
Use of Riluzole for the Treatment of Hereditary Ataxias: A Systematic Review

 , ,
, ,  , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
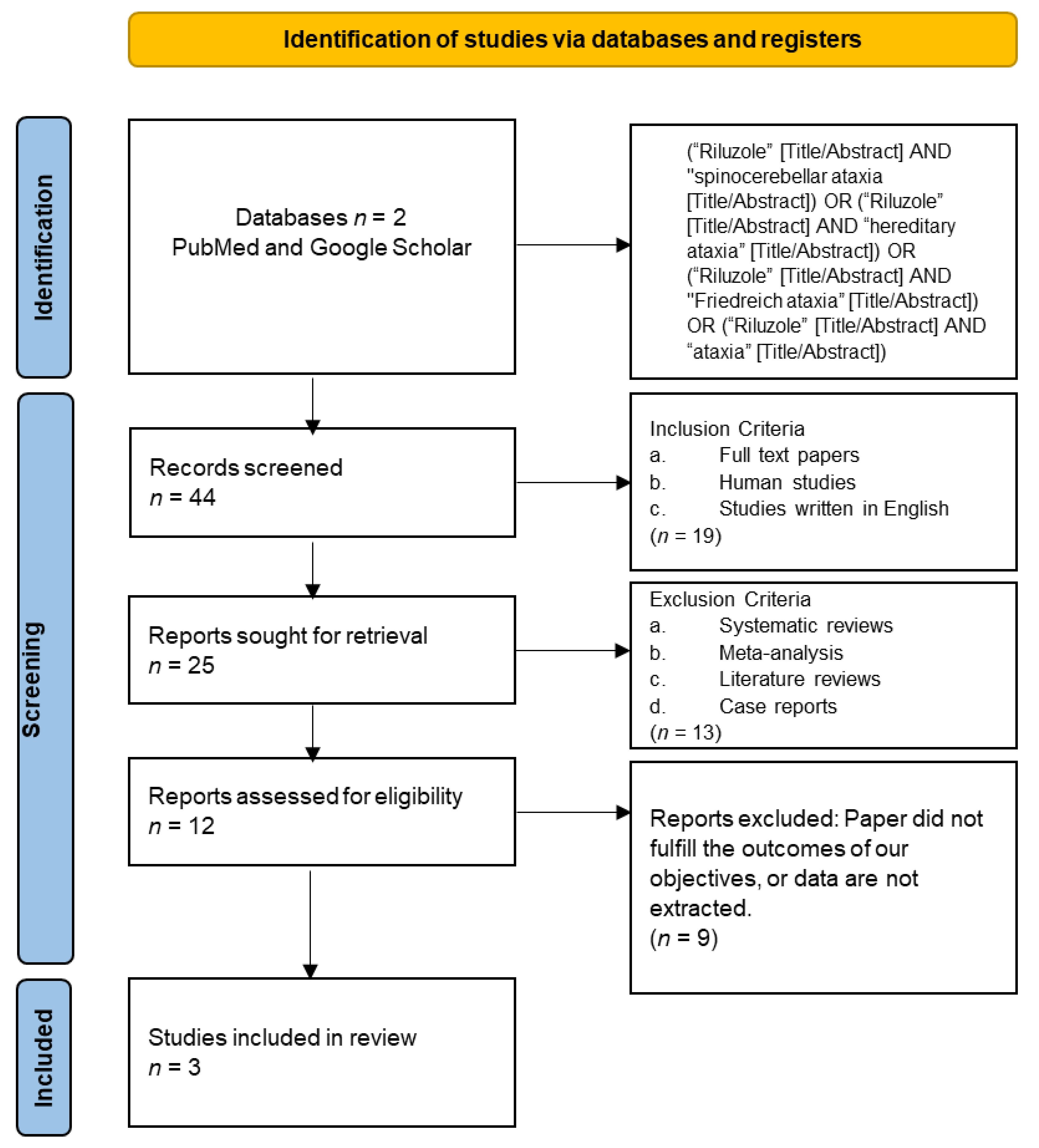
2.1.1. Eligibility Criteria and Study Selection
2.1.2. Database and Search Strategy
2.1.3. Data Extraction and Analysis
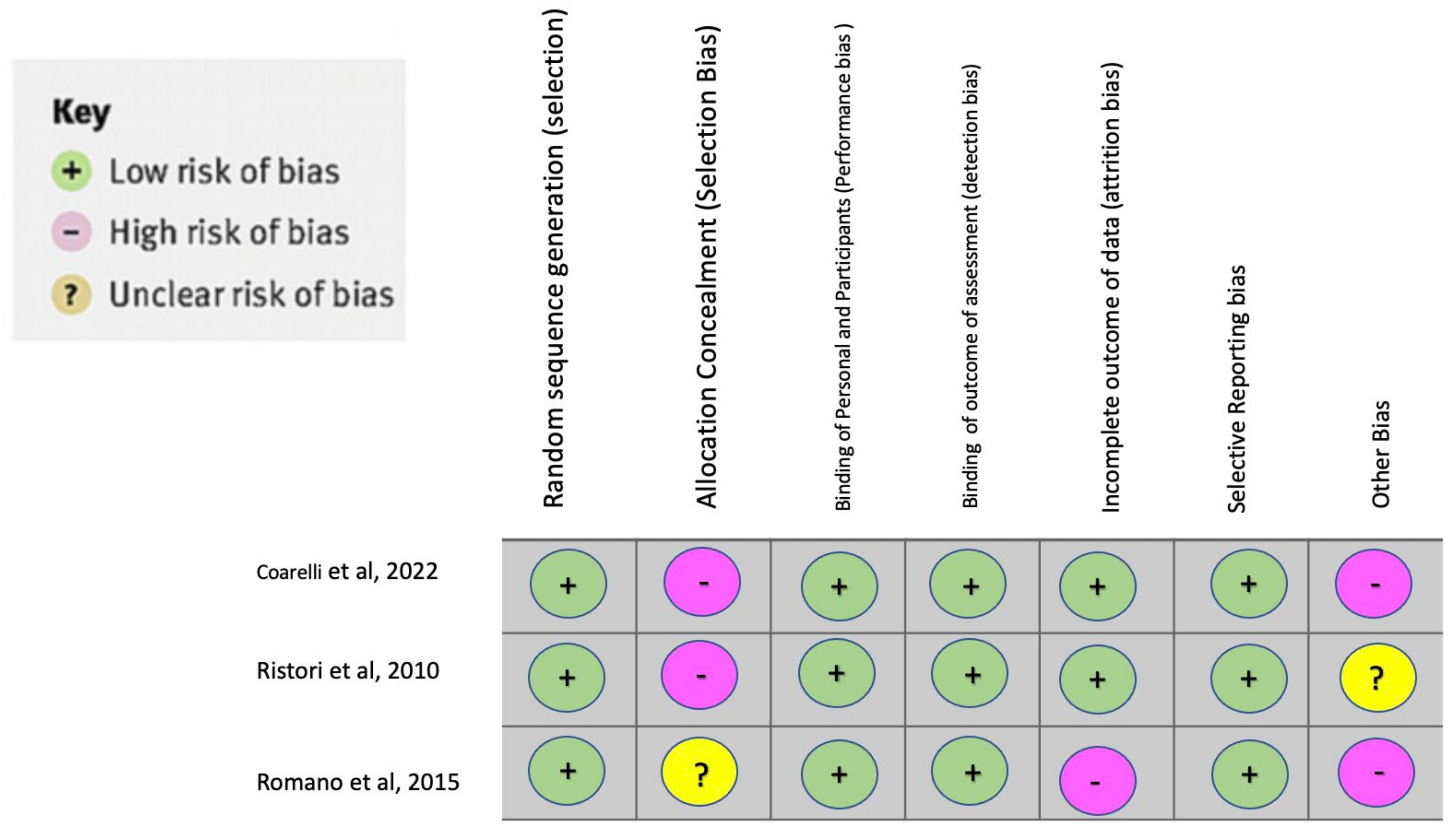
2.1.4. Bias Assessment
3. Results
3.1. Study Characteristics
3.2. Study Limitations
4. Discussion
4.1. Rationale of Riluzole for Hereditary Ataxia
4.2. Clinical Trials of Riluzole for Hereditary Ataxia
5. New Perspectives (Future)
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miller, R.G.; Mitchell, J.D.; Moore, D.H. Riluzole for amyotrophic lateral sclerosis (ALS)/motor neuron disease (MND). Cochrane Database Syst. Rev. 2012, Online First. [Google Scholar] [CrossRef]
- Cifra, A.; Mazzone, G.L.; Nistri, A. Riluzole: What it does to spinal and brainstem neurons and how it does it. Neuroscientist 2013, 19, 137–144. [Google Scholar] [CrossRef]
- Kuo, S.-H. Ataxia. Continuum 2019, 25, 1036–1054. [Google Scholar] [CrossRef] [PubMed]
- Delatycki, M.B.; Bidichandani, S.I. Friedreich ataxia—Pathogenesis and implications for therapies. Neurobiol. Dis. 2019, 132, 104606. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, R.; Yau, W.Y.; O’Connor, E.; Houlden, H. Spinocerebellar ataxia: An update. J. Neurol. 2019, 266, 533–544. [Google Scholar] [CrossRef] [PubMed]
