
Psychopathology and Integrity of the Superior Longitudinal Fasciculus in Deficit and Nondeficit Schizophrenia

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Clinical Assessments
2.3. Acquisition and Measures
2.4. Image Processing and Quality
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Participants
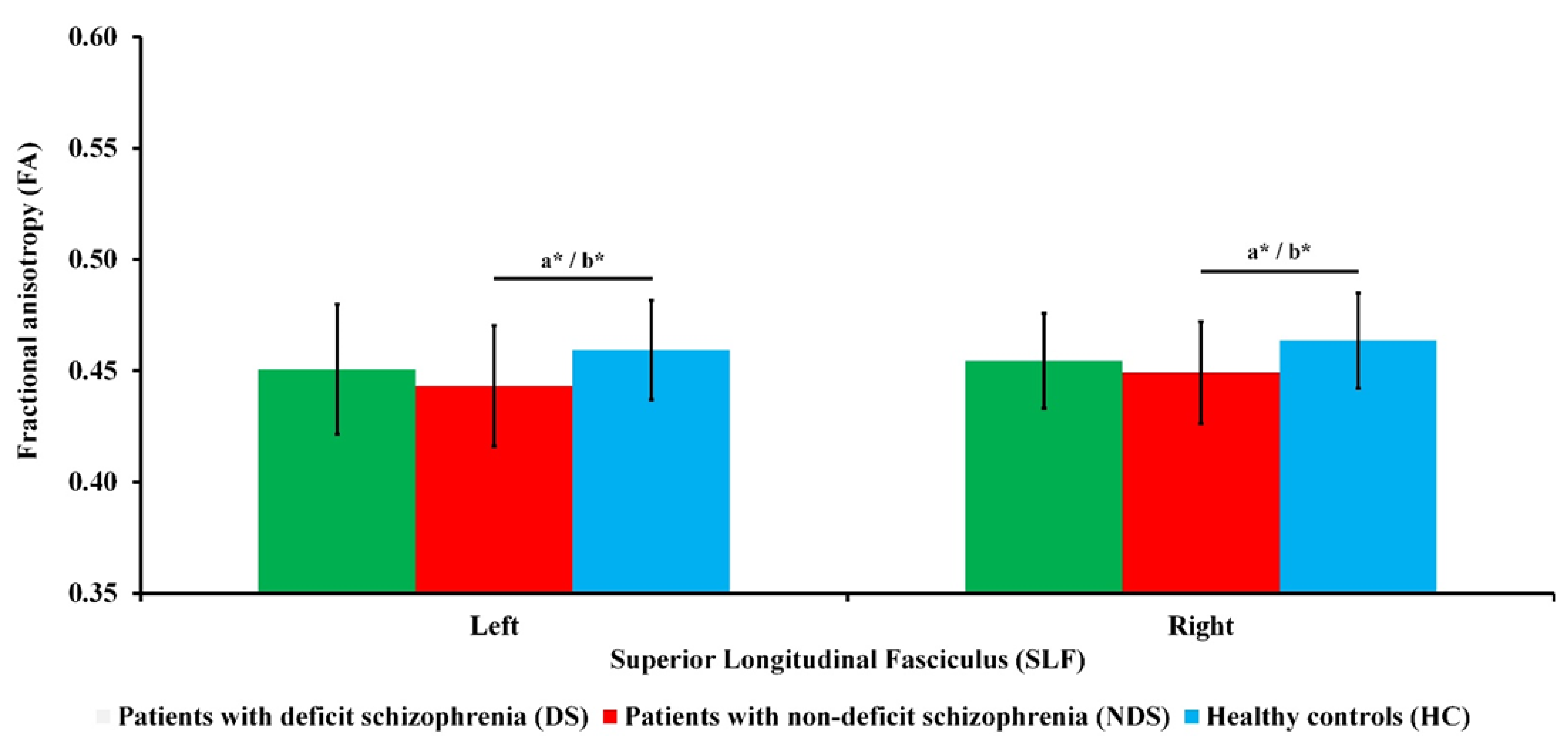
3.2. Differences in FA Measures
3.3. Relationship between FA Measures and Psychopathological Dimensions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thiebaut de Schotten, M.; Foulon, C.; Nachev, P. Brain Disconnections Link Structural Connectivity with Function and Behaviour. Nat. Commun. 2020, 11, 5094. [Google Scholar] [CrossRef]
- Wang, X.; Pathak, S.; Stefaneanu, L.; Yeh, F.C.; Li, S.; Fernandez-Miranda, J.C. Subcomponents and Connectivity of the Superior Longitudinal Fasciculus in the Human Brain. Brain Struct. Funct. 2016, 221, 2075–2092. [Google Scholar] [CrossRef]
- Nakajima, R.; Kinoshita, M.; Shinohara, H.; Nakada, M. The Superior Longitudinal Fascicle: Reconsidering the Fronto-Parietal Neural Network Based on Anatomy and Function. Brain Imaging Behav. 2019, 12, 309–323. [Google Scholar] [CrossRef] [PubMed]
- Verhelst, H.; Dhollander, T.; Gerrits, R.; Vingerhoets, G. Fibre-Specific Laterality of White Matter in Left and Right Language Dominant People. Neuroimage 2021, 230, 117812. [Google Scholar] [CrossRef]
- Friston, K.; Brown, H.R.; Siemerkus, J.; Stephan, K.E. The Dysconnection Hypothesis (2016). Schizophr. Res. 2016, 176, 83–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawidowski, B.; Górniak, A.; Podwalski, P.; Lebiecka, Z.; Misiak, B.; Samochowiec, J. The Role of Cytokines in the Pathogenesis of Schizophrenia. J. Clin. Med. 2021, 10, 3849. [Google Scholar] [CrossRef] [PubMed]
- Cao, B.; Chen, Y.; Ren, Z.; Pan, Z.; McIntyre, R.S.; Wang, D. Dysregulation of Kynurenine Pathway and Potential Dynamic Changes of Kynurenine in Schizophrenia: A Systematic Review and Meta-Analysis. Neurosci. Biobehav. Rev. 2021, 123, 203–214. [Google Scholar] [CrossRef]
- Liu, J.; Li, S.; Li, X.; Li, W.; Yang, Y.; Guo, S.; Lv, L.; Xiao, X.; Yao, Y.G.; Guan, F.; et al. Genome-Wide Association Study Followed by Trans-Ancestry Meta-Analysis Identify 17 New Risk Loci for Schizophrenia. BMC Med. 2021, 19, 1–15. [Google Scholar] [CrossRef]
- Dong, D.; Wang, Y.; Chang, X.; Luo, C.; Yao, D. Dysfunction of Large-Scale Brain Networks in Schizophrenia: A Meta-Analysis of Resting-State Functional Connectivity. Schizophr. Bull. 2018, 44, 168–181. [Google Scholar] [CrossRef]
- Zhou, Y.; Fan, L.; Qiu, C.; Jiang, T. Prefrontal Cortex and the Dysconnectivity Hypothesis of Schizophrenia. Neurosci. Bull. 2015, 31, 207–219. [Google Scholar] [CrossRef] [Green Version]
- Curran, K.M.; Emsell, L.; Leemans, A. Quantitative DTI Measures. In Diffusion Tensor Imaging; Springer: New York, NY, USA, 2016; pp. 65–87. ISBN 9781493931187. [Google Scholar]
