

Repetitive Transcranial Magnetic Stimulation (rTMS) in Post-Traumatic Stress Disorder: Study Protocol of a Nationwide Randomized Controlled Clinical Trial of Neuro-Enhanced Psychotherapy “TraumaStim”

 ,
,  , and
, and
Abstract
:1. Background
2. Study Aims
3. Primary Research Objective
4. Secondary Research Objective
- Different dimensions of PTSD assessed using CAPS-5 at M3 and M6 post-treatment;
- The severity of PTSD assessed using PCL at each visit;
- Anxiety symptoms at V13 (end of treatment), M1, M3, and M6 post-treatment;
- Depressive symptoms at V13 (end of treatment), M1, M3, and M6 post-treatment;
- Changes in social cognition at M3 post-treatment;
- Changes in quality of life at M1, M3, and M6 post-treatment;
- The safety of the intervention.
5. Methods and Design
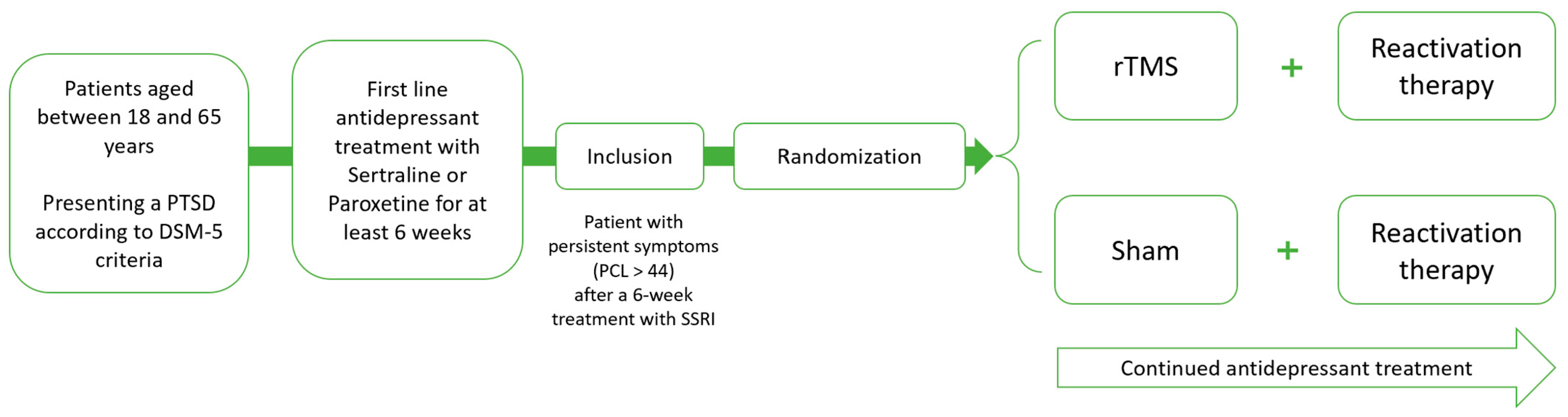
5.1. Study Design
5.2. Ethical Considerations
5.3. Inclusion Criteria Patients Aged between 18 and 65 Years
- Presenting PTSD according to DSM-5 criteria;
- Patient with persistent symptoms (PCL > 44) after 6 weeks of treatment with SSRI;
- Patient with health insurance (AME excepted);
- Signed written informed consent.
Exclusion Criteria History of Epilepsy or Seizure
- Cochlear implants;
- Cardiac pacemaker or intracardiac lines, or metal in the body;
- Strong dissociative tendencies, evidenced by an average score > 20 on the DES;
- Lifetime psychotic or bipolar disorder;
- Antisocial personality or borderline personality;
- Brain injury defined by medical report;
- Current substance dependence (including alcohol, excluding tobacco);
- Acute suicidal ideation;
- No adequate mastering of the French language or no ability to consent;
- Pregnancy (confirmed by a urine beta-HCG) or breastfeeding;
- Absence of birth control;
- Patient under legal protection measures and/or deprived of freedom;
- Participation in any other interventional study or in the exclusion period of any other interventional study.
