
MaDoPO: Magnetic Detection of Positions and Orientations of Segmented Deep Brain Stimulation Electrodes: A Radiation-Free Method Based on Magnetoencephalography

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
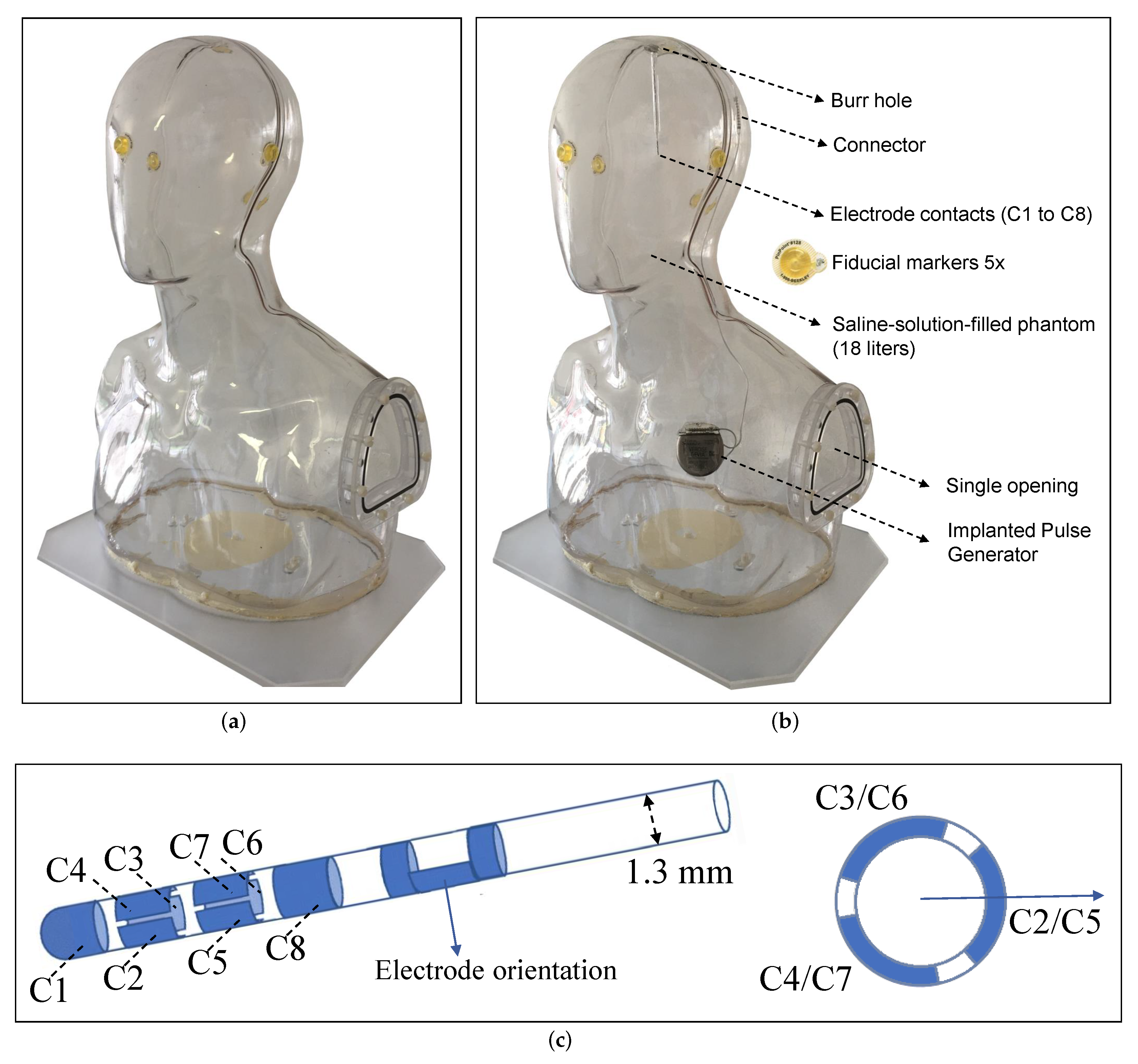
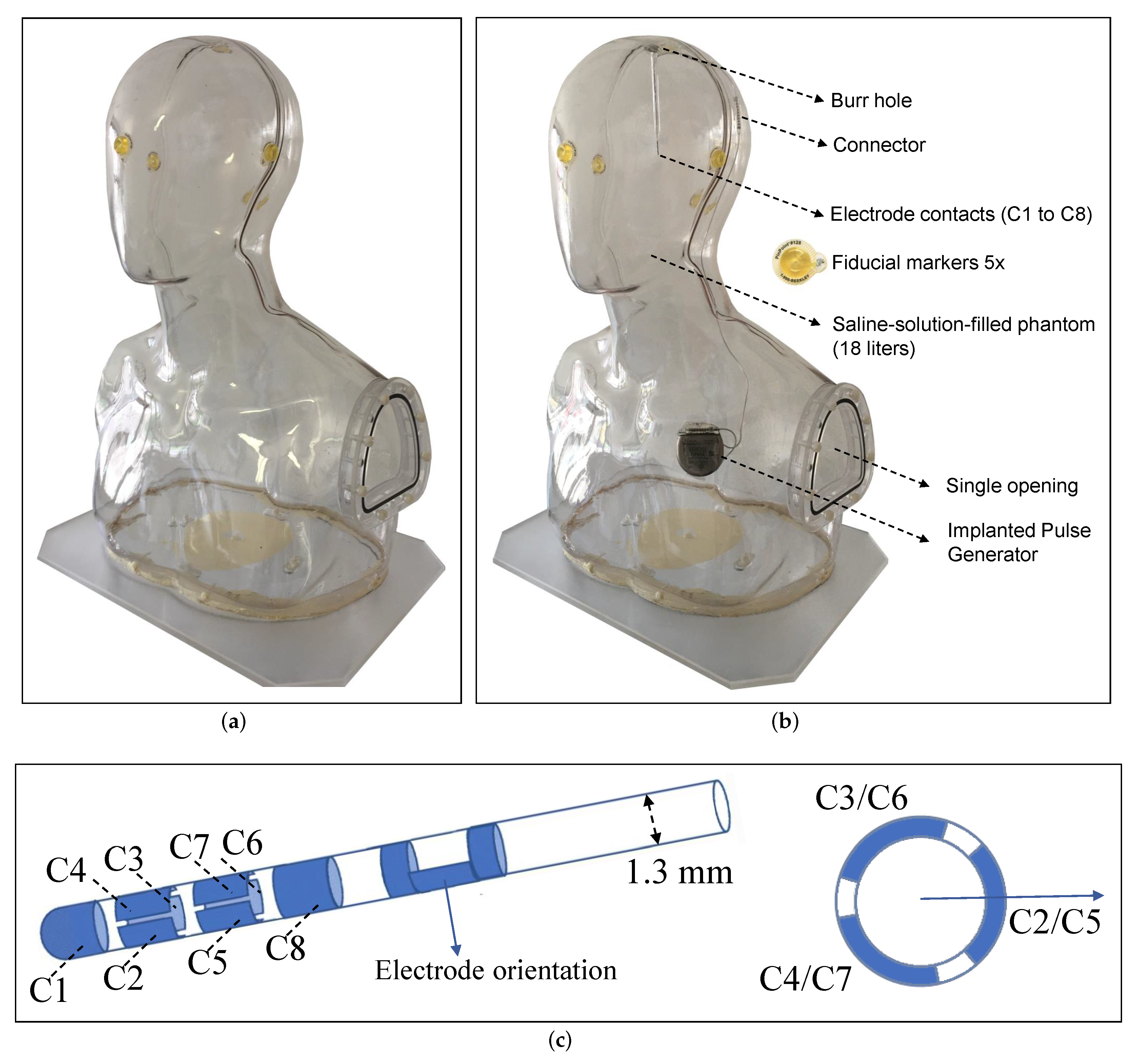
2.1. Phantom Design
2.2. Neuroimaging of the Phantom
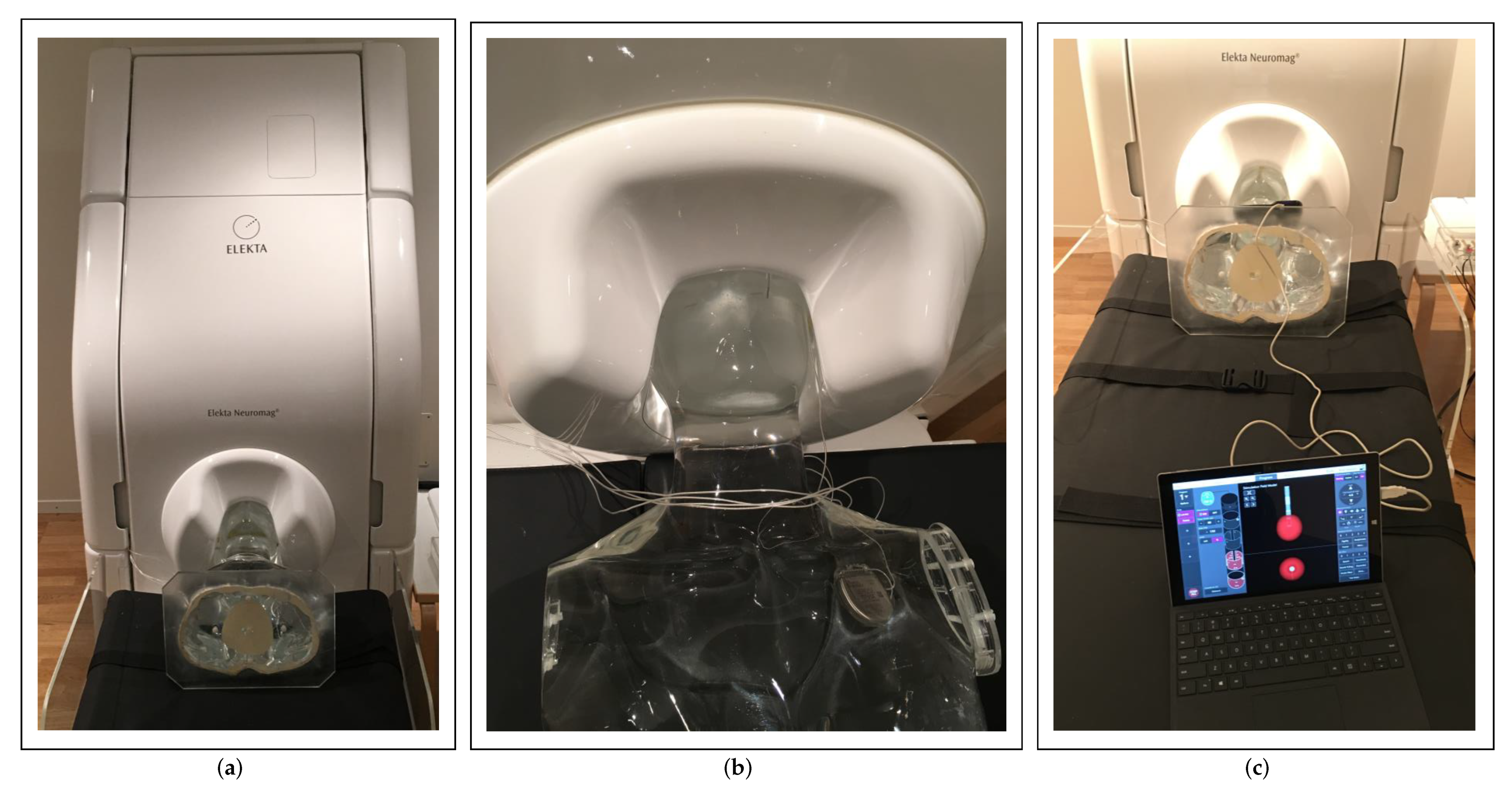
2.3. MEG Preparation
2.4. MEG Data Acquisition
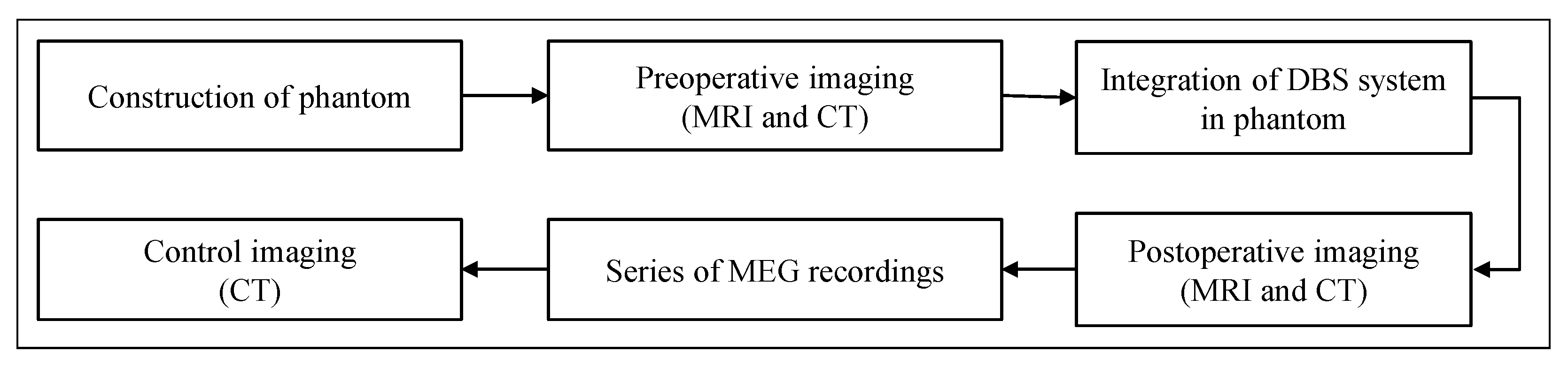
2.5. The Pipeline of the MaDoPO Method
2.6. Signal Processing of Measured Data
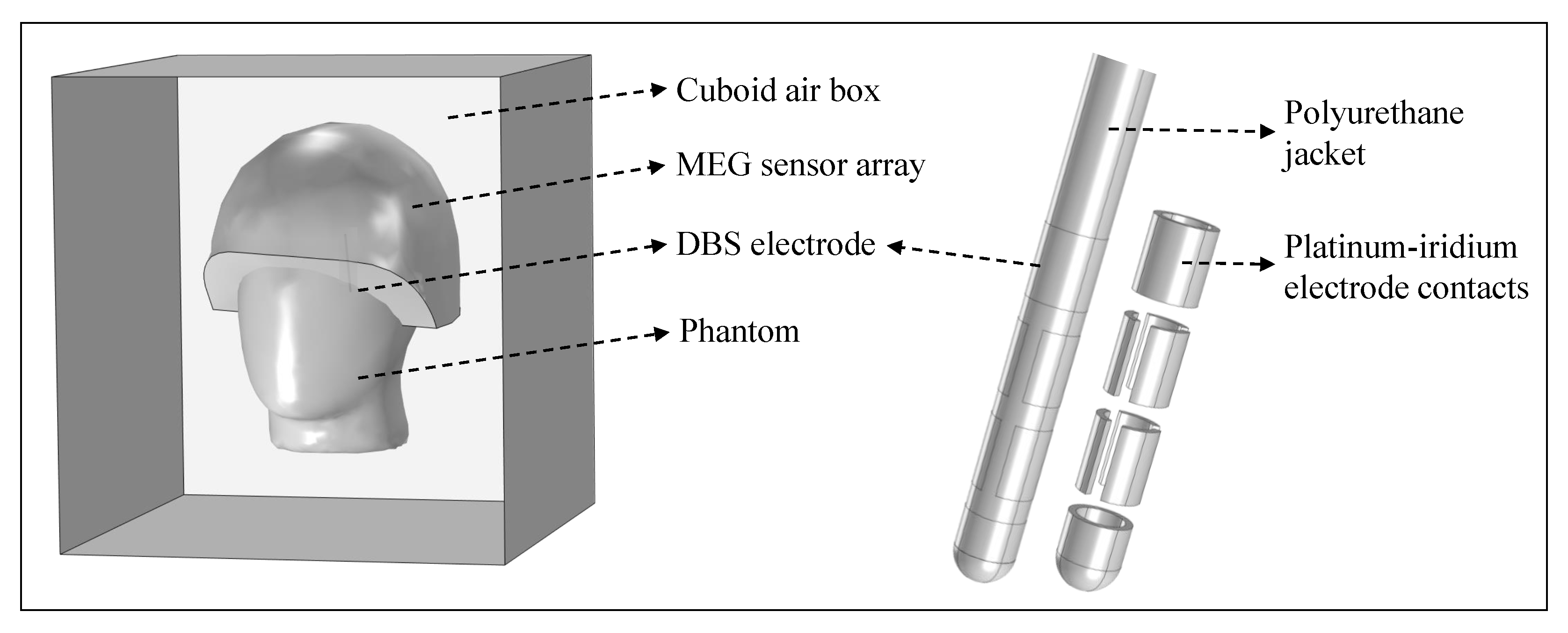
2.7. Modeling
2.7.1. Simplified Model
2.7.2. The Finite Element Electromagnetic Model
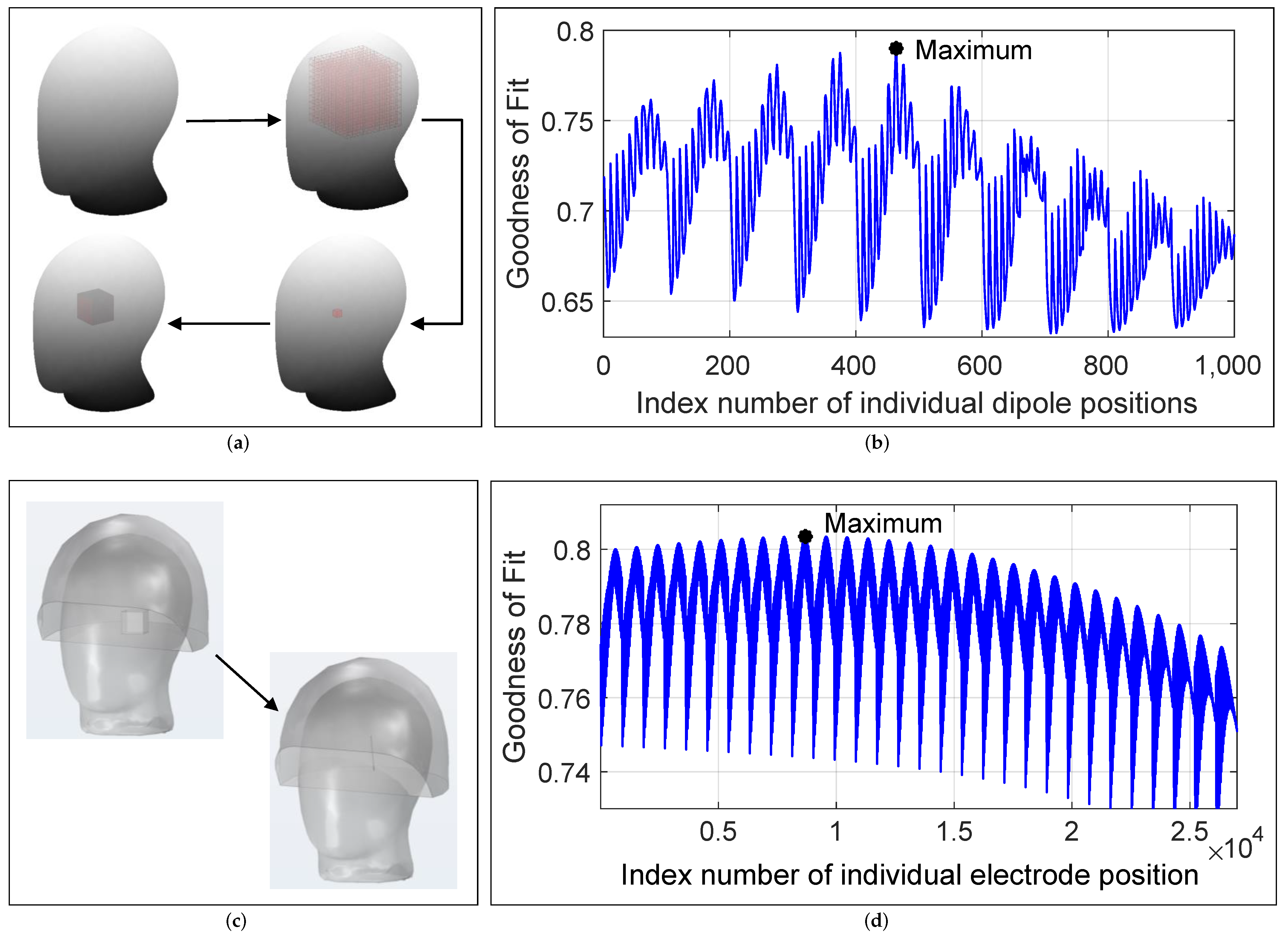
2.8. The Method Used for Electrode Localization
2.9. The Method Used for Electrode Orientation Detection
3. Electrode Localization Results
3.1. Electrode Pre- and Post-Localization
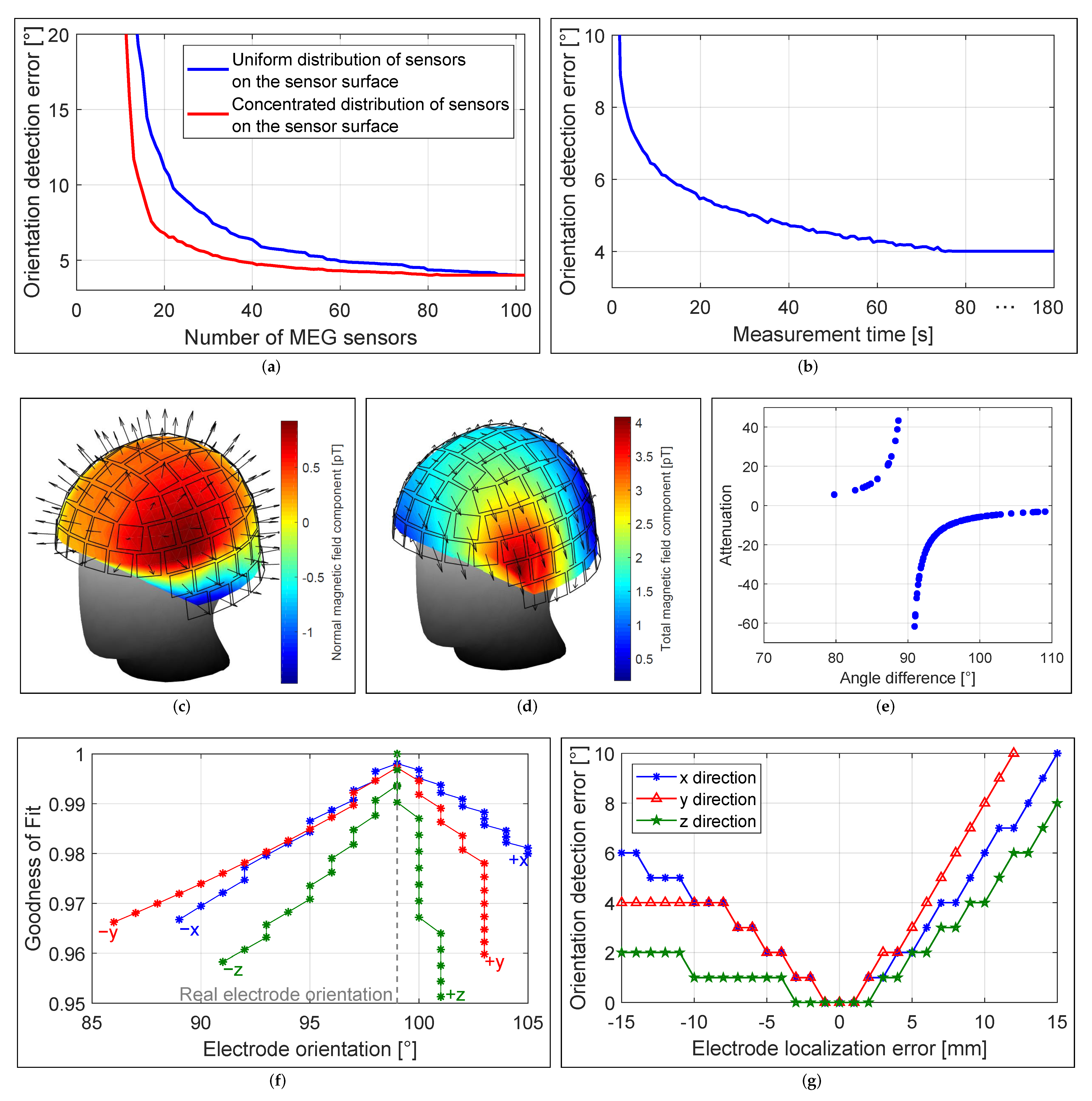
3.2. Localization Accuracy and Number of Sensors
3.3. Localization Accuracy and Number of Recordings
3.4. Localization Accuracy and Measurement Time
3.5. Localization Accuracy and Sensor Orientation
4. Electrode Orientation Detection Results
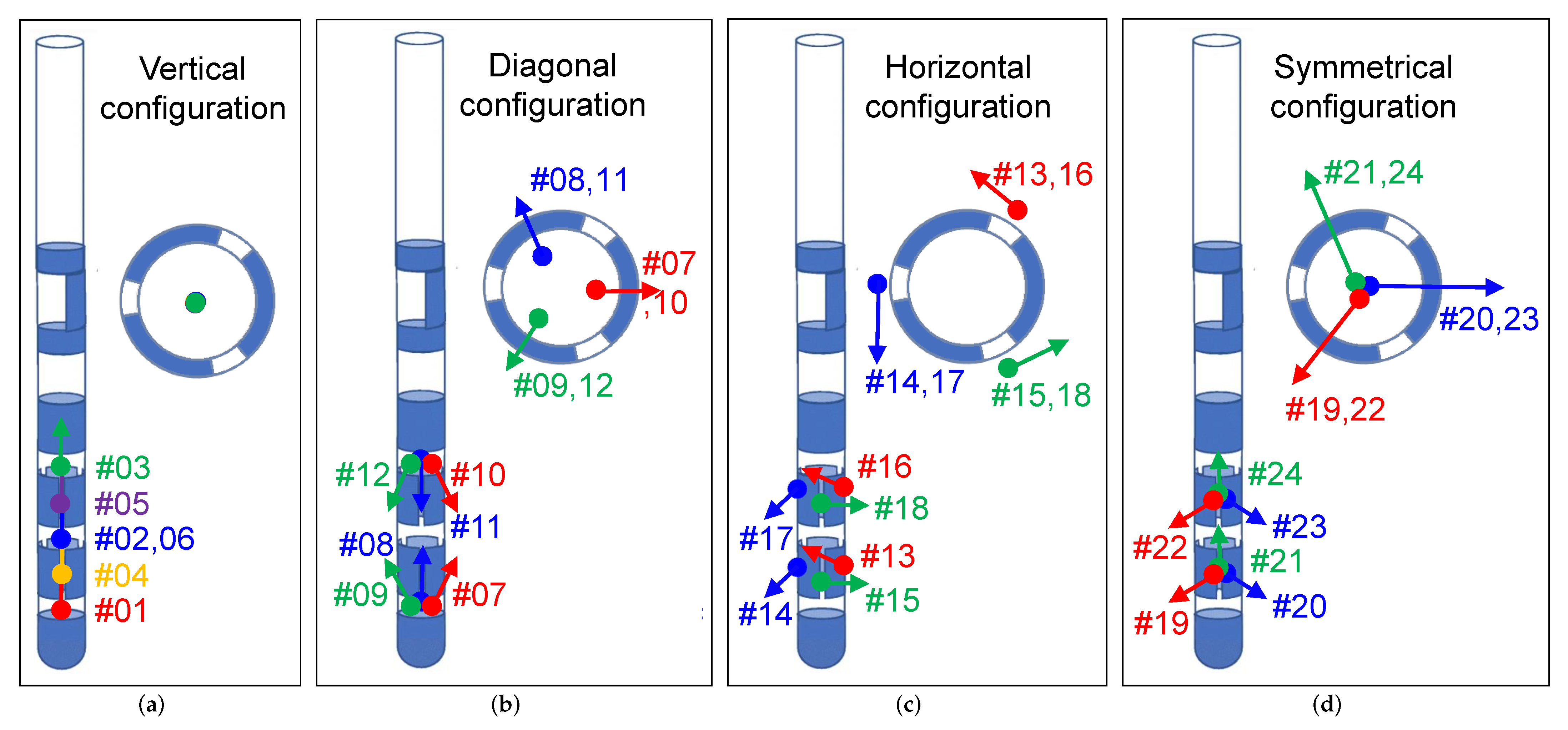
4.1. Diagonal Electrode Configuration
4.2. Horizontal Electrode Configuration
4.3. Symmetrical Electrode Configuration
4.4. Horizontal and Symmetrical Electrode Configuration
4.5. Orientation Detection Accuracy and Number of Sensors
4.6. Orientation Detection Accuracy and Measurement Time
4.7. Orientation Detection Accuracy and Sensor Orientation
4.8. Orientation Detection Accuracy and Localization Error
