
Central Disorders of Hypersomnolence: Association with Fatigue, Depression and Sleep Inertia Prevailing in Women


 ,
,
Abstract
1. Introduction
2. Material and Methods
2.1. Participants and Study Design
2.2. Diagnostic Interview Content and Assessment Instruments
2.3. Statistical Analyses
3. Results
3.1. Demographic Data and Questionnaire Results
3.2. Sex Differences in the Revealed Data and Assessment Instruments
3.3. Comorbid Psychiatric Diseases
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- American Academy of Sleep Medicine. International Classification of Sleep Disorders-ICSD, 3rd ed.; American Academy of Sleep Medicine: Westchester, IL, USA, 2014. [Google Scholar]
- Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; Psychiatric Association: Washington, DC, USA, 2021.
- Kallweit, U.; Bassetti, C. Nosological classification, definition, and epidemiology. In Sleep Medicine Textbook, 2nd ed.; Bassetti, C., McNicholas, W., Paunio, T., Peigneux, P., Eds.; European Sleep Research Society: Regensburg, Germany, 2021; pp. 379–385. ISBN 9781119789017. [Google Scholar]
- Billiard, M.; Sonka, K. Idiopathic hypersomnia: Historical account, critical review of current tests and criteria, diagnostic evaluation in the absence of biological markers and robust electroencephalographic criteria. Nat. Sci. Sleep 2022, 14, 311–322. [Google Scholar] [CrossRef]
- Ambati, A.; Hillary, R.; Leu-Semenescu, S.; Ollila, H.M.; Lin, L.; During, E.H.; Farber, N.; Rico, J.; Faraco, J.; Leary, E.; et al. Kleine-Levin syndrome is associated with birth difficulties and genetic variants in the TRANK1 gene loci. Proc. Natl. Acad. Sci. USA 2021, 118, 12. [Google Scholar] [CrossRef]
- Morse, A.M.; Sanjeev, K. Narcolepsy and psychiatric disorders: Comorbidities or shared pathophysiology? Med. Sci. 2018, 6, 16. [Google Scholar] [CrossRef] [PubMed]
- Meyer, C.; Ferrari, G.J., Jr.; Andrade, R.D.; Barbosa, D.G.; da Silva, R.C.; Pelegrini, A.; Gomes Felden, E.P. Factors associated with excessive daytime sleepiness among Brazilian adolescents. Chronobiol. Int. 2019, 36, 1240–1248. