
The Role of Reirradiation in Childhood Progressive Diffuse Intrinsic Pontine Glioma (DIPG): An Ongoing Challenge beyond Radiobiology

 , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
4.1. Systemic Therapies
4.2. Radiotherapy
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Warren, K.E. Diffuse intrinsic pontine glioma: Poised for progress. Front. Oncol. 2012, 2, 205. [Google Scholar] [CrossRef]
- Hargrave, D.; Bartels, U.; Bouffet, E. Diffuse brainstem glioma in children: Critical review of clinical trials. Lancet Oncol. 2006, 7, 241–248. [Google Scholar] [CrossRef]
- Jansen, M.H.; van Vuurden, D.G.; Vandertop, W.P.; Kaspers, G.J. Diffuse intrinsic pontine gliomas: A systematic update on clinical trials and biology. Cancer Treat. Rev. 2012, 38, 27–35. [Google Scholar] [CrossRef]
- Robison, N.J.; Kieran, M.W. Diffuse intrinsic pontine glioma: A reassessment. J. Neuro-Oncol. 2014, 119, 7–15. [Google Scholar] [CrossRef]
- Albright, A.L.; Price, R.A.; Buthkelch, A.N. Brain stem gliomas of children. Cancer 1983, 52, 2313–2319. [Google Scholar] [CrossRef]
- Massimino, M.; Biassoni, V.; Miceli, R.; Schiavello, E.; Warmuth-Metz, M.; Modena, P.; Casanova, M.; Pecori, E.; Giangaspero, F.; Antonelli, M.; et al. Results of nimotuzumab and vinorelbine, radiation and re-irradiation for diffuse pontine glioma in childhood. J. Neuro-Oncol. 2014, 118, 305–312. [Google Scholar] [CrossRef]
- Chapman, C.H.; Hara, J.H.; Molinaro, A.M.; Clarke, J.L.; Oberheim Bush, N.A.; Taylor, J.W.; Butowski, N.A.; Chang, S.M.; Fogh, S.E.; Sneed, P.K.; et al. Reirradiation of recurrent high-grade glioma and development of prognostic scores for progression and survival. Neurooncol. Pract. 2019, 6, 364–374. [Google Scholar] [CrossRef]
- Fowler, J.F. The linear-quadratic formula and progress in fractionated radiotherapy. Br. J. Radiol. 1989, 62, 679–694. [Google Scholar] [CrossRef]
- Frappaz, D.; Schell, M.; Thiesse, P.; Marec-Bérard, P.; Mottolese, C.; Perol, D.; Bergeron, C.; Philip, T.; Ricci, A.C.; Galand-Desme, S.; et al. Preradiation chemotherapy may improve survival in pediatric diffuse intrinsic brainstem gliomas: Final results of BSG 98 prospective trial. Neuro-Oncol. 2008, 10, 599–607. [Google Scholar] [CrossRef]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef]
