
Visuomotor Tracking Task for Enhancing Activity in Motor Areas of Stroke Patients


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
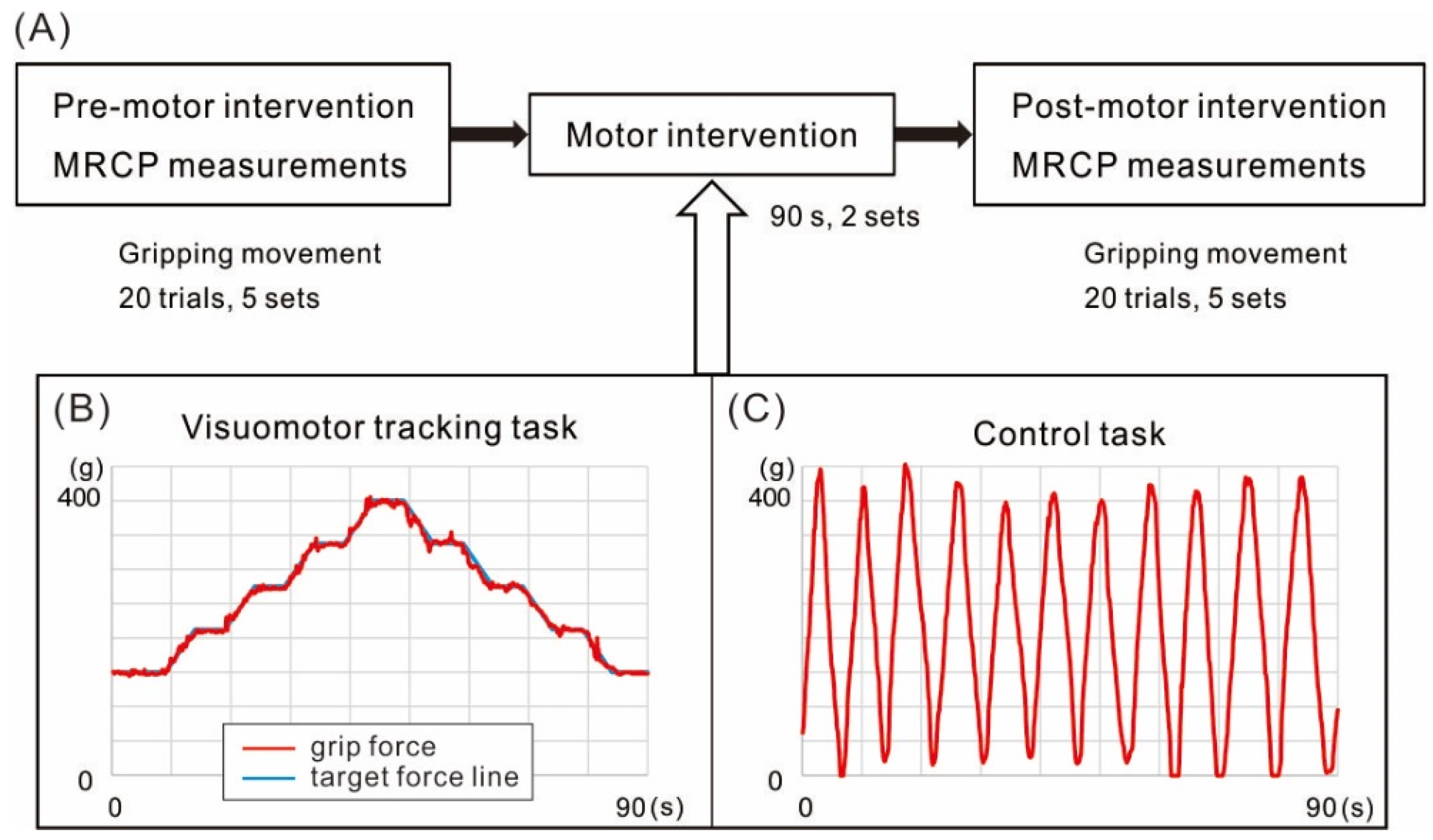
2.2. Two Manual Tasks of Motor Intervention
2.3. Experimental Design
2.4. Electroencephalogram Recordings
2.5. Statistical Analyses
3. Results
3.1. Comparison of Gripping Force during MRCPs Measurement
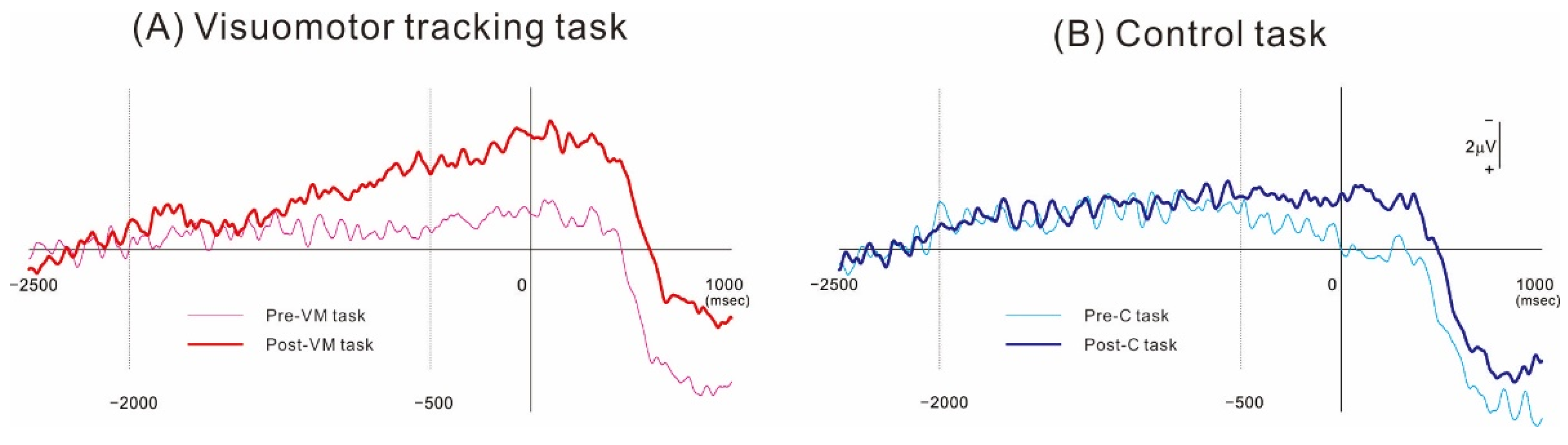
3.2. MRCP Measures from the Ipsilesional Hemisphere
3.3. MRCP Measures from the Contralesional Hemisphere
3.4. MRCP in the Normal Subjects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Takeuchi, N.; Tada, T.; Toshima, M.; Chuma, T.; Matsuo, Y.; Ikoma, K. Inhibition of the unaffected motor cortex by 1 Hz re-petitive transcranical magnetic stimulation enhances motor performance and training effect of the paretic hand in patients with chronic stroke. J. Rehabilit. Med. 2008, 40, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Khedr, E.M.; Abdel-Fadeil, M.R.; Farghali, A.; Qaid, M. Role of 1 and 3 Hz repetitive transcranial magnetic stimulation on motor function recovery after acute ischaemic stroke. Eur. J. Neurol. 2009, 16, 1323–1330. [Google Scholar] [CrossRef] [PubMed]
- Du, J.; Tian, L.; Liu, W.; Hu, J.; Xu, G.; Ma, M.; Fan, X.; Ye, R.; Jiang, Y.; Yin, Q.; et al. Effects of repetitive transcranial magnetic stimulation on motor recovery and motor cortex excitability in patients with stroke: A ran-domized controlled trial. Eur. J. Neurol. 2016, 23, 1666–1672. [Google Scholar] [CrossRef] [PubMed]
- Du, J.; Yang, F.; Hu, J.; Hu, J.; Xu, Q.; Cong, N.; Zhang, Q.; Liu, L.; Mantini, D.; Zhang, Z.; et al. Effects of high- and low-frequency repetitive transcranial magnetic stimulation on motor recovery in early stroke patients: Evidence from a ran-domized controlled trial with clinical, neurophysiological and functional imaging assessments. NeuroImage Clin. 2019, 21, 101620. [Google Scholar] [CrossRef] [PubMed]
- Taub, E.; Miller, N.E.; Novack, T.A.; Cook, E.W., 3rd; Fleming, W.C.; Nepomuceno, C.S.; Connell, J.S.; Crago, J.E. Technique to improve chronic motor deficit after stroke. Arch. Phys. Med. Rehabilt. 1993, 74, 347–354. [Google Scholar]
- Taub, E.; Uswatte, G.; Pidikiti, R. Constraint-Induced Movement Therapy: A new family of techniques with broad application to physical rehabilitation--a clinical review. J. Rehabilit. Res. Dev. 1999, 36, 237–251. [Google Scholar]