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, J.; Li, S.X.; Chan, N.Y.; Yu, M.M.M.; Lam, S.P.; Chan, J.W.Y.; Li, A.M.; Wing, Y.K. Excessive daytime sleepiness among children and adolescents: Prevalence, correlates, and pubertal effects. Sleep Med. 2019, 53, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hawley, C.J.; Gale, T.M.; Sivakumaran, T.; Paul, S.; Kondan, V.R.G.; Farag, A.; Shahzad, J. Excessive daytime sleepiness in psychiatric disorders: Prevalence, correlates and significance. Psychiatry Res. 2010, 175, 138–141. [Google Scholar] [CrossRef]
- Ma, Z.; Tao, Y.; Chen, H.; Zhang, Y.; Pan, Y.; Meng, D.; Fan, F. An exploration of self-reported sleep inertia symptoms using network analysis. Nat. Sci. Sleep 2022, 14, 661–674. [Google Scholar] [CrossRef]
- Vernet, C.; Arnulf, I. Idiopathic hypersomnia with and without long sleep time: A controlled series of 75 patients. Sleep 2009, 32, 753–759. [Google Scholar] [CrossRef]
- Nevsimalova, S.; Susta, M.; Prihodova, I.; Maurowich Horvat, E.; Milata, M.; Sonka, K. Idiopathic hypersomnia: A homogeneous or heterogeneous disease? Sleep Med. 2021, 80, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.M.; Priest, R.G.; Zulley, J.; Smirne, S.; Paiva, T. Prevalence of narcolepsy symptomatology and diagnosis in the European general population, Neurology 2002, 58, 1826–1833. Neurology 2022, 58, 1826–1833. [Google Scholar] [CrossRef]
- Piilgaard, L.; Rose, L.; Gylling Hviid, C.; Kohlmeier, K.A.; Rahbek Kornum, B. Sex-related difference within sleep-wake dynamics, cataplexy, and EEG fast-delta power in narcolepsy mouse model. Sleep 2022, 45, zsac058. [Google Scholar] [CrossRef]
- Zhang, Z.; Dauvilliers, Y.; Plazzi, G.; Mayer, G.; Lammers, G.J.; Santamaria, J.; Partinen, M.; Overeem, S.; del Rio Villegas, R.; Sonka, K.; et al. Idling for decades: A European study on risk factors associated with the delay before a narcolepsy diagnosis. Nat. Sci. Sleep 2022, 14, 1031–1047. [Google Scholar] [CrossRef]
- Won, C.; Mahmoudi, M.; Purvis, T.; Mathur, A.; Mohsenin, V. The impact of gender on timeliness of narcolepsy diagnosis. J. Clin. Sleep Med. 2014, 10, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Gool, J.K.; Zhang, Z.; Oei, M.S.S.L.; Mathias, S.; Dauvilliers, Y.; Mayer, G.; Plazzi, G.; del Rio Villegas, R.; Santamaria, J.; Šonka, K.; et al. Data-driven phenotyping of central disorders of hypersomnolence