
Microanatomic Morphometric Characteristics of the Third Ventricle Floor
 ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Statement
References
- Lu, L.; Chen, H.; Weng, S.; Xu, Y. Endoscopic Third Ventriculostomy versus Ventriculoperitoneal Shunt in Patients with Obstructive Hydrocephalus: Meta-Analysis of Randomized Controlled Trials. World Neurosurg. 2019, 129, 334–340. [Google Scholar] [CrossRef]
- Kulkarni, A.V.; Riva-Cambrin, J.; Browd, S.R. Use of the ETV Success Score to explain the variation in reported endoscopic third ventriculostomy success rates among published case series of childhood hydrocephalus. J. Neurosurg. Pediatr. 2011, 7, 143–146. [Google Scholar] [CrossRef] [PubMed]
- Theologou, M.; Natsis, K.; Kouskouras, K.; Chatzinikolaou, F.; Varoutis, P.; Skoulios, N.; Tsitouras, V.; Tsonidis, C. Cerebrospinal Fluid Homeostasis and Hydrodynamics: A Review of Facts and Theories. Eur. Neurol. 2022, 85, 313–325. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, E.V.; Lane, B.; Deshmukh, A.; Rosenbloom, M.J.; Desmond, J.E.; Lim, K.O.; Pfefferbaum, A. In vivo mammillary body volume deficits in amnesic and nonamnesic alcoholics. Alcohol. Clin. Exp. Res. 1999, 23, 1629–1636. [Google Scholar] [CrossRef]
- DeCuypere, M.; Teo, C. Complications of Endoscopic Third Ventriculostomy. In Pediatric Hydrocephalus; Springer: Cham, Switzerland, 2019; pp. 1563–1577. [Google Scholar]
- Schroeder, H.W.; Niendorf, W.R.; Gaab, M.R. Complications of endoscopic third ventriculostomy. J. Neurosurg. 2002, 96, 1032–1040. [Google Scholar] [CrossRef]
- Katz, D.M.; Chandar, K. Thalamus. In Encyclopedia of the Neurological Sciences; Academic Press: Cambridge, MA, USA, 2014; pp. 425–430. [Google Scholar]