- Liepert, J.; Bauder, H.; Miltner, W.H.R.; Taub, E.; Weiller, C. Treatment-Induced Cortical Reorganization after Stroke in Humans. Stroke 2000, 31, 1210–1216. [Google Scholar] [CrossRef]
- Pavlides, C.; Miyashita, E.; Asanuma, H. Projection from the sensory to the motor cortex is important in learning motor skills in the monkey. J. Neurophysiol. 1993, 70, 733–741. [Google Scholar] [CrossRef]
- Quaney, B.M.; He, J.; Timberlake, G.; Dodd, K.; Carr, C. Visuomotor training improves stroke-related ipsilesional upper ex-tremity impairments. Neurorehabilt. Neural Repair 2010, 24, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Kornhuber, H.H.; Deecke, L. Brain potential changes in voluntary and passive movements in humans: Readiness potential and reafferent potentials. Pflugers Arch. 2016, 468, 1115–1124. [Google Scholar] [CrossRef] [PubMed]
- Neshige, R.; Lüders, H.; Shibasaki, H. Recording of movement-related potentials from scalp and cortex in man. Brain 1988, 111, 719–736. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, A.; Lüders, H.O.; Burgess, R.C.; Shibasaki, H. Movement-related potentials recorded from supplementary motor area and primary motor area. Role of supplementary motor area in voluntary movements. Brain 1992, 115, 1017–1043. [Google Scholar] [CrossRef] [PubMed]
- Honda, M.; Nagamine, T.; Fukuyama, H.; Yonekura, Y.; Kimura, J.; Shibasaki, H. Movement-related cortical potentials and regional cerebral blood flow change in patients with stroke after motor recovery. J. Neurol. Sci. 1997, 146, 117–126. [Google Scholar] [CrossRef]
- Kaneno, T.; Sato, A.; Akizuki, K.; Yamaguchi, A.; Yasaki, K.; Morita, Y. Assessing the adjustability of grasping force using the iWakka in elderly individuals. J. Phys. Ther. Sci. 2017, 29, 2215–2219. [Google Scholar] [CrossRef] [PubMed]
- Oda, S.; Shibata, M.; Moritani, T. Force-dependent changes in movement-related cortical potentials. J. Electromyogr. Kinesiol. 1996, 6, 247–252. [Google Scholar] [CrossRef]
- Siemionow, V.; Yue, G.H.; Ranganathan, V.K.; Liu, J.Z.; Sahgal, V. Relationship between motor activity-related cortical po-tential and voluntary muscle activation. Exp. Brain Res. 2000, 133, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Wasaka, T.; Nakata, H.; Kida, T.; Kakigi, R. Changes in the centrifugal gating effect on somatosensory evoked potentials de-pending on the level of contractile force. Exp. Brain Res. 2005, 166, 118–125. [Google Scholar] [CrossRef]