with unsupervised clustering. Neurology 2022, 98, 23. [Google Scholar] [CrossRef]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders, 2nd ed.; Diagnostic and Coding Manual; American Academy of Sleep Medicine: Westchester, IL, USA, 2005. [Google Scholar]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Dauvilliers, Y.; Beziat, S.; Pesenti, C.; Lopez, R.; Barateau, L.; Carlander, B.; Lucas, G.; Tafti, M.; Morin, C.; Billiard, M.; et al. Measurement of narcolepsy symptoms: The Narcolepsy severity score. Neurology 2017, 88, 1358–1365. [Google Scholar] [CrossRef]
- Dauvilliers, Y.; Evangelista, E.; Barateau, L.; Lopez, R.; Chenini, S.; Delbos, C.; Beziat, S.; Jaussent, I. Measurement of idiopathic hypersomnia. Idiopathic hypersomnia severity scale. Neurology 2019, 92, 1358–1365. [Google Scholar] [CrossRef] [PubMed]
- Snaith, R.P. The hospital anxiety and depression scale. Health Qual. Life Outcomes 2003, 1, 29. [Google Scholar] [CrossRef]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef]
- Kanady, J.C.; Harvey, A.G. Development and validation of the sleep inertia questionnaire (SIQ) and assessment of sleep inertia in analogue and clinical depression. Cogn. Ther. Res. 2015, 39, 601–612. [Google Scholar] [CrossRef]
- Chokroverty, S. Sleep deprivation and excessive daytime sleepiness. In Sleep Disorders Medicine. Basic Science, Technical Considerations and Clinical Aspects, 4th ed.; Chokroverty, S., Ed.; Springer: New York, NY, USA, 2017; Volume 1, pp. 29–39. ISBN 978-1-4939-6576-2. [Google Scholar]
- Veauthier, C. Younger age, female sex, and high number of awakening and arousals predict fatigue in patients with sleep disorders: A retrospective polysomnographic retrospective study. Neuropeychiatr. Dis. Treat. 2013, 9, 1483–1494. [Google Scholar] [CrossRef]
- Droogleever Fortuyn, H.A.; Fronczek, R.; Smits, M.; Overeem, S.; Lappenschaar, M.; Kalkman, J.; Renirer, W.; Buitelaar, J.; Lammers, G.J. Severe fatigue in narcolepsy with cataplexy. J. Sleep Res. 2012, 21, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Dauvilliers, Y.; Lopez, R.; Ohayon, M.; Bayard, S. Hypersomnia and depressive symptoms: Methodological and clinical aspects. BMC Med. 2013, 11, 78. [Google Scholar] [CrossRef]