- Takahashi, T.; Yucel, M.; Yung, A.R.; Wood, S.J.; Phillips, L.J.; Berger, G.E.; Ang, A.; Soulsby, B.; McGorry, P.D.; Suzuki, M.; et al. Adhesio interthalamica in individuals at high-risk for developing psychosis and patients with psychotic disorders. Prog. Neuropsychopharmacol. Biol. Psychiatry 2008, 32, 1708–1714. [Google Scholar] [CrossRef] [PubMed]
- Rose, J. The cell structure of the mamillary body in the mammals and in man. J. Anat. 1939, 74, 91–115. [Google Scholar] [PubMed]
- Tisserand, D.J.; Visser, P.J.; van Boxtel, M.P.; Jolles, J. The relation between global and limbic brain volumes on MRI and cognitive performance in healthy individuals across the age range. Neurobiol. Aging 2000, 21, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.D.; Castanho, P.; Bazira, P.; Sanders, K. Anatomical variations of the circle of Willis and their prevalence, with a focus on the posterior communicating artery: A literature review and meta-analysis. Clin. Anat. 2021, 34, 978–990. [Google Scholar] [CrossRef] [PubMed]
- Solak, S.; Ustabasioglu, F.E.; Alkan, A.; Kula, O.; Sut, N.; Tuncbilek, N. Anatomical variations of the circle of Willis in children. Pediatr. Radiol. 2021, 51, 2581–2587. [Google Scholar] [CrossRef] [PubMed]
- Yeniceri, I.O.; Cullu, N.; Deveer, M.; Yeniceri, E.N. Circle of Willis variations and artery diameter measurements in the Turkish population. Folia Morphol. (Warsz) 2017, 76, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Volovici, V.; Varvari, I.; Dirven, C.M.F.; Dammers, R. The membrane of Liliequist-a safe haven in the middle of the brain. A narrative review. Acta Neurochir. (Wien) 2020, 162, 2235–2244. [Google Scholar] [CrossRef] [PubMed]