- Dade, M.; Berzero, G.; Izquierdo, C.; Giry, M.; Benazra, M.; Delattre, J.Y.; Psimaras, D.; Alentorn, A. Neurological Syndromes Associated with Anti-GAD Antibodies. Int. J. Mol. Sci. 2020, 21, E3701. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, J.F.; Betté, S.; Tambo, W.; Tao, F.; Cozar, J.C.; Isaacson, S. Multiple System Atrophy—Cerebellar Type: Clinical Picture and Treatment of an Often-Overlooked Disorder. Cureus 2020, 12, e10741. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Coarelli, G.; Heinzmann, A.; Ewenczyk, C.; Fischer, C.; Chupin, M.; Monin, M.L.; Hurmic, H.; Calvas, F.; Calvas, P.; Goizet, C.; et al. Safety and efficacy of riluzole in spinocerebellar ataxia type 2 in France (ATRIL): A multicentre, randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2022, 21, 225–233. [Google Scholar] [CrossRef]
- Ristori, G.; Romano, S.; Visconti, A.; Cannoni, S.; Spadaro, M.; Frontali, M.; Pontieri, F.E.; Vanacore, N.; Salvetti, M. Riluzole in cerebellar ataxia: A randomized, double-blind, placebo-controlled pilot trial. Neurology 2010, 74, 839–845. [Google Scholar] [CrossRef] [PubMed]
- Romano, S.; Coarelli, G.; Marcotulli, C.; Leonardi, L.; Piccolo, F.; Spadaro, M.; Frontali, M.; Ferraldeschi, M.; Vulpiani, M.C.; Ponzelli, F.; et al. Riluzole in patients with hereditary cerebellar ataxia: A randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2015, 14, 985–991. [Google Scholar] [CrossRef]
- Romano, S.; Coarelli, G.; Vanacore, N.; Salvetti, M.; Ristori, G. Riluzole in patients with hereditary cerebellar ataxia—Authors’ reply. Lancet Neurol. 2016, 15, 789. [Google Scholar] [CrossRef]
- Schmidt, J.; Schmidt, T.; Golla, M.; Lehmann, L.; Weber, J.J.; Hübener-Schmid, J.; Riess, O. In vivo assessment of riluzole as a potential therapeutic drug for spinocerebellar ataxia type 3. J. Neurochem. 2016, 138, 150–162. [Google Scholar] [CrossRef] [PubMed]
