
Evaluation of Anesthetic Specific EEG Dynamics during State Transitions between Loss and Return of Responsiveness

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Monitoring
2.3. Clinical Protocol
2.4. EEG Recording and CSI Calculation
2.5. CSI and EEG Analysis
2.6. Statistical Analysis
3. Results
3.1. Demographics
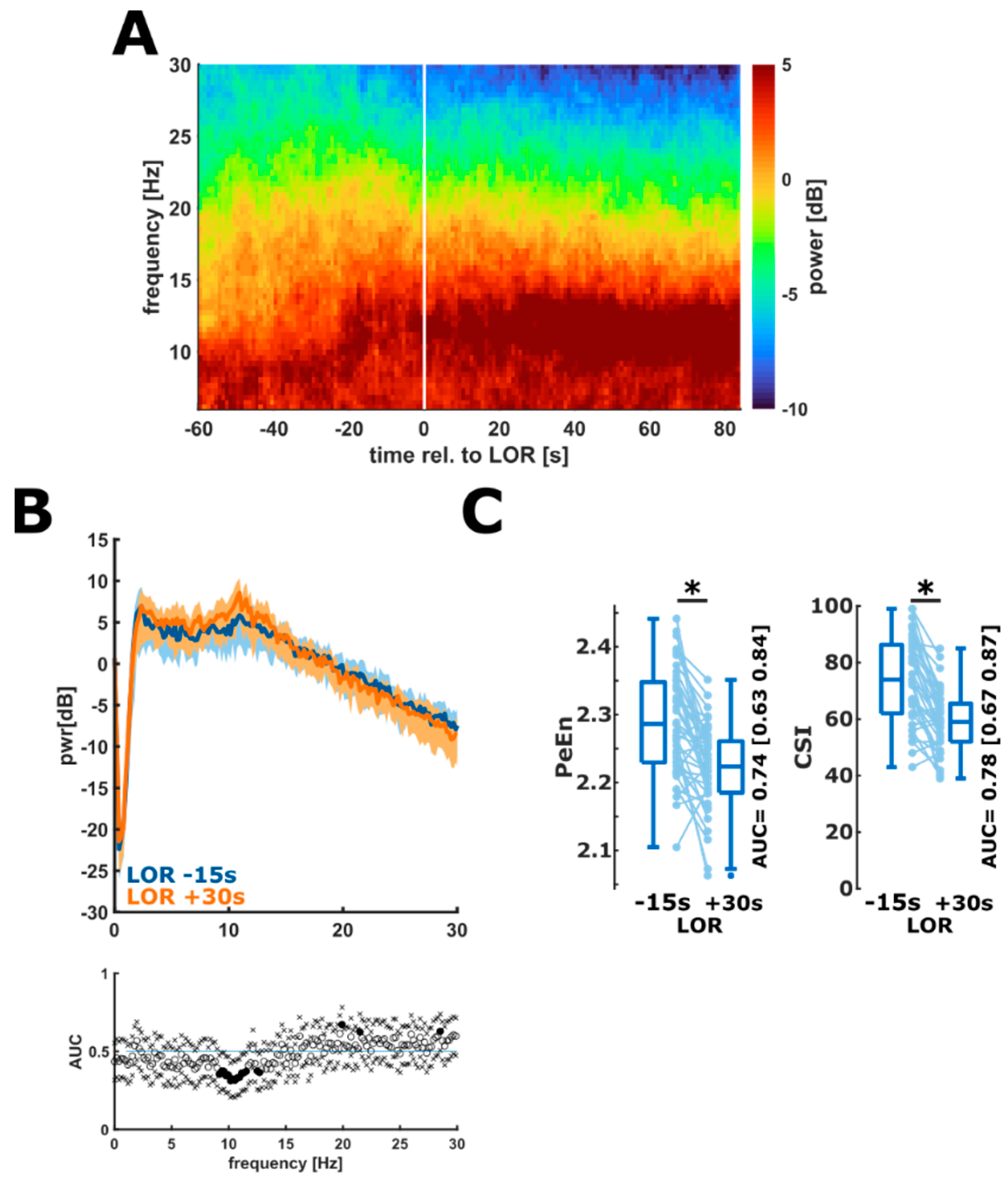
3.2. EEG and Index Features during Propofol-Induced Loss of Responsiveness
3.3. Substance Specific Differences in the EEG and CSI Features during ROR
3.4. Implications of Substance-Specific Differences on Monitoring
4. Discussion
4.1. Impact on EEG-Based Monitoring
4.2. Clinical Implications
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rampil, I.J. A Primer for EEG Signal Processing in Anesthesia. Anesthesiology 1998, 89, 980–1002. [Google Scholar] [CrossRef] [PubMed]
- Drover, D.; Ortega, H.R. Patient state index. Best Pr. Res. Clin. Anaesthesiol. 2006, 20, 121–128. [Google Scholar] [CrossRef]
- Viertio-Oja, H.; Maja, V.; Sarkela, M.; Talja, P.; Tenkanen, N.; Tolvanen-Laakso, H.; Paloheimo, M.; Vakkuri, A.; Yli-Hankala, A.; Merilainen, P. Description of the Entropy algorithm as applied in the Datex-Ohmeda S/5 Entropy Module. Acta Anaesthesiol. Scand. 2004, 48, 154–161. [Google Scholar] [CrossRef]
- Jensen, E.W.; Litvan, H.; Revuelta, M.; Rodriguez, B.E.; Caminal, P.; Martinez, P.; Vereecke, H.; Struys, M. Cerebral State Index during Propofol Anesthesia: A Comparison with the Bispectral Index and the A-Line ARX Index. Anesthesiology 2006, 105, 28–36. [Google Scholar] [CrossRef]
- Hesse, S.; Kreuzer, M.; Hight, D.; Gaskell, A.; Devari, P.; Singh, D.; Taylor, N.; Whalin, M.; Lee, S.; Sleigh, J. Association of electroencephalogram trajectories during emergence from anaesthesia with delirium in the post-anaesthesia care unit: An early sign of postoperative complications. BJA Br. J. Anaesth. 2019, 122, 622–634. [Google Scholar] [CrossRef] [PubMed]
- Fritz, B.A.; Kalarickal, P.L.; Maybrier, H.R.; Muench, M.R.; Dearth, D.; Chen, Y.; Escallier, K.E.; Ben Abdallah, A.; Lin, N.; Avidan, M.S. Intraoperative Electroencephalogram Suppression Predicts Postoperative Delirium. Anesth. Analg. 2016, 122, 234–242. [Google Scholar] [CrossRef]
- Aldecoa, C.; Bettelli, G.; Bilotta, F.; Sanders, R.D.; Audisio, R.; Borozdina, A.; Cherubini, A.; Jones, C.; Kehlet, H.; MacLullich, A. European Society of Anaesthesiology evidence-based and consensus-based guideline on postoperative delirium. Eur. J. Anaesthesiol. 2017, 34, 192–214. [Google Scholar] [CrossRef] [PubMed]
- Pilge, S.; Zanner, R.; Schneider, G.; Blum, J.; Kreuzer, M.; Kochs, E. Time Delay of Index Calculation: Analysis of Cerebral State, Bispectral, and Narcotrend Indices. Anesthesiology 2006, 104, 488–494. [Google Scholar] [CrossRef]
