
Customized Manual Muscle Testing for Post-Stroke Upper Extremity Assessment


Abstract
:1. Introduction
1.1. Functional Diagnosis of Post-Stroke Patients’ Upper Extremities
1.2. Manual Muscle Testing Scoring System and Its Patient-Customized Variations
- (a)
- (b)
- the Kendall Scale, which uses a percentage gradation of the muscle strength and assesses individual muscles [14];
- (c)
- Daniel and Worthingham’s scale, which uses a five-point scale defined as normal, good, fair, poor, trace and zero, and assesses muscles that perform a joint motion, rather than individual muscles [15];
- (d)
1.3. Customizing the Manual Muscle Testing Scoring System for Post-Stroke Patients
- -
- Patient-related: When using the MMT scoring scale for patients with stroke or significant neuromotor dysfunctions, a constraint of the classical MMT is that muscle force is evaluated on an ordinal scale rather than a continuous scale [21]. Thus, subtle variations in muscle strength are challenging to identify, especially because, in neuro-rehabilitation, the recovery process is longer than that in other rehabilitation areas (musculoskeletal, post trauma etc.). These issues are of primary clinical importance because although small changes in post-stroke muscle force may not be evident on the MMT scale, slight improvements in muscle strength may be enough to adjust the training programs or the goals set for stroke patients [15,21].
- -
- Examiner-related: The results of the MMT scale depends on the examiner’s skills to provide external resistance to the motion performed by the patient, especially with regard to the 4th and 5th grades, at least in regard to Daniel and Worthingham’s testing [15]. In addition to the resistance provided by gravity to the weight of the mobilized segment, the therapist tries to bring the segment into the initial position after the movement has been performed for the complete amplitude, with an added resistance of a moderate type (defined as the 4th grade) or with a maximum resistance or a breaktest (defined as the 5th grade/‘normal’/’good’ depending on the variant used). Moreover, the assessment may fluctuate, if in a clinical examination or study, there are more examiners working with different patients. Previous studies highlight that, due to MMT variability, the results of the inter-rater reliability values are disputable [20,23]. Finally, it can be challenging for inexperienced physicians or physiotherapists (with 5 to 10 years of experience) to distinguish subtle fluctuations in muscle force when using MMT [24].
- -
- Scoring-related: Since significant differences may be considered in the six-point scale of the MMT system, its guidelines suggest using the symbols ‘+/−‘before or after the scoring numbers so as to give a more accurate framework for assessing muscle strength [25]. In addition to the MMT scoring differences, another important reasoning for customizing the MMT scale for post-stroke patients is the technique used in muscle strength evaluation. The Kendall technique implies individual muscle assessment and, at present, its beneficial didactic and instructional value is preserved. However, it cannot be used in clinical programs, which need the assessment of synergistic muscle groups that perform movements on different motion axes. Daniel and Worthingham’s technique is also important in practice. It assesses muscle groups that mobilize a segment in a specific analytical direction of movement, and this way, it allows a more functional assessment that relates to directions of movement and muscle groups than is the case for a specific muscle. Therefore, the required assessment time is shorter, and, at the same time, important information is provided about the patient’s muscle strength. In neuro-rehabilitation, physical therapy programs focus on relearning functional movements by counteracting abnormal movement patterns characteristic of the post-stroke condition. Therefore, an assessment of muscle groups is more appropriate for establishing a functional diagnosis and setting goals [15]. Our research proposes a modified scoring for the MMT system that is customized for post-stroke patients, based on the active range of motion degrees, specific to each analytical motion and muscle group that performs the movement. We hypothesized that if we scored MMT based on a range of motion degrees that was divided into four sections, we could obtain more specific and accurate MMT values in post-stroke patients, which may be successfully used by clinicians and researchers. Moreover, by assessing the group muscles involved in unidirectional joint movement, the time used for the assessment would be reduced compared to a single muscle assessment (responding to an essential need of the human resources implied in the clinical assessment). Patients’ fatigue, which is a limiting factor of their physical activity and movement, would also be reduced. Therefore, our primary outcome was to identify if the adapted MMT scoring system was a reliable and valid tool in post-stroke assessment, and secondarily, to identify the muscle groups’ inference in the UE functionality for performing ADLs and thus predict the limb’s rehabilitation.
2. Materials and Methods
2.1. Study Localization and Ethical Issues
2.2. Participants
- (a)
- being a chronic survivor of a stroke that occurred more than six months and less than four years earlier;
- (b)
- not suffering from severe cognitive impairments, global or transcortical sensory aphasia, anemia, atrial fibrillation, or NYHA class IV heart failure;
- (c)
- having no other injury or dysfunction of the UE, such as fractures, periarthritis, or moderate-severe pain;
- (d)
- being able to perform at least 30-degree flexion and scapulohumeral abduction against gravity and at least 30-degree elbow flexion against gravity.