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lozano, A.; Lipsman, N. Probing and Regulating Dysfunctional Circuits Using Deep Brain Stimulation. Neuron 2013, 77, 406–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vedam-Mai, V.; Deisseroth, K.; Giordano, J.; Lazaro-Munoz, G.; Chiong, W.; Suthana, N.; Langevin, J.P.; Gill, J.; Goodman, W.; Provenza, N.R.; et al. Proceedings of the Eighth Annual Deep Brain Stimulation Think Tank: Advances in Optogenetics, Ethical Issues Affecting DBS Research, Neuromodulatory Approaches for Depression, Adaptive Neurostimulation, and Emerging DBS Technologies. Front. Hum. Neurosci. 2021, 15, 169. [Google Scholar] [CrossRef]
- Harmsen, I.E.; Elias, G.J.; Beyn, M.E.; Boutet, A.; Pancholi, A.; Germann, J.; Mansouri, A.; Lozano, C.S.; Lozano, A.M. Clinical trials for deep brain stimulation: Current state of affairs. Brain Stimul. 2020, 13, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Lange, F.; Steigerwald, F.; Malzacher, T.; Brandt, G.A.; Odorfer, T.M.; Roothans, J.; Reich, M.M.; Fricke, P.; Volkmann, J.; Matthies, C.; et al. Reduced Programming Time and Strong Symptom Control Even in Chronic Course through Imaging-Based DBS Programming. Front. Neurol. 2021, 12, 2072. [Google Scholar] [CrossRef]
- Butson, C.R.; McIntyre, C.C. Current steering to control the volume of tissue activated during deep brain stimulation. Brain Stimul. 2008, 1, 7–15. [Google Scholar] [CrossRef] [Green Version]
- Steigerwald, F.; Müller, L.; Johannes, S.; Matthies, C.; Volkmann, J. Directional deep brain stimulation of the subthalamic nucleus: A pilot study using a novel neurostimulation device. Mov. Disord. 2016, 31, 1240–1243. [Google Scholar] [CrossRef]