- Rahimi Shourmasti, F.; Goudarzi, I.; Lashkarbolouki, T.; Abrari, K.; Elahdadi Salmani, M.; Goudarzi, A. Effects of riluzole on harmaline induced tremor and ataxia in rats: Biochemical, histological and behavioral studies. Eur. J. Pharmacol. 2012, 695, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Janahmadi, M.; Goudarzi, I.; Kaffashian, M.R.; Behzadi, G.; Fathollahi, Y.; Hajizadeh, S. Co-treatment with riluzole, a neuroprotective drug, ameliorates the 3-acetylpyridine-induced neurotoxicity in cerebellar Purkinje neurones of rats: Behavioural and electrophysiological evidence. Neurotoxicology 2009, 30, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Velázquez-Pérez, L.; Rodríguez-Labrada, R. Riluzole and spinocerebellar ataxia type 2: The ATRIL trial. Lancet Neurol. 2022, 21, 204–205. [Google Scholar] [CrossRef]
- Brandsma, R.; Kremer, H.P.H.; Sival, D.A. Riluzole in patients with hereditary cerebellar ataxia. Lancet Neurol. 2016, 15, 788. [Google Scholar] [CrossRef]
- Ortiz, J.F.; Khan, S.A.; Salem, A.; Lin, Z.; Iqbal, Z.; Jahan, N. Post-Marketing Experience of Edaravone in Amyotrophic Lateral Sclerosis: A Clinical Perspective and Comparison with the Clinical Trials of the Drug. Cureus. 2020, 12, e10818. [Google Scholar] [CrossRef] [PubMed]
- Ristori, G. Riluzole in Patients with Spinocerebellar Ataxia Type 7: A Randomized, Double-blind, Placebo-controlled Pilot Trial with a Lead in Phase. 2018. Available online: clinicaltrials.gov (accessed on 20 June 2022).