2.3. Outcome Measures
2.4. Procedures
2.4.1. Shoulder
2.4.2. Elbow
2.4.3. Forearm
2.4.4. Wrist
2.5. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, H.-T.; Huang, J.-J.; Pan, C.-W.; Chi, H.-I.; Pan, M.-C. Inertial Sensing Based Assessment Methods to Quantify the Effectiveness of Post-Stroke Rehabilitation. Sensors 2015, 15, 16196–16209. [Google Scholar] [CrossRef] [Green Version]
- Shih, M.M.; Rogers, J.C.; Skidmore, E.R.; Irrgang, J.J.; Holm, M.B. Measuring stroke survivors’ functional status independence: Five perspectives. Am. J. Occup. Ther. 2009, 63, 600–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teasell, R.; Hussein, N.; Mirkowski, M.; Vanderlaan, D.; Saikaley, M.; Longval, M.; Iruthayarajah, J. Hemiplegic Upper Extremity Rehabilitation. In Stroke Rehabilitation Handbook; Evidence-Based Review of Stroke Rehabilitation: London, ON, Canada, 2020; Available online: http://www.ebrsr.com/sites/default/files/EBRSR%20Handbook%20Chapter%204_Upper%20Extremity%20Post%20Stroke_ML.pdf (accessed on 5 March 2022).
- Pierella, C.; Pirondini, E.; Kinany, N.; Coscia, M.; Giang, C.; Miehlbradt, J.; Magnin, C.; Nicolo, P.; Dalise, S.; Sgherri, G.; et al. A multimodal approach to capture post-stroke temporal dynamics of recovery. J. Neural Eng. 2020, 17, 045002. [Google Scholar] [CrossRef]
- Tsuzuki, K.; Kawakami, M.; Nakamura, T.; Oshima, O.; Hijikata, N.; Suda, M.; Yamada, Y.; Okuyama, K.; Tsuji, T. Do somatosensory deficits predict efficacy of neurorehabilitation using neuromuscular electrical stimulation for moderate to severe motor paralysis of the upper limb in chronic stroke? Ther. Adv. Neurol. Disord. 2021, 14, 17562864211039335. [Google Scholar] [CrossRef]
- Woytowicz, E.J.; Rietschel, J.C.; Goodman, R.N.; Conroy, S.S.; Sorkin, J.D.; Whitall, J.; McCombe Waller, S. Determining Levels of Upper Extremity Movement Impairment by Applying a Cluster Analysis to the Fugl-Meyer Assessment of the Upper Extremity in Chronic Stroke. Arch. Phys. Med. Rehabil. 2017, 98, 456–462. [Google Scholar] [CrossRef] [Green Version]
- Stinear, C.M.; Smith, M.C.; Byblow, W.D. Prediction Tools for Stroke Rehabilitation. Stroke 2019, 50, 3314–3322. [Google Scholar] [CrossRef] [PubMed]
- O’Dell, M.W.; Lin, D.C.; Palagos, A. The physiatric history and physical examination. In Bradomm’s Physical Medicine and Rehabilitation, 5th ed.; Cifu, D.X., Ed.; Elsevier: Philadelphia, PA, USA, 2016; pp. 3–7. [Google Scholar]
- Essers, B.; Coremans, M.; Veerbeek, J.; Luft, A.; Verheyden, G. Daily Life Upper Limb Activity for Patients with Match and Mismatch between Observed Function and Perceived Activity in the Chronic Phase Post Stroke. Sensors 2021, 21, 5917. [Google Scholar] [CrossRef] [PubMed]
- Koroleva, E.S.; Kazakov, S.D.; Tolmachev, I.V.; Loonen, A.J.M.; Ivanova, S.A.; Alifirova, V.M. Clinical Evaluation of Different Treatment Strategies for Motor Recovery in Poststroke Rehabilitation during the First 90 Days. J. Clin. Med. 2021, 10, 3718. [Google Scholar] [CrossRef] [PubMed]
- Halmai, E.J. Quality and outcome measures for medical rehabilitation. In Braddom’s Rehabilitation Care: A Clinical Handbook, 1st ed.; Cifu, D., Lew, H.L., Eds.; Elsevier: Philadelphia, PA, USA, 2018; pp. 39–43. [Google Scholar]
- Gadotti, I.C.; Vieira, E.R.; Magee, D.J. Importance and Clarification of Measurement Properties in Rehabilitation. Rev. Bras. Fisioter. 2006, 10, 137–146. [Google Scholar] [CrossRef] [Green Version]
- Fawcett, A.L. Principles of Assessment and Outcome Measurement for Occupational Therapists and Physiotherapists: Theory, Skills and Application; John Wiley & Sons Ltd.: Chicester, UK, 2007; pp. 16–39. [Google Scholar]
- Kendall, F.P.; McCreary, E.K.; Provance, P.G. Muscles: Testing and Function with Posture and Pain. Baltimore, 5th ed.; Kendall, P., Ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005. [Google Scholar]
- Hislop, H.J.; Avers, D.; Brown, M. Worthingham’s Muscle Testing: Techniques of Manual Examination and Performance Testing, 1st ed.; Elsevier: St. Louis, IN, USA, 2019. [Google Scholar]
- Naqvi, U.; Sherman, A. Muscle strength grading. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK436008/ (accessed on 9 April 2021).