- Schillings, M.L.; Kalkman, J.S.; van der Werf, S.P.; Bleijenberg, G.; van Engelen, B.G.M.; Zwarts, M.J. Central adaptations during repetitive contractions assessed by the readiness potential. Eur. J. Appl. Physiol. 2006, 97, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Siemionow, V.; Fang, Y.; Calabrese, L.; Sahgal, V.; Yue, G.H. Altered central nervous system signal during motor performance in chronic fatigue syndrome. Clin. Neurophysiol. 2004, 115, 2372–2381. [Google Scholar] [CrossRef] [PubMed]
- Berchicci, M.; Menotti, F.; Macaluso, A.; Di Russo, F. The neurophysiology of central and peripheral fatigue during sub-maximal lower limb isometric contractions. Front. Hum. Neurosci. 2013, 7, 135. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Shibasaki, H.; Barrett, G.; Halliday, E.; Halliday, A.M. Components of the movement-related cortical potential and their scalp topography. Electroencephalogr. Clin. Neurophysiol. 1980, 49, 213–226. [Google Scholar] [CrossRef]
- Hummel, F.; Celnik, P.; Giraux, P.; Floel, A.; Wu, W.-H.; Gerloff, C.; Cohen, L.G. Effects of non-invasive cortical stimulation on skilled motor function in chronic stroke. Brain 2005, 128, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Bosnell, R.A.; Kincses, T.; Stagg, C.J.; Tomassini, V.; Kischka, U.; Jbabdi, S.; Woolrich, M.W.; Andersson, J.; Matthews, P.M.; Johansen-Berg, H. Motor Practice Promotes Increased Activity in Brain Regions Structurally Disconnected After Subcortical Stroke. Neurorehabilit. Neural Repair 2011, 25, 607–616. [Google Scholar] [CrossRef] [PubMed]
- Russo, C.; Veronelli, L.; Casati, C.; Monti, A.; Perucca, L.; Ferraro, F.; Corbo, M.; Vallar, G.; Bolognini, N. Explicit motor se-quence learning after stroke: A neuropsychological study. Exp. Brain Res. 2021, 239, 2303–2316. [Google Scholar] [CrossRef] [PubMed]
- Classen, J.; Gerloff, C.; Honda, M.; Hallett, M. Integrative visuomotor behavior is associated with interregionally coherent oscillations in the human brain. J. Neurophysiol. 1998, 79, 1567–1573. [Google Scholar] [CrossRef] [PubMed]