- Cohen, K.J.; Heideman, R.L.; Zhou, T.; Holmes, E.J.; Lavey, R.S.; Bouffet, E.; Pollack, I.F. Temozolomide in the treatment of children with newly diagnosed diffuse intrinsic pontine gliomas: A report from the Children’s Oncology Group. Neuro-Oncol. 2011, 13, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Kilburn, L.B.; Kocak, M.; Baxter, P.; Poussaint, T.Y.; Paulino, A.C.; McIntyre, C.; Lemenuel-Diot, A.; Lopez-Diaz, C.; Kun, L.; Chintagumpala, M.; et al. A pediatric brain tumor consortium phase II trial of capecitabine rapidly disintegrating tablets with concomitant radiation therapy in children with newly diagnosed diffuse intrinsic pontine gliomas. Pediatr. Blood Cancer 2018, 65, e26832. [Google Scholar] [CrossRef] [PubMed]
- Chiang, J.; Diaz, A.K.; Makepeace, L.; Li, X.; Han, Y.; Li, Y.; Klimo, P.; Boop, F.A.; Baker, S.J.; Gajjar, A.; et al. Clinical, imaging, and molecular analysis of pediatric pontine tumors lacking characteristic imaging features of DIPG. Acta Neuropathol. Commun. 2020, 8, 57. [Google Scholar] [CrossRef] [PubMed]
- Walker, D.A.; Liu, J.; Kieran, M.; Jabado, N.; Picton, S.; Packer, R.; St Rose, C.; CPN Paris 2011 Conference Consensus Group. A multi-disciplinary consensus statement concerning surgical approaches to low-grade, high-grade astrocytomas and diffuse intrinsic pontine gliomas in childhood (CPN Paris 2011) using the Delphi method. Neuro-Oncol. 2013, 15, 462–468. [Google Scholar] [CrossRef] [PubMed]
- Truffaux, N.; Philippe, C.; Paulsson, J.; Andreiuolo, F.; Guerrini-Rousseau, L.; Cornilleau, G.; Le Dret, L.; Richon, C.; Lacroix, L.; Puget, S.; et al. Preclinical evaluation of dasatinib alone and in combination with cabozantinib for the treatment of diffuse intrinsic pontine glioma. Neuro-Oncol. 2015, 17, 953–964. [Google Scholar] [CrossRef]
- Chakravarti, A.; Wang, M.; Robins, H.I.; Lautenschlaeger, T.; Curran, W.J.; Brachman, D.G.; Schultz, C.J.; Choucair, A.; Dolled-Filhart, M.; Christiansen, J.; et al. RTOG 0211: A phase 1/2 study of radiation therapy with concurrent gefitinib for newly diagnosed glioblastoma patients. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 1206–1211. [Google Scholar] [CrossRef]
- Raizer, J.J.; Abrey, L.E.; Lassman, A.B.; Chang, S.M.; Lamborn, K.R.; Kuhn, J.G.; Yung, W.A.; Gilbert, M.R.; Aldape, K.A.; Wen, P.Y.; et al. A phase II trial of erlotinib in patients with recurrent malignant gliomas and nonprogressive glioblastoma multiforme postradiation therapy. Neuro-Oncol. 2010, 12, 95–103. [Google Scholar] [CrossRef]