- University of California, Los Angeles: An Open Pilot Trial of BHV-4157 in Adult Subjects with Cerebellar Ataxia. 2022. Available online: clinicaltrials.gov (accessed on 20 June 2022).
- Ristori, G. Efficacy of Riluzole in Hereditary Cerebellar Ataxia: A Randomized Double-Blind Placebo-Controlled Trial. 2015. Available online: clinicaltrials.gov (accessed on 20 June 2022).
- Assistance Publique—Hôpitaux de Paris: Multicenter, Randomized, Double Blind, Placebo Controlled Clinical Trial with Riluzole in Spinocerebellar Ataxia Type 2. 2021. Available online: clinicaltrials.gov (accessed on 20 June 2022).
- Andrea, S. Hospital: Phase 2 Study of Riluzole Effects on Patients With Chronic Cerebellar Ataxia. 2014. Available online: clinicaltrials.gov (accessed on 20 June 2022).


{kind=link}
{kind=link}
{kind=link}
| Hereditary Ataxia | Clinical Features |
|---|---|
| Friedreich’s ataxia [4] | The most common disorder is FRDA, caused by a GAA trinucleotide repeat expansion in the Frataxin gene. FRDA causes progressive ataxia, dysarthria, cardiomyopathy, and an increased risk of diabetes mellitus; most patients require a wheelchair by the age of 15 with a marked reduction in lifespan, with the onset of death being around 36 years. |
| Spinocerebellar ataxia [5] | Transmitted in an autosomal dominant fashion; caused by CAG nucleotide repeat expansions that encode polyglutamine. The classic triad of SCAs includes gait ataxia and incoordination, nystagmus, and dysarthria; however, patients can present with additional findings such as pyramidal or cognitive dysfunction. In the last decade, much progress has been made by targeting downstream pathways with antisense oligonucleotides (ASOs), providing therapeutic relief in some patients. |
| GAD-related neurological syndrome [6] | GAD-related neurological syndrome, specifically cerebellar ataxia, is another rare hereditary autoimmune cerebellar disorder associated with genetic and environmental risk factors and the presence of GAD (glutamic acid decarboxylase) antibodies. The pathogenic role of GAD Ab in cerebellar ataxia is a reduced GABAergic transmission. The clinical presentation includes gait ataxia, dysarthria, and nystagmus, corresponding to primary participation of the cerebellar vermis. The disease shows a symptom onset that ranges from subacute to chronic, and the disease progression can last from months to years. Brain MRI reveals vermis atrophy, and CSF analysis shows CSF-specific oligoclonal bands and intrathecal synthesis of GAD Ab. |
| Multiple system atrophy—cerebellar phenotype [7] | MSA is part of the family of a-synucleinopathies, and there are two main types, the MSA parkinsonian type (MSA-P) and cerebellar (MSA-C). MSA-C type is caused by olivopontocerebellar atrophy degeneration. The main symptoms are gait and limb ataxia, dysarthria, eye movement abnormalities such as dysmetria, and saccadic intrusion. The diagnosis is mainly clinical, and treatment is only symptomatic. |
| Author and Year of Publication | Country | Study Design | No. of Pts. in the Treatment Group | No. of Pts. in the Control Group | Patient Selection | Dose, Duration, Route, of Administration |
|---|---|---|---|---|---|---|
| Coarelli et al., 2022 [11] | France | Clinical Trial | 22 | 23 | Patients with SCA Type 2 | Riluzole 50 mg orally or placebo twice per day for 12 months |