- Fushimi, Y.; Miki, Y.; Ueba, T.; Kanagaki, M.; Takahashi, T.; Yamamoto, A.; Haque, T.L.; Konishi, J.; Takahashi, J.A.; Hashimoto, N.; et al. Liliequist membrane: Three-dimensional constructive interference in steady state MR imaging. Radiology 2003, 229, 360–365; discussion 365. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.S.; Zheng, H.P.; Zhang, F.H.; Wang, R.M. Microsurgical anatomy of Liliequist’s membrane demonstrating three-dimensional configuration. Acta Neurochir. (Wien) 2011, 153, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Giussani, C.; Guida, L.; Trezza, A.; Sganzerla, E.P. Effectiveness of Intraventricular Endoscopic Lamina Terminalis Fenestration in Comparison with Standard ETV: Systematic Review of Literature. World Neurosurg. 2017, 103, 257–264. [Google Scholar] [CrossRef] [PubMed]
- de Divitiis, O.; Angileri, F.F.; d’Avella, D.; Tschabitscher, M.; Tomasello, F. Microsurgical anatomic features of the lamina terminalis. Neurosurgery 2002, 50, 563–569; discussion 569–570. [Google Scholar] [CrossRef] [PubMed]
- Syamuleya, V.N.; Sing’ombe, I.; Mutalife, F.; Mutemwa, S.; Kafumukache, E.; Erzingatsian, K. The anatomy of the Lamina terminalis and Cisterna Chiasmatica: A cadaveric study at the University Teaching Hospital, Lusaka, Zambia. Anat. J. Afr. 2019, 8, 1452–1459. [Google Scholar] [CrossRef]
- Gammal, T.E.; Allen, M.B., Jr.; Brooks, B.S.; Mark, E.K. MR evaluation of hydrocephalus. AJR Am. J. Roentgenol. 1987, 149, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Wollenweber, F.A.; Schomburg, R.; Probst, M.; Schneider, V.; Hiry, T.; Ochsenfeld, A.; Mueller, M.; Dillmann, U.; Fassbender, K.; Behnke, S. Width of the third ventricle assessed by transcranial sonography can monitor brain atrophy in a time- and cost-effective manner--results from a longitudinal study on 500 subjects. Psychiatry Res. 2011, 191, 212–216. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
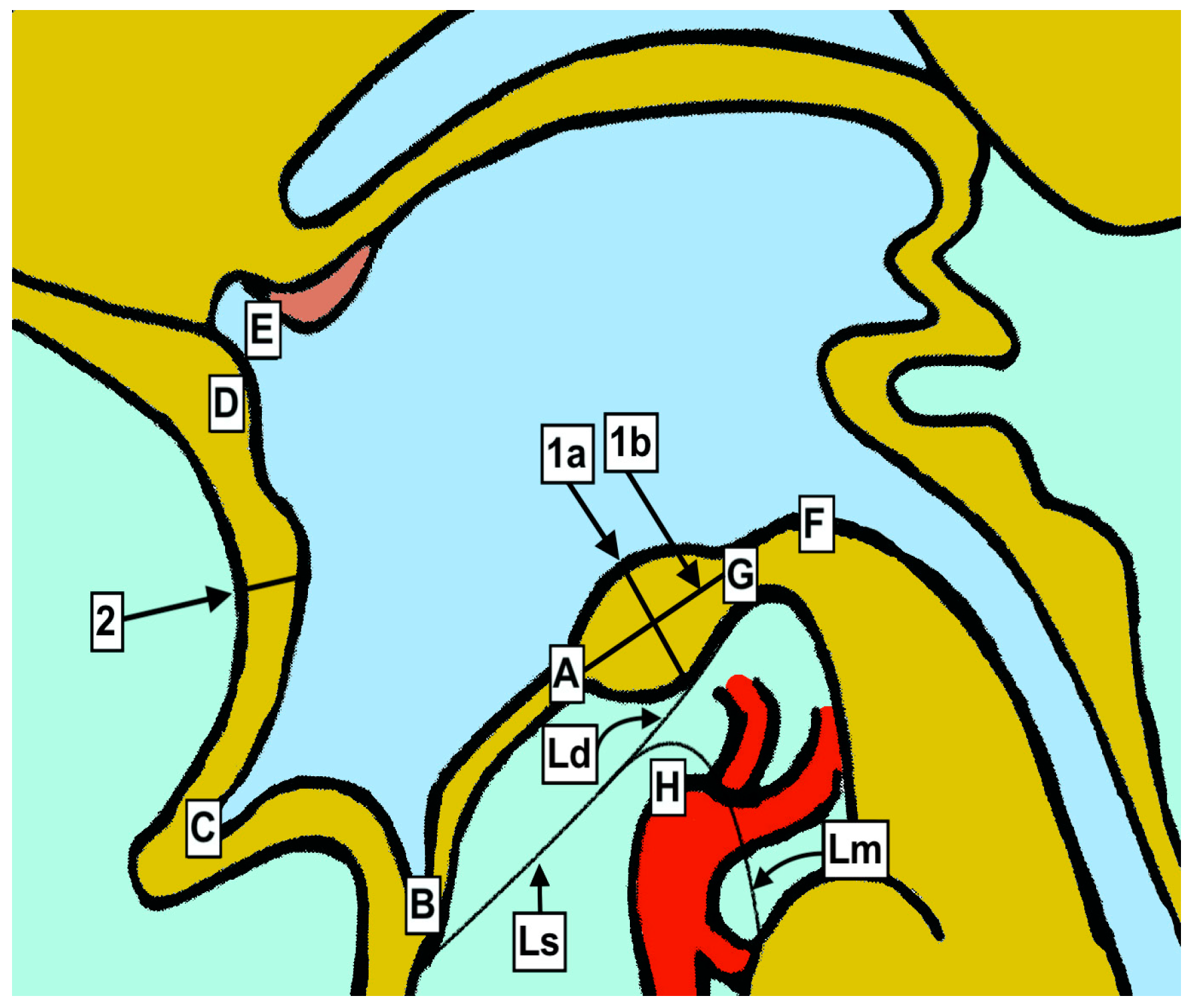