- Pollo, C.; Kaelin-Lang, A.; Oertel, M.F.; Stieglitz, L.; Taub, E.; Fuhr, P.; Lozano, A.M.; Raabe, A.; Schüpbach, M. Directional deep brain stimulation: An intraoperative double-blind pilot study. Brain 2014, 137, 2015–2026. [Google Scholar] [CrossRef] [Green Version]
- Schnitzler, A.; Mir, P.; Brodsky, M.; Verhagen, L.; Groppa, S.; Alvarez, R.; Evans, A.; Blazquez, M.; Nagel, S.; Pilitsis, J.; et al. Directional Deep Brain Stimulation for Parkinson’s Disease: Results of an International Crossover Study With Randomized, Double-Blind Primary Endpoint. Neuromodulation 2021. [Google Scholar] [CrossRef]
- Engelhardt, J.; Guehl, D.; Damon-Perrière, N.; Branchard, O.; Burbaud, P.; Cuny, E. Localization of Deep Brain Stimulation Electrode by Image Registration Is Software Dependent: A Comparative Study between Four Widely Used Software Programs. Stereotact. Funct. Neurosurg. 2018, 96, 364–369. [Google Scholar] [CrossRef]
- Ellenbogen, J.R.; Tuura, R.; Ashkan, K. Localisation of DBS Electrodes Post-Implantation, to CT or MRI? Which Is the Best Option? Stereotact. Funct. Neurosurg. 2018, 96, 347–348. [Google Scholar] [CrossRef] [Green Version]
- Pinsker, M.; Herzog, J.; Falk, D.; Volkmann, J.; Deuschl, G.; Mehdorn, H.M. Accuracy and Distortion of Deep Brain Stimulation Electrodes on Postoperative MRI and CT. Zentralblatt für Neurochirurgie 2008, 69, 144–147. [Google Scholar] [CrossRef]
