Cell. Longev. 2022, 2022, 2694316. [Google Scholar] [CrossRef]
- Yao, M.; Hervé, D.; Jouvent, E.; Duering, M.; Reyes, S.; Godin, O.; Guichard, J.P.; Dichgans, M.; Chabriat, H. Dilated Perivascular Spaces in Small-Vessel Disease: A Study in CADASIL. Cerebrovasc. Dis. Basel Switz. 2014, 37, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Lasaponara, S.; Mauro, F.; Carducci, F.; Paoletti, P.; Tombini, M.; Quattrocchi, C.C.; Mallio, C.A.; Errante, Y.; Scarciolla, L.; Ben-Soussan, T.D. Increased Alpha Band Functional Connectivity Following the Quadrato Motor Training: A Longitudinal Study. Front. Hum. Neurosci. 2017, 11, 282. [Google Scholar] [CrossRef] [PubMed]
- Cai, K.; Tain, R.; Das, S.; Damen, F.C.; Sui, Y.; Valyi-Nagy, T.; Elliott, M.A.; Zhou, X.J. The Feasibility of Quantitative MRI of Perivascular Spaces at 7T. J. Neurosci. Methods 2015, 256, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, J.; Berezuk, C.; McNeely, A.A.; Scott, C.J.M.; Gao, F.; Black, S.E. Visible Virchow-Robin Spaces on Magnetic Resonance Imaging of Alzheimer’s Disease Patients and Normal Elderly from the Sunnybrook Dementia Study. J. Alzheimers Dis. JAD 2015, 43, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, G.; Kim, H.J.; Fox, Z.; Jäger, H.R.; Wilson, D.; Charidimou, A.; Na, H.K.; Na, D.L.; Seo, S.W.; Werring, D.J. MRI-Visible Perivascular Space Location Is Associated with Alzheimer’s Disease Independently of Amyloid Burden. Brain J. Neurol. 2017, 140, 1107–1116. [Google Scholar] [CrossRef] [PubMed]
- Steward, C.E.; Venkatraman, V.K.; Lui, E.; Malpas, C.B.; Ellis, K.A.; Cyarto, E.V.; Vivash, L.; O’Brien, T.J.; Velakoulis, D.; Ames, D.; et al. Assessment of the DTI-ALPS Parameter Along the Perivascular Space in Older Adults at Risk of Dementia. J. Neuroimaging Off. J. Am. Soc. Neuroimaging 2021, 31, 569–578. [Google Scholar] [CrossRef] [PubMed]
- Sepehrband, F.; Barisano, G.; Sheikh-Bahaei, N.; Choupan, J.; Cabeen, R.P.; Lynch, K.M.; Crawford, M.S.; Lan, H.; Mack, W.J.; Chui, H.C.; et al. Volumetric Distribution of Perivascular Space in Relation to Mild Cognitive Impairment. Neurobiol. Aging 2021, 99, 28–43. [Google Scholar] [CrossRef]
- Hilal, S.; Tan, C.S.; Adams, H.H.H.; Habes, M.; Mok, V.; Venketasubramanian, N.; Hofer, E.; Ikram, M.K.; Abrigo, J.; Vernooij, M.W.; et al. Enlarged Perivascular Spaces and Cognition: A Meta-Analysis of 5 Population-Based Studies. Neurology 2018, 91, e832–e842. [Google Scholar] [CrossRef]
- Charidimou, A.; Jaunmuktane, Z.; Baron, J.-C.; Burnell, M.; Varlet, P.; Peeters, A.; Xuereb, J.; Jäger, R.; Brandner, S.; Werring, D.J. White Matter Perivascular Spaces: An MRI Marker in Pathology-Proven Cerebral Amyloid Angiopathy? Neurology 2014, 82, 57–62. [Google Scholar] [CrossRef]
- van Veluw, S.J.; Biessels, G.J.; Bouvy, W.H.; Spliet, W.G.; Zwanenburg, J.J.; Luijten, P.R.; Macklin, E.A.; Rozemuller, A.J.; Gurol, M.E.; Greenberg, S.M.; et al. Cerebral Amyloid Angiopathy Severity Is Linked to Dilation of Juxtacortical Perivascular Spaces. J. Cereb. Blood Flow. Metab. Off. J. Int. Soc. Cereb. Blood Flow. Metab. 2016, 36, 576–580. [Google Scholar] [CrossRef]
