
Association between Deep Medullary Veins in the Unaffected Hemisphere and Functional Outcome in Acute Cardioembolic Stroke: An Observational Retrospective Study

 , ,
, ,
Abstract
1. Introduction
2. Methods
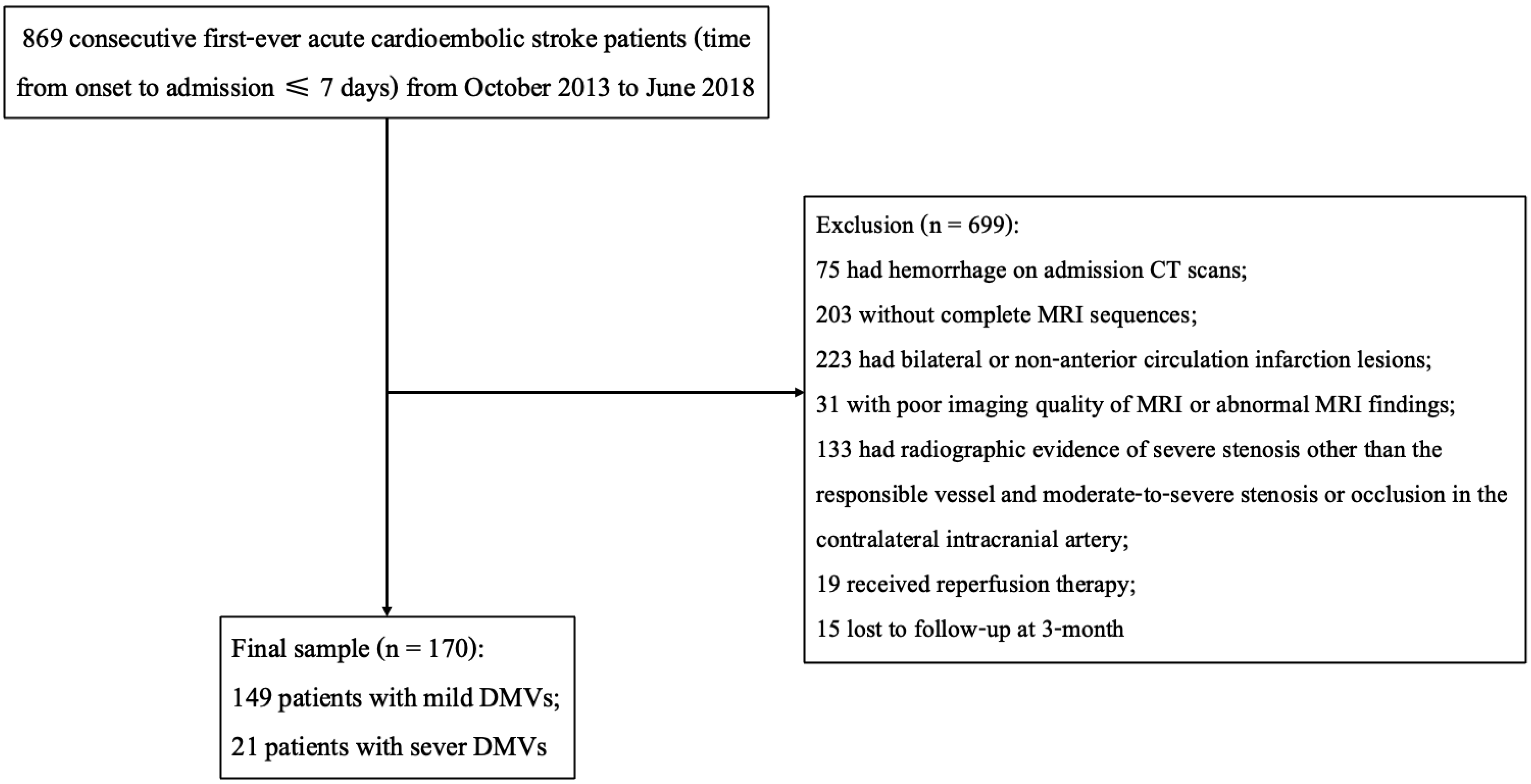
2.1. Study Participants
2.2. Clinical Assessment and Follow-Up Outcome Measures
2.3. Neuroimaging Acquisition: CT and MRI
2.4. Assessment of DMVs Grade and Other Neuroimaging Characteristics
2.5. Statistical Analysis
2.6. Ethical Standards and Participants’ Consent
3. Results
3.1. Baseline Information and Comparison between the Two DMVs Groups
3.2. Comparison of Clinical Features and Neuroimaging Characteristics between the Two Functional Outcome Groups
3.3. Association between Severe DMVs Grades and Three-Month Poor Functional Outcomes
3.4. Stratified Analyses to Identify Variables That May Modify the Association between Severe DMVs and Three-Month Functional Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, S.; Wu, B.; Liu, M.; Chen, Z.; Wang, W.; Anderson, C.S.; Sandercock, P.; Wang, Y.; Huang, Y.; Cui, L.; et al. Stroke in China: Advances and challenges in epidemiology, prevention, and management. Lancet Neurol. 2019, 18, 394–405. [Google Scholar] [CrossRef]
- Hart, R.; Pearce, L.; Miller, V.; Anderson, D.; Rothrock, J.; Albers, G.; Nasco, E. Cardioembolic vs. noncardioembolic strokes in atrial fibrillation: Frequency and effect of antithrombotic agents in the stroke prevention in atrial fibrillation studies. Cerebrovasc. Dis. 2000, 10, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zheng, L.; Cheng, Y.; Zhang, S.; Wu, B.; Wang, D.; Zhang, S.; Tao, W.; Wu, S.; Liu, M. Trends in Outcomes of Patients With Ischemic Stroke Treated Between 2002 and 2016: Insights From a Chinese Cohort. Circulation Cardiovasc. Qual. Outcomes 2019, 12, e005610. [Google Scholar] [CrossRef] [PubMed]
- Charles Lee, M.A.P.; Charles, M.; Kenney, C.M., III. MR Evaluation of Developmental Venous Anomalies: Medullary Venous Anatomy of Venous Angiomas. Am. Soc. Neuroradiol. 1996, 17, 61–70. [Google Scholar]
- Friedman, D.P. Abnormalities ofthe Deep MedullaryWhite Matter Veins: MR Imaging Findings. Am. J. Roentgenol. 1997, 168, 1103–1108. [Google Scholar] [CrossRef] [PubMed]
- Morita, N.; Harada, M.; Uno, M.; Matsubara, S.; Matsuda, T.; Nagahiro, S.; Nishitani, H. Ischemic findings of T2*-weighted 3-tesla MRI in acute stroke patients. Cerebrovasc. Dis. 2008, 26, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Horie, N.; Morikawa, M.; Nozaki, A.; Hayashi, K.; Suyama, K.; Nagata, I. “Brush Sign” on susceptibility-weighted MR imaging indicates the severity of moyamoya disease. AJNR. Am. J. Neuroradiol. 2011, 32, 1697–1702. [Google Scholar] [CrossRef]