- Sparasci, D.; Gobbi, C.; Castelnovo, A.; Riccitelli, G.C.; Disanto, G.; Zecca, C.; Manconi, M. Fatigue, sleepiness and depression in multiple sclerosis: Defining the overlaps for a better phenotyping. J. Neurol. 2022, 269, 4961–4971. [Google Scholar] [CrossRef]
- Fronczek, R.; Arnulf, I.; Bauman, C.R.; Maski, K.; Pizza, F.; Trotti, L.M. To split or to lump? Classifying the central disorders of hypersomnolence. Sleep 2020, 43, zsaa044. [Google Scholar] [CrossRef]
- Buskova, J.; Dvorakova, T.; Kralova, R.; Nevsimalova, S.; Milata, M.; Galuskova, K.; Dostalova, S.; Sonka, K. Narcolepsy severity scale and its psychometric features in the patients with narcolepsy type 1 in the Czech Republic. Cs. Slov. Neurol. Neurochir. 2022; in press. (In Czech) [Google Scholar]
- Gudka, S.; Haynes, E.; Scotney, J.; Mukherjee, S.; Frenkel, S.; Sivam, S.; Swieca, J.; Chamula, K.; Cunnington, D.; Saini, B. Narcolepsy: Clomorbidities, complexities, and future directions. Sleep Med. Rev. 2022; in press. [Google Scholar] [CrossRef]
- BaHamman, A.S.; Alnakshabandi, K.; Pandi-Perumal, S.R. Neuropsychiatric correlates of narcolepsy. Curr. Psychiatry Rep. 2020, 22, 36. [Google Scholar] [CrossRef]
- Chen, Q.; de Lecea, L.; Hu, Z.; Gao, D. The hypocretin/orexin system: An increasingly important role in neuropsychiatry. Med. Res. Rev. 2015, 35, 152–197. [Google Scholar] [CrossRef] [PubMed]
- Canellas, F.; Lin, L.; Julia, M.R.; Clemente, A.; Vives-Bauza, C.; Ollila, H.M.; Hong, S.C.; Arboleya, S.M.; Einen, M.E.; Faraco, J.; et al. Dual cases of type 1 narcolepsy with schizophrenia and other psychotic disorders. J. Clin. Sleep Med. 2014, 10, 1011–1018. [Google Scholar] [CrossRef]
- Lu, J.; Huang, M.L.; Li, J.H.; Jin, K.Y.; Li, M.H.; Mou, T.T.; Fronczek, R.; Duan, J.F.; Xu, W.J.; Swaab, D.; et al. Changes of hypocretin (orexin) system in schizophrenia: From plasma to brain. Schizophr. Bull. 2021, 47, 1310–1319. [Google Scholar] [CrossRef] [PubMed]
- Arnulf, I.; Leu-Semenescu, S.; Doder, P. Precision medicine for idiopathic hypersomnia. Sleep Med. Clin. 2019, 14, 333–350. [Google Scholar] [CrossRef] [PubMed]