5.4. Intervention
5.4.1. rTMS Protocol
5.4.2. Reactivation Therapy
5.5. Number of Participating Sites
5.6. Participant Identification
5.7. Randomization
5.8. Blinding Methods and Measures to Protect Blinding
5.9. Unblinding Procedures, If Applicable
6. Procedure and Data Collection
6.1. Inclusion Procedure
6.2. Patient Recruitment
6.3. Overview of Study
7. Outcomes and Instruments
7.1. Sample Characteristics
7.2. Primary Outcome Measure
7.3. Secondary Outcome Measures
- PTSD severity scores at M3 and M6 (repetition, avoidance, and neurovegetative activation) measured using CAPS-5 (structured interview);
- PTSD severity score measured using the PTSD Checklist (PCL-5 self-questionnaire) at M1, M3, and M6;
- Dissociative symptom severity scores assessed by the Clinician-Administered Dissociative States Scale (CADSS), the Multidimensional Assessment of Interoceptive Awareness (MAIA), and the Dissociative Experiences Scale (DES) at V1, V13, M1, M3, and M6.
- The severity scores of the dimensions of anxiety (measured using HAM-A) and depression (measured using HAM-D) at M1, M3, and M6.
- Social cognition at M0 and M3 assessed using the Eckman test, “reading the Mind in the Eyes” test (Baron-Cohen, test des Faux-Pas (Baron-Cohen), Empathy Quotient questionnaire (Baron-Cohen), and Toronto Alexithymia Scale (TAS-20).
- Quality of life assessed using WHOQOL EuroQol Health Measure, EQ-5D-5L;
- Proportion of adverse events during the active treatment phase and during the follow-up.
8. Statistical Analyses
8.1. Power Analysis
8.2. Primary Criterion Analysis
8.3. Secondary Criteria Analysis
9. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karam, E.G.; Friedman, M.J.; Hill, E.D.; Kessler, R.C.; McLaughlin, K.A.; Petukhova, M.; Sampson, L.; Shahly, V.; Angermeyer, M.C.; Bromet, E.J.; et al. Cumulative traumas and risk thresholds: 12-month PTSD in the World Mental Health (WMH) surveys. Depress. Anxiety 2014, 31, 130–142. [Google Scholar] [CrossRef] [PubMed]
- Sareen, J. Posttraumatic stress disorder in adults: Impact, comorbidity, risk factors, and treatment. Can. J. Psychiatry 2014, 59, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Sonnega, A.; Bromet, E.; Hughes, M.; Nelson, C.B. Posttraumatic stress disorder in the National Comorbidity Survey. Arch. Gen. Psychiatry 1995, 52, 1048–1060. [Google Scholar] [CrossRef] [PubMed]
- Williams, T.; Phillips, N.J.; Stein, D.J.; Ipser, J.C. Pharmacotherapy for post traumatic stress disorder (PTSD). Cochrane Database Syst. Rev. 2022, 3, CD002795. [Google Scholar] [CrossRef]
- Shalev, A.; Liberzon, I.; Marmar, C. Post-Traumatic Stress Disorder. N. Engl. J. Med. 2017, 376, 2459–2469. [Google Scholar] [CrossRef]
- Steenkamp, M.M.; Litz, B.T.; Hoge, C.W.; Marmar, C.R. Psychotherapy for Military-Related PTSD: A Review of Randomized Clinical Trials. JAMA 2015, 314, 489–500. [Google Scholar] [CrossRef]
- Malikowska-Racia, N.; Salat, K. Recent advances in the neurobiology of posttraumatic stress disorder: A review of possible mechanisms underlying an effective pharmacotherapy. Pharmacol. Res. 2019, 142, 30–49. [Google Scholar] [CrossRef]
- Valero-Cabré, A.; Amengual, J.L.; Stengel, C.; Pascual-Leone, A.; Coubard, O.A. Transcranial magnetic stimulation in basic and clinical neuroscience: A comprehensive review of fundamental principles and novel insights. Neurosci. Biobehav. Rev. 2017, 83, 381–404, Erratum in Neurosci. Biobehav. Rev. 2019, 96, 414. [Google Scholar] [CrossRef]