- Soares, J.M.; Marques, P.; Alves, V.; Sousa, N. A Hitchhiker’s Guide to Diffusion Tensor Imaging. Front. Neurosci. 2013, 7, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Dennis, E.L.; Disner, S.G.; Fani, N.; Salminen, L.E.; Logue, M.; Clarke, E.K.; Haswell, C.C.; Averill, C.L.; Baugh, L.A.; Bomyea, J.; et al. Altered White Matter Microstructural Organization in Posttraumatic Stress Disorder across 3047 Adults: Results from the PGC-ENIGMA PTSD Consortium. Mol. Psychiatry 2019, 26, 4315–4330. [Google Scholar] [CrossRef]
- Kelly, S.; Jahanshad, N.; Zalesky, A.; Kochunov, P.; Agartz, I.; Alloza, C.; Andreassen, O.A.; Arango, C.; Banaj, N.; Bouix, S.; et al. Widespread White Matter Microstructural Differences in Schizophrenia across 4322 Individuals: Results from the ENIGMA Schizophrenia DTI Working Group. Mol. Psychiatry 2018, 23, 1261–1269. [Google Scholar] [CrossRef] [Green Version]
- Koshiyama, D.; Fukunaga, M.; Okada, N.; Morita, K.; Nemoto, K.; Usui, K.; Yamamori, H.; Yasuda, Y.; Fujimoto, M.; Kudo, N.; et al. White Matter Microstructural Alterations across Four Major Psychiatric Disorders: Mega-Analysis Study in 2937 Individuals. Mol. Psychiatry 2020, 25, 883–895. [Google Scholar] [CrossRef] [Green Version]
- Alba-Ferrara, L.M.; de Erausquin, G.A. What Does Anisotropy Measure? Insights from Increased and Decreased Anisotropy in Selective Fiber Tracts in Schizophrenia. Front. Integr. Neurosci. 2013, 7, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tyburski, E.; Podwalski, P.; Waszczuk, K.; Rek-Owodziń, K.; Mak, M.; Plichta, P.; Bielecki, M.; Rudkowski, K.; Szelepajło, M.; Kucharska-Mazur, J.; et al. Relationship of Corpus Callosum Integrity with Working Memory, Planning, and Speed of Processing in Patients with First-Episode and Chronic Schizophrenia. J. Clin. Med. 2021, 10, 3158. [Google Scholar] [CrossRef] [PubMed]
- Koshiyama, D.; Fukunaga, M.; Okada, N.; Morita, K.; Nemoto, K.; Yamashita, F.; Yamamori, H.; Yasuda, Y.; Fujimoto, M.; Kelly, S.; et al. Role of Frontal White Matter and Corpus Callosum on Social Function in Schizophrenia. Schizophr. Res. 2018, 202, 180–187. [Google Scholar] [CrossRef]
- Podwalski, P.; Tyburski, E.; Szczygieł, K.; Waszczuk, K.; Rek-Owodziń, K.; Mak, M.; Plichta, P.; Bielecki, M.; Rudkowski, K.; Kucharska-Mazur, J.; et al. White Matter Integrity of the Corpus Callosum and Psychopathological Dimensions in Deficit and Non-Deficit Schizophrenia Patients. J. Clin. Med. 2021, 10, 2225. [Google Scholar] [CrossRef]
- Podwalski, P.; Szczygieł, K.; Tyburski, E.; Sagan, L.; Misiak, B.; Samochowiec, J. Magnetic Resonance Diffusion Tensor Imaging in Psychiatry: A Narrative Review of Its Potential Role in Diagnosis. Pharmacol. Rep. 2020, 73, 43–56. [Google Scholar] [CrossRef]
- Dong, D.; Wang, Y.; Chang, X.; Jiang, Y.; Klugah-Brown, B.; Luo, C.; Yao, D. Shared Abnormality of White Matter Integrity in Schizophrenia and Bipolar Disorder: A Comparative Voxel-Based Meta-Analysis. Schizophr. Res. 2017, 185, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Joo, S.W.; Kim, H.; Jo, Y.T.; Ahn, S.; Choi, Y.J.; Park, S.; Kang, Y.; Lee, J. White Matter Impairments in Patients with Schizophrenia: A Multisite Diffusion MRI Study. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 111, 110381. [Google Scholar] [CrossRef] [PubMed]