- Paternostro-Sluga, T.; Grim-Stieger, M.; Posch, M.; Schuhfried, O.; Vacariu, G.; Mittermaier, C.; Bittner, C.; Fialka-Moser, V. Reliability and validity of the Medical Research Council (MRC) scale and a modified scale for testing muscle strength in patients with radial palsy. J. Rehabil. Med. 2008, 40, 665–671. [Google Scholar] [CrossRef] [Green Version]
- Noreau, L.; Vachon, J. Comparison of three methods to assess muscular strength in individuals with spinal cord injury. Spinal Cord 1998, 36, 716–723. [Google Scholar] [CrossRef] [Green Version]
- Lovett, R.W.; Martin, E.G. Certain aspects of infantile paralysis and a description of a method of muscle testing. JAMA 1916, 66, 729–733. [Google Scholar] [CrossRef]
- Bohannon, R.W. Manual muscle testing: Does it meet the standards of an adequate screening test? Clin. Rehabil. 2005, 19, 662–667. [Google Scholar] [CrossRef]
- Ciesla, N.; Dinglas, V.; Fan, E.; Kho, M.; Kuramoto, J.; Needham, D. Manual muscle testing: A method of measuring extremity muscle strength applied to critically ill patients. J. Vis. Exp. 2011, 12, 2632. [Google Scholar] [CrossRef]
- Mahony, K.; Hunt, A.; Daley, D.; Sims, S.; Adams, R. Inter-Tester Reliability and Precision of Manual Muscle Testing and Hand-Held Dynamometry in Lower Limb Muscles of Children with Spina Bifida. Phys. Occup. Ther. Pediatr. 2009, 29, 44–59. [Google Scholar] [CrossRef]
- Cuthbert, S.C.; Goodheart, G.J., Jr. On the reliability and validity of manual muscle testing: A literature review. Chiropr. Osteopat. 2007, 15, 4. [Google Scholar] [CrossRef] [Green Version]
- Conable, K.M.; Rosner, A.L. A narrative review of manual muscle testing and implications for muscle testing research. J. Chiropr. Med. 2011, 10, 157–165. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, S.; Jaszczak, S.L.T.; Steffensen, A.K.S.; Debrabant, B. Using 4+ to grade near-normal muscle strength does not improve agreement. Chiropr. Man. Ther. 2017, 25, 28. [Google Scholar] [CrossRef] [Green Version]
- Rayegani, S.M.; Raeissadat, S.A.; Alikhani, E.; Bayat, M.; Bahrami, M.H.; Karimzadeh, A. Evaluation of complete functional status of patients with stroke by Functional Independence Measure scale on admission, discharge, and six months poststroke. Iran. J. Neurol. 2016, 15, 202–208. [Google Scholar]
- Quinn, T.J.; Taylor-Rowan, M.; Coyte, A.; Clark, A.; Musgrave, S.D.; Metcalf, A.K.; Day, D.J.; Bachmann, M.O.; Warburton, E.A.; Potter, J.F.; et al. Pre-Stroke Modified Rankin Scale: Evaluation of Validity, Prognostic Accuracy, and Association with Treatment. Front. Neurol. 2017, 8, 275. [Google Scholar] [CrossRef]
- Shinohara, Y.; Minematsu, K.; Amano, T.; Ohashi, Y. Modified Rankin Scale with Expanded Guidance Scheme and Interview Questionnaire: Interrater Agreement and Reproducibility of Assessment. Cerebrovasc. Dis. 2006, 21, 271–278. [Google Scholar] [CrossRef]
