
Clinical Implications of Prominent Cortical Vessels on Susceptibility-Weighted Imaging in Acute Ischemic Stroke Patients Treated with Recanalization Therapy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
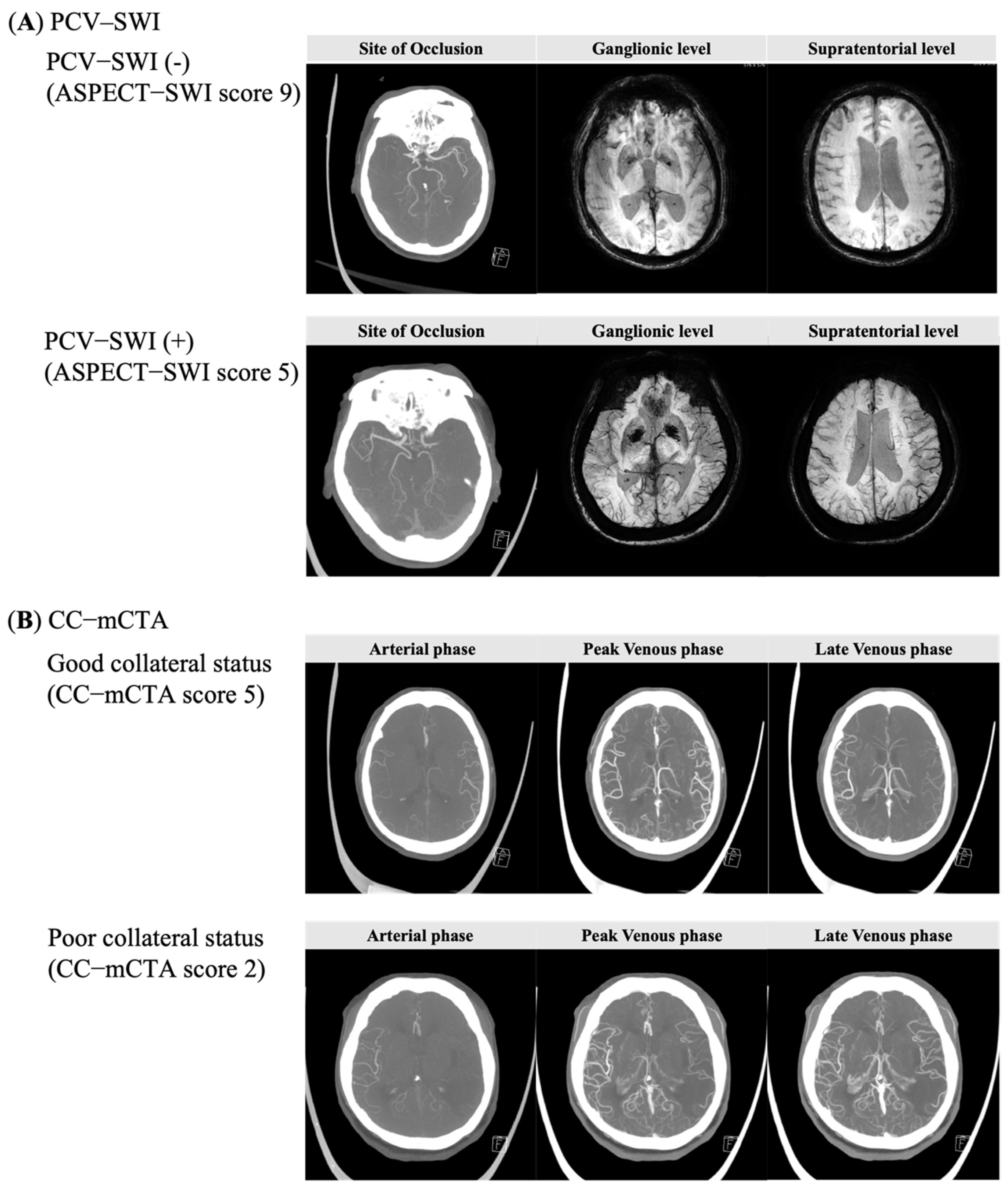
2.2. Imaging Analyses
2.3. Data Collection
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Clinical and Imaging Predictors Associated with Outcomes
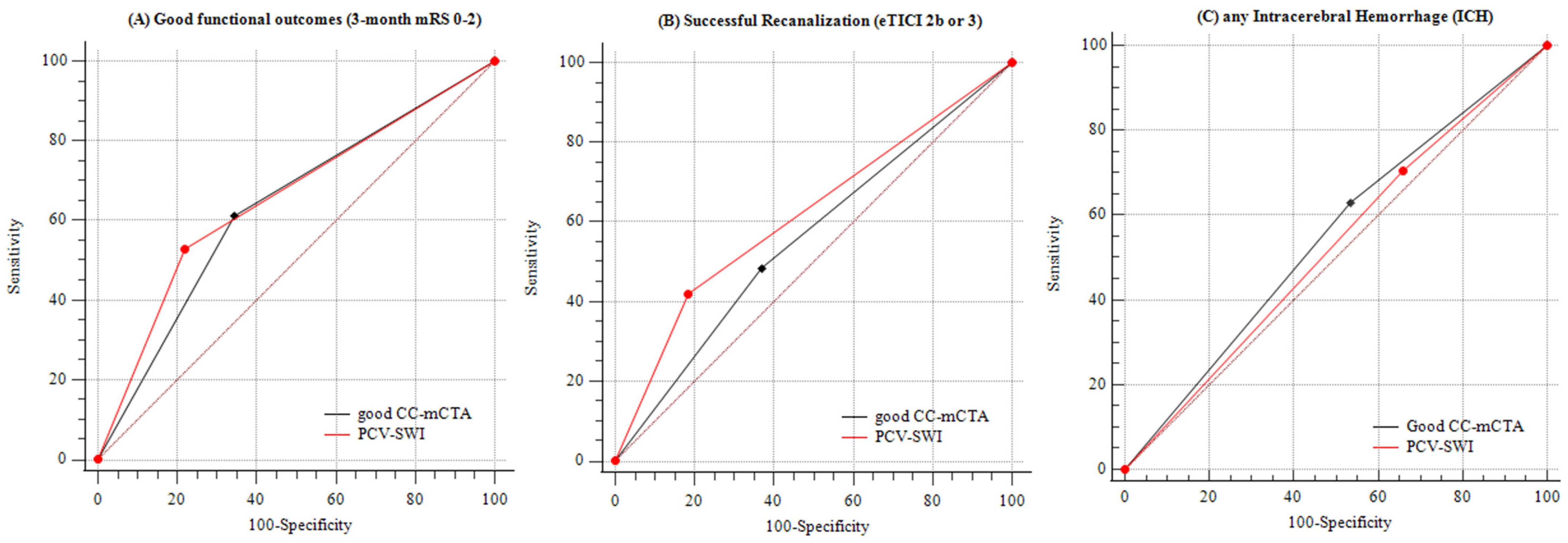
3.3. Comparison of Accuracy between PCV–SWI and CC–mCTA for Predicting Outcomes
3.4. Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AIS | acute ischemic stroke |
| LVO | large vessel occlusion |
| mCTA | multiphase computerized tomography angiography |
| SWI | susceptibility-weighted imaging |
| PCV–SWI | prominent cortical vessels on SWI |
| CC–mCTA | leptomenineal collateral circulation on mCTA |
| ASPECTS | Alberta Stroke Program Early CT Score |
| NIHSS | National Institute of Health Stroke scale |
| mRS | modified Rankin Scale |
| TOAST | Trial of Org 10172 in Acute Stroke Treatment |
| eTICI | expanded Thrombolysis in Cerebral Infarction |
| ICH | intracerebral hemorrhage |
| SD | standard deviation |
| ORs | odds ratios |
| CIs | confidence intervals |
| IQR | interquartile range |
| AIC | Akaike information criterion |
| BIC | Bayesian information criterion |
| AUC | area under the receiver operating curve |
| LAA | large artery atherosclerosis |
| CE | cardioembolism |
| OE | other etiology |
| OEF | oxygen extraction fraction |
| DSA | digital subtraction angiography |
| PWI | perfusion-weighted imaging |
| TOF | time-of-flight |
References
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart Disease and Stroke Statistics-2019 Update: A Report from the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef] [PubMed]
- Kitchen, P.; Salman, M.M.; Halsey, A.M.; Clarke-Bland, C.; MacDonald, J.A.; Ishida, H.; Vogel, H.J.; Almutiri, S.; Logan, A.; Kreida, S.; et al. Targeting Aquaporin-4 Subcellular Localization to Treat Central Nervous System Edema. Cell 2020, 181, 784–799.e19. [Google Scholar] [CrossRef]
- Salman, M.M.; Kitchen, P.; Halsey, A.; Wang, M.X.; Tornroth-Horsefield, S.; Conner, A.C.; Badaut, J.; Iliff, J.J.; Bill, R.M. Emerging Roles for Dynamic Aquaporin-4 Subcellular Relocalization in CNS Water Homeostasis. Brain 2021, awab311. [Google Scholar] [CrossRef] [PubMed]