- Reinacher, P.; Krüger, M.; Coenen, V.; Shah, M.; Roelz, R.; Jenkner, C.; Egger, K. Determining the Orientation of Directional Deep Brain Stimulation Electrodes Using 3D Rotational Fluoroscopy. Am. J. Neuroradiol. 2017, 38, 1111–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunsche, S.; Neudorfer, C.; Majdoub, F.E.; Maarouf, M.; Sauner, D. Determining the Rotational Orientation of Directional Deep Brain Stimulation Leads Employing Flat-Panel Computed Tomography. Oper. Neurosurg. 2018, 16, 465–470. [Google Scholar] [CrossRef]
- Sitz, A.; Hoevels, M.; Hellerbach, A.; Gierich, A.; Luyken, K.; Dembek, T.A.; Klehr, M.; Wirths, J.; Visser-Vandewalle, V.; Treuer, H. Determining the orientation angle of directional leads for deep brain stimulation using computed tomography and digital X-ray imaging: A phantom study. Med. Phys. 2017, 44, 4463–4473. [Google Scholar] [CrossRef] [PubMed]
- Dembek, T.A.; Hellerbach, A.; Jergas, H.; Eichner, M.; Wirths, J.; Dafsari, H.S.; Barbe, M.T.; Hunsche, S.; Visser-Vandewalle, V.; Treuer, H. DiODe v2: Unambiguous and Fully-Automated Detection of Directional DBS Lead Orientation. Brain Sci. 2021, 11, 1450. [Google Scholar] [CrossRef] [PubMed]
- Kurtev-Rittstieg, R.; Achatz, S.; Nourinia, A.; Mittermeyer, S. Orientation of Directional Deep Brain Stimulation Leads on CT: Resolving the Ambiguity. bioRxiv 2020. [Google Scholar] [CrossRef]
- Iacono, M.I.; Atefi, S.R.; Mainardi, L.; Walker, H.C.; Angelone, L.M.; Bonmassar, G. A Study on the Feasibility of the Deep Brain Stimulation (DBS) Electrode Localization Based on Scalp Electric Potential Recordings. Front. Physiol. 2019, 9, 1788. [Google Scholar] [CrossRef]