- Meseguer-Henarejos, A.-B.; Sánchez-Meca, J.; López-Pina, J.-A.; Carles-Hernández, R. Inter- and intra-rater reliability of the Modified Ashworth Scale: A systematic review and meta-analysis. Eur. J. Phys. Rehabil. Med. 2018, 54, 576–590. [Google Scholar] [CrossRef]
- Zurawski, E.; Behm, K.; Dunlap, C.; Koo, J.; Ismail, F.; Boulias, C.; Reid, S.; Phadke, C.P. Interrater Reliability of the Modified Ashworth Scale with Standardized Movement Speeds: A Pilot Study. Physiother. Can. 2019, 71, 348–354. [Google Scholar] [CrossRef]
- Beebe, J.A.; Lang, C.E. Active Range of Motion Predicts Upper Extremity Function 3 Months After Stroke. Stroke 2009, 40, 1772–1779. [Google Scholar] [CrossRef]
- Kim, S.-G.; Kim, E.-K. Test-retest reliability of an active range of motion test for the shoulder and hip joints by unskilled examiners using a manual goniometer. J. Phys. Ther. Sci. 2016, 28, 722–724. [Google Scholar] [CrossRef] [Green Version]
- Hernández, E.D.; Galeano, C.P.; Barbosa, N.E.; Forero, S.M.; Nordin, Å.; Sunnerhagen, K.S.; Alt Murphy, M. Intra- and inter-rater reliability of Fugl-Meyer Assessment of Upper Extremity in stroke. J. Rehabil. Med. 2019, 51, 652–659. [Google Scholar] [CrossRef] [Green Version]
- Roman, N.; Miclaus, R.; Repanovici, A.; Nicolau, C. Equal Opportunities for Stroke Survivors’ Rehabilitation: A Study on the Validity of the Upper Extremity Fugl-Meyer Assessment Scale Translated and Adapted into Romanian. Medicina 2020, 56, 409. [Google Scholar] [CrossRef]
- Amano, S.; Umeji, A.; Uchita, A.; Hashimoto, Y.; Takebayashi, T.; Takahashi, K.; Uchiyama, Y.; Domen, K. Clinimetric properties of the Fugl-Meyer assessment with adapted guidelines for the assessment of arm function in hemiparetic patients after stroke. Top. Stroke Rehabil. 2018, 25, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Yen, H.-C.; Luh, J.-J.; Teng, T.; Pan, G.-S.; Chen, W.-S.; Hsun, C.-C.; Jeng, J.-S. Reliability of lower extremity muscle strength measurements with handheld dynamometry in stroke patients during the acute phase: A pilot reliability study. J. Phys. Ther. Sci. 2017, 29, 317–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunnstrom, S.; Lehmkuhl, L.D.; Smith, L.K. Brunnstrom’s Clinical Kinesiology; F.A. Davis Co.: Philadelphia, PA, USA, 2012. [Google Scholar]
- Namdari, S.; Yagnik, G.; Ebaugh, D.D.; Nagda, S.; Ramsey, M.L.; Williams, G.R., Jr.; Mehta, S. Defining functional shoulder range of motion for activities of daily living. J. Shoulder Elb. Surg. 2012, 21, 1177–1183. [Google Scholar] [CrossRef] [PubMed]
- Jackson, J.E. Quartimax Rotation. In Encyclopedia of Biostatistics; Armitage, P., Colton, T., Eds.; Wiley StatsRef online: Hoboken, NJ, USA, 2014. [Google Scholar] [CrossRef]
- Koyuncu, I.; Kılıç, A.F. The use of exploratory and confirmatory factor analyses: A document analysis. Ted EgitimVeBilim 2019, 44, 361–388. [Google Scholar] [CrossRef]