- Rosso, C.; Belleville, M.; Pires, C.; Dormont, D.; Crozier, S.; Chiras, J.; Samson, Y.; Bonneville, F. Clinical usefulness of the visibility of the transcerebral veins at 3T on T2*-weighted sequence in acute stroke patients. Eur. J. Radiol. 2012, 81, 1282–1287. [Google Scholar] [CrossRef]
- Chen, C.Y.; Chen, C.I.; Tsai, F.Y.; Tsai, P.H.; Chan, W.P. Prominent vessel sign on susceptibility-weighted imaging in acute stroke: Prediction of infarct growth and clinical outcome. PLoS ONE 2015, 10, e0131118. [Google Scholar] [CrossRef]
- Mucke, J.; Möhlenbruch, M.; Kickingereder, P.; Kieslich, P.; Bäumer, P.; Gumbinger, C.; Purrucker, J.; Mundiyanapurath, S.; Schlemmer, H.; Bendszus, M.; et al. Asymmetry of deep medullary veins on susceptibility weighted MRI in patients with acute MCA stroke is associated with poor outcome. PLoS ONE 2015, 10, e0120801. [Google Scholar] [CrossRef]
- Han, X.; Ouyang, L.; Zhang, C.; Ma, H.; Qin, J. Relationship between deep medullary veins in susceptibility-weighted imaging and ipsilateral cerebrovascular reactivity of middle cerebral artery in patients with ischemic stroke. Exp. Ther. Med. 2016, 11, 2217–2220. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Payabvash, S.; Benson, J.; Taleb, S.; Rykken, J.; Hoffman, B.; Oswood, M.; McKinney, A. Prominent cortical and medullary veins on susceptibility-weighted images of acute ischaemic stroke. Br. J. Radiol. 2016, 89, 20160714. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Yuan, L.; Jackson, A.; Sun, J.; Huang, P.; Xu, X.; Mao, Y.; Lou, M.; Jiang, Q.; Zhang, M. Prominence of Medullary Veins on Susceptibility-Weighted Images Provides Prognostic Information in Patients with Subacute Stroke. AJNR. Am. J. Neuroradiol. 2016, 37, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Wang, L.; Li, Z.; Wang, S.; Wang, G. Related Factors of Asymmetrical Vein Sign in Acute Middle Cerebral Artery Stroke and Correlation with Clinical Outcome. J. Stroke Cerebrovasc. Dis. 2017, 26, 2346–2353. [Google Scholar] [CrossRef]
- Duan, Y.; Xu, Z.; Li, H.; Cai, X.; Chang, C.; Yang, B. Prominent deep medullary veins: A predictive biomarker for stroke risk from transient ischemic attack? Acta Radiol. 2018, 59, 606–611. [Google Scholar] [CrossRef]
- Lou, M.; Chen, Z.; Wan, J.; Hu, H.; Cai, X.; Shi, Z.; Sun, J. Susceptibility-diffusion mismatch predicts thrombolytic outcomes: A retrospective cohort study. AJNR. Am. J. Neuroradiol. 2014, 35, 2061–2067. [Google Scholar] [CrossRef]
- Dejobert, M.; Cazals, X.; Annan, M.; Debiais, S.; Lauvin, M.A.; Cottier, J.P. Susceptibility-Diffusion Mismatch in Hyperacute Stroke: Correlation with Perfusion-Diffusion Mismatch and Clinical Outcome. J. Stroke Cerebrovasc. Dis. 2016, 25, 1760–1766. [Google Scholar] [CrossRef]