- Yalaz, M.; Teplyuk, A.; Muthuraman, M.; Deuschl, G.; Höft, M. The Magnetic Properties of Electrical Pulses Delivered by Deep Brain Stimulation Systems. IEEE Trans. Instrum. Meas. 2020, 69, 4303–4313. [Google Scholar] [CrossRef]
- Yalaz, M.; Teplyuk, A.; Deuschl, G.; Höft, M. Dipole Fit Localization of the Deep Brain Stimulation Electrode Using 3D Magnetic Field Measurements. IEEE Sens. J. 2020, 20, 9550–9557. [Google Scholar] [CrossRef]
- Yalaz, M.; Noor, M.S.; McIntyre, C.C.; Butz, M.; Schnitzler, A.; Deuschl, G.; Höft, M. DBS electrode localization and rotational orientation detection using SQUID-based magnetoencephalography. J. Neural Eng. 2021, 18, 026021. [Google Scholar] [CrossRef]
- Yalaz, M.; Deuschl, G.; Butz, M.; Schnitzler, A.; Helmers, A.K.; Höft, M. Investigation of Magnetoelectric Sensor Requirements for Deep Brain Stimulation Electrode Localization and Rotational Orientation Detection. Sensors 2021, 21, 2527. [Google Scholar] [CrossRef]
- Yalaz, M.; Deuschl, G.; Noor, M.S.; Butz, M.; Schnitzler, A.; Helmers, A.K.; Höft, M. Determining the rotational orientation of directional deep brain stimulation electrodes using magnetoencephalography. J. Neural Eng. 2021, 18, 056056. [Google Scholar] [CrossRef] [PubMed]
- Boto, E.; Holmes, N.; Leggett, J.; Roberts, G.; Shah, V.; Meyer, S.; Muñoz, L.; Mullinger, K.; Tierney, T.; Bestmann, S.; et al. Moving magnetoencephalography towards real-world applications with a wearable system. Nature 2018, 555, 657–661. [Google Scholar] [CrossRef] [PubMed]