- Boulouis, G.; Charidimou, A.; Pasi, M.; Roongpiboonsopit, D.; Xiong, L.; Auriel, E.; van Etten, E.S.; Martinez-Ramirez, S.; Ayres, A.; Vashkevich, A.; et al. Hemorrhage Recurrence Risk Factors in Cerebral Amyloid Angiopathy: Comparative Analysis of the Overall Small Vessel Disease Severity Score versus Individual Neuroimaging Markers. J. Neurol. Sci. 2017, 380, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Shen, T.; Yue, Y.; Zhao, S.; Xie, J.; Chen, Y.; Tian, J.; Lv, W.; Lo, C.-Y.Z.; Hsu, Y.-C.; Kober, T.; et al. The Role of Brain Perivascular Space Burden in Early-Stage Parkinson’s Disease. NPJ Park. Dis. 2021, 7, 12. [Google Scholar] [CrossRef] [PubMed]
- Donahue, E.K.; Murdos, A.; Jakowec, M.W.; Sheikh-Bahaei, N.; Toga, A.W.; Petzinger, G.M.; Sepehrband, F. Global and Regional Changes in Perivascular Space in Idiopathic and Familial Parkinson’s Disease. Mov. Disord. Off. J. Mov. Disord. Soc. 2021, 36, 1126–1136. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-L.; Chen, P.-C.; Lu, C.-H.; Tsai, N.-W.; Yu, C.-C.; Chou, K.-H.; Lai, Y.-R.; Taoka, T.; Lin, W.-C. Associations among Cognitive Functions, Plasma DNA, and Diffusion Tensor Image along the Perivascular Space (DTI-ALPS) in Patients with Parkinson’s Disease. Oxid. Med. Cell. Longev. 2021, 2021, 4034509. [Google Scholar] [CrossRef]
- Conforti, R.; Cirillo, M.; Saturnino, P.P.; Gallo, A.; Sacco, R.; Negro, A.; Paccone, A.; Caiazzo, G.; Bisecco, A.; Bonavita, S.; et al. Dilated Virchow-Robin Spaces and Multiple Sclerosis: 3 T Magnetic Resonance Study. Radiol. Med. 2014, 119, 408–414. [Google Scholar] [CrossRef]
- Etemadifar, M.; Hekmatnia, A.; Tayari, N.; Kazemi, M.; Ghazavi, A.; Akbari, M.; Maghzi, A.-H. Features of Virchow-Robin Spaces in Newly Diagnosed Multiple Sclerosis Patients. Eur. J. Radiol. 2011, 80, e104–e108. [Google Scholar] [CrossRef] [PubMed]
- Wuerfel, J.; Haertle, M.; Waiczies, H.; Tysiak, E.; Bechmann, I.; Wernecke, K.D.; Zipp, F.; Paul, F. Perivascular Spaces—MRI Marker of Inflammatory Activity in the Brain? Brain J. Neurol. 2008, 131, 2332–2340. [Google Scholar] [CrossRef]
- Kilsdonk, I.D.; Steenwijk, M.D.; Pouwels, P.J.W.; Zwanenburg, J.J.M.; Visser, F.; Luijten, P.R.; Geurts, J.J.G.; Barkhof, F.; Wattjes, M.P. Perivascular Spaces in MS Patients at 7 Tesla MRI: A Marker of Neurodegeneration? Mult. Scler. Houndmills Basingstoke Engl. 2015, 21, 155–162. [Google Scholar] [CrossRef]
- Miyata, M.; Kakeda, S.; Iwata, S.; Nakayamada, S.; Ide, S.; Watanabe, K.; Moriya, J.; Tanaka, Y.; Korogi, Y. Enlarged Perivascular Spaces Are Associated with the Disease Activity in Systemic Lupus Erythematosus. Sci. Rep. 2017, 7, 12566. [Google Scholar] [CrossRef]
- Di Costanzo, A.; Di Salle, F.; Santoro, L.; Bonavita, V.; Tedeschi, G. Dilated Virchow-Robin Spaces in Myotonic Dystrophy: Frequency, Extent and Significance. Eur. Neurol. 2001, 46, 131–139. [Google Scholar] [CrossRef]