- Carey, D.P.; Liddle, J. Hemifield or hemispace: What accounts for the ipsilateral advantages in visually guided aiming? Exp. Brain Res. 2013, 230, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Sterr, A.; Shen, S.; Kranczioch, C.; Szameitat, A.J.; Hou, W.; Sorger, B. fMRI effects of task demand and feedback accuracy on grip force tracking. Neurosci. Lett. 2009, 457, 61–65. [Google Scholar] [CrossRef]
- Karni, A.; Meyer, G.; Jezzard, P.; Adams, M.M.; Turner, R.; Ungerleider, L.G. Functional MRI evidence for adult motor cortex plasticity during motor skill learning. Nature 1995, 377, 155–158. [Google Scholar] [CrossRef]
- Taylor, M.J. Bereitschaftspontential during the acquisition of a skilled motor task. Electroencephalogr. Clin. Neurophysiol. 1978, 45, 568–576. [Google Scholar] [CrossRef]
- Lang, W.; Beisteiner, R.; Lindinger, G.; Deecke, L. Changes of cortical activity when executing learned motor sequences. Exp. Brain Res. 1992, 89, 435–440. [Google Scholar] [CrossRef]
- Kitamura, J.; Shibasaki, H.; Takeuchi, T. Cortical potentials preceding voluntary elbow movement in recovered hemiparesis. Electroencephalogr. Clin. Neurophysiol. 1996, 98, 149–156. [Google Scholar] [CrossRef]
- Yilmaz, O.; Birbaumer, N.; Ramos-Murguialday, A. Movement related slow cortical potentials in severely paralyzed chronic stroke patients. Front. Hum. Neurosci. 2015, 8, 1033. [Google Scholar] [CrossRef] [PubMed]
- Matsuura, A.; Onoda, K.; Oguro, H.; Yamaguchi, S. Magnetic stimulation and movement-related cortical activity for acute stroke with hemiparesis. Eur. J. Neurol. 2015, 22, 1526–1532. [Google Scholar] [CrossRef]
- Wade, D.T.; Langton-Hewer, R.; Wood, V.A.; Skilbeck, C.E.; Ismail, H.M. The hemiplegic arm after stroke: Measurement and recovery. J. Neurol. Neurosurg. Psychiatry 1983, 46, 521–524. [Google Scholar] [CrossRef] [PubMed]
- Swayne, O.B.; Rothwell, J.C.; Ward, N.S.; Greenwood, R.J. Stages of Motor Output Reorganization after Hemispheric Stroke Suggested by Longitudinal Studies of Cortical Physiology. Cereb. Cortex 2008, 18, 1909–1922. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patient | Age (Years) | Sex | Time since Stroke (Days) | Handedness | Type of Stroke | Paretic Side | FMA | MMSE |
|---|---|---|---|---|---|---|---|---|
| 1 | 69 | M | 59 | Right | infarction | Left | 27 | 27 |
| 2 | 67 | F | 38 | Right | infarction | Right | 58 | 30 |
| 3 | 65 | M | 145 | Right | hemorrhage | Right | 63 | 14 |
| 4 | 70 | F | 100 | Right | hemorrhage | Right | 54 | 23 |