- Luo, S.; Yang, L.; Luo, Y. Susceptibility-weighted imaging predicts infarct size and early-stage clinical prognosis in acute ischemic stroke. Neurol. Sci. 2018, 39, 1049–1055. [Google Scholar] [CrossRef]
- Park, M.G.; Yang, T.I.; Oh, S.J.; Baik, S.K.; Kang, Y.H.; Park, K.P. Multiple hypointense vessels on susceptibility-weighted imaging in acute ischemic stroke: Surrogate marker of oxygen extraction fraction in penumbra? Cerebrovasc. Dis. 2014, 38, 254–261. [Google Scholar] [CrossRef]
- Xu, Z.; Duan, Y.; Yang, B.; Huang, X.; Pei, Y.; Li, X. Asymmetric Deep Medullary Veins in Patients With Occlusion of a Large Cerebral Artery: Association With Cortical Veins, Leptomeningeal Collaterals, and Prognosis. Front. Neurol. 2019, 10, 1292. [Google Scholar] [CrossRef]
- Kesavadas, C.; Santhosh, K.; Thomas, B. Susceptibility weighted imaging in cerebral hypoperfusion-can we predict increased oxygen extraction fraction? Neuroradiology 2010, 52, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Tamura, H.; Hatazawa, J.; Toyoshima, H.; Shimosegawa, E.; Okudera, T. Detection of deoxygenation-related signal change in acute ischemic stroke patients by T2*-weighted magnetic resonance imaging. Stroke 2002, 33, 967–971. [Google Scholar] [CrossRef] [PubMed]
- Celeste, F.; Muratori, M.; Mapelli, M.; Pepi, M. The Evolving Role and Use of Echocardiography in the Evaluation of Cardiac Source of Embolism. J. Cardiovasc. Echogr. 2017, 27, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Wu, B.; Hao, Z.; Kong, F.; Tao, W.; Wang, D.; He, S.; Liu, M. Characteristics, treatment and outcome of ischemic stroke with atrial fibrillation in a Chinese hospital-based stroke study. Cerebrovasc. Dis. 2011, 31, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wang, Y.; Akamatsu, Y.; Lee, C.C.; Stetler, R.A.; Lawton, M.T.; Yang, G.Y. Vascular remodeling after ischemic stroke: Mechanisms and therapeutic potentials. Prog. Neurobiol. 2014, 115, 138–156. [Google Scholar] [CrossRef] [PubMed]
- Shuaib, A.; Butcher, K.; Mohammad, A.A.; Saqqur, M.; Liebeskind, D.S. Collateral blood vessels in acute ischaemic stroke: A potential therapeutic target. Lancet Neurol. 2011, 10, 909–921. [Google Scholar] [CrossRef]
- Jiang, H.F.; Zhang, Y.Q.; Pang, J.X.; Shao, P.N.; Qiu, H.C.; Liu, A.F.; Li, C.; Jin, M.; Man, F.Y.; Jiang, W.J. Factors associated with prominent vessel sign on susceptibility-weighted imaging in acute ischemic stroke. Sci. Rep. 2021, 11, 5641. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wang, Y.; Guo, W.; Cheng, Y.; Zhang, S.; Wu, B.; Liu, M. Temporal trends of atrial fibrillation and/or rheumatic heart disease-related ischemic stroke, and anticoagulant use in Chinese population: An 8-year study. Int. J. Cardiol. 2021, 322, 258–264. [Google Scholar] [CrossRef]