- Sylvain, N.J.; Salman, M.M.; Pushie, M.J.; Hou, H.; Meher, V.; Herlo, R.; Peeling, L.; Kelly, M.E. The Effects of Trifluoperazine on Brain Edema, Aquaporin-4 Expression and Metabolic Markers during the Acute Phase of Stroke Using Photothrombotic Mouse Model. Biochim. Biophys. Acta Biomembr. 2021, 1863, 183573. [Google Scholar] [CrossRef]
- Goyal, M.; Menon, B.K.; van Zwam, W.H.; Dippel, D.W.J.; Mitchell, P.J.; Demchuk, A.M.; Dávalos, A.; Majoie, C.B.L.M.; van der Lugt, A.; de Miquel, M.A.; et al. Endovascular Thrombectomy after Large-Vessel Ischaemic Stroke: A Meta-Analysis of Individual Patient Data from Five Randomised Trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar] [CrossRef]
- Ko, S.B.; Park, H.K.; Kim, B.M.; Heo, J.H.; Rha, J.H.; Kwon, S.U.; Kim, J.S.; Lee, B.C.; Suh, S.H.; Jung, C.; et al. 2019 Update of the Korean Clinical Practice Guidelines of Stroke for Endovascular Recanalization Therapy in Patients with Acute Ischemic Stroke. J. Stroke 2019, 21, 231–240. [Google Scholar] [CrossRef]
- Ahmed, N.; Audebert, H.; Turc, G.; Cordonnier, C.; Christensen, H.; Sacco, S.; Sandset, E.C.; Ntaios, G.; Charidimou, A.; Toni, D.; et al. Consensus Statements and Recommendations from the ESO-Karolinska Stroke Update Conference, Stockholm 11–13 November 2018. Eur. Stroke J. 2019, 4, 307–317. [Google Scholar] [CrossRef] [Green Version]
- Heit, J.J.; Zaharchuk, G.; Wintermark, M. Advanced Neuroimaging of Acute Ischemic Stroke: Penumbra and Collateral Assessment. Neuroimaging Clin. N. Am. 2018, 28, 585–597. [Google Scholar] [CrossRef]
- Kim, J.T.; Cho, B.H.; Choi, K.H.; Park, M.S.; Kim, B.J.; Park, J.M.; Kang, K.; Lee, S.J.; Kim, J.G.; Cha, J.K.; et al. Magnetic Resonance Imaging Versus Computed Tomography Angiography Based Selection for Endovascular Therapy in Patients with Acute Ischemic Stroke. Stroke 2019, 50, 365–372. [Google Scholar] [CrossRef] [Green Version]