- Schumacker, R.E.; Lomax, R.G. A Beginner’s Guide to Structural Equation Modeling, 3rd ed.; Routledge Academic: New York, NY, USA, 2010; pp. 83–88. [Google Scholar]
- Schmitt, W.H.; Cuthbert, S.C. Common errors and clinical guidelines for manual muscle testing: “the arm test” and other inaccurate procedures. Chiropr. Osteopat. 2008, 19, 16. [Google Scholar] [CrossRef] [Green Version]
- Barbano, R.L. Handbook of Manual Muscle Testing. Neurology 2000, 54, 1211. [Google Scholar] [CrossRef]
- Lang, C.E.; Bland, M.D.; Bailey, R.R.; Schaefer, S.Y.; Birkenmeier, R.L. Assessment of upper extremity impairment, function, and activity after stroke: Foundations for clinical decision making. J. Hand Ther. 2013, 26, 104–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, C.E.; Edwards, D.F.; Birkenmeier, R.L.; Dromerick, A.W. Estimating minimal clinically important differences of upper-extremity measures early after stroke. Arch. Phys. Med. Rehabil. 2008, 89, 1693–1700. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Zhao, G.; Zhou, Y.; Chen, X.; Ji, Z.; Wang, L. Relationship of EMG/SMG features and muscle strength level: An exploratory study on anterior muscles during plantar-flexion among hemiplegia patients. Biomed. Eng. Online 2014, 13, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Clarkson, H.M. Musculoskeletal Assessment: Joint Range of Motion and Manual Muscle Strength; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2000. [Google Scholar]
- Bohannon, R.W. Considerations and Practical Options for Measuring Muscle Strength: A Narrative Review. Biomed. Res. Int. 2019, 2019, 8194537. [Google Scholar] [CrossRef]
- Lewandowska-Sroka, P.; Stabrawa, R.; Kozak, D.; Poświata, A.; Łysoń-Uklańska, B.; Bienias, K.; Roksela, A.; Kliś, M.; Mikulski, M. The Influence of EMG-Triggered Robotic Movement on Walking, Muscle Force and Spasticity after an Ischemic Stroke. Medicina 2021, 57, 227. [Google Scholar] [CrossRef]
- Fayazi, M.; Dehkordi, S.N.; Dadgoo, M.; Salehi, M. Test-retest reliability of Motricity Index strength assessments for lower extremity in post stroke hemiparesis. Med. J. Islam. Repub. Iran 2012, 26, 27–30. [Google Scholar]
- Doussoulin, A.; Rivas, C.; Bacco, J.; Sepúlveda, P.; Carvallo, G.; Gajardo, C.; Soto, A.; Rivas, R. Prevalence of Spasticity and Postural Patterns in the Upper Extremity Post Stroke. J. Stroke Cerebrovasc. Dis. 2020, 29, 105253. [Google Scholar] [CrossRef]
- Schwarz, A.; Bhagubai, M.M.C.; Wolterink, G.; Held, J.P.O.; Luft, A.R.; Veltink, P.H. Assessment of Upper Limb Movement Impairments after Stroke Using Wearable Inertial Sensing. Sensors 2020, 20, 4770. [Google Scholar] [CrossRef]
- Mateo, S.; Roby-Brami, A.; Reilly, K.T.; Rossetti, Y.; Collet, C.; Rode, G. Upper limb kinematics after cervical spinal cord injury: A review. J. Neuroeng. Rehabil. 2015, 12, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, K.J.; Gallina, A.; Neva, J.L.; Ivanova, T.D.; Snow, N.J.; Ledwell, N.M.; Xiao, Z.G.; Menon, C.; Boyd, L.A.; Garland, S.J. Effect of repetitive transcranial magnetic stimulation combined with robot-assisted training on wrist muscle activation post-stroke. Clin. Neurophysiol. 2019, 130, 1271–1279. [Google Scholar] [CrossRef] [PubMed]