- Hatano, S. Experience from a multicentre stroke register: A preliminary report. Bull. World Health Organ. 1976, 54, 541–553. [Google Scholar]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef]
- Liu, J.; Wang, D.; Li, J.; Lin, J.; Xiong, Y.; Liu, B.; Wei, C.; Wu, B.; Ma, Z.; Zhang, S.; et al. Cerebral Microbleeds Do Not Predict Hemorrhagic Transformation in Acute Ischemic Stroke Patients with Atrial Fibrillation and/or Rheumatic Heart Disease. Curr. Neurovascular Res. 2017, 14, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Wei, C.; Liu, J.; Li, J.; Liu, M. A Non-linear Association Between Total Small Vessel Disease Score and Hemorrhagic Transformation After Ischemic Stroke With Atrial Fibrillation and/or Rheumatic Heart Disease. Front. Neurol. 2019, 10, 769. [Google Scholar] [CrossRef] [PubMed]
- Ott, B.; Zamani, A.; Kleefield, J.; Funkenstein, H. The clinical spectrum of hemorrhagic infarction. Stroke 1986, 17, 630–637. [Google Scholar] [CrossRef] [PubMed]
- Ye, C.; Wang, Y.; Song, Q.; Liu, J.; Wei, C.; Liu, M. Association Between Coagulation Function and Spontaneous Hemorrhagic Transformation in Acute Ischemic Stroke. Curr. Neurovascular Res. 2020, 17, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Hacke, W.; Kaste, M.; Fieschi, C.; von Kummer, R.; Davalos, A.; Meier, D.; Larrue, V.; Bluhmki, E.; Davis, S.; Donnan, G.; et al. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Second European-Australasian Acute Stroke Study Investigators. Lancet 1998, 352, 1245–1251. [Google Scholar] [CrossRef]
- Hacke, W.; Kaste, M.; Bluhmki, E.; Brozman, M.; Dávalos, A.; Guidetti, D.; Larrue, V.; Lees, K.; Medeghri, Z.; Machnig, T.; et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N. Engl. J. Med. 2008, 359, 1317–1329. [Google Scholar] [CrossRef]
- Li, J.; Zhang, P.; Wu, S.; Yi, X.; Wang, C.; Liu, M. Factors associated with favourable outcome in large hemispheric infarctions. BMC Neurol. 2018, 18, 152. [Google Scholar] [CrossRef]
- Zha, A.M.; Sari, M.; Torbey, M.T. Recommendations for management of large hemispheric infarction. Curr. Opin. Crit. Care 2015, 21, 91–98. [Google Scholar] [CrossRef]
- Terasawa, Y.; Yamamoto, N.; Morigaki, R.; Fujita, K.; Izumi, Y.; Satomi, J.; Harada, M.; Nagahiro, S.; Kaji, R. Brush sign on 3-T T2*-weighted MRI as a potential predictor of hemorrhagic transformation after tissue plasminogen activator therapy. Stroke 2014, 45, 274–276. [Google Scholar] [CrossRef]
- Wang, T.; Zhu, L.; Hu, C.; Gong, S.; Jiang, H.; Chen, H.; Li, J. The diagnostic value of susceptibility-weighted imaging for ischemic penumbra in patients with acute ischemic stroke. Technol. Health Care Off. J. Eur. Soc. Eng. Med. 2017, 25, 449–457. [Google Scholar] [CrossRef]