- Bang, O.Y.; Saver, J.L.; Kim, S.J.; Kim, G.M.; Chung, C.S.; Ovbiagele, B.; Lee, K.H.; Liebeskind, D.S. Collateral Flow Predicts Response to Endovascular Therapy for Acute Ischemic Stroke. Stroke 2011, 42, 693–699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen, I.G.; Mulder, M.J.; Goldhoorn, R.B.; Boers, A.M.; van Es, A.C.; Yo, L.S.; Hofmeijer, J.; Martens, J.M.; van Walderveen, M.A.; van der Kallen, B.F.; et al. Impact of Single Phase CT Angiography Collateral Status on Functional Outcome Over Time: Results from the MR CLEAN Registry. J. Neurointerv. Surg. 2019, 11, 866–873. [Google Scholar] [CrossRef]
- Sarraj, A.; Hassan, A.E.; Grotta, J.; Blackburn, S.; Day, A.; Abraham, M.; Sitton, C.; Dannenbaum, M.; Cai, C.; Pujara, D.; et al. Early Infarct Growth Rate Correlation with Endovascular Thrombectomy Clinical Outcomes: Analysis from the SELECT Study. Stroke 2021, 52, 57–69. [Google Scholar] [CrossRef] [PubMed]
- Liebeskind, D.S.; Saber, H.; Xiang, B.; Jadhav, A.P.; Jovin, T.G.; Haussen, D.C.; Budzik, R.F.; Bonafe, A.; Bhuva, P.; Yavagal, D.R.; et al. Collateral Circulation in Thrombectomy for Stroke after 6 to 24 Hours in the DAWN Trial. Stroke 2021, STROKEAHA121034471. [Google Scholar] [CrossRef] [PubMed]
- Menon, B.K.; d’Esterre, C.D.; Qazi, E.M.; Almekhlafi, M.; Hahn, L.; Demchuk, A.M.; Goyal, M. Multiphase CT Angiography: A New Tool for the Imaging Triage of Patients with Acute Ischemic Stroke. Radiology 2015, 275, 510–520. [Google Scholar] [CrossRef] [Green Version]
- Goyal, M.; Demchuk, A.M.; Menon, B.K.; Eesa, M.; Rempel, J.L.; Thornton, J.; Roy, D.; Jovin, T.G.; Willinsky, R.A.; Sapkota, B.L.; et al. Randomized Assessment of Rapid Endovascular Treatment of Ischemic Stroke. N. Engl. J. Med. 2015, 372, 1019–1030. [Google Scholar] [CrossRef] [Green Version]
- Hermier, M.; Nighoghossian, N. Contribution of Susceptibility-Weighted Imaging to Acute Stroke Assessment. Stroke 2004, 35, 1989–1994. [Google Scholar] [CrossRef] [Green Version]
- Verma, R.K.; Hsieh, K.; Gratz, P.P.; Schankath, A.C.; Mordasini, P.; Zubler, C.; Kellner-Weldon, F.; Jung, S.; Schroth, G.; Gralla, J.; et al. Leptomeningeal Collateralization in Acute Ischemic Stroke: Impact on Prominent Cortical Veins in Susceptibility-Weighted Imaging. Eur. J. Radiol. 2014, 83, 1448–1454. [Google Scholar] [CrossRef]
- Park, M.G.; Yang, T.I.; Oh, S.J.; Baik, S.K.; Kang, Y.H.; Park, K.P. Multiple Hypointense Vessels on Susceptibility-Weighted Imaging in Acute Ischemic Stroke: Surrogate Marker of Oxygen Extraction Fraction in Penumbra? Cerebrovasc. Dis. 2014, 38, 254–261. [Google Scholar] [CrossRef]