- Yan, T.; Xie, Q.; Zheng, Z.; Zou, K.; Wang, L. Different frequency repetitive transcranial magnetic stimulation (rTMS) for posttraumatic stress disorder (PTSD): A systematic review and meta-analysis. J. Psychiatr. Res. 2017, 89, 125–135. [Google Scholar] [CrossRef]
- Boggio, P.S.; Rocha, M.; Oliveira, M.O.; Fecteau, S.; Cohen, R.B.; Campanhã, C.; Ferreira-Santos, E.; Meleiro, A.; Corchs, F.; Zaghi, S.; et al. Noninvasive brain stimulation with high-frequency and low-intensity repetitive transcranial magnetic stimulation treatment for posttraumatic stress disorder. J. Clin. Psychiatry 2010, 71, 992–999. [Google Scholar] [CrossRef] [PubMed]
- Cohen, H.; Kaplan, Z.; Kotler, M.; Kouperman, I.; Moisa, R.; Grisaru, N. Repetitive transcranial magnetic stimulation of the right dorsolateral prefrontal cortex in posttraumatic stress disorder: A double-blind, placebo-controlled study. Am. J. Psychiatry 2004, 161, 515–524. [Google Scholar] [CrossRef]
- Isserles, M.; Shalev, A.Y.; Roth, Y.; Peri, T.; Kutz, I.; Zlotnick, E.; Zangen, A. Effectiveness of deep transcranial magnetic stimulation combined with a brief exposure procedure in post-traumatic stress disorder—A pilot study. Brain Stimul. 2013, 6, 377–383. [Google Scholar] [CrossRef]
- Rosenberg, P.B.; Mehndiratta, R.B.; Mehndiratta, Y.P.; Wamer, A.; Rosse, R.B.; Balish, M. Repetitive transcranial magnetic stimulation treatment of comorbid posttraumatic stress disorder and major depression. J. Neuropsychiatry Clin. Neurosci. 2002, 14, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Zhou, D.D.; Wang, W.; Wang, G.M.; Li, D.Q.; Kuang, L. An updated meta-analysis: Short-term therapeutic effects of repeated transcranial magnetic stimulation in treating obsessive-compulsive disorder. J. Affect. Disord. 2017, 215, 187–196. [Google Scholar] [CrossRef]
- Kozel, F.A.; Motes, M.A.; Didehbani, N.; DeLaRosa, B.; Bass, C.; Schraufnagel, C.D.; Jones, P.; Morgan, C.R.; Spence, J.S.; Kraut, M.A.; et al. Repetitive TMS to augment cognitive processing therapy in combat veterans of recent conflicts with PTSD: A randomized clinical trial. J. Affect. Disord. 2018, 229, 506–514. [Google Scholar] [CrossRef]
- Schnurr, P.P.; Friedman, M.J.; Engel, C.C.; Foa, E.B.; Shea, M.T.; Chow, B.K.; Resick, P.A.; Thurston, V.; Orsillo, S.M.; Haug, R.; et al. Cognitive behavioral therapy for posttraumatic stress disorder in women: A randomized controlled trial. JAMA 2007, 297, 820–830. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, S.; Wheelwright, S.; Hill, J. The ‘Reading the mind in the eyes’ test revised version: A study with normal adults, and adults with Asperger Syndrome or High-Functioning autism. J. Child Psychol. Psychiatry 2001, 42, 241–252. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; O’Riordan, M.; Jones, R.; Stone, V.E.; Plaisted, K. A new test of social sensitivity: Detection of faux pas in normal children and children with Asperger syndrome. J. Autism Dev. Disord. 1999, 29, 407–418. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; Wheelwright, S. The Empathy Quotient (EQ). An investigation of adults with Asperger Syndrome or High Functioning Autism, and normal sex differences. J. Autism Dev. Disord. 2004, 34, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Bagby, R.M.; Taylor, G.J.; Parker, J.D.A. The Twenty-Item Toronto Alexithymia Scale—I.I. Convergent, discriminant, and concurrent validity. J. Psychosom. Res. 1994, 38, 33–34. [Google Scholar] [CrossRef]