| 5 | 83 | M | 72 | Right | infarction | Right | 60 | 24 |
| 6 | 62 | M | 91 | Left | infarction | Right | 60 | 26 |
| 7 | 49 | M | 43 | Right | infarction | Right | 65 | 28 |
| 8 | 57 | M | 51 | Right | infarction | Right | 61 | 30 |
| 9 | 45 | M | 54 | Right | infarction | Left | 62 | 30 |
| 10 | 59 | M | 48 | Left | hemorrhage | Right | 61 | 29 |
| 11 | 62 | F | 92 | Right | hemorrhage | Left | 57 | 25 |
| 12 | 53 | M | 72 | Right | hemorrhage | Right | 60 | 30 |
| 13 | 71 | M | 120 | Right | infarction | Right | 64 | 21 |
| 14 | 48 | F | 24 | Right | hemorrhage | Right | 59 | 30 |
| 15 | 54 | M | 63 | Right | hemorrhage | Right | 50 | 30 |
| 16 | 68 | F | 73 | Right | hemorrhage | Right | 45 | 18 |
| 17 | 67 | F | 92 | Right | hemorrhage | Right | 59 | 30 |
| 18 | 36 | F | 64 | Right | infarction | Left | 18 | 30 |
| 19 | 75 | M | 29 | Right | infarction | Right | 62 | 26 |
| 20 | 59 | M | 37 | Right | infarction | Right | 59 | 30 |
| 21 | 68 | M | 36 | Right | infarction | Right | 33 | 26 |
| Peak Amplitude (g) | Control Task | Visuomotor Tracking Task | ||
| Pre | Post | Pre | Post | |
| Mean | 411.7 | 404.6 | 406.5 | 407.2 |
| SD | 44.1 | 41.8 | 36.5 | 39.8 |
| Peak Latency (ms) | Control Task | Visuomotor Tracking Task | ||
| Pre | Post | Pre | Post | |
| Mean | 345.3 | 333.6 | 320.8 | 306.8 |
| SD | 161.2 | 153.2 | 164.5 | 160.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wasaka, T.; Ando, K.; Nomura, M.; Toshima, K.; Tamaru, T.; Morita, Y. Visuomotor Tracking Task for Enhancing Activity in Motor Areas of Stroke Patients. Brain Sci. 2022, 12, 1063. https://doi.org/10.3390/brainsci12081063
Wasaka T, Ando K, Nomura M, Toshima K, Tamaru T, Morita Y. Visuomotor Tracking Task for Enhancing Activity in Motor Areas of Stroke Patients. Brain Sciences. 2022; 12(8):1063. https://doi.org/10.3390/brainsci12081063
Chicago/Turabian StyleWasaka, Toshiaki, Kohei Ando, Masakazu Nomura, Kazuya Toshima, Tsukasa Tamaru, and Yoshifumi Morita. 2022. "Visuomotor Tracking Task for Enhancing Activity in Motor Areas of Stroke Patients" Brain Sciences 12, no. 8: 1063. https://doi.org/10.3390/brainsci12081063
APA StyleWasaka, T., Ando, K., Nomura, M., Toshima, K., Tamaru, T., & Morita, Y. (2022). Visuomotor Tracking Task for Enhancing Activity in Motor Areas of Stroke Patients. Brain Sciences, 12(8), 1063. https://doi.org/10.3390/brainsci12081063