| Anatomical Points of Interest | Correlation with Figure 1 | |
|---|---|---|
| Mamillary body anteroposterior diameter | 1a | |
| Mamillary body cranio-caudal diameter | 1b | |
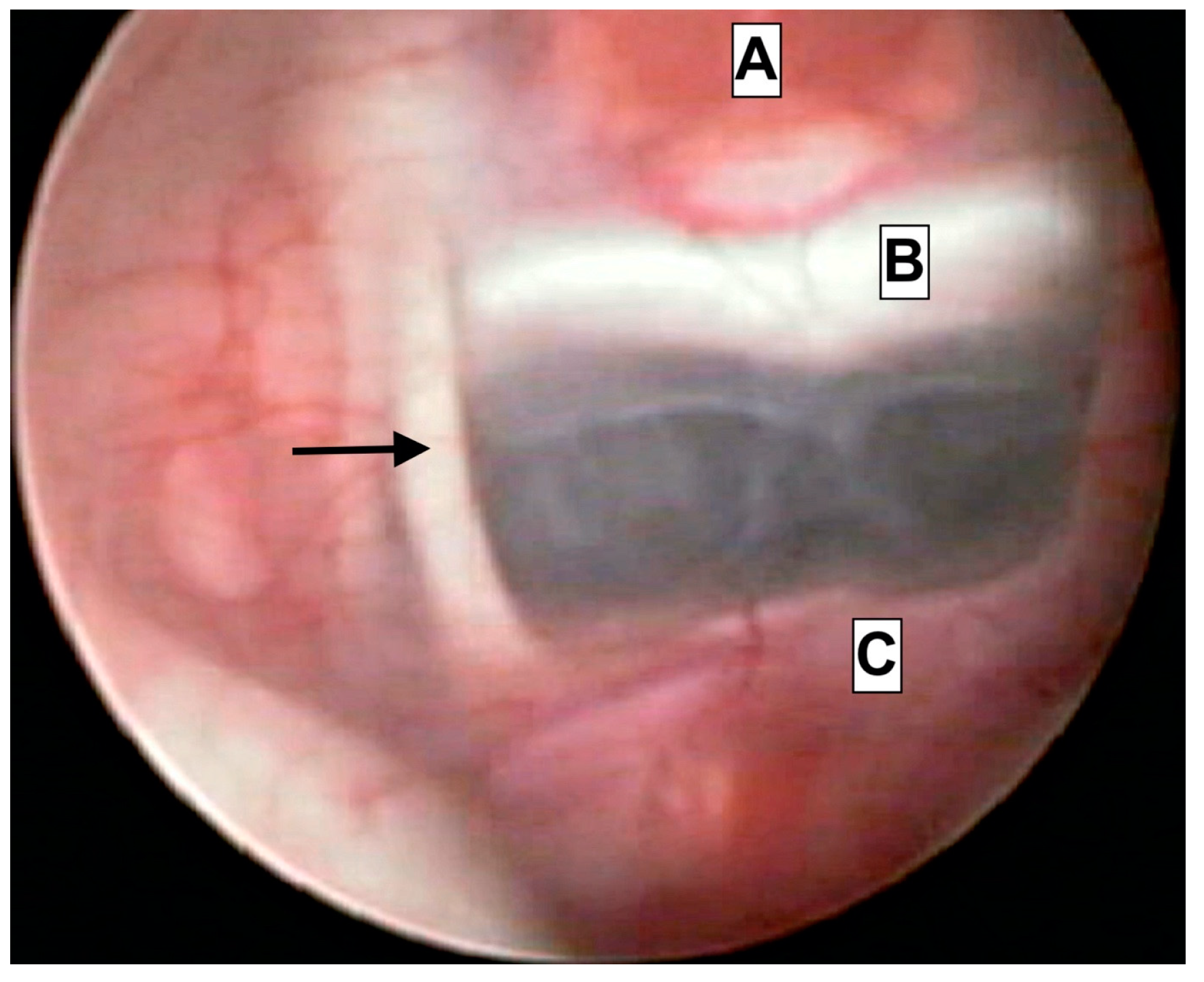
| Intraventricular projection of mamillary body | 1a (Figure 2) | |
| Ventricle floor diameter—front mamillary border | A | |
| Liliequist membrane diameter | Ld | |
| Lamina terminalis diameter | 2 | |
| Anterior border of mamillary body | Anterior border of foramen of Monro | A-E |
| Posterior border of mamillary body | Anterior border of foramen of Monro | G-E |
| Anterior border of mamillary body | Infundibular recess | A-B |
| Anterior border of mamillary body | Basilar artery apex | A-H |
| Anterior border of mamillary body | Optic recess | A-C |
| Infundibular recess | Anterior commissure | B-D |
| Sylvian aqueduct entrance | Anterior commissure | F-D |
| Cadavers | 1a | 1b | 1a Figure 2 | A | Ld | 2 | A-E | G-E | A-B | A-H | A-C | B-D | F-D |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C1 | 4.86 | 4.94 | 2.11 | 0.89 | 0.13 | 0.10 | 17.22 | 19.21 | 7.95 | 4.47 | 7.04 | 13.93 | 23.64 |
| C2 | 5.26 | 3.93 | 1.29 | 1.73 | 0.16 | 0.25 | 18.43 | 17.29 | 5.23 | 2.50 | 4.78 | 15.47 | 21.34 |
| C3 | 4.74 | 3.67 | 1.39 | 1.48 | 0.24 | 0.50 | 17.12 | 16.20 | 7.06 | 2.71 | 6.49 | 15.59 | 22.50 |
| C4 | 4.97 | 4.10 | 0.95 | 1.56 | 0.14 | 0.33 | 16.25 | 14.97 | 2.47 | 2.68 | 6.42 | 14.40 | 17.52 |
| C5 | 5.07 | 3.93 | 1.44 | 1.62 | 0.12 | 0.37 | 18.17 | 17.18 | 3.41 | 5.29 | 8.90 | 12.24 | 25.69 |
| C6 | 4.90 | 4.45 | 1.20 | 1.43 | 0.08 | 0.34 | 16.37 | 14.40 | 5.19 | 4.62 | 4.97 | 12.89 | 20.40 |
| C7 | 4.72 | 4.07 | 1.84 | 1.61 | 0.25 | 0.31 | 13.03 | 14.55 | 6.58 | 4.01 | 8.58 | 12.71 | 18.70 |
| C8 | 5.07 | 4.19 | 1.55 | 1.72 | 0.31 | 0.27 | 16.69 | 17.23 | 6.94 | 3.30 | 9.29 | 15.50 | 25.44 |