- Snickars, J.; Persson, H.; Sunnerhagen, K.S. Early clinical predictors of motor function in the upper extremity one month post-stroke. J. Rehabil. Med. 2017, 49, 216–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, X.L.; Tong, K.Y.; Wei, X.J.; Rong, W.; Susanto, E.A.; Ho, S. The effects of post-stroke upper-limb training with an electromyography (EMG)-driven hand robot. J. Electromyogr. Kinesiol. 2013, 23, 1065–1074. [Google Scholar] [CrossRef]
- Ballester, B.R.; Ward, N.S.; Brander, F.; Maier, M.; Kelly, K.; Verschure, P.F.M.J. Relationship between intensity and recovery in post-stroke rehabilitation: A retrospective analysis. J. Neurol. Neurosurg. Psychiatry 2021, 93, 226–228. [Google Scholar] [CrossRef]
- Adomavičienė, A.; Daunoravičienė, K.; Kubilius, R.; Varžaitytė, L.; Raistenskis, J. Influence of New Technologies on Post-Stroke Rehabilitation: A Comparison of Armeo Spring to the Kinect System. Medicina 2019, 55, 98. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Hernández, M.; Polonio-López, B.; Corregidor-Sánchez, A.-I.; Martín-Conty, J.L.; Mohedano-Moriano, A.; Criado-Álvarez, J.-J. Effects of Specific Virtual Reality-Based Therapy for the Rehabilitation of the Upper Limb Motor Function Post-Ictus: Randomized Controlled Trial. Brain Sci. 2021, 11, 555. [Google Scholar] [CrossRef]
- Zhang, Z.; Prilutsky, B.I.; Butler, A.J.; Shinohara, M.; Ghovanloo, M. Design and Preliminary Evaluation of a Tongue-Operated Exoskeleton System for Upper Limb Rehabilitation. Int. J. Environ. Res. Public Health 2021, 18, 8708. [Google Scholar] [CrossRef]
- Kim, K.-H.; Jang, S.-H. Effects of Task-Specific Training after Cognitive Sensorimotor Exercise on Proprioception, Spasticity, and Gait Speed in Stroke Patients: A Randomized Controlled Study. Medicina 2021, 57, 1098. [Google Scholar] [CrossRef]
- Qian, C.; Li, W.; Jia, T.; Li, C.; Lin, P.-J.; Yang, Y.; Ji, L. Quantitative Assessment of Motor Function by an End-Effector Upper Limb Rehabilitation Robot Based on Admittance Control. Appl. Sci. 2021, 11, 6854. [Google Scholar] [CrossRef]
- Nemes, D.; Catan, L.; Poenaru, D.; Dragoi, M.; Amaricai, E.; Popa, D.; Onofrei, R.; Surducan, D.; Puenea, G.; Prejbeanu, R.; et al. Life quality in patients with Type III ankylosingapondylitis and secondary seronegativespondylarthropathies. In Proceedings of the 6th World Congress of the International-Society-of-Physical-and-Rehabilitation-Medicine (ISPRM), San Juan, Puerto Rico, 12–16 June 2011; pp. 9–11. [Google Scholar]