- Hill, R.M.; Boto, E.; Rea, M.; Holmes, N.; Leggett, J.; Coles, L.A.; Papastavrou, M.; Everton, S.K.; Hunt, B.A.; Sims, D.; et al. Multi-channel whole-head OPM-MEG: Helmet design and a comparison with a conventional system. NeuroImage 2020, 219, 116995. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.M.; Pfeiffer, C.; Ruffieux, S.; Riaz, B.; Winkler, D.; Schneiderman, J.F.; Lundqvist, D. On-scalp MEG SQUIDs are sensitive to early somatosensory activity unseen by conventional MEG. NeuroImage 2020, 221, 117157. [Google Scholar] [CrossRef]
- Juárez-Paz, L.M. In silico Accuracy and Energy Efficiency of Two Steering Paradigms in Directional Deep Brain Stimulation. Front. Neurol. 2020, 11, 1360. [Google Scholar] [CrossRef]
- Pasku, V.; De Angelis, A.; De Angelis, G.; Arumugam, D.D.; Dionigi, M.; Carbone, P.; Moschitta, A.; Ricketts, D.S. Magnetic Field-Based Positioning Systems. IEEE Commun. Surv. Tutor. 2017, 19, 2003–2017. [Google Scholar] [CrossRef]
- Oostenveld, R.; Fries, P.; Maris, E.; Schoffelen, J.M. FieldTrip: Open Source Software for Advanced Analysis of MEG, EEG, and Invasive Electrophysiological Data. Comput. Intell. Neurosci. 2011, 2011, 156869. [Google Scholar] [CrossRef]
- Horn, A.; Kühn, A.A. Lead-DBS: A toolbox for deep brain stimulation electrode localizations and visualizations. NeuroImage 2015, 107, 127–135. [Google Scholar] [CrossRef]
- Horn, A.; Li, N.; Dembek, T.A.; Kappel, A.; Boulay, C.; Ewert, S.; Tietze, A.; Husch, A.; Perera, T.; Neumann, W.J.; et al. Lead-DBS v2: Towards a comprehensive pipeline for deep brain stimulation imaging. NeuroImage 2019, 184, 293–316. [Google Scholar] [CrossRef]
- Mosher, J.C.; Lewis, P.S.; Leahy, R.M. Multiple dipole modeling and localization from spatio-temporal MEG data. IEEE Trans. Biomed. Eng. 1992, 39, 541–557. [Google Scholar] [CrossRef] [PubMed]