- Wen, P.Y.; Chang, S.M.; Lamborn, K.R.; Kuhn, J.G.; Norden, A.D.; Cloughesy, T.F.; Robins, H.I.; Lieberman, F.S.; Gilbert, M.R.; Mehta, M.P.; et al. Phase I/II study of erlotinib and temsirolimus for patients with recurrent malignant gliomas: North American Brain Tumor Consortium trial 04-02. Neuro-Oncol. 2014, 16, 567–578. [Google Scholar] [CrossRef]
- Peereboom, D.M.; Shepard, D.R.; Ahluwalia, M.S.; Brewer, C.J.; Agarwal, N.; Stevens, G.H.; Suh, J.H.; Toms, S.A.; Vogelbaum, M.A.; Weil, R.J.; et al. Phase II trial of erlotinib with temozolomide and radiation in patients with newly diagnosed glioblastoma multiforme. J. Neurooncol. 2010, 98, 93–99. [Google Scholar] [CrossRef]
- Chornenkyy, Y.; Agnihotri, S.; Yu, M.; Buczkowicz, P.; Rakopoulos, P.; Golbourn, B.; Garzia, L.; Siddaway, R.; Leung, S.; Rutka, J.T.; et al. Poly-ADP-Ribose Polymerase as a Therapeutic Target in Pediatric Diffuse Intrinsic Pontine Glioma and Pediatric High-Grade Astrocytoma. Mol. Cancer Ther. 2015, 14, 2560–2568. [Google Scholar] [CrossRef]
- Warren, K.E.; Killian, K.; Suuriniemi, M.; Wang, Y.; Quezado, M.; Meltzer, P.S. Genomic aberrations in pediatric diffuse intrinsic pontine gliomas. Neuro-Oncol. 2012, 14, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Hummel, T.R.; Salloum, R.; Drissi, R.; Kumar, S.; Sobo, M.; Goldman, S.; Pai, A.; Leach, J.; Lane, A.; Pruitt, D.; et al. A pilot study of bevacizumab-based therapy in patients with newly diagnosed high-grade gliomas and diffuse intrinsic pontine gliomas. J. Neuro-Oncol. 2016, 127, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Chandra, P.S. Diffuse Intrinsic Pontine Gliomas: Will there Ever be a Light at the End of the Dark Tunnel? Neurol. India 2023, 71, 2–4. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Suh, C.O. Radiotherapy for Diffuse Intrinsic Pontine Glioma: Insufficient but Indispensable. Brain Tumor Res. Treat. 2023, 11, 79–85. [Google Scholar] [CrossRef]
- Gallitto, M.; Lazarev, S.; Wasserman, I.; Stafford, J.M.; Wolden, S.L.; Terezakis, S.A.; Bindra, R.S.; Bakst, R.L. Role of Radiation Therapy in the Management of Diffuse Intrinsic Pontine Glioma: A Systematic Review. Adv. Radiat. Oncol. 2019, 4, 520–531. [Google Scholar] [CrossRef]
- Park, J.; Yea, J.W.; Park, J.W. Hypofractionated radiotherapy versus conventional radiotherapy for diffuse intrinsic pontine glioma: A systematic review and meta-analysis. Medicine 2020, 99, e22721. [Google Scholar] [CrossRef]