- Kwakkel, G.; Lannin, N.A.; Borschmann, K.; English, C.; Ali, M.; Churilov, L.; Saposnik, G.; Winstein, C.; van Wegen, E.E.; Wolf, S.L.; et al. Standardized measurement of sensorimotor recovery in stroke trials: Consensus-based core recommendations from the Stroke Recovery and Rehabilitation Roundtable. Int. J. Stroke 2017, 12, 451–461. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Grade | Description | Criteria |
|---|---|---|
| 0 | No contraction | No contraction can be felt in the muscle |
| 1 | Trace muscle contraction | Muscle contraction can be felt on palpation but without motion |
| 2 | Poor muscle contraction | Muscle contraction and motion of the segment in a gravity discarded position (gravity minimized) |
| 3 | Muscle contraction | Full motion of the segment against gravity |
| 4 | Good muscle contraction | Full motion of the segment against gravity and moderate resistance |
| 5 | Normal muscle contraction | Full motion of the segment against gravity and maximal resistance |
| Characteristic | UE (n = 41) |
|---|---|
| Age (mean/SD) | 63.05/6.82 |
| Gender (n/%) | |
| Male | 20/48.78% |
| Female | 21/51.22% |
| Time since stroke (years) (mean/SD) | 1.91/1.00 |
| Affected side (n) | |
| Left | 16/37.50% |
| Right | 25/62.50% |
| Type of Assessment | Aim | Instrument Characteristic |
|---|---|---|
| Functional Independence Measure (FIM) | Identifying and assessing patients’ independence in performing activities of daily living (ADLs). | A reliable and valid instrument with a good construct validity in post-stroke patients [26] |
| Modified Rankin Scale (MRS) | Assessing stroke severity and patients’ degree of disability. | Concurrent validity. A robust predictor of prognosis and validity, with modest inter-rater reliability on ICC [27,28] |
| Modified Ashworth Scale (MAS) | Measuring spasticity. | Satisfactory inter-and intra-rater agreement. Moderate reliability, with better reliability in UE than in LE assessment [29,30] |
| Active Range of Motion (AROM) | Assessing the range of motion of human body joints. | Excellent test-retest reliability score. Can predict UE function at three months post-stroke [31,32] |
| Manual Muscle Testing (MMT) | Assessing muscle strength. | Validity needs to be re-evaluated [24] |
| Fugl–Meyer Upper Extremity Assessment (FMUE) | Assessing the UE motor functioning, sensation, and coordination. | Good reliability, construct validity, inter-rater and intra-rater reliability [33,34,35] |
| AROM Split Value | MMT Value | MMT Technique |
|---|---|---|
| 100% (4/4) * AROM max | 4 | Moderate resistance |
| 75% (3/4) * AROM max | 3.75 | * Slight resistance against Gravity |
| 50% (2/4) * AROM max | 3.50 | Slight resistance against Gravity |
| 25% (1/4) * AROM max | 3.25 | Slight resistance against Gravity |
| 100% (4/4) * AROM max | 3 | Against gravity |
| 75% (3/4) * AROM max | 2.75 | Against gravity |
| 50% (2/4) * AROM max | 2.50 | Against gravity |
| 25% (1/4) * AROM max | 2.25 | Against gravity |
| 100% (4/4) * AROM max | 2 | Minimized gravity |
| 75% (3/4) * AROM max | 1.75 | Minimized gravity |