- Vitolo, E.; Tatu, M.K.; Pignolo, C.; Cauda, F.; Costa, T.; Ando, A.; Zennaro, A. White Matter and Schizophrenia: A Meta-Analysis of Voxel-Based Morphometry and Diffusion Tensor Imaging Studies. Psychiatry Res.-Neuroimaging 2017, 270, 8–21. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Cao, D.; Liang, X.; Zhao, J. Schizophrenia Symptomatic Associations with Diffusion Tensor Imaging Measured Fractional Anisotropy of Brain: A Meta-Analysis. Neuroradiology 2017, 59, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Bloemen, O.J.N.; de Koning, M.B.; Schmitz, N.; Nieman, D.H.; Becker, H.E.; de Haan, L.; Dingemans, P.; Linszen, D.H.; van Amelsvoort, T.A.M.J. White-Matter Markers for Psychosis in a Prospective Ultra-High-Risk Cohort. Psychol. Med. 2010, 40, 1297–1304. [Google Scholar] [CrossRef]
- Carletti, F.; Woolley, J.B.; Bhattacharyya, S.; Perez-Iglesias, R.; Fusar Poli, P.; Valmaggia, L.; Broome, M.R.; Bramon, E.; Johns, L.; Giampietro, V.; et al. Alterations in White Matter Evident before the Onset of Psychosis. Schizophr. Bull. 2012, 38, 1170–1179. [Google Scholar] [CrossRef]
- Karlsgodt, K.H.; Niendam, T.A.; Bearden, C.E.; Cannon, T.D. White Matter Integrity and Prediction of Social and Role Functioning in Subjects at Ultra-High Risk for Psychosis. Biol. Psychiatry 2009, 66, 562–569. [Google Scholar] [CrossRef] [Green Version]
- Krakauer, K.; Nordentoft, M.; Glenthøj, B.Y.; Raghava, J.M.; Nordholm, D.; Randers, L.; Glenthøj, L.B.; Ebdrup, B.H.; Rostrup, E. White Matter Maturation during 12 Months in Individuals at Ultra-High-Risk for Psychosis. Acta Psychiatr. Scand. 2018, 137, 65–78. [Google Scholar] [CrossRef]
- Kristensen, T.D.; Mandl, R.C.W.; Raghava, J.M.; Jessen, K.; Jepsen, J.R.M.; Fagerlund, B.; Glenthøj, L.B.; Wenneberg, C.; Krakauer, K.; Pantelis, C.; et al. Widespread Higher Fractional Anisotropy Associates to Better Cognitive Functions in Individuals at Ultra-High Risk for Psychosis. Hum. Brain Mapp. 2019, 40, 5185–5201. [Google Scholar] [CrossRef]
- Wang, C.; Ji, F.; Hong, Z.; Poh, J.S.; Krishnan, R.; Lee, J.; Rekhi, G.; Keefe, R.S.E.; Adcock, R.A.; Wood, S.J.; et al. Disrupted Salience Network Functional Connectivity and White-Matter Microstructure in Persons at Risk for Psychosis: Findings from the LYRIKS Study. Psychol. Med. 2016, 46, 2771–2783. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, A.; Lenz, C.; Smieskova, R.; Harrisberger, F.; Walter, A.; Riecher-Rössler, A.; Simon, A.; Lang, U.E.; McGuire, P.; Fusar-Poli, P.; et al. Brain Diffusion Changes in Emerging Psychosis and the Impact of State-Dependent Psychopathology. NeuroSignals 2015, 23, 71–83. [Google Scholar] [CrossRef]
- Leroux, E.; Poirel, N.; Dollfus, S. Anatomical Connectivity of the Visuospatial Attentional Network in Schizophrenia: A Diffusion Tensor Imaging Tractography Study. J. Neuropsychiatry Clin. Neurosci. 2020, 32, 266–273. [Google Scholar] [CrossRef]
- Chawla, N.; Deep, R.; Khandelwal, S.K.; Garg, A. Reduced Integrity of Superior Longitudinal Fasciculus and Arcuate Fasciculus as a Marker for Auditory Hallucinations in Schizophrenia: A DTI Tractography Study. Asian J. Psychiatr. 2019, 44, 179–186. [Google Scholar] [CrossRef]