- Yang, L.; Luo, S. Clinical Application of Susceptibility-Weighted Imaging in the Evaluation of Leptomeningeal Collateralization. Medicine 2018, 97, e13345. [Google Scholar] [CrossRef]
- Huang, P.; Chen, C.H.; Lin, W.C.; Lin, R.T.; Khor, G.T.; Liu, C.K. Clinical Applications of Susceptibility Weighted Imaging in Patients with Major Stroke. J. Neurol. 2012, 259, 1426–1432. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.Y.; Chen, C.I.; Tsai, F.Y.; Tsai, P.H.; Chan, W.P. Prominent Vessel Sign on Susceptibility-Weighted Imaging in Acute Stroke: Prediction of Infarct Growth and Clinical Putcome. PLoS ONE 2015, 10, e0131118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Shi, T.; Chen, B.; Lin, G.; Xu, Y.; Geng, Y. Prominent Hypointense Vessel Sign on Susceptibility-Weighted Imaging Is Associated with Clinical Outcome in Acute Ischaemic Stroke. Eur. Neurol. 2018, 79, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Luo, S.; Yang, L.; Luo, Y. Susceptibility-Weighted Imaging Predicts Infarct Size and Early-Stage Clinical Prognosis in Acute Ischemic Stroke. Neurol. Sci. 2018, 39, 1049–1055. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Xiao, W.M.; Luo, G.P.; Liu, Y.L.; Qu, J.F.; Fang, X.W.; Wang, F.; Chen, Y.K. Asymmetrical Cortical Vein Sign Predicts Early Neurological Deterioration in Acute Ischemic Stroke Patients with Severe Intracranial Arterial Stenosis or Occlusion. BMC Neurol. 2020, 20, 331. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Roh, H.G.; Lee, S.B.; Jeon, Y.S.; Park, J.J.; Lee, T.J.; Jung, Y.J.; Choi, J.W.; Chun, Y.I.; Ki, H.J.; et al. Collateral Estimation by Susceptibility-Weighted Imaging and Prediction of Functional Outcomes after Acute Anterior Circulation Ischemic Stroke. Sci. Rep. 2021, 11, 21370. [Google Scholar] [CrossRef]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., 3rd. Classification of Subtype of Acute Ischemic Stroke. Definitions for Use in a Multicenter Clinical Trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noser, E.A.; Shaltoni, H.M.; Hall, C.E.; Alexandrov, A.V.; Garami, Z.; Cacayorin, E.D.; Song, J.K.; Grotta, J.C.; Campbell, M.S., 3rd. Aggressive Mechanical Clot Disruption: A Safe Adjunct to Thrombolytic Therapy in Acute Stroke? Stroke 2005, 36, 292–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mittal, S.; Wu, Z.; Neelavalli, J.; Haacke, E.M. Susceptibility-Weighted Imaging: Technical Aspects and Clinical Applications, Part 2. AJNR Am. J. Neuroradiol. 