- Bivard, A.; Krishnamurthy, V.; Stanwell, P.; Yassi, N.; Spratt, N.; Nilsson, M.; Levi, C.; Davis, S.; Parsons, M. Spectroscopy of reperfused tissue after stroke reveals heightened metabolism in patients with good clinical outcomes. J. Cereb. Blood Flow Metab. Off. J. Int. Soc. Cereb. Blood Flow Metab. 2014, 34, 1944–1950. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhu, L.; Hou, B.; Wang, T.; Xu, D.; Tan, C.; Zhang, H.; Li, C.; Wang, J. Study on the correlation between the circle of Willis structure and collateral circulation in bilateral carotid artery occlusion. Neurol. Sci. 2021, 42, 5335–5342. [Google Scholar] [CrossRef] [PubMed]
- Iryo, Y.; Hirai, T.; Nakamura, M.; Inoue, Y.; Watanabe, M.; Ando, Y.; Azuma, M.; Nishimura, S.; Shigematsu, Y.; Kitajima, M.; et al. Collateral circulation via the circle of Willis in patients with carotid artery steno-occlusive disease: Evaluation on 3-T 4D MRA using arterial spin labelling. Clin. Radiol. 2015, 70, 960–965. [Google Scholar] [CrossRef] [PubMed]
- Brouns, R.; De Deyn, P.P. The complexity of neurobiological processes in acute ischemic stroke. Clin. Neurol. Neurosurg. 2009, 111, 483–495. [Google Scholar] [CrossRef] [PubMed]
- Minhas, J.; Rook, W.; Panerai, R.; Hoiland, R.; Ainslie, P.; Thompson, J.; Mistri, A.; Robinson, T. Pathophysiological and clinical considerations in the perioperative care of patients with a previous ischaemic stroke: A multidisciplinary narrative review. Br. J. Anaesth. 2020, 124, 183–196. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2018, 49, e46–e110. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All | Mild-to-Moderate DMVs | Severe DMVs | p | |
|---|---|---|---|---|
| (n = 170) | (Grades ≤ 2, n = 149) | (Grade = 3, n = 21) | ||
| Clinical features | ||||
| Age (years), median (IQR) | 72 (60–78) | 71 (60–78) | 76 (57–79) | 0.519 |
| Male, n (%) | 68 (40.0) | 61 (40.9) | 7 (33.3) | 0.505 |
| Hypertension, n (%) | 74 (43.5) | 67 (45.0) | 7 (33.3) | 0.314 |
| Diabetes mellitus, n (%) | 49 (28.8) | 45 (30.2) | 4 (19.0) | 0.291 |
| Hyperlipidemia, n (%) | 35 (20.6) | 32 (21.5) | 3 (14.3) | 0.573 |
| Atrial fibrillation, n (%) | 140 (82.4) | 124 (83.2) | 16 (76.2) | 0.539 |
| Rheumatic heart disease, n (%) | 42 (24.7) | 38 (25.2) | 4 (19.0) | 0.601 |
| Congestive heart failure, n (%) | 14 (8.2) | 10 (6.7) | 4 (19.0) | 0.076 |
| Mitral valve stenosis, n (%) | 14 (8.2) | 14 (9.4) | 0 | 0.221 |
| Infective endocarditis, n (%) | 1 (0.6) | 1 (0.7) | 0 | 1 |
| Prior antiplatelet, n (%) | 49 (28.8) | 44 (29.5) | 5 (23.8) | 0.588 |
| Prior anticoagulation, n (%) | 30 (17.6) | 28 (18.8) | 2 (9.5) | 0.376 |
| Smoking, n (%) | 35 (20.6) | 31 (20.8) | 4 (19.0) | 1 |