- Viher, P.V.; Stegmayer, K.; Federspiel, A.; Bohlhalter, S.; Wiest, R.; Walther, S. Altered Diffusion in Motor White Matter Tracts in Psychosis Patients with Catatonia. Schizophr. Res. 2020, 220, 210–217. [Google Scholar] [CrossRef]
- McClure, M.M.; Graff, F.S.; Triebwasser, J.; Perez-Rodriguez, M.M.; Rosell, D.R.; Szeszko, P.R.; Chu, K.W.; New, A.S.; Siever, L.J.; Hazlett, E.A. Neuroimaging Predictors of Response to Cognitive Remediation and Social Skills Training: A Pilot Study in Veterans with Schizophrenia. Psychiatry Res.-Neuroimaging 2019, 293, 2018–2020. [Google Scholar] [CrossRef] [PubMed]
- Berrios, G.E. Positive and Negative Symptoms and Jackson. Arch. Gen. Psychiatry 1985, 42, 95. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, T.; Wagman, A.M.I.; Heinrichs, W.; Ph, D. Deficit and Nondeficit Forms of Schizophrenia: The Concept. Am. J. Psychiatry 1988, 145, 578–583. [Google Scholar] [CrossRef]
- Galderisi, S.; Mucci, A.; Dollfus, S.; Nordentoft, M.; Falkai, P.; Kaiser, S.; Giordano, G.M.; Vandevelde, A.; Nielsen, M.Ø.; Glenthøj, L.B.; et al. EPA Guidance on Assessment of Negative Symptoms in Schizophrenia. Eur. Psychiatry 2021, 64, e23. [Google Scholar] [CrossRef]
- Kirkpatrick, B.; Mucci, A.; Galderisi, S. Primary, Enduring Negative Symptoms: An Update on Research. Schizophr. Bull. 2017, 43, 730–736. [Google Scholar] [CrossRef]
- Fervaha, G.; Agid, O.; Foussias, G.; Siddiqui, I.; Takeuchi, H.; Remington, G. Neurocognitive Impairment in the Deficit Subtype of Schizophrenia. Eur. Arch. Psychiatry Clin. Neurosci. 2016, 266, 397–407. [Google Scholar] [CrossRef]
- Kirkpatrick, B.; Buchanan, R.W.; Ross, D.E.; Carpenter, J. A Separate Disease within the Syndrome of Schizophrenia. Arch. Gen. Psychiatry 2001, 58, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Mucci, A.; Merlotti, E.; Üçok, A.; Aleman, A.; Galderisi, S. Primary and Persistent Negative Symptoms: Concepts, Assessments and Neurobiological Bases. Schizophr. Res. 2017, 186, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Tan, A.S.; Chew, Q.H.; Sim, K. Cerebral White Matter Changes in Deficit and Non-Deficit Subtypes of Schizophrenia. J. Neural Transm. 2020, 127, 1073–1079. [Google Scholar] [CrossRef]
- Chee, T.T.; Chua, L.; Morrin, H.; Lim, M.F.; Fam, J.; Ho, R. Neuroanatomy of Patients with Deficit Schizophrenia: An Exploratory Quantitative Meta-Analysis of Structural Neuroimaging Studies. Int. J. Environ. Res. Public Health 2020, 17, 6227. [Google Scholar] [CrossRef] [PubMed]
- Giordano, G.M.; Pezzella, P.; Quarantelli, M.; Bucci, P.; Prinster, A.; Soricelli, A.; Perrottelli, A.; Giuliani, L.; Fabrazzo, M.; Galderisi, S. Investigating the Relationship between White Matter Connectivity and Motivational Circuits in Subjects with Deficit Schizophrenia: A Diffusion Tensor Imaging (Dti) Study. J. Clin. Med. 2022, 11, 61. [Google Scholar] [CrossRef] [PubMed]
- Spalletta, G.; De Rossi, P.; Piras, F.; Iorio, M.; Dacquino, C.; Scanu, F.; Girardi, P.; Caltagirone, C.; Kirkpatrick, B.; Chiapponi, C. Brain White Matter Microstructure in Deficit and Non-Deficit Subtypes of Schizophrenia. Psychiatry Res.-Neuroimaging 2015, 231, 252–261. [Google Scholar] [CrossRef]