2009, 30, 232–252. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; Hu, J.; Miao, Y.; Shen, H.; Tao, D.; Yang, Z.; Li, Q.; Xuan, S.Y.; Raza, W.; Alzubaidi, S.; et al. In Vivo Measurement of Oxygenation Changes after Stroke Using Susceptibility Weighted Imaging Filtered Phase Data. PLoS ONE 2013, 8, e63013. [Google Scholar] [CrossRef]
- Xia, S.; Utriainen, D.; Tang, J.; Kou, Z.; Zheng, G.; Wang, X.; Shen, W.; Haacke, E.M.; Lu, G. Decreased Oxygen Saturation in Asymmetrically Prominent Cortical Veins in Patients with Cerebral Ischemic Stroke. Magn. Reson. Imaging 2014, 32, 1272–1276. [Google Scholar] [CrossRef] [PubMed]
- Santhosh, K.; Kesavadas, C.; Thomas, B.; Gupta, A.K.; Thamburaj, K.; Kapilamoorthy, T.R. Susceptibility Weighted Imaging: A New Tool in Magnetic Resonance Imaging of Stroke. Clin. Radiol. 2009, 64, 74–83. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patients, No. (%) | ||||
|---|---|---|---|---|
| Overall (n = 100) | PCV–SWI (ASPECT–SWI, 0–7) (n = 67) | No PCV–SWI (ASPECT–SWI 8–10) (n = 33) | p-Value | |
| Demographics and clinical characteristics | ||||
| Age, mean (SD), years | 70 (13) | 71.4 (13) | 68 (13) | 0.15 a |
| Male sex | 54 (54.0) | 34 (50.7) | 20 (60.6) | 0.35 b |
| Baseline NIHSS score, median (IQR) | 16 (12, 18) | 16 (13, 19) | 15 (11, 18) | 0.18 c |
| Baseline SBP, median (IQR), mmHg | 140 (130, 160) | 140 (130, 160) | 140 (129, 160) | 0.43 c |
| Baseline glucose concentration, median (IQR) mg/dL | 130 (113, 160) | 137 (113, 157) | 124 (110, 169) | 0.88 c |
| Pre-stroke mRS | 0.98 d | |||
| 0 | 90 (90.0) | 61 (91.0) | 29 (87.9) | |
| 1 | 8 (8.0) | 4 (6.0) | 4 (12.1) | |
| 2 | 2 (2.0) | 2 (3.0) | 0 | |
| TOAST classification | 0.35 d | |||
| Large artery atherosclerosis | 19 (19.) | 9 (13.4) | 10 (30.3) | |
| Cardioembolism | 63 (63.0) | 47 (70.1) | 16 (48.5) | |
| Other determined or undetermined | 18 (18.0) | 11 (16.4) | 7 (21.2) | |
| History of stroke | 20 (20.0) | 16 (23.9) | 4 (12.1) | 0.20 e |
| Hypertension | 70 (70.0) | 50 (74.6) | 20 (60.6) | 0.15 b |