- Hellerbach, A.; Dembek, T.A.; Hoevels, M.; Holz, J.A.; Gierich, A.; Luyken, K.; Barbe, M.T.; Wirths, J.; Visser-Vandewalle, V.; Treuer, H. DiODe: Directional Orientation Detection of Segmented Deep Brain Stimulation Leads: A Sequential Algorithm Based on CT Imaging. Stereotact. Funct. Neurosurg. 2018, 96, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Meyer, S.S.; Bonaiuto, J.; Lim, M.; Rossiter, H.; Waters, S.; Bradbury, D.; Bestmann, S.; Brookes, M.; Callaghan, M.F.; Weiskopf, N.; et al. Flexible head-casts for high spatial precision MEG. J. Neurosci. Methods 2017, 276, 38–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koshev, N.; Butorina, A.; Skidchenko, E.; Kuzmichev, A.; Ossadtchi, A.; Ostras, M.; Fedorov, M.; Vetoshko, P. Evolution of MEG: A first MEG-feasible fluxgate magnetometer. Hum. Brain Mapp. 2021, 42, 4844–4856. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Electrode Localization | Electrode Orientation Detection | ||||||
|---|---|---|---|---|---|---|---|
| Vertical Configuration | Diagonal Config. | Horizontal Config. | Symmetrical Config. | ||||
| No. | Contacts: (−) vs. (+) | No. | Contacts: (−) vs. (+) | No. | Contacts: (−) vs. (+) | No. | Contacts: (−) vs. (+) |
| #01 | C1 vs. C234 | #07 | C1 vs. C2 | #13 | C2 vs. C3 | #19 | C23 vs. C4 |
| #02 | C234 vs. C567 | #08 | C1 vs. C3 | #14 | C3 vs. C4 | #20 | C34 vs. C2 |
| #03 | C567 vs. C8 | #09 | C1 vs. C4 | #15 | C4 vs. C2 | #21 | C42 vs. C3 |
| #04 | C1 vs. C567 | #10 | C5 vs. C8 | #16 | C5 vs. C6 | #22 | C56 vs. C7 |