- Kitis, O.; Ozalay, O.; Zengin, E.B.; Haznedaroglu, D.; Eker, M.C.; Yalvac, D.; Oguz, K.; Coburn, K.; Gonul, A.S. Reduced Left Uncinate Fasciculus Fractional Anisotropy in Deficit Schizophrenia but Not in Non-Deficit Schizophrenia. Psychiatry Clin. Neurosci. 2012, 66, 34–43. [Google Scholar] [CrossRef]
- Lei, W.; Li, N.; Deng, W.; Li, M.; Huang, C.; Ma, X.; Wang, Q.; Guo, W.; Li, Y.; Jiang, L.; et al. White Matter Alterations in First Episode Treatment-Naïve Patients with Deficit Schizophrenia: A Combined VBM and DTI Study. Sci. Rep. 2015, 5, 1–11. [Google Scholar] [CrossRef]
- Voineskos, A.N.; Foussias, G.; Lerch, J.; Felsky, D.; Remington, G.; Rajji, T.K.; Lobaugh, N.; Pollock, B.G.; Mulsant, B.H. Neuroimaging Evidence for the Deficit Subtype of Schizophrenia. JAMA Psychiatry 2013, 70, 472–480. [Google Scholar] [CrossRef] [Green Version]
- Sagarwala, R.; Nasrallah, H.A. White Matter Pathology Is Shared across Multiple Psychiatric Brain Disorders: Is Abnormal Diffusivity a Transdiagnostic Biomarker for Psychopathology? Biomark. Neuropsychiatry 2020, 2, 100010. [Google Scholar] [CrossRef]
- Galderisi, S.; DeLisi, L.E.; Borgwardt, S. Neuroimaging of Schizophrenia and Other Primary Psychotic Disorders: Achievements and Perspectives; Springer: Berlin/Heidelberg, Germany, 2019; ISBN 9783319973074. [Google Scholar]
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines; World Health Organization: Geneva, Switzerland, 1992; ISBN 9241544228. [Google Scholar]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The Development and Validation of a Structured Diagnostic Psychiatric Interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59, 22–33. [Google Scholar]
- Szulc, A.; Dudek, D.; Samochowiec, J.; Wojnar, M.; Heitzman, J.; Gałecki, P. Rekomendacje Dotyczące Leczenia Schizofrenii z Objawami Negatywnymi. Standardy Farmakoterapii Polskiego Towarzstwa Psychiatrycznego Część 2. Psychiatra Pol. 2019, 2674, 1–16. [Google Scholar]
- Szulc, A.; Dudek, D.; Samochowiec, J.; Wojnar, M.; Heitzman, J.; Gałecki, P. Recommendations for the Treatment of Schizophrenia with Negative Symptoms. Standards of Pharmacotherapy by the Polish Psychiatric Association (Polskie Towarzystwo Psychiatryczne), Part 2. Psychiatr. Pol. 2019, 53, 525–540. [Google Scholar] [CrossRef] [PubMed]
- Hasan, A.; Falkai, P.; Wobrock, T.; Lieberman, J.; Glenthoj, B.; Gattaz, W.F.; Thibaut, F.; Möller, H.J.; Altamura, A.C.; Andreasen, N.; et al. World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for Biological Treatment of Schizophrenia, Part 2: Update 2012 on the Long-Term Treatment of Schizophrenia and Management of Antipsychotic-Induced Side Effects. World J. Biol. Psychiatry 2013, 14, 2–44. [Google Scholar] [CrossRef]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The Positive and Negative Syndrome Scale (PANSS) for Schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef]