| Romano et al., 2015 [13] | Italy | Clinical trial | 28 (19 SCA; 9 FRDA) | 27 (19 SCA; 8 FRDA) | Patients with SCA or FRDA | Riluzole 50 mg orally or placebo twice daily for 12 months |
| Ristori et al., 2010 [12] | Italy | Clinical trial | 19 | 19 | Patients with cerebellar ataxias of different etiologies: 8 FRDA, 8 SCA (type 1 (2), type 2 (4), type 2b (2)), 6 multiple system atrophy type C, 2 multiple sclerosis, 1 anti-GAD, 1 anti Yo, 13 ataxias of unknown origin | Riluzole 100 mg/day or placebo for 8 weeks |
| Author and Year of Publication | Country | Outcome | Results | Main Conclusion |
|---|---|---|---|---|
| Coarelli et al., 2022 [11] | France | SARA score | SARA score improved 1 point in 7 patients (32%) in the treatment group versus 9 patients in the placebo group (39%), with a mean difference of −10.3% (95% CI −37.4% to 19.2%; p = (0.75). There was a median increase in the SARA score by 0.5 points (IQR −1.5 to 1.5) in the riluzole group versus a 0.3 point (−1.0 to 2.5) increase in the placebo group (p = 0.70). In both groups, the number of patients who experienced adverse events was similar (Riluzole, 16 (73%) patients vs. placebo, 19 (83%) patients; p = 0.49). The severity of these parameters was measured with the Common Terminology Criteria for Adverse Events. | There was no clinical or radiological improvement in patients with SCA type 2 treated with riluzole. There were no serious adverse events reported in the riluzole group. The adverse events were not statistically significant compared to the control group. |
| Romano et al., 2015 [14] | Italy | SARA score | In the riluzole group, 14 of 28 (50%) patients showed an improvement in SARA score compared to 3 (11%) of 27 patients in the placebo group (OR 8.00, 95% CI 1.95–32.83; p = 0.002). There were no severe adverse events recorded in either group.Two participants in the riluzole group had an increase in liver enzymes (less than two times above normal limits). Mild adverse effects were recorded in two of the riluzole participants and two of the placebo participants. | Riluzole improved clinical outcomes in patients with SCA and FRDA with statistically significant results. The medication was well tolerated. |
| Ristori et al., 2010 [12] | Italy | ICARS | A 5-point reduction in the ICARS was considered clinically relevant at the time of the trial’s design. The riluzole group presented a significantly higher ICARS 5-point drop compared to placebo after 4 weeks in 9/19 treatment group versus 1/19 in the placebo group. (OR) = 16.2; 95% confidence interval (CI) 1.8–147.1) and After 8 weeks the ICARS 5-point drop drop in 13/19 cases in the treatment group versus 1/19 in the place group; OR = 39.0; 95% CI 4.2–364.2). In the subgroups of the ICAR 5 score, this were the results: Total ICARS Score: After treatment, the mean change in the riluzole group was 7.05 (4.96) versus 0.16 (2.65); (p < 0.001) in the placebo group. Static sub scores: Decreased in the treatment group −2.11 (2.75) versus 0.68 (1.94); (p < 0.001) in the place group. For kinetic function in the riluzole group the score changed −4.11 (2.96) versus 0.37 (2.0); (p < 0.001) in the placebo group. For Dysarthria there was an improvement in the function in the riluzole group −0.74 (0.81) versus 0.05 (0.40) (p < 0.001) in the placebo. Adverse effects were sporadic and minor. Values are mean (SD). | Riluzole was effective as symptomatic therapy in various disorders that cause cerebellar ataxia. The results were statically significant. There were no major side effects in either group, or the treatment was well tolerated. |