- Buskova, J.; Novak, T.; Miletinova, E.; Kralova, R.; Kostalova, J.; Klikova, M.; Veldova, K. Subjective symptoms and objective measures in idiopathic hypersomnia and hypersomnia associated with psychiatric disorders: A prospective cross-sectional study. J. Clin. Sleep Med. 2022, 18, 713–720. [Google Scholar] [CrossRef]



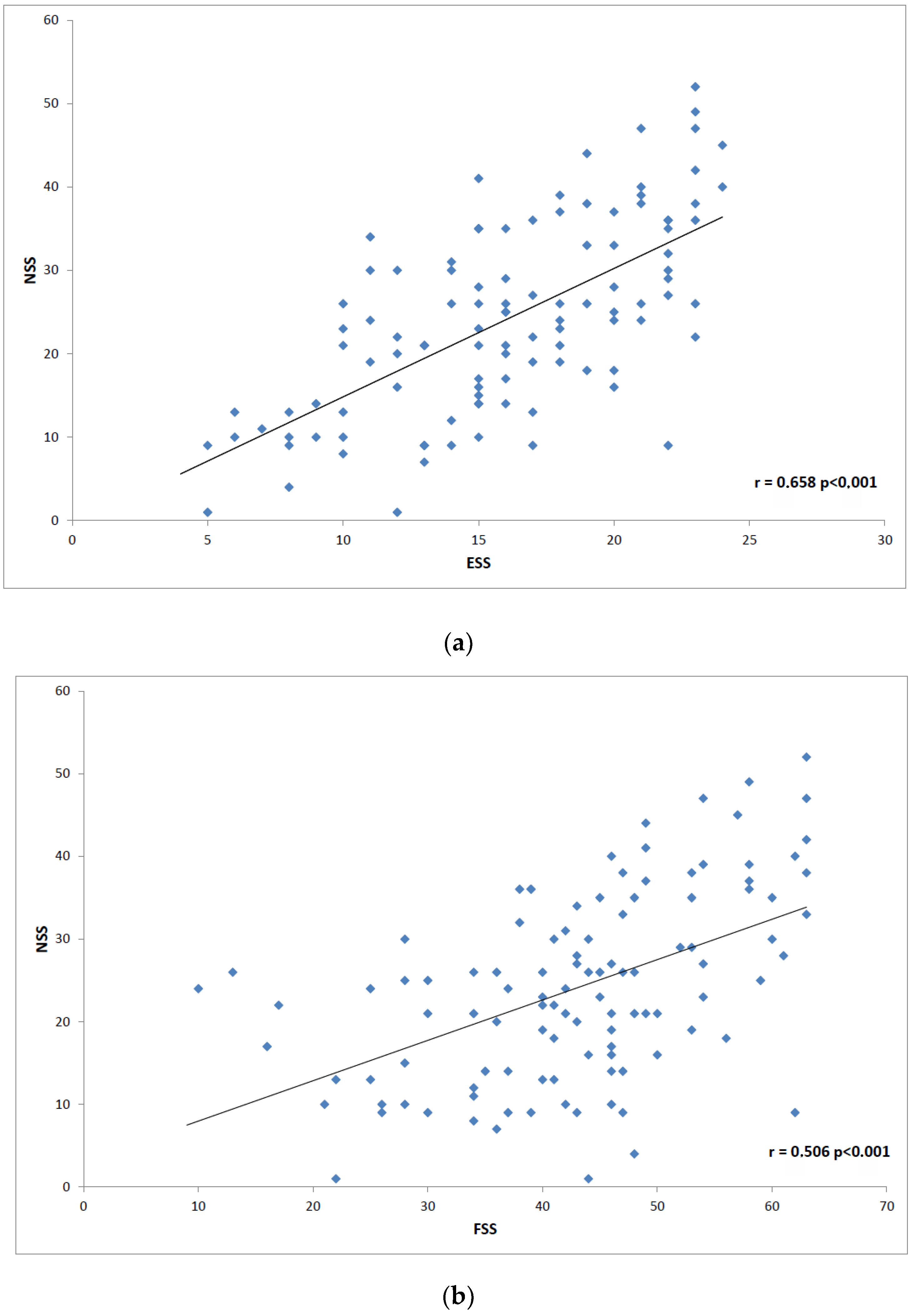{kind=link}
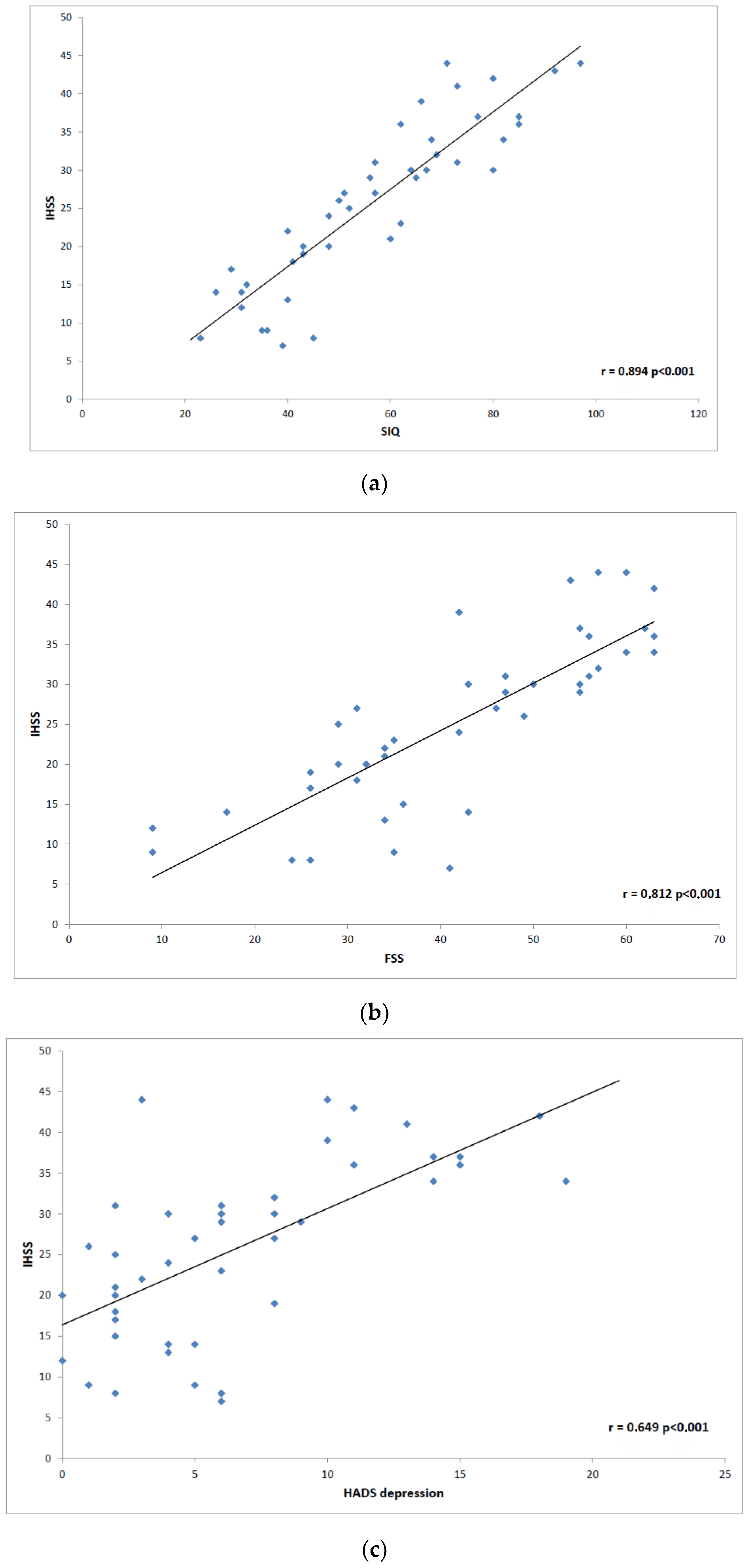{kind=link}
| Parameters | NT1 | NT2 | IH | Total | Sign. |
|---|---|---|---|---|---|
| Age (years) | 33 ± 12.7 | 35.5 ± 14.3 | 41 ± 13.2 | 35.45 ± 13.39 | NT1 vs. NT2 NS NT1 vs. IH ** NT2 vs. IH NS |
| N women (%) | 87 53 (61%) | 22 13 (59%) | 39 27 (69%) | 148 93 (63%) | NS |
| BMI | 30.3 ± 7.6 | 25.7 ± 4.8 | 26.5 ± 6.0 | 28.64 ± 7.16 | NT1 vs. NT2 ** NT1 vs. IH ** NT2 vs. IH NS |
| HADS Anxiety | 5.78 ± 3.90 | 6.91 ± 4.23 | 7.15 ± 4.52 | 6.32 ± 4.14 | NT1 vs. NT2 NS NT1 vs. IH NS NT2 vs. IH NS |
| HADS Depression | 4.61 ± 3.59 | 6.45 ± 4.96 | 6.69 ± 5.18 | 5.45 ± 4.36 | NT1 vs. NT2 NS NT1 vs. IH * NT2 vs. IH NS |
| ESS | 16.83 ± 4.68 | 12.95 ± 4.37 | 13.74 ± 4.78 | 15.44 ± 4.93 | NT1 vs. NT2 ** NT1 vs. IH ** NT2 vs. IH NS |
| NSS | 26.47 ± 10.87 | 14.91 ± 8.17 | - | 23.91 ± 11.41 | NT1 vs. NT2 *** |
| IHSS | - | - | 25.93 ± 10.96 | 25.93 ± 10.96 | - |
| FSS | 43.57 ± 11.46 | 41.09 ± 12.91 | 42.0 ± 15.84 | 42.79 ± 12.90 | NS |
| SIQ | 47.79 ± 14.86 | 53.24 ± 19.33 | 57.56 ± 19.72 | 51.16 ± 17.34 | NT1 vs. NT2 NS NT1 vs. IH ** NT2 vs. IH NS |
| IH1 N = 21 | IH2 N = 18 | Sign. | |
|---|---|---|---|
| IHSS | 21.71 ± 9.64 | 33.71 ± 7.77 | p < 0.001 |
| HADS Anxiety Mean ± SD | 6.43 ± 3.93 | 8.00 ± 5.11 | NS |
| HADS Depression Mean ± SD | 5.62 ± 4.93 | 7.94 ± 5.31 | NS |
| FSS Mean ± SD | 36.67 ± 14.96 | 48.22 ± 14.89 | p < 0.05 |
| ESS Mean ± SD | 12.29 ± 4.53 | 15.44 ± 4.62 | p < 0.05 |
| SIQ Mean ± SD | 50.8 ± 20.6 | 65.5 ± 15.7 | p < 0.05 |
| NT1 N = 87 | NT2 N = 22 | IH N = 39 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| W N = 53 | M N = 34 | Sign. | W N = 13 | M N = 9 | Sign. | W N = 27 | M N = 12 | Sign. | |
| HADS Anxiety Mean ± SE | 6.15 ± 0.56 | 5.18 ± 0.71 | NS | 8.46 ± 1.13 | 4.67 ± 1.35 | p < 0.05 | 7.74 ± 0.78 | 5.83 ± 1.17 | NS |
| HADS Depression Mean ± SD | 4.85 ± 0.59 | 4.24 ± 0.74 | NS | 7.69 ± 1.18 | 4.67 ± 1.42 | NS | 7.30 ± 0.82 | 5.33 ± 1.23 | NS |