- Shafer, A.; Dazzi, F. Meta-Analysis of the Positive and Negative Syndrome Scale (PANSS) Factor Structure. J. Psychiatr. Res. 2019, 115, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Goetz, R.R.; Corcoran, C.; Yale, S.; Stanford, A.D.; Kimhy, D.; Amador, X.; Malaspina, D. Validity of a ‘Proxy’ for the Deficit Syndrome Derived from the Positive And Negative Syndrome Scale (PANSS). Schizophr. Res. 2007, 93, 169–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tatsumi, K.; Kirkpatrick, B.; Strauss, G.P.; Opler, M. The Brief Negative Symptom Scale in Translation: A Review of Psychometric Properties and Beyond. Eur. Neuropsychopharmacol. 2020, 33, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Dollfus, S.; Mach, C.; Morello, R. Self-Evaluation of Negative Symptoms. Schizophr. Bull. 2016, 42, 571–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, R.C.W. Global Assessment of Functioning: A Modified Scale. Psychosomatics 1995, 36, 267–275. [Google Scholar] [CrossRef]
- Leemans, A.; Jeurissen, B.; Sijbers, J.; Jones, D.K. ExploreDTI: A Graphical Toolbox for Processing, Analyzing, and Visualizing Diffusion MR Data. Proc. Int. Soc. Magn. Reson. Med. 2009, 17, 3537. [Google Scholar]
- Hair, J.F., Jr.; Black, W.C.; Babin, B.J.; Anderson, R. Multivariate Data Analysis: A Global Perspective, 7th ed.; Pearson Educational International: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Wendt, H.W. Dealing with a Common Problem in Social Science: A Simplified Rank-Biserial Coefficient of Correlation Based on the U Statistic. Eur. J. Soc. Psychol. 1972, 2, 463–465. [Google Scholar] [CrossRef]
- Cohen, J. A Power Primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Camchong, J.; MacDonald, A.W.; Bell, C.; Mueller, B.A.; Lim, K.O. Altered Functional and Anatomical Connectivity in Schizophrenia. Schizophr. Bull. 2011, 37, 640–650. [Google Scholar] [CrossRef] [PubMed]
- Saarinen, A.I.L.; Huhtaniska, S.; Pudas, J.; Björnholm, L.; Jukuri, T.; Tohka, J.; Granö, N.; Barnett, J.H.; Kiviniemi, V.; Veijola, J.; et al. Structural and Functional Alterations in the Brain Gray Matter among First-Degree Relatives of Schizophrenia Patients: A Multimodal Meta-Analysis of FMRI and VBM Studies. Schizophr. Res. 2020, 216, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Uranova, N.A.; Vikhreva, O.V.; Rakhmanova, V.I.; Orlovskaya, D.D. Dystrophy of Oligodendrocytes and Adjacent Microglia in Prefrontal Gray Matter in Schizophrenia. Front. Psychiatry 2020, 11, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatton, S.N.; Lagopoulos, J.; Hermens, D.F.; Hickie, I.B.; Scott, E.; Bennett, M.R. White Matter Tractography in Early Psychosis: Clinical and Neurocognitive Associations. J. Psychiatry Neurosci. 2014, 39, 417–427. [Google Scholar] [CrossRef] [Green Version]
- Rotarska-Jagiela, A.; Oertel-Knoechel, V.; DeMartino, F.; van de Ven, V.; Formisano, E.; Roebroeck, A.; Rami, A.; Schoenmeyer, R.; Haenschel, C.; Hendler, T.; et al. Anatomical Brain Connectivity and Positive Symptoms of Schizophrenia: A Diffusion Tensor Imaging Study. Psychiatry Res.-Neuroimaging 2009, 174, 9–16. [Google Scholar] [CrossRef]
- Seok, J.H.; Park, H.J.; Chun, J.W.; Lee, S.K.; Cho, H.S.; Kwon, J.S.; Kim, J.J. White Matter Abnormalities Associated with Auditory Hallucinations in Schizophrenia: A Combined Study of Voxel-Based Analyses of Diffusion Tensor Imaging and Structural Magnetic Resonance Imaging. Psychiatry Res.-Neuroimaging 2007, 156, 93–104. [Google Scholar] [CrossRef]