| Drinking, n (%) | 26 (15.3) | 22 (14.8) | 4 (19.0) | 0.534 |
| Baseline NIHSS, median (IQR) | 8 (4–13) | 8 (4–12) | 15 (6.5–18) | 0.002 |
| Admission SBP, mmHg, mean (SD) | 134.5 (22.7) | 136.0 (22.6) | 124.6(21.4) | 0.031 |
| Admission DBP, mmHg, mean (SD) | 81.3 (14.5) | 81.7 (15.3) | 78.4 (16.5) | 0.355 |
| Onset-to-admission time, hours, median (IQR) | 24 (4–48) | 24 (4–48) | 5 (2.5–66) | 0.262 |
| Antiplatelet in hospital, n (%) | 137 (80.6) | 119 (79.9) | 18 (85.7) | 0.769 |
| Anticoagulation in hospital, n (%) | 53 (31.2) | 46 (30.9) | 7 (33.3) | 0.820 |
| 3-month mRS, median (IQR) | 2 (1–4) | 2 (1–3) | 4 (3–4) | 0.002 |
| Neuroimaging characteristics | ||||
| HT, n (%) | 74 (43.5) | 65 (43.6) | 9 (42.9) | 0.947 |
| HI, n (%) | 52 (30.6) | 46 (30.9) | 6 (28.6) | 0.830 |
| PH, n (%) | 22 (12.9) | 19 (12.8) | 3 (14.3) | 1 |
| Symptomatic HT, n (%) | 17 (10.0) | 12 (8.1) | 5 (23.8) | 0.41 |
| Large hemispheric infarction, n (%) | 57 (33.5) | 44 (29.5) | 13 (61.9) | 0.003 |
| Good Functional Outcome (3-Month mRS < 3, n = 88) | Poor Functional Outcome (3-Month mRS ≥ 3, n = 82) | p | |
|---|---|---|---|
| Clinical features | |||
| Age (years), median (IQR) | 69 (58–77) | 75 (61–80) | 0.020 |
| Male, n (%) | 39 (57.4) | 29 (42.6) | 0.234 |
| Hypertension, n (%) | 36 (48.6) | 38 (51.4) | 0.475 |
| Diabetes mellitus, n (%) | 21 (42.9) | 28 (57.1) | 0.139 |
| Hyperlipidemia, n (%) | 15 (42.9) | 20 (57.1) | 0.237 |
| Atrial fibrillation, n (%) | 75 (85.2) | 65 (79.3) | 0.308 |
| Rheumatic heart disease, n (%) | 21 (23.9) | 21 (25.6) | 0.792 |
| Congestive heart failure, n (%) | 4 (28.6) | 10 (71.4) | 0.070 |
| Mitral valve stenosis, n (%) | 6 (6.8) | 8 (9.8) | 0.486 |
| Infective endocarditis, n (%) | 0 | 1 (1.2) | 0.482 |
| Prior antiplatelet, n (%) | 26 (53.1) | 23 (46.9) | 0.830 |
| Prior anticoagulation, n (%) | 17 (56.7) | 13 (43.3) | 0.554 |
| Smoking, n (%) | 18 (51.4) | 17 (48.6) | 0.964 |
| Drinking, n (%) | 16 (61.5) | 10 (38.5) | 0.279 |
| Baseline NIHSS, median (IQR) | 5 (2–9) | 12 (8–16) | 0.001 |
| Admission SBP, mmHg, mean (SD) | 135.3 (21.4) | 133.7 (24.1) | 0.646 |
| Admission DBP, mmHg, mean (SD) | 83.3 (14.1) | 79.1 (16.6) | 0.046 |
| Onset-to-admission time, hours, median (IQR) | 23.5 (4–48) | 24 (3–48) | 0.998 |
| Antiplatelet in hospital, n (%) | 71 (51.8) | 66 (48.2) | 0.975 |
| Anticoagulation in hospital, n (%) | 38 (71.7) | 15 (28.3) | <0.001 |
| Neuroimaging characteristics | |||
| HT, n (%) | 26 (35.1) | 48 (64.9) | 0.001 |
| Large hemispheric infarction, n (%) | 15 (26.3) | 42 (73.7) | 0.001 |
| DMVs grade, n (%) | <0.001 | ||
| Mild-to-moderate DMVs | 85 (96.6) | 64 (78.0) | |
| Severe DMVs | 3 (3.4) | 18 (22.0) |
| Unadjusted | Adjusted | |||||