- Taber, K.H.; Shaw, J.B.; Loveland, K.A.; Pearson, D.A.; Lane, D.M.; Hayman, L.A. Accentuated Virchow-Robin Spaces in the Centrum Semiovale in Children with Autistic Disorder. J. Comput. Assist. Tomogr. 2004, 28, 263–268. [Google Scholar] [CrossRef]
- Ozato, N.; Saitou, S.; Yamaguchi, T.; Katashima, M.; Misawa, M.; Jung, S.; Mori, K.; Kawada, H.; Katsuragi, Y.; Mikami, T.; et al. Association between Visceral Fat and Brain Structural Changes or Cognitive Function. Brain Sci. 2021, 11, 1036. [Google Scholar] [CrossRef]
- Aribisala, B.S.; Riha, R.L.; Valdes Hernandez, M.; Muñoz Maniega, S.; Cox, S.; Radakovic, R.; Taylor, A.; Pattie, A.; Corley, J.; Redmond, P.; et al. Sleep and Brain Morphological Changes in the Eighth Decade of Life. Sleep. Med. 2020, 65, 152–158. [Google Scholar] [CrossRef]
- Song, T.-J.; Park, J.-H.; Choi, K.H.; Chang, Y.; Moon, J.; Kim, J.-H.; Choi, Y.; Kim, Y.-J.; Lee, H.W. Moderate-to-Severe Obstructive Sleep Apnea Is Associated with Cerebral Small Vessel Disease. Sleep. Med. 2017, 30, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Månberg, A.; Skene, N.; Sanders, F.; Trusohamn, M.; Remnestål, J.; Szczepińska, A.; Aksoylu, I.S.; Lönnerberg, P.; Ebarasi, L.; Wouters, S.; et al. Altered Perivascular Fibroblast Activity Precedes ALS Disease Onset. Nat. Med. 2021, 27, 640–646. [Google Scholar] [CrossRef] [PubMed]
- Lanfranconi, S.; Markus, H.S. COL4A1 Mutations as a Monogenic Cause of Cerebral Small Vessel Disease: A Systematic Review. Stroke 2010, 41, e513–e518. [Google Scholar] [CrossRef] [PubMed]
- Lynch, S.A.; Hall, K.; Precious, S.; Wilkies, A.O.; Hurst, J.A. Two Further Cases of Sener Syndrome: Frontonasal Dysplasia and Dilated Virchow-Robin Spaces. J. Med. Genet. 2000, 37, 466–470. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Habib, T.; Salimeen, M.; Pradhan, A.; Singh, M.; Wang, M.; Wu, F.; Zhang, Y.; Gao, L.; Yang, G.; et al. Quantification of Visible Virchow-Robin Spaces for Detecting the Functional Status of the Glymphatic System in Children with Newly Diagnosed Idiopathic Generalized Epilepsy. Seizure 2020, 78, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Chan, Y.L.; Deng, M.; Chen, Y.K.; Mok, V.; Wang, D.F.; Ungvari, G.S.; Chu, C.-W.W.; Tang, W.K. Enlarged Perivascular Spaces in the Centrum Semiovale Are Associated with Poststroke Depression: A 3-Month Prospective Study. J. Affect. Disord. 2018, 228, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Opel, R.A.; Christy, A.; Boespflug, E.L.; Weymann, K.B.; Case, B.; Pollock, J.M.; Silbert, L.C.; Lim, M.M. Effects of Traumatic Brain Injury on Sleep and Enlarged Perivascular Spaces. J. Cereb. Blood Flow. Metab. Off. J. Int. Soc. Cereb. Blood Flow. Metab. 2019, 39, 2258–2267. [Google Scholar] [CrossRef]
- Mahammedi, A.; Wang, L.L.; Williamson, B.J.; Khatri, P.; Kissela, B.; Sawyer, R.P.; Shatz, R.; Khandwala, V.; Vagal, A. Small Vessel Disease, a Marker of Brain Health: What the Radiologist Needs to Know. AJNR Am. J. Neuroradiol. 2022, 43, 650–660. [Google Scholar] [CrossRef] [PubMed]
- Cervantes-Arslanian, A.; Garcia, H.H.; Rapalino, O. Imaging of Infectious and Inflammatory Cystic Lesions of the Brain, a Narrative Review. Expert. Rev. Neurother. 2023, 23, 237–247. [Google Scholar] [CrossRef] [PubMed]