| C9 | 5.38 | 4.17 | 2.27 | 0.50 | 0.19 | 0.21 | 16.73 | 18.50 | 6.95 | 4.66 | 8.68 | 11.71 | 26.01 |
| C10 | 5.22 | 4.37 | 0.91 | 1.70 | 0.11 | 0.29 | 12.56 | 12.08 | 3.62 | 3.1 | 5.04 | 14.78 | 23.43 |
| C11 | 5.06 | 4.12 | 2.15 | 0.26 | 0.21 | 0.38 | 18.97 | 20.22 | 8.60 | 5.84 | 10.79 | 15.49 | 22.50 |
| C12 | 4.38 | 4.03 | 1.47 | 0.50 | 0.14 | 0.14 | 13.34 | 13.74 | 10.83 | 6.66 | 10.36 | 11.72 | 20.90 |
| C13 | 4.99 | 4.12 | 1.63 | 0.59 | 0.27 | 0.19 | 16.63 | 17.63 | 7.33 | 7.71 | 11.38 | 11.88 | 26.65 |
| C14 | 4.52 | 3.60 | 1.84 | 0.34 | 0.31 | 0.26 | 16.57 | 16.72 | 9.53 | 6.45 | 10.86 | 14.69 | 23.30 |
| C15 | 4.20 | 3.25 | 1.38 | 0.39 | 0.27 | 0.12 | 14.58 | 14.06 | 4.70 | 6.30 | 10.05 | 10.77 | 19.77 |
| C16 | 5.69 | 4.90 | 2.10 | 1.77 | 0.09 | 1.16 | 16.83 | 17.02 | 5.60 | 6.62 | 9.63 | 14.72 | 24.70 |
| C17 | 4.53 | 4.48 | 1.15 | 1.37 | 0.21 | 0.54 | 17.34 | 17.57 | 6.05 | 4.37 | 9.26 | 11.64 | 22.34 |
| C18 | 5.02 | 4.97 | 1.98 | 0.86 | 0.15 | 0.35 | 16.85 | 17.98 | 5.14 | 6.73 | 8.73 | 12.07 | 19.87 |
| C19 | 4.49 | 4.53 | 1.58 | 1.11 | 0.19 | 0.95 | 17.15 | 16.97 | 6.11 | 3.83 | 8.48 | 13.16 | 22.01 |
| C20 | 4.62 | 4.06 | 2.01 | 0.94 | 0.12 | 0.87 | 16.83 | 17.24 | 4.97 | 5.58 | 7.93 | 14.65 | 21.89 |
| C21 | 5.01 | 4.88 | 1.65 | 1.59 | 0.22 | 1.03 | 17.79 | 17.29 | 6.07 | 2.94 | 6.29 | 15.21 | 23.12 |
| C22 | 5.29 | 5.04 | 1.44 | 1.37 | 0.17 | 0.65 | 17.59 | 17.71 | 7.44 | 6.89 | 8.48 | 13.35 | 20.98 |
| C23 | 4.91 | 3.47 | 1.24 | 1.26 | 0.19 | 0.58 | 17.42 | 17.07 | 6.47 | 5.04 | 8.18 | 14.72 | 21.69 |
| C24 | 4.74 | 4.04 | 1.27 | 1.03 | 0.21 | 0.73 | 16.38 | 16.54 | 7.08 | 6.94 | 7.39 | 13.89 | 24.43 |
| C25 | 5.09 | 3.98 | 2.89 | 1.68 | 0.24 | 0.43 | 18.24 | 19.67 | 8.31 | 7.07 | 8.17 | 15.62 | 22.77 |
| Parameters | Shapiro (p) | Descriptives | Min | Max | |