| 50% (2/4) * AROM max | 1.5 | Minimized gravity |
| 25% (1/4) * AROM max | 1.25 | Minimized gravity |
| 0–25% * AROM max | 1 | Minimized gravity |
| 0% * AROM max | 0 | Minimized |
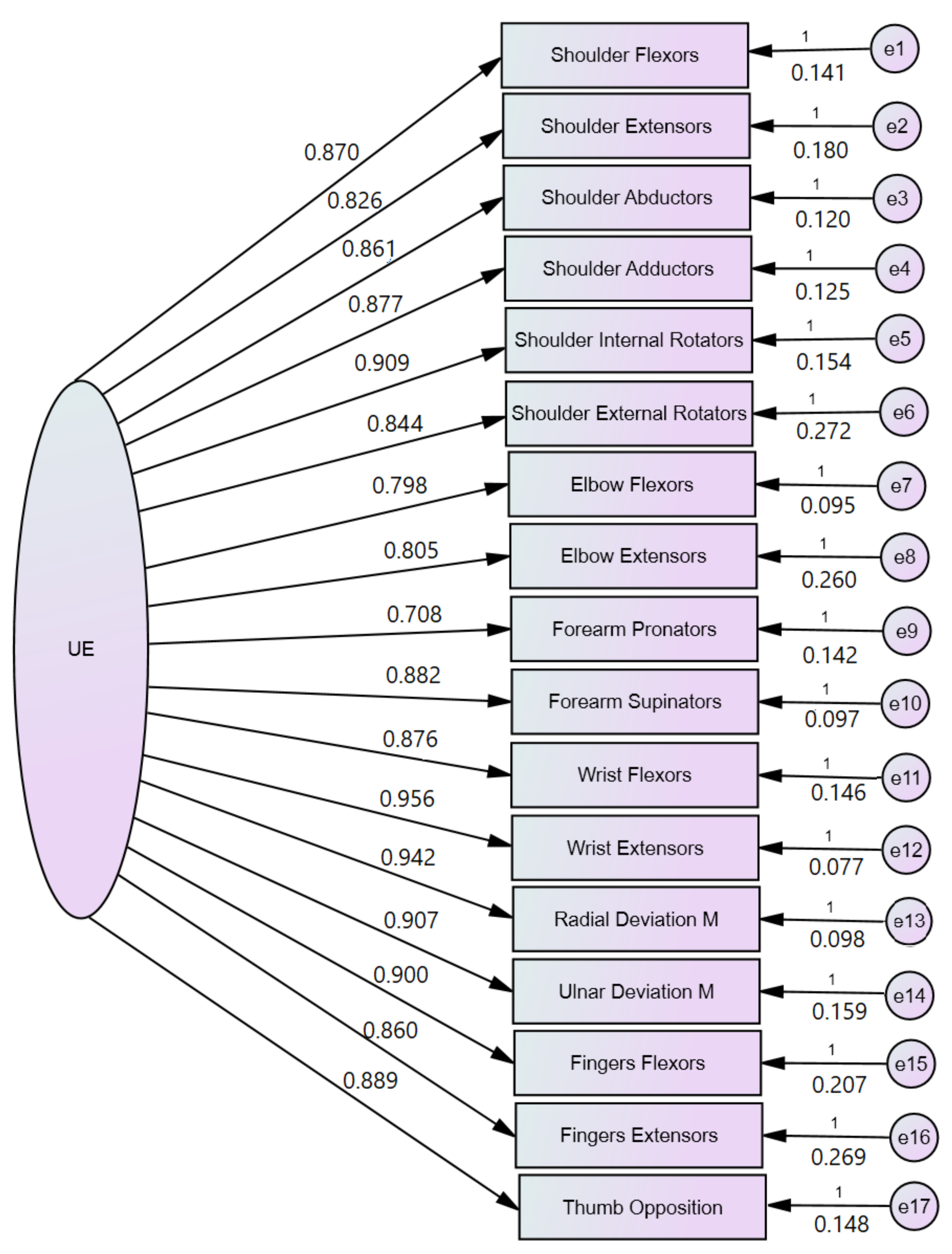
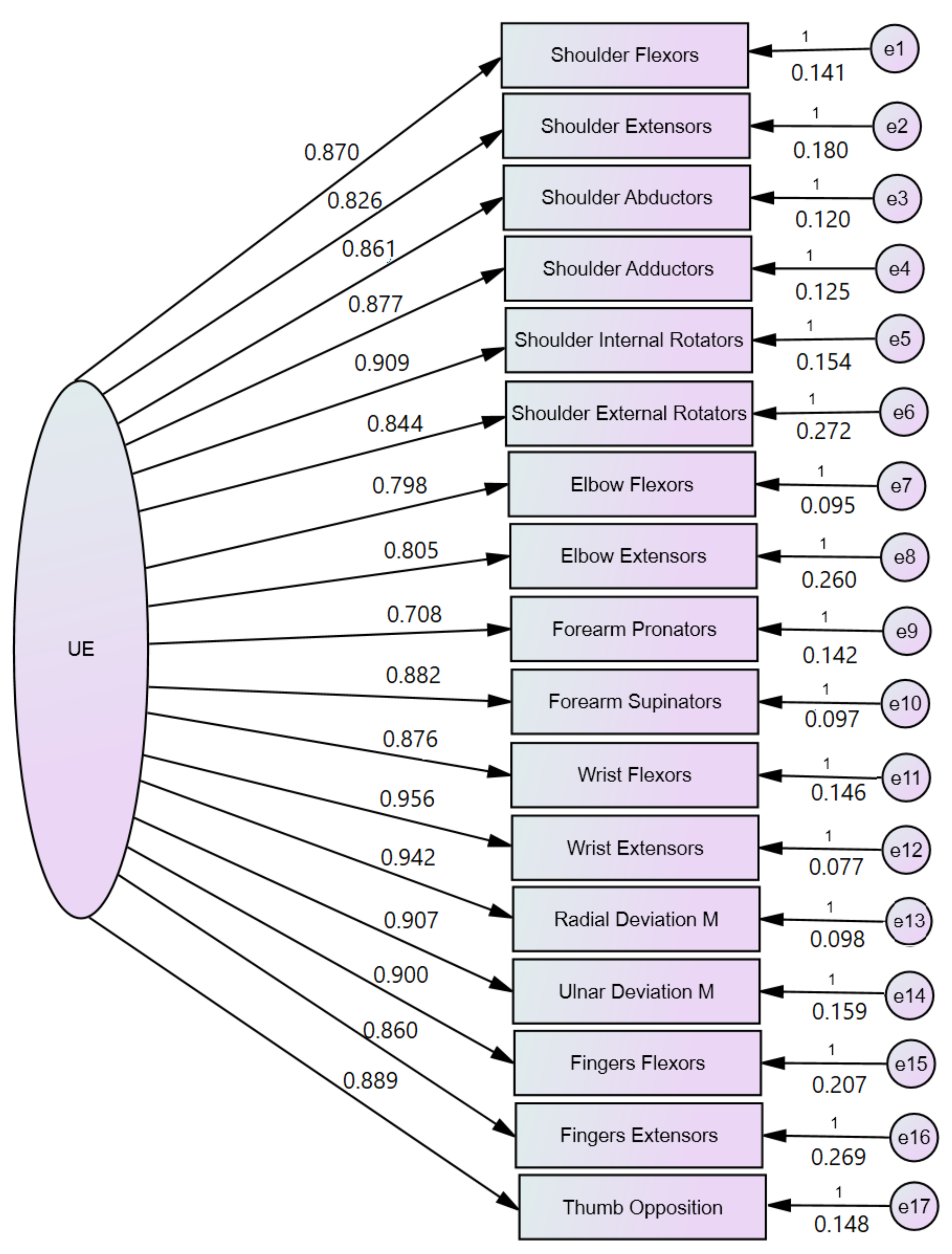
| Muscle Group | Mean ± SD (n = 41) | Communalities Extraction (EFA) | Factor Matrix Loading (EFA) | Standardized Regression Weights SEM (CFA) |
|---|---|---|---|---|
| Shoulder Flexors | 3.00 ± 0.77 | 0.791 | 0.889 | 0.870 |
| Shoulder Extensors | 3.03 ± 0.76 | 0.706 | 0.840 | 0.826 |
| Shoulder Abductors | 2.92 ± 0.69 | 0.779 | 0.883 | 0.861 |
| Shoulder Adductors | 3.08 ± 0.75 | 0.787 | 0.887 | 0.877 |
| Shoulder Int. Rotators | 2.72 ± 0.95 | 0.807 | 0.898 | 0.909 |
| Shoulder Ext. Rotators | 2.54 ± 0.98 | 0.737 | 0.858 | 0.844 |
| Elbow Flexors | 3.29 ± 0.52 | 0.667 | 0.816 | 0.798 |
| Elbow Extensors | 3.17 ± 0.87 | 0.648 | 0.805 | 0.805 |
| Forearm Pronators | 3.12 ± 0.54 | 0.521 | 0.722 | 0.708 |
| Forearm Supinators | 2.79 ± 0.67 | 0.791 | 0.889 | 0.882 |
| Wrist Flexors | 2.80 ± 0.80 | 0.762 | 0.873 | 0.876 |
| Wrist Extensors | 2.58 ± 0.95 | 0.898 | 0.948 | 0.956 |
| Radial Deviation M | 2.39 ± 0.94 | 0.874 | 0.935 | 0.942 |
| Ulnar Deviation m | 2.56 ± 0.96 | 0.803 | 0.896 | 0.907 |
| Fingers II-V Flexors | 2.98 ± 1.06 | 0.785 | 0.875 | 0.900 |
| Fingers II-V Extensors | 2.71 ± 1.03 | 0.710 | 0.842 | 0.860 |
| Thumb opposition M | 2.76 ± 0.85 | 0.763 | 0.874 | 0.889 |
| Model | Unstandardized Coefficients (B) | Standardized Coefficient β | p | R2 |
|---|---|---|---|---|
| 1. (Constant) | 1.342 | 0.000 | 0.822 | |
| Wrist extensors | 0.734 | 0.909 | 0.000 | |
| 2. (Constant) | 0.647 | 0.001 | 0.898 | |
| Wrist Extensors + | 0.467 | 0.578 | 0.000 | |
| Shoulder abductors | 0.474 | 0.425 | 0.000 | |
| 3. (Constant) | 0.578 | 0.001 | 0.911 | |
| Wrist Extensors + | 0.285 | 0.353 | 0.002 | |
| Shoulder abductors+ | 0.449 | 0.402 | 0.000 | |
| Fingers Flexors | 0.205 | 0.282 | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roman, N.A.; Miclaus, R.S.; Nicolau, C.; Sechel, G. Customized Manual Muscle Testing for Post-Stroke Upper Extremity Assessment. Brain Sci. 2022, 12, 457. https://doi.org/10.3390/brainsci12040457
Roman NA, Miclaus RS, Nicolau C, Sechel G. Customized Manual Muscle Testing for Post-Stroke Upper Extremity Assessment. Brain Sciences. 2022; 12(4):457. https://doi.org/10.3390/brainsci12040457
Chicago/Turabian StyleRoman, Nadinne Alexandra, Roxana Steliana Miclaus, Cristina Nicolau, and Gabriela Sechel. 2022. "Customized Manual Muscle Testing for Post-Stroke Upper Extremity Assessment" Brain Sciences 12, no. 4: 457. https://doi.org/10.3390/brainsci12040457
APA StyleRoman, N. A., Miclaus, R. S., Nicolau, C., & Sechel, G. (2022). Customized Manual Muscle Testing for Post-Stroke Upper Extremity Assessment. Brain Sciences, 12(4), 457. https://doi.org/10.3390/brainsci12040457