- Lo Greco, M.C.; Milazzotto, R.; Liardo, R.L.E.; Acquaviva, G.; La Rocca, M.; Altieri, R.; Certo, F.; Barbagallo, G.M.; Basile, A.; Foti, P.V.; et al. Relapsing High—Grade Glioma from Peritumoral Zone: Critical Review of Radiotherapy Treatment Options. Brain Sci. 2022, 12, 416. [Google Scholar] [CrossRef]
- Fontanilla, H.P.; Pinnix, C.C.; Ketonen, L.M.; Woo, S.Y.; Vats, T.S.; Rytting, M.E.; Wolff, J.E.; Mahajan, A. Palliative reirradiation for progressive diffuse intrinsic pontine glioma. Am. J. Clin. Oncol. 2012, 35, 51–57. [Google Scholar] [CrossRef]
- Janssens, G.O.; Gandola, L.; Bolle, S.; Mandeville, H.; Ramos-Albiac, M.; van Beek, K.; Benghiat, H.; Hoeben, B.; Morales La Madrid, A.; Kortmann, R.D.; et al. Survival benefit for patients with diffuse intrinsic pontine glioma (DIPG) undergoing re-irradiation at first progression: A matched-cohort analysis on behalf of the SIOP-E-HGG/DIPG working group. Eur. J. Cancer 2017, 73, 38–47. [Google Scholar] [CrossRef]
- Janssens, G.O.; Kramm, C.M.; von Bueren, A.O. Diffuse intrinsic pontine gliomas (DIPG) at recurrence: Is there a window to test new therapies in some patients? J. Neuro-Oncol. 2018, 139, 501. [Google Scholar] [CrossRef]
- Amsbaugh, M.J.; Mahajan, A.; Thall, P.F.; McAleer, M.F.; Paulino, A.C.; Grosshans, D.; Khatua, S.; Ketonen, L.; Fontanilla, H.; McGovern, S.L. A Phase 1/2 Trial of Reirradiation for Diffuse Intrinsic Pontine Glioma. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Krishnatry, R.; Manjali, J.J.; Chinnaswamy, G.; Chatterjee, A.; Goda, J.S.; Janu, A.; Sahu, A.; Jalali, R.; Gupta, T. Clinical approach to re-irradiation for recurrent diffuse intrinsic pontine glioma. Jpn. J. Clin. Oncol. 2021, 51, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Spatola, C.; Liardo, R.L.E.; Milazzotto, R.; Raffaele, L.; Salamone, V.; Basile, A.; Foti, P.V.; Palmucci, S.; Cirrone, G.A.P.; Cuttone, G.; et al. Radiotherapy of Conjunctival Melanoma: Role and Challenges of Brachytherapy, Photon-Beam and Protontherapy. Appl. Sci. 2020, 10, 9071. [Google Scholar] [CrossRef]
- Foti, P.V.; Inì, C.; Travali, M.; Farina, R.; Palmucci, S.; Spatola, C.; Liardo, R.L.E.; Milazzotto, R.; Raffaele, L.; Salamone, V.; et al. MR Imaging–Pathologic Correlation of Uveal Melanomas Undergoing Secondary Enucleation after Proton Beam Radiotherapy. Appl. Sci. 2021, 11, 4310. [Google Scholar] [CrossRef]