|---|---|---|---|---|---|---|
| Variable | OR | 95% CI | p | OR | 95% CI | p |
| Severe DMVs | 7.769 | 2.25–28.22 | 0.001 | 5.830 | 1.266–26.856 | 0.024 |
| Age † | 1.023 | 0.998–1.048 | 0.068 | 1.026 | 0.993–1.059 | 0.124 |
| Baseline NIHSS † | 1.237 | 1.151–1.328 | <0.001 | 1.191 | 1.099–1.290 | <0.001 |
| DBP on admission † | 0.982 | 0.963–1.002 | 0.078 | 0.982 | 0.957–1.008 | 0.174 |
| Congestive heart failure | 2.917 | 0.877–9.698 | 0.081 | 2.671 | 0.506–14.088 | 0.247 |
| Anticoagulation in hospital | 0.295 | 0.146–0.594 | 0.001 | 0.393 | 0.154–1.006 | 0.051 |
| Presence of HT | 3.367 | 1.785–6.350 | <0.001 | 1.355 | 0.569–3.226 | 0.493 |
| Large hemispheric infarction | 5.110 | 2.526–10.336 | <0.001 | 1.747 | 0.689–4.426 | 0.240 |
| Variable | OR | 95% CI | p | p for Interaction |
|---|---|---|---|---|
| Age | 0.610 | |||
| <65 | 4.820 | 0.590–39.369 | 0.142 | |
| ≥65 | 4.371 | 0.442–43.209 | 0.207 | |
| Baseline NIHSS | 0.140 | |||
| <15 | 8.903 | 1.543–51.383 | 0.015 | |
| ≥15 | 2.271 | 0.158–32.637 | 0.546 | |
| Anticoagulation in hospital | 0.998 | |||
| Yes | 0.850 | 0.092–7.859 | 0.886 | |
| No | NA | NA | NA | |
| Presence of HT | 0.332 | |||
| Yes | 0.920 | 0.072–11.709 | 0.949 | |
| No | 15.071 | 1.823–124.583 | 0.012 | |
| Large hemispheric infarction | 0.646 | |||
| Yes | 21.515 | 0.526–880.754 | 0.105 | |
| No | 3.898 | 0.611–24.885 | 0.150 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ye, C.; Liu, J.; Wei, C.; Wang, Y.; Song, Q.; Pan, R.; Tao, W.; Wu, B.; Liu, M. Association between Deep Medullary Veins in the Unaffected Hemisphere and Functional Outcome in Acute Cardioembolic Stroke: An Observational Retrospective Study. Brain Sci. 2022, 12, 978. https://doi.org/10.3390/brainsci12080978
Ye C, Liu J, Wei C, Wang Y, Song Q, Pan R, Tao W, Wu B, Liu M. Association between Deep Medullary Veins in the Unaffected Hemisphere and Functional Outcome in Acute Cardioembolic Stroke: An Observational Retrospective Study. Brain Sciences. 2022; 12(8):978. https://doi.org/10.3390/brainsci12080978
Chicago/Turabian StyleYe, Chen, Junfeng Liu, Chenchen Wei, Yanan Wang, Quhong Song, Ruosu Pan, Wendan Tao, Bo Wu, and Ming Liu. 2022. "Association between Deep Medullary Veins in the Unaffected Hemisphere and Functional Outcome in Acute Cardioembolic Stroke: An Observational Retrospective Study" Brain Sciences 12, no. 8: 978. https://doi.org/10.3390/brainsci12080978
APA StyleYe, C., Liu, J., Wei, C., Wang, Y., Song, Q., Pan, R., Tao, W., Wu, B., & Liu, M. (2022). Association between Deep Medullary Veins in the Unaffected Hemisphere and Functional Outcome in Acute Cardioembolic Stroke: An Observational Retrospective Study. Brain Sciences, 12(8), 978. https://doi.org/10.3390/brainsci12080978