| FSS Mean ± SD | 44.30 ± 1.72 | 42.44 ± 2.15 | NS | 48.54 ± 3.47 | 30.33 ± 4.18 | p < 0.01 | 43.48 ± 2.41 | 38.67 ± 3.62 | NS |
| ESS Mean ± SD | 17.40 ± 0.63 | 15.94 ± 0.78 | NS | 15.08 ± 1.27 | 9.89 ± 1.52 | p < 0.01 | 13.89 ± 0.88 | 13.42 ± 1.32 | NS |
| SIQ Mean ± SD | 48.85 ± 2.30 | 46.15 ± 2.87 | NS | 60.42 ± 4.82 | 43.67 ± 5.57 | p < 0.05 | 59.30 ± 3.22 | 53.67 ± 4.82 | NS |
| Psychiatric Disease | NT1 N = 87 | NT2 N = 22 | IH N = 39 | Total N = 148 |
|---|---|---|---|---|
| Mixed anxiety-depressive disorder | 19 (21.9%) | 8 (36.4%) | 16 (41.0%) | 43 (29.0%) |
| Depression | 3 (3.5%) | 0 (0.0%) | 3 (7.7%) | 6 (4.1%) |
| General anxiety syndrome | 5 (5.8%) | 0 (0.0%) | 2 (5.1%) | 7 (4.7%) |
| Attention deficit hyperactivity disorder | 2 (2.3%) | 2 (9.1%) | 0 (0.0%) | 4 (2.7%) |
| Pervasive developmental disorders | 2 (2.3%) | 0 (0.0%) | 0 (0.0%) | 2 (1.3%) |
| Schizophrenia | 2 (2.3%) | 0 (0.0%) | 0 (0.0%) | 2 (1.3 %) |
| Total | 33 (38.1 %) | 10 (45.5%) | 21 (53.8%) | 64 (43.1%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nevsimalova, S.; Skibova, J.; Galuskova, K.; Prihodova, I.; Dostalova, S.; Maurovich-Horvat, E.; Šonka, K. Central Disorders of Hypersomnolence: Association with Fatigue, Depression and Sleep Inertia Prevailing in Women. Brain Sci. 2022, 12, 1491. https://doi.org/10.3390/brainsci12111491
Nevsimalova S, Skibova J, Galuskova K, Prihodova I, Dostalova S, Maurovich-Horvat E, Šonka K. Central Disorders of Hypersomnolence: Association with Fatigue, Depression and Sleep Inertia Prevailing in Women. Brain Sciences. 2022; 12(11):1491. https://doi.org/10.3390/brainsci12111491
Chicago/Turabian StyleNevsimalova, Sona, Jelena Skibova, Karolina Galuskova, Iva Prihodova, Simona Dostalova, Eszter Maurovich-Horvat, and Karel Šonka. 2022. "Central Disorders of Hypersomnolence: Association with Fatigue, Depression and Sleep Inertia Prevailing in Women" Brain Sciences 12, no. 11: 1491. https://doi.org/10.3390/brainsci12111491
APA StyleNevsimalova, S., Skibova, J., Galuskova, K., Prihodova, I., Dostalova, S., Maurovich-Horvat, E., & Šonka, K. (2022). Central Disorders of Hypersomnolence: Association with Fatigue, Depression and Sleep Inertia Prevailing in Women. Brain Sciences, 12(11), 1491. https://doi.org/10.3390/brainsci12111491