- Szeszko, P.R.; Robinson, D.G.; Ashtari, M.; Vogel, J.; Betensky, J.; Sevy, S.; Ardekani, B.A.; Lencz, T.; Malhotra, A.K.; McCormack, J.; et al. Clinical and Neuropsychological Correlates of White Matter Abnormalities in Recent Onset Schizophrenia. Neuropsychopharmacology 2008, 33, 976–984. [Google Scholar] [CrossRef] [Green Version]
- Szeszko, P.R.; Tan, E.T.; Uluğ, A.M.; Kingsley, P.B.; Gallego, J.A.; Rhindress, K.; Malhotra, A.K.; Robinson, D.G.; Marinelli, L. Investigation of Superior Longitudinal Fasciculus Fiber Complexity in Recent Onset Psychosis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 81, 114–121. [Google Scholar] [CrossRef]
- Kristensen, T.D.; Glenthøj, L.B.; Ragahava, J.M.; Syeda, W.; Mandl, R.C.W.; Wenneberg, C.; Krakauer, K.; Fagerlund, B.; Pantelis, C.; Glenthøj, B.Y.; et al. Changes in Negative Symptoms Are Linked to White Matter Changes in Superior Longitudinal Fasciculus in Individuals at Ultra-High Risk for Psychosis. Schizophr. Res. 2021, 237, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Rowland, L.M.; Spieker, E.A.; Francis, A.; Barker, P.B.; Carpenter, W.T.; Buchanan, R.W. White Matter Alterations in Deficit Schizophrenia. Neuropsychopharmacology 2009, 34, 1514–1522. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, B.; Galderisi, S. Deficit Schizophrenia: An Update. World Psychiatry 2008, 7, 143–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlsgodt, K.H.; van Erp, T.G.M.; Poldrack, R.A.; Bearden, C.E.; Nuechterlein, K.H.; Cannon, T.D. Diffusion Tensor Imaging of the Superior Longitudinal Fasciculus and Working Memory in Recent-Onset Schizophrenia. Biol. Psychiatry 2008, 63, 512–518. [Google Scholar] [CrossRef]
- DeRosse, P.; Ikuta, T.; Peters, B.D.; Karlsgodt, K.H.; Szeszko, P.R.; Malhotra, A.K. Adding Insult to Injury: Childhood and Adolescent Risk Factors for Psychosis Predict Lower Fractional Anisotropy in the Superior Longitudinal Fasciculus in Healthy Adults. Psychiatry Res.-Neuroimaging 2014, 224, 296–302. [Google Scholar] [CrossRef] [Green Version]
- Ohtani, T.; Bouix, S.; Hosokawa, T.; Saito, Y.; Eckbo, R.; Ballinger, T.; Rausch, A.; Melonakos, E.; Kubicki, M. Abnormalities in White Matter Connections between Orbitofrontal Cortex and Anterior Cingulate Cortex and Their Associations with Negative Symptoms in Schizophrenia: A DTI Study. Schizophr. Res. 2014, 157, 190–197. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.H.; Kubicki, M.; Asami, T.; Seidman, L.J.; Goldstein, J.M.; Mesholam-Gately, R.I.; McCarley, R.W.; Shenton, M.E. Extensive White Matter Abnormalities in Patients with First-Episode Schizophrenia: A Diffusion Tensor Imaging (DTI) Study. Schizophr. Res. 2013, 143, 231–238. [Google Scholar] [CrossRef] [Green Version]
- Pillmann, F.; Arndt, T.; Ehrt, U.; Haring, A.; Kumbier, E.; Marneros, A. An Analysis of Wernicke’s Original Case Records: His Contribution to the Concept of Cycloid Psychoses. Hist. Psychiatry 2000, 11, 355–369. [Google Scholar] [CrossRef]

{kind=link}
| Patients with Deficit Schizophrenia (DS) (n = 26) | Patients with Nondeficit Schizophrenia (NDS) (n = 42) | Healthy Controls (HC) (n = 36) | F/H/χ2/t/Z | p | ɳ2/E/V/d/rU | |
|---|---|---|---|---|---|---|