| Author and Year of Study Start Date | Study Name | Conditions treated | Primary Outcomes | Secondary Outcomes | Dose, Duration, Route, of Administration |
|---|---|---|---|---|---|
| Ristoroi G. 2018 [21]. | Riluzole in Patients with Spinocerebellar Ataxia Type 7. A Randomized, Double-blind, Placebo-controlled Pilot Trial with a Lead in Phase | Spinocerebellar Ataxia Type 7 | 1. Visual acuity expressed as log MAR units 2. Proportion of patients with stable SARA score | 1. Farnsworth D15 Arrangement Test 2. Visual evoked potentials 3. Electroretinography 4. Optical Coherence tomography 5. SARA score | Treated: Riluzole 50 mg Orally twice daily for 12 months Control: Placebo drug for 6 months and riluzole during the last 6 months of study |
| Perlman S. 2018 [22] | An Open Pilot Trial of BHV-4157 | SCA, SCA Type 1, SCA Type 2, SCA Type 3, SCA Type 6, and MSA-C | SARA Score | 1. 8-Meter Walk Test 2. Sheehan Suicidality Tracking Scale 3. Beck Depression Inventory 4. Beck Anxiety Inventory | BHV-4157 dose, duration, and route not specified |
| Ristoroi G. 2010 [23] | Efficacy of Riluzole in Hereditary Cerebellar Ataxia | Cerebellar Ataxia | SARA Score | 1. Baropodometric parameters 2. Quality of life: SF-36 3. Depression: Beck Scale | Riluzole 50 mg orally or placebo twice per day for 12 months |
| Durr A. 2018 [24] | Multicenter, Randomized, Double Blind, Placebo Controlled Clinical Trial with Riluzole in Spinocerebellar Ataxia Type 2 | Spinocerebellar Ataxia Type 2 | Change in Ataxia symptoms SARA score | 1. Change in Ataxia symptoms SARA Score 2. Change in extracerebellar symptoms (Inventory of Non-Ataxia Signs (INAS)) 3. 12 months survival | Riluzole 50 mg orally or placebo twice per day for 12 months |
| Ristoroi G. 2005 [25] | Phase 2 Study of Riluzole Effects on Patients with Chronic Cerebellar Ataxia | Cerebellar Ataxia Hereditary Ataxia Multiple Sclerosis | ICARS total scores and subscores (oculomotor, kinetic, postural, speech) | None | Riluzole 50 mg orally or placebo twice per day for 8 weeks |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayala, I.N.; Aziz, S.; Argudo, J.M.; Yepez, M.; Camacho, M.; Ojeda, D.; Aguirre, A.S.; Oña, S.; Andrade, A.F.; Vasudhar, A.; et al. Use of Riluzole for the Treatment of Hereditary Ataxias: A Systematic Review. Brain Sci. 2022, 12, 1040. https://doi.org/10.3390/brainsci12081040
Ayala IN, Aziz S, Argudo JM, Yepez M, Camacho M, Ojeda D, Aguirre AS, Oña S, Andrade AF, Vasudhar A, et al. Use of Riluzole for the Treatment of Hereditary Ataxias: A Systematic Review. Brain Sciences. 2022; 12(8):1040. https://doi.org/10.3390/brainsci12081040
Chicago/Turabian StyleAyala, Iván Nicolas, Syed Aziz, Jennifer M. Argudo, Mario Yepez, Mikaela Camacho, Diego Ojeda, Alex S. Aguirre, Sebastian Oña, Andres F. Andrade, Ananya Vasudhar, and et al. 2022. "Use of Riluzole for the Treatment of Hereditary Ataxias: A Systematic Review" Brain Sciences 12, no. 8: 1040. https://doi.org/10.3390/brainsci12081040
APA StyleAyala, I. N., Aziz, S., Argudo, J. M., Yepez, M., Camacho, M., Ojeda, D., Aguirre, A. S., Oña, S., Andrade, A. F., Vasudhar, A., Moncayo, J. A., Hassen, G., Ortiz, J. F., & Tambo, W. (2022). Use of Riluzole for the Treatment of Hereditary Ataxias: A Systematic Review. Brain Sciences, 12(8), 1040. https://doi.org/10.3390/brainsci12081040