- Sharma, V.; Prabhash, K.; Noronha, V.; Tandon, N.; Joshi, A. A Systematic Approach to Diagnosis of Cystic Brain Lesions. South Asian J. Cancer 2013, 2, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Erkinjuntti, T.; Inzitari, D.; Pantoni, L.; Wallin, A.; Scheltens, P.; Rockwood, K.; Roman, G.C.; Chui, H.; Desmond, D.W. Research Criteria for Subcortical Vascular Dementia in Clinical Trials. J. Neural Transm. Suppl. 2000, 59, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, P.; Trippier, S.; Lawrence, A.J.; Lambert, C.; Zeestraten, E.; Williams, O.A.; Patel, B.; Morris, R.G.; Barrick, T.R.; MacKinnon, A.D.; et al. Lacunar Infarcts, but Not Perivascular Spaces, Are Predictors of Cognitive Decline in Cerebral Small-Vessel Disease. Stroke 2018, 49, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Robles, L.A.; Paez, J.M.; Ayala, D.; Boleaga-Duran, B. Intracranial Glioependymal (Neuroglial) Cysts: A Systematic Review. Acta Neurochir. 2018, 160, 1439–1449. [Google Scholar] [CrossRef] [PubMed]
- Altafulla, J.J.; Suh, S.; Bordes, S.; Prickett, J.; Iwanaga, J.; Loukas, M.; Dumont, A.S.; Tubbs, R.S. Choroidal Fissure and Choroidal Fissure Cysts: A Comprehensive Review. Anat. Cell Biol. 2020, 53, 121–125. [Google Scholar] [CrossRef]
- Yamashita, K.; Zong, X.; Hung, S.-C.; Lin, W.; Castillo, M. Hippocampal Sulcus Remnant: Common Finding in Nonelderly Adults on Ultra-High-Resolution 7T Magnetic Resonance Imaging. J. Comput. Assist. Tomogr. 2020, 44, 43–46. [Google Scholar] [CrossRef]
- Buffa, G.B.; Chaves, H.; Serra, M.M.; Stefanoff, N.I.; Gagliardo, A.S.; Yañez, P. Multinodular and Vacuolating Neuronal Tumor of the Cerebrum (MVNT): A Case Series and Review of the Literature. J. Neuroradiol. J. Neuroradiol. 2020, 47, 216–220. [Google Scholar] [CrossRef]
- Luzzi, S.; Elia, A.; Del Maestro, M.; Elbabaa, S.K.; Carnevale, S.; Guerrini, F.; Caulo, M.; Morbini, P.; Galzio, R. Dysembryoplastic Neuroepithelial Tumors: What You Need to Know. World Neurosurg. 2019, 127, 255–265. [Google Scholar] [CrossRef]
- Abergel, A.; Lacalm, A.; Massoud, M.; Massardier, J.; des Portes, V.; Guibaud, L. Expanding Porencephalic Cysts: Prenatal Imaging and Differential Diagnosis. Fetal Diagn. Ther. 2017, 41, 226–233. [Google Scholar] [CrossRef]
- Hinojosa-Rodríguez, M.; Harmony, T.; Carrillo-Prado, C.; Van Horn, J.D.; Irimia, A.; Torgerson, C.; Jacokes, Z. Clinical Neuroimaging in the Preterm Infant: Diagnosis and Prognosis. NeuroImage Clin. 2017, 16, 355–368. [Google Scholar] [CrossRef] [PubMed]
- Sarbu, N.; Shih, R.Y.; Oleaga, L.; Smirniotopoulos, J.G. RadioGraphics Update: White Matter Diseases with Radiologic-Pathologic Correlation. Radiogr. Rev. Publ. Radiol. Soc. N. Am. Inc. 2020, 40, E4–E7. [Google Scholar] [CrossRef] [PubMed]
- Lerner, A.; Shiroishi, M.S.; Zee, C.-S.; Law, M.; Go, J.L. Imaging of Neurocysticercosis. Neuroimaging Clin. N. Am. 2012, 22, 659–676. [Google Scholar] [CrossRef] [PubMed]