- Skevington, S.M.; Lotfy, M.; O’Connell, K.A. The World Health Organization’s WHOQOL-BREF quality of life assessment: Psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual. Life Res. 2004, 13, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Greiner, W.; Weijnen, T.; Nieuwenhuizen, M.; Oppe, S.; Badia, X.; Busschbach, J.; Buxton, M.; Dolan, P.; Kind, P.; Krabbe, P.; et al. A single European currency for EQ-5D health states. Results from a six-country study. Eur. J. Health Econ. 2003, 4, 222–231. [Google Scholar] [CrossRef] [PubMed]
- Kan, R.L.D.; Zhang, B.B.B.; Zhang, J.J.Q.; Kranz, G.S. Non-invasive brain stimulation for posttraumatic stress disorder: A systematic review and meta-analysis. Transl. Psychiatry 2020, 10, 168. [Google Scholar] [CrossRef] [PubMed]
- Ahmadizadeh, M.J.; Rezaei, M. Unilateral right and bilateral dorsolateral prefrontal cortex transcranial magnetic stimulation in treatment post-traumatic stress disorder: A randomized controlled study. Brain Res. Bull. 2018, 140, 334–340. [Google Scholar] [CrossRef]
- Cohen, S.L.; Bikson, M.; Badran, B.W.; George, M.S. A visual and narrative timeline of US FDA milestones for Transcranial Magnetic Stimulation (TMS) devices. Brain Stimul. 2022, 15, 73–75. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Visit | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PDI | ✕ | ||||||||||||||||
| HCG | ✕ | ||||||||||||||||
| Active/Sham rTMS | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | |||||
| Trauma Script | ✕ | ||||||||||||||||
| Reactivation | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | |||||
| MINI-5 | ✕ | ✕ | |||||||||||||||
| CAPS-5 | ✕ | ✕ | ✕ | ✕ | |||||||||||||
| PCL-5 | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ||||||||
| CGI | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | |||||||||
| Eckman Test | ✕ | ✕ | |||||||||||||||
| Empathy Quotient | ✕ | ✕ | |||||||||||||||
| Baron-Cohen | ✕ | ✕ | |||||||||||||||
| TAS-20 | ✕ | ✕ | |||||||||||||||
| HAM-D | ✕ | ✕ | ✕ | ✕ | ✕ | ||||||||||||
| HAM-A | ✕ | ✕ | ✕ | ✕ | ✕ | ||||||||||||
| WHOQOL | ✕ | ✕ | ✕ | ✕ | |||||||||||||
| EQ-5D-5L | ✕ | ✕ | ✕ | ✕ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferreri, F.; Mouchabac, S.; Sylvestre, V.; Millet, B.; El Hage, W.; Adrien, V.; Bourla, A. Repetitive Transcranial Magnetic Stimulation (rTMS) in Post-Traumatic Stress Disorder: Study Protocol of a Nationwide Randomized Controlled Clinical Trial of Neuro-Enhanced Psychotherapy “TraumaStim”. Brain Sci. 2023, 13, 1274. https://doi.org/10.3390/brainsci13091274
Ferreri F, Mouchabac S, Sylvestre V, Millet B, El Hage W, Adrien V, Bourla A. Repetitive Transcranial Magnetic Stimulation (rTMS) in Post-Traumatic Stress Disorder: Study Protocol of a Nationwide Randomized Controlled Clinical Trial of Neuro-Enhanced Psychotherapy “TraumaStim”. Brain Sciences. 2023; 13(9):1274. https://doi.org/10.3390/brainsci13091274
Chicago/Turabian StyleFerreri, Florian, Stephane Mouchabac, Vincent Sylvestre, Bruno Millet, Wissam El Hage, Vladimir Adrien, and Alexis Bourla. 2023. "Repetitive Transcranial Magnetic Stimulation (rTMS) in Post-Traumatic Stress Disorder: Study Protocol of a Nationwide Randomized Controlled Clinical Trial of Neuro-Enhanced Psychotherapy “TraumaStim”" Brain Sciences 13, no. 9: 1274. https://doi.org/10.3390/brainsci13091274
APA StyleFerreri, F., Mouchabac, S., Sylvestre, V., Millet, B., El Hage, W., Adrien, V., & Bourla, A. (2023). Repetitive Transcranial Magnetic Stimulation (rTMS) in Post-Traumatic Stress Disorder: Study Protocol of a Nationwide Randomized Controlled Clinical Trial of Neuro-Enhanced Psychotherapy “TraumaStim”. Brain Sciences, 13(9), 1274. https://doi.org/10.3390/brainsci13091274