| Diabetes mellitus | 24 (24.0) | 17 (25.4) | 7 (21.2) | 0.65 b |
| Dyslipidemia | 14 (14.0) | 9 (13.4) | 5 (15.2) | 0.82 b |
| Atrial fibrillation | 57 (57.0) | 42 (62.7) | 15 (45.5) | 0.10 b |
| Current smoker | 22 (22.0) | 11 (16.4) | 11 (33.3) | 0.06 b |
| Pre-stroke medication | ||||
| Antiplatelet or anticoagulants agents | 41 (41.0) | 29 (43.3) | 12 (36.4) | 0.51 b |
| Statin | 17 (17.0) | 11 (16.4) | 6 (17.2) | 0.82 b |
| Reperfusion therapy type | ||||
| IV thrombolysis | 15 (15.0) | 9 (13.4) | 6 (18.2) | 0.73 d |
| Endovascular treatment | 30 (30.0) | 21 (31.3) | 9 (27.3) | |
| Combined therapy | 55 (55.0) | 37 (55.2) | 18 (54.5) | |
| Site of occlusion | 0.45 d | |||
| Middle cerebral artery | ||||
| M1 | 59 (59.0) | 37 (55.2) | 22 (66.7) | |
| M2 | 4 (4.0) | 3 (4.5) | 1 (3.0) | |
| Internal carotid artery | 37 (37.0) | 27 (40.3) | 10 (30.3) | |
| ASPECTS–SWI, median (IQR) | 4 (2, 6) | 4 (3, 6) | 9 (8, 9) | <0.01 c |
| Collateral score–mCTA, median (IQR) | 3 (2, 4) | 3 (2, 4) | 4 (4, 4) | <0.01 c |
| Good collateral status (CC–mCTA, 4–5) | 44 (44.0) | 17 (25.4) | 27 (81.8) | <0.01 b |
| Outcomes | ||||
| Successful recanalization (eTICI 2b-3) | 62 (62.0) | 36 (53.7) | 26 (78.8) | 0.02 b |
| Any intracerebral hemorrhage | 27 (27.0) | 19 (28.4) | 8 (24.2) | 0.66 b |
| 3-month mRS score | <0.01 b | |||
| 0–2 | 36 (36.0) | 17 (25.4) | 19 (57.6) | |
| 3–6 | 64 (64.0) | 50 (74.6) | 14 (42.4) | |
| Unadjusted OR | Adjusted OR | |||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age | 0.96 (0.93, 0.99) | 0.02 | 0.98 (0.93, 1.03) | 0.41 |
| Sex (male) | 1.88 (0.81, 4.36) | 0.14 | 0.86 (0.28, 2.64) | 0.79 |
| Baseline NIHSS score | 0.88 (0.81, 0.96) | 0.01 | 0.89 (0.80, 0.99) | 0.03 |
| Initial glucose, mg/dL | 0.99 (0.97, 0.99) | 0.03 | 0.98 (0.97, 0.99) | <0.01 |
| History of stroke | 0.25 (0.07, 0.93) | 0.04 | 0.25 (0.05, 1.36) | 0.11 |
| History of hypertension | 0.23 (0.01, 0.57) | <0.01 | 0.32 (0.10, 1.01) | 0.051 |
| Prior antithrombotic agent | 0.41 (0.17, 0.99) | 0.046 | 0.79 (0.25, 2.54) | 0.70 |
| Site of occlusion | 0.33 | |||
| M2 (reference) | - | |||
| M1 | 2.90 (0.29, 29.5) | 0.34 | ||
| Internal carotid artery | 0.58 (0.05, 6.57) | 0.66 | ||
| PCV–SWI | 0.25 (0.10, 0.61) | <0.01 | 0.24 (0.08, 0.70) | 0.01 |