- Indelicato, D.J.; Rotondo, R.L.; Uezono, H.; Sandler, E.S.; Aldana, P.R.; Ranalli, N.J.; Beier, A.D.; Morris, C.G.; Bradley, J.A. Outcomes following proton therapy for pediatric low-grade glioma. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 149–156. [Google Scholar] [CrossRef]
- Indelicato, D.J.; Flampouri, S.; Rotondo, R.L.; Bradley, J.A.; Morris, C.G.; Aldana, P.R.; Sandler, E.; Mendenhall, N.P. Incidence and dosimetric parameters of pediatric brainstem toxicity following proton therapy. Acta Oncol. 2014, 53, 1298–1304. [Google Scholar] [CrossRef]
- Upadhyay, R.; Liao, K.; Grosshans, D.R.; McGovern, S.L.; Frances McAleer, M.; Zaky, W.; Chintagumpala, M.M.; Mahajan, A.; Nana Yeboa, D.; Paulino, A.C. Quantifying the risk and dosimetric variables of symptomatic brainstem injury after proton beam radiation in pediatric brain tumors. Neuro-Oncol. 2022, 24, 1571–1581. [Google Scholar] [CrossRef]
- Yock, T.I.; Constine, L.S.; Mahajan, A. Protons, the brainstem, and toxicity: Ingredients for an emerging dialectic. Acta Oncol. 2014, 53, 1279–1282. [Google Scholar] [CrossRef]
- Haas-Kogan, D.; Indelicato, D.; Paganetti, H.; Esiashvili, N.; Mahajan, A.; Yock, T.; Flampouri, S.; MacDonald, S.; Fouladi, M.; Stephen, K.; et al. National Cancer Institute workshop on proton therapy for children: Considerations regarding brainstem injury. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 152–168. [Google Scholar] [CrossRef]
- Morales La Madrid, A.; Santa-María, V.; Cruz Martinez, O.; Mora, J.; Puerta Roldan, P.; Guillen Quesada, A.; Suñol Capella, M.; de Torres Gomez-Pallete, C.; Lassaletta, A.; Laperriere, N.; et al. Second re-irradiation for DIPG progression, re-considering “old strategies” with new approaches. Child’s Nerv. Syst. ChNS Off. J. Int. Soc. Pediatr. Neurosurg. 2017, 33, 849–852. [Google Scholar] [CrossRef]
- Bergengruen, P.M.; Hernaíz Driever, P.; Budach, V.; Zips, D.; Grün, A. Second course of re-irradiation in pediatric diffuse intrinsic pontine glioma: A case study. Strahlenther. Onkol. 2023, 199, 773–777. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, A.; Stavinoha, P.L.; Rongthong, W.; Brodin, N.P.; McGovern, S.L.; El Naqa, I.; Palmer, J.D.; Vennarini, S.; Indelicato, D.J.; Aridgides, P.; et al. Neurocognitive Effects and Necrosis in Childhood Cancer Survivors Treated with Radiation Therapy: A PENTEC Comprehensive Review. Int. J. Radiat. Oncol. Biol. Phys. 2021, S0360-3016(21)00127-9. [Google Scholar] [CrossRef] [PubMed]