- Duarte, S.B.L.; Oshima, M.M.; do Amaral Mesquita, J.V.; do Nascimento, F.B.P.; de Azevedo, P.C.; Reis, F. Magnetic Resonance Imaging Findings in Central Nervous System Cryptococcosis: Comparison between Immunocompetent and Immunocompromised Patients. Radiol. Bras. 2017, 50, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Starkey, J.; Moritani, T.; Kirby, P. MRI of CNS Fungal Infections: Review of Aspergillosis to Histoplasmosis and Everything in Between. Clin. Neuroradiol. 2014, 24, 217–230. [Google Scholar] [CrossRef] [PubMed]
- Marcus, C.; Feizi, P.; Hogg, J.; Summerfield, H.; Castellani, R.; Sriwastava, S.; Marano, G.D. Imaging in Differentiating Cerebral Toxoplasmosis and Primary CNS Lymphoma with Special Focus on FDG PET/CT. AJR Am. J. Roentgenol. 2021, 216, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Masamed, R.; Meleis, A.; Lee, E.W.; Hathout, G.M. Cerebral Toxoplasmosis: Case Review and Description of a New Imaging Sign. Clin. Radiol. 2009, 64, 560–563. [Google Scholar] [CrossRef] [PubMed]
- Zafeiriou, D.I.; Batzios, S.P. Brain and Spinal MR Imaging Findings in Mucopolysaccharidoses: A Review. AJNR Am. J. Neuroradiol. 2013, 34, 5–13. [Google Scholar] [CrossRef]
- Matheus, M.G.; Castillo, M.; Smith, J.K.; Armao, D.; Towle, D.; Muenzer, J. Brain MRI Findings in Patients with Mucopolysaccharidosis Types I and II and Mild Clinical Presentation. Neuroradiology 2004, 46, 666–672. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Condition | Main PVS Burden Location | |
|---|---|---|
| Physiological | Aging [66,67] | Basal ganglia and centrum semiovale |
| Male sex [33] | Centrum semiovale | |
| Later time of day [33] | Basal ganglia and centrum semiovale | |
| Spaceflights [68] | Basal ganglia and centrum semiovale | |
| Pathological | Hypertension [66] | Basal ganglia |
| Cerebral small vessel disease [29,66] | Basal ganglia | |
| Alzheimer’s disease [15,76,77,78] | Centrum semiovale | |
| Cerebral amyloid angiopathy [82,83] | Centrum semiovale | |
| Parkinson’s disease [85,86] | Basal ganglia | |
| Multiple sclerosis [88,89,90,91] | Centrum semiovale | |
| Spaceflight-associated neuro-ocular syndrome [68] | Centrum semiovale | |
| High BMI/visceral fat [33] | Basal Ganglia | |
| Sleep dysfunction [96] | Centrum semiovale | |
| Obstructive sleep apnea [97] | Basal ganglia and centrum semiovale | |
| Myotonic dystrophy [93] | Centrum semiovale | |
| Amyotrophic lateral sclerosis [98] | Basal ganglia and centrum semiovale | |
| Systemic lupus erythematosus [92] | Centrum semiovale | |
| CADASIL [74] | Centrum semiovale | |
| Mutations in type IV collagen [99] | Basal ganglia and centrum semiovale | |
| Sener syndrome [100] | Centrum semiovale | |
| Pediatric idiopathic generalized epilepsy [101] | Centrum semiovale | |
| Autism spectrum disorders [94] | Centrum semiovale | |
| Depression [102] | Centrum semiovale |
| Features | PVS | Subcortical Infarct | Lacune | WMH | Giant PVS | Benign Intracranial Cysts | Neoplastic Intracranial Cysts | Vascular and Inflammatory Cysts | Infectious Cysts | Mucopolysaccharidosis |
|---|---|---|---|---|---|---|---|---|---|---|