| Imaging Modality | Adjusted OR (95% CI) | p-Value | C Statistic | AIC | BIC | |
|---|---|---|---|---|---|---|
| Good functional outcome (3-month mRS 0–2) a | ASPECT-SWI (0–10), increase per 1 score | 1.45 (1.16, 1.82) | <0.01 | 0.86 | 105 | 129 |
| PCV–SWI (≤7 versus >7) | 0.24 (0.08, 0.70) | 0.01 | 0.84 | 112 | 135 | |
| CC–mCTA (0–5), increase per 1 score | 2.04 (1.26, 3.30) | <0.01 | 0.85 | 108 | 132 | |
| Good CC–mCTA (≥4 versus <4) | 1.91 (0.71, 5.13) | 0.19 | 0.80 | 117 | 140 | |
| Successful recanalization (eTICI 2b or 3) b | ASPECT-SWI (0–10), increase per 1 score | 1.23 (1.08, 1.51) | <0.01 | 0.69 | 132 | 145 |
| PCV–SWI (≤7 versus >7) | 0.23 (0.08, 0.65) | <0.01 | 0.75 | 124 | 137 | |
| CC–mCTA (0–5), increase per 1 score | 1.49 (1.04, 2.13) | 0.03 | 0.70 | 127 | 140 | |
| Good CC–mCTA (≥4 versus <4) | 1.65 (0.68, 3.98) | 0.27 | 0.67 | 131 | 144 | |
| Any intracerebral hemorrhage c | ASPECT-SWI (0–10), increase per 1 score | 0.91 (0.77, 1.07) | 0.27 | 0.62 | 124 | 137 |
| PCV–SWI (≤7 versus >7) | 1.33 (0.50, 3.55) | 0.57 | 0.61 | 125 | 138 | |
| CC–mCTA (0–5), increase per 1 score | 0.92 (0.64, 1.33) | 0.67 | 0.61 | 125 | 138 | |
| Good CC–mCTA (≥4 versus <4) | 0.69 (0.27, 1.76) | 0.44 | 0.62 | 124 | 137 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, M.; Lee, M. Clinical Implications of Prominent Cortical Vessels on Susceptibility-Weighted Imaging in Acute Ischemic Stroke Patients Treated with Recanalization Therapy. Brain Sci. 2022, 12, 184. https://doi.org/10.3390/brainsci12020184
Oh M, Lee M. Clinical Implications of Prominent Cortical Vessels on Susceptibility-Weighted Imaging in Acute Ischemic Stroke Patients Treated with Recanalization Therapy. Brain Sciences. 2022; 12(2):184. https://doi.org/10.3390/brainsci12020184
Chicago/Turabian StyleOh, Misun, and Minwoo Lee. 2022. "Clinical Implications of Prominent Cortical Vessels on Susceptibility-Weighted Imaging in Acute Ischemic Stroke Patients Treated with Recanalization Therapy" Brain Sciences 12, no. 2: 184. https://doi.org/10.3390/brainsci12020184
APA StyleOh, M., & Lee, M. (2022). Clinical Implications of Prominent Cortical Vessels on Susceptibility-Weighted Imaging in Acute Ischemic Stroke Patients Treated with Recanalization Therapy. Brain Sciences, 12(2), 184. https://doi.org/10.3390/brainsci12020184