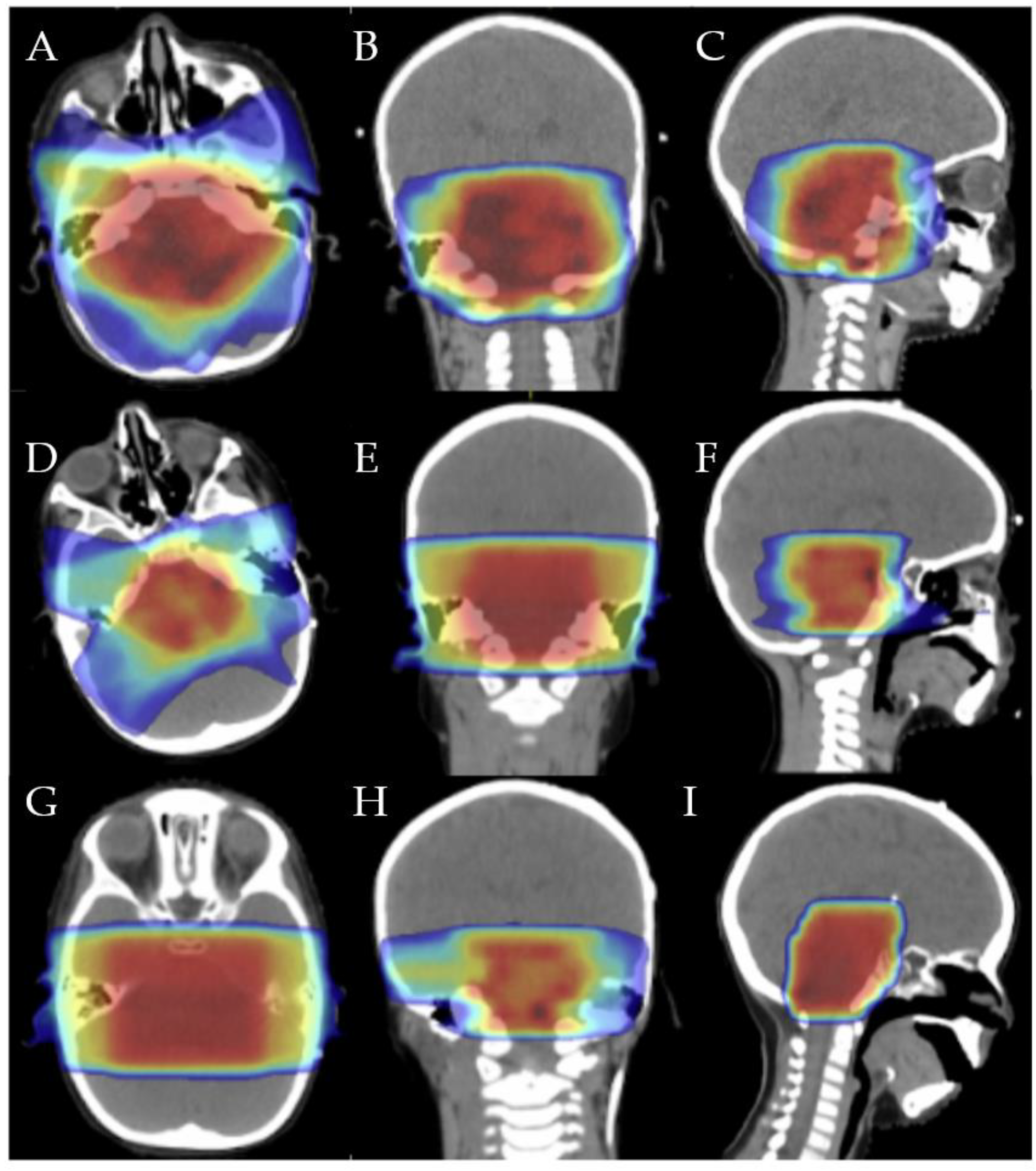

{kind=link}
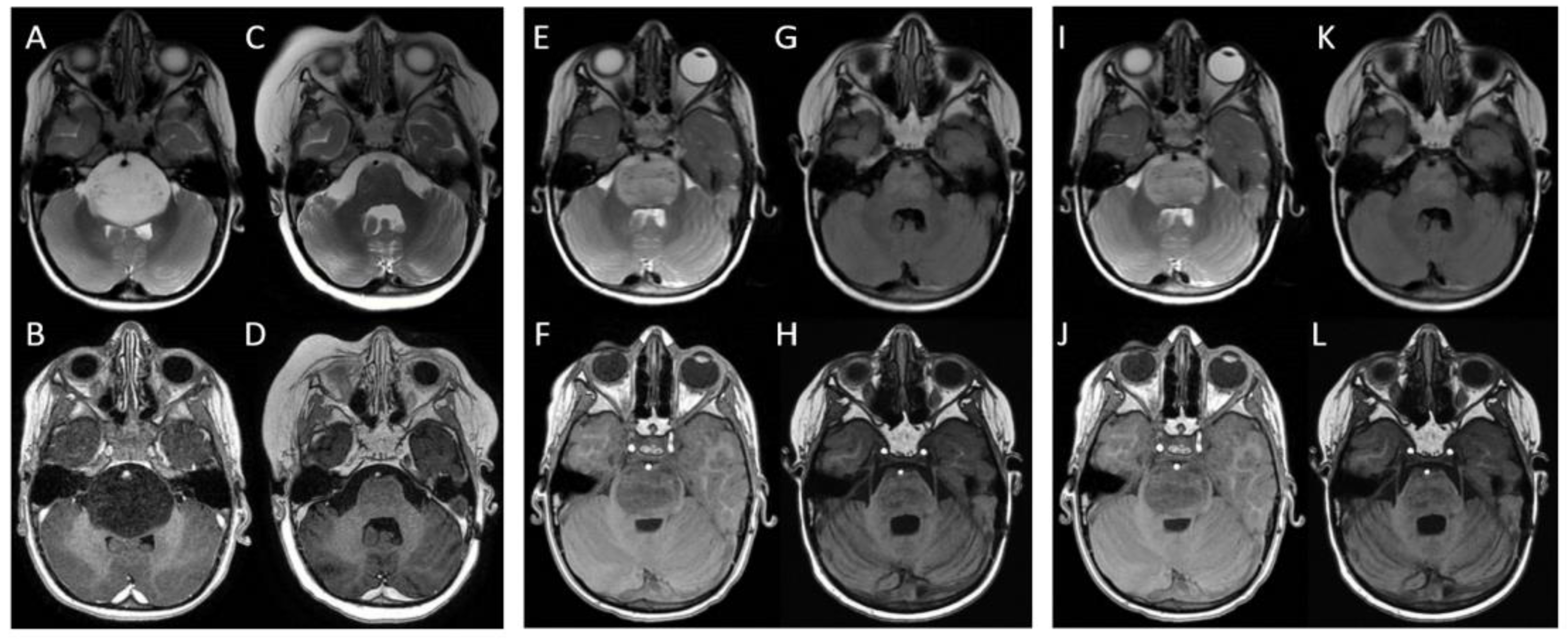
{kind=link}
| Time to First Progression | Time to Second Progression | Overall Survival | |
|---|---|---|---|
| Child n. 1 | 9 months | 6 months | 24 months |
| Child n. 2 | 6 months | 4 months | 18 months |
| Child n. 3 | 6 months | 3 months | 17 months |
| Median value ± standard deviation | 7 ± 1.7 months | 4.3 ± 1.5 months | 19.6 ± 3.7 months |
| I Radiotherapy Course | II Radiotherapy Course | III Radiotherapy Course | EQD2cum (α/β = 10) | |
|---|---|---|---|---|
| Our experience | 2 Gy × 27 fx = 54 Gy | 1.8 Gy × 11 fx = 19.8 Gy | 2 Gy × 6 fx = 12 Gy | 85.5 Gy |
| La Madrid et al. [40] | 1.8 Gy × 30 fx = 54 Gy | 1.8 Gy × 17 fx = 30.6 Gy | 1.8 × 12 fx = 21.6 Gy | 104.4 Gy |
| 3 Gy × 13 fx = 39 Gy | 2 Gy × 10 fx = 20 Gy | 2 Gy × 10 fx = 20 Gy | 82.2 Gy | |
| Bergengruen et al. [41] | 1.8 Gy × 30 fx = 54 Gy | 2 Gy × 18 fx = 36 Gy | 1.8 Gy × 12 fx = 21.6 Gy | 110.3 Gy |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo Greco, M.C.; Milazzotto, R.; Liardo, R.L.E.; Foti, P.V.; Palmucci, S.; Basile, A.; Pergolizzi, S.; Spatola, C. The Role of Reirradiation in Childhood Progressive Diffuse Intrinsic Pontine Glioma (DIPG): An Ongoing Challenge beyond Radiobiology. Brain Sci. 2023, 13, 1449. https://doi.org/10.3390/brainsci13101449
Lo Greco MC, Milazzotto R, Liardo RLE, Foti PV, Palmucci S, Basile A, Pergolizzi S, Spatola C. The Role of Reirradiation in Childhood Progressive Diffuse Intrinsic Pontine Glioma (DIPG): An Ongoing Challenge beyond Radiobiology. Brain Sciences. 2023; 13(10):1449. https://doi.org/10.3390/brainsci13101449
Chicago/Turabian StyleLo Greco, Maria Chiara, Roberto Milazzotto, Rocco Luca Emanuele Liardo, Pietro Valerio Foti, Stefano Palmucci, Antonio Basile, Stefano Pergolizzi, and Corrado Spatola. 2023. "The Role of Reirradiation in Childhood Progressive Diffuse Intrinsic Pontine Glioma (DIPG): An Ongoing Challenge beyond Radiobiology" Brain Sciences 13, no. 10: 1449. https://doi.org/10.3390/brainsci13101449
APA StyleLo Greco, M. C., Milazzotto, R., Liardo, R. L. E., Foti, P. V., Palmucci, S., Basile, A., Pergolizzi, S., & Spatola, C. (2023). The Role of Reirradiation in Childhood Progressive Diffuse Intrinsic Pontine Glioma (DIPG): An Ongoing Challenge beyond Radiobiology. Brain Sciences, 13(10), 1449. https://doi.org/10.3390/brainsci13101449