| FLAIR | ↓↓ | ↑↑ | ↓↓ with ↑ rim | ↑↑ | ↓↓ with ↑ rim | ↓↓ (↑ in neurenteric cysts) | ↑↑with possible ↑ rim | ↓↓ with ↑ rim | Variable | ↓↓ with ↑ rim |
| T2 | ↑↑ | ↑↑ | ↑↑ | ↑ | ↑↑ | ↑↑ | ↑/↑↑ | ↑↑ | Variable | ↑↑ |
| T1 | ↓↓ | ↓↓ | ↓↓ | ↓ | ↓↓ | ↓↓ (↑ in neurenteric cysts) | ↓/↓↓ | ↓↓ | Variable | ↓↓ |
| Enhancement | - | - | - | - | - | - | ↑ of solid tissue | ↑ in active inflammation | Variable (eccentric target sign for neurotoxoplasmosis, cyst wall for neurocysticercosis) | - |
| DWI | - | Restricted | - | - | - | Restricted in epidermoid cyst | Restricted | - | Restricted in cryptococcosis | - |
| Size | ≤2 mm | ≤20 mm | 3–15 mm | ≥3 mm | ≥15 mm | ≥15 mm | ≥15 mm | ≥3 mm | ≥15 mm | ≥3 mm |
| Shape | Dot-like or tubular | Dot-like or tubular | Wedge | Rounded or irregular | Bizarre cystic configurations | Rounded | Bizarre cystic configurations (“bubbly” for DNET) | Bizarre in encephalomalacia, linear or ovoid in multiple sclerosis | Rounded or irregular | Dot-like or tubular |
| Location | Symmetric in white matter or lower basal ganglia | Subcortical territory of a perforating arteriole | Asymmetric in white matter or upper basal ganglia | Symmetric in periventricular white matter | Mesencephalothalamic region (type III), anterior superior temporal lobe (type IV) | Single intra-axial, subarachnoid or intraventricular | Single intra-axial | Encephalomalacia have connections with the subarachnoid space; perivenular distribution in multiple sclerosis | Multiple intra-axials, subarachnoids or intraventriculars | Basal ganglia, corpus callosum, and white matter |
| Other | - | - | - | - | - | - | Change in follow up | Clinical picture | Clinical picture | Clinical picture |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parillo, M.; Vaccarino, F.; Di Gennaro, G.; Kumar, S.; Van Goethem, J.; Beomonte Zobel, B.; Quattrocchi, C.C.; Parizel, P.M.; Mallio, C.A. Overview of the Current Knowledge and Conventional MRI Characteristics of Peri- and Para-Vascular Spaces. Brain Sci. 2024, 14, 138. https://doi.org/10.3390/brainsci14020138
Parillo M, Vaccarino F, Di Gennaro G, Kumar S, Van Goethem J, Beomonte Zobel B, Quattrocchi CC, Parizel PM, Mallio CA. Overview of the Current Knowledge and Conventional MRI Characteristics of Peri- and Para-Vascular Spaces. Brain Sciences. 2024; 14(2):138. https://doi.org/10.3390/brainsci14020138
Chicago/Turabian StyleParillo, Marco, Federica Vaccarino, Gianfranco Di Gennaro, Sumeet Kumar, Johan Van Goethem, Bruno Beomonte Zobel, Carlo Cosimo Quattrocchi, Paul M. Parizel, and Carlo Augusto Mallio. 2024. "Overview of the Current Knowledge and Conventional MRI Characteristics of Peri- and Para-Vascular Spaces" Brain Sciences 14, no. 2: 138. https://doi.org/10.3390/brainsci14020138
APA StyleParillo, M., Vaccarino, F., Di Gennaro, G., Kumar, S., Van Goethem, J., Beomonte Zobel, B., Quattrocchi, C. C., Parizel, P. M., & Mallio, C. A. (2024). Overview of the Current Knowledge and Conventional MRI Characteristics of Peri- and Para-Vascular Spaces. Brain Sciences, 14(2), 138. https://doi.org/10.3390/brainsci14020138