| Age: M (SD) | 38.38 (6.47) | 38.61 (7.12) | 37.39 (7.82) | 0.30 a | 0.740 | 0.01 f |
| Years of education: M (SD) | 12.28 (2.90) | 13.33 (2.58) | 14.53 (2.63) | 9.31 b | 0.010 | 0.09 g |
| Sex: female/male | 7/19 | 23/19 | 21/15 | 6.88 c | 0.032 | 0.22 h |
| Antipsychotic medications: | ||||||
| Atypical: n (%) | 18 (69.23) | 26 (61.90) | - | 2.12 c | 0.547 | 0.12 h |
| Atypical and typical: n (%) | 7 (26.93) | 12 (28.60) | - | |||
| Typical: n (%) | 0 (0.00) | 3 (7.10) | - | |||
| No medications: n (%) | 1 (3.84) | 1 (2.40) | - | |||
| Chlorpromazine equivalent (mg): M (SD) | 698.73 (321.77) | 627.50 (303.75) | - | 0.92 d | 0.724 | 0.23 i |
| Duration of illness: M (SD) | 16.92 (6.01) | 13.60 (4.90) | - | −2.31 e | 0.084 | 0.33 j |
| Exacerbation: M (SD) | 5.62 (2.53) | 6.71 (5.11) | - | −0.19 e | 0.854 | 0.03 j |
| Global functioning in GAF: M (SD) | 50.40 (15.14) | 58.53 (14.53) | - | −2.18 d | 0.099 | 0.54 i |
| PANSS (by [48]): | ||||||
| Positive Symptoms: M (SD) | 7.46 (2.8) | 8.14 (4.5) | - | −0.12 e | 1.000 | 0.02 j |
| Negative Symptoms: M (SD) | 22.81 (4.5) | 13.29 (4.3) | - | −5.98 e | 0.000 | 0.87 j |
| Disorganization: M (SD) | 12.81 (3.5) | 11.21 (3.8) | - | −2.24 e | 0.100 | 0.32 j |
| Affect: M (SD) | 8.58 (3.5) | 9.26 (3.6) | - | −0.93 e | 1.000 | 0.13 j |
| Resistance: M (SD) | 4.38 (0.6) | 4.90 (2.5) | - | −0.17 e | 1.000 | 0.02 j |
| PANSS (by [57]): | ||||||
| Negative Symptoms: M (SD) | 20.77 (4.1) | 12.93 (3.6) | - | −5.76 e | 0.000 | 0.83 j |
| BNSS total score: M (SD) | 47.42 (9.6) | 19.48 (11.8) | - | −6.05 e | 0.000 | 0.88 j |
| SNS total score: M (SD) | 22.54 (7.8) | 9.52 (6.9) | - | −5.35 e | 0.000 | 0.77 j |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Podwalski, P.; Tyburski, E.; Szczygieł, K.; Rudkowski, K.; Waszczuk, K.; Andrusewicz, W.; Kucharska-Mazur, J.; Michalczyk, A.; Mak, M.; Cyranka, K.; et al. Psychopathology and Integrity of the Superior Longitudinal Fasciculus in Deficit and Nondeficit Schizophrenia. Brain Sci. 2022, 12, 267. https://doi.org/10.3390/brainsci12020267
Podwalski P, Tyburski E, Szczygieł K, Rudkowski K, Waszczuk K, Andrusewicz W, Kucharska-Mazur J, Michalczyk A, Mak M, Cyranka K, et al. Psychopathology and Integrity of the Superior Longitudinal Fasciculus in Deficit and Nondeficit Schizophrenia. Brain Sciences. 2022; 12(2):267. https://doi.org/10.3390/brainsci12020267
Chicago/Turabian StylePodwalski, Piotr, Ernest Tyburski, Krzysztof Szczygieł, Krzysztof Rudkowski, Katarzyna Waszczuk, Wojciech Andrusewicz, Jolanta Kucharska-Mazur, Anna Michalczyk, Monika Mak, Katarzyna Cyranka, and et al. 2022. "Psychopathology and Integrity of the Superior Longitudinal Fasciculus in Deficit and Nondeficit Schizophrenia" Brain Sciences 12, no. 2: 267. https://doi.org/10.3390/brainsci12020267
APA StylePodwalski, P., Tyburski, E., Szczygieł, K., Rudkowski, K., Waszczuk, K., Andrusewicz, W., Kucharska-Mazur, J., Michalczyk, A., Mak, M., Cyranka, K., Misiak, B., Sagan, L., & Samochowiec, J. (2022). Psychopathology and Integrity of the Superior Longitudinal Fasciculus in Deficit and Nondeficit Schizophrenia. Brain Sciences, 12(2), 267. https://doi.org/10.3390/brainsci12020267