| #05 | C234 vs. C8 | #11 | C6 vs. C8 | #17 | C6 vs. C7 | #23 | C67 vs. C5 |
| #06 | C1 vs. C8 | #12 | C7 vs. C8 | #18 | C7 vs. C5 | #24 | C75 vs. C6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yalaz, M.; Maling, N.; Deuschl, G.; Juárez-Paz, L.M.; Butz, M.; Schnitzler, A.; Helmers, A.-K.; Höft, M. MaDoPO: Magnetic Detection of Positions and Orientations of Segmented Deep Brain Stimulation Electrodes: A Radiation-Free Method Based on Magnetoencephalography. Brain Sci. 2022, 12, 86. https://doi.org/10.3390/brainsci12010086
Yalaz M, Maling N, Deuschl G, Juárez-Paz LM, Butz M, Schnitzler A, Helmers A-K, Höft M. MaDoPO: Magnetic Detection of Positions and Orientations of Segmented Deep Brain Stimulation Electrodes: A Radiation-Free Method Based on Magnetoencephalography. Brain Sciences. 2022; 12(1):86. https://doi.org/10.3390/brainsci12010086
Chicago/Turabian StyleYalaz, Mevlüt, Nicholas Maling, Günther Deuschl, León M. Juárez-Paz, Markus Butz, Alfons Schnitzler, Ann-Kristin Helmers, and Michael Höft. 2022. "MaDoPO: Magnetic Detection of Positions and Orientations of Segmented Deep Brain Stimulation Electrodes: A Radiation-Free Method Based on Magnetoencephalography" Brain Sciences 12, no. 1: 86. https://doi.org/10.3390/brainsci12010086
APA StyleYalaz, M., Maling, N., Deuschl, G., Juárez-Paz, L. M., Butz, M., Schnitzler, A., Helmers, A.-K., & Höft, M. (2022). MaDoPO: Magnetic Detection of Positions and Orientations of Segmented Deep Brain Stimulation Electrodes: A Radiation-Free Method Based on Magnetoencephalography. Brain Sciences, 12(1), 86. https://doi.org/10.3390/brainsci12010086