|---|---|---|---|---|---|
| Age | 0.1012 | 61.72 * | (±10.08) | 34 | 75 |
| 1a | 0.9704 | 4.91 * | (±0.34) | 4.2 | 5.69 |
| 1b | 0.2415 | 4.21 * | (±0.48) | 3.2 | 5.04 |
| 1a Figure 2 | 0.2881 | 1.63 * | (±0.46) | 0.91 | 2.89 |
| A | 0.01241 | 1.37 ‡ | (±0.75) | 0.26 | 1.77 |
| Ld | 0.6264 | 0.19 * | (±0.07) | 0.08 | 0.31 |
| 2 | 0.01157 | 0.35 ‡ | (±0.32) | 0.10 | 1.16 |
| A-E | 0.001672 | 16.83 ‡ | (±1.04) | 12.56 | 18.97 |
| G-E | 0.1607 | 16.76 * | (±1.9) | 12.08 | 20.22 |
| A-B | 0.9854 | 6.39 * | (±1.9) | 2.47 | 10.83 |
| A-H | 0.1148 | 5.05 * | (±1.62) | 2.50 | 7.71 |
| A-C | 0.4471 | 8.25 * | (±1.84) | 4.78 | 11.38 |
| B-D | 0.03542 | 13.93 ‡ | (±2.54) | 10.77 | 15.62 |
| F-D | 0.9865 | 22.46 * | (±2.29) | 17.52 | 26.65 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Theologou, M.; Kouskouras, K.; Natsis, K.; Varoutis, P.; Zaggelidou, E.; Tsonidis, C. Microanatomic Morphometric Characteristics of the Third Ventricle Floor. Brain Sci. 2023, 13, 580. https://doi.org/10.3390/brainsci13040580
Theologou M, Kouskouras K, Natsis K, Varoutis P, Zaggelidou E, Tsonidis C. Microanatomic Morphometric Characteristics of the Third Ventricle Floor. Brain Sciences. 2023; 13(4):580. https://doi.org/10.3390/brainsci13040580
Chicago/Turabian StyleTheologou, Marios, Konstantinos Kouskouras, Konstantinos Natsis, Panagiotis Varoutis, Eleni Zaggelidou, and Christos Tsonidis. 2023. "Microanatomic Morphometric Characteristics of the Third Ventricle Floor" Brain Sciences 13, no. 4: 580. https://doi.org/10.3390/brainsci13040580
APA StyleTheologou, M., Kouskouras, K., Natsis, K., Varoutis, P., Zaggelidou, E., & Tsonidis, C. (2023). Microanatomic Morphometric Characteristics of the Third Ventricle Floor. Brain Sciences, 13(4), 580. https://doi.org/10.3390/brainsci13040580