- Zanner, R.; Pilge, S.; Kochs, E.F.; Kreuzer, M.; Schneider, G. Time delay of electroencephalogram index calculation: Analysis of cerebral state, bispectral, and Narcotrend indices using perioperatively recorded electroencephalographic signals. Br. J. Anaesth. 2009, 103, 394–399. [Google Scholar] [CrossRef] [PubMed]
- Akeju, O.; Westover, M.B.; Pavone, K.J.; Sampson, A.L.; Hartnack, K.E.; Brown, E.N.; Purdon, P.L. Effects of sevoflurane and propofol on frontal electroencephalogram power and coherence. Anesthesiology 2014, 121, 990–998. [Google Scholar] [CrossRef]
- Stankovski, T.; Petkoski, S.; Raeder, J.; Smith, A.F.; McClintock, P.V.; Stefanovska, A. Alterations in the coupling functions between cortical and cardio-respiratory oscillations due to anaesthesia with propofol and sevoflurane. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2016, 374, 20150186. [Google Scholar] [CrossRef]
- Purdon, P.L.; Sampson, A.; Pavone, K.J.; Brown, E.N. Clinical Electroencephalography for Anesthesiologists Part I: Background and Basic Signatures. Anesthesiology 2015, 123, 937–960. [Google Scholar] [CrossRef]
- Ni, K.; Cooter, M.; Gupta, D.K.; Thomas, J.; Hopkins, T.J.; Miller, T.E.; James, M.L.; Kertai, M.D.; Berger, M. Paradox of age: Older patients receive higher age-adjusted minimum alveolar concentration fractions of volatile anaesthetics yet display higher bispectral index values. Br. J. Anaesth. 2019, 123, 288–297. [Google Scholar] [CrossRef]
- Kreuzer, M.; Stern, M.A.; Hight, D.; Berger, S.; Schneider, G.; Sleigh, J.W.; García, P.S. Spectral and Entropic Features Are Altered by Age in the Electroencephalogram in Patients under Sevoflurane Anesthesia. Anesthesiology 2020, 132, 1003–1016. [Google Scholar] [CrossRef]
- Purdon, P.; Pavone, K.; Akeju, O.; Smith, A.; Sampson, A.; Lee, J.; Zhou, D.; Solt, K.; Brown, E. The Ageing Brain: Age-dependent changes in the electroencephalogram during propofol and sevoflurane general anaesthesia. Br. J. Anaesth. 2015, 115, i46–i57. [Google Scholar] [CrossRef]
- Schultz, A.; Grouven, U.; Zander, I.; Beger, F.A.; Siedenberg, M.; Schultz, B. Age-related effects in the EEG during propofol anaesthesia. Acta Anaesthesiol. Scand. 2004, 48, 27–34. [Google Scholar] [CrossRef]
- Obert, D.P.; Schweizer, C.; Zinn, S.; Kratzer, S.; Hight, D.; Sleigh, J.; Schneider, G.; García, P.S.; Kreuzer, M. The influence of age on EEG-based anaesthesia indices. J. Clin. Anesth. 2021, 73, 110325. [Google Scholar] [CrossRef]
- Chander, D.; Garcia, P.S.; MacColl, J.N.; Illing, S.; Sleigh, J.W. Electroencephalographic variation during end maintenance and emergence from surgical anesthesia. PLoS ONE 2014, 9, e106291. [Google Scholar] [CrossRef]
- Hight, D.F.; Dadok, V.M.; Szeri, A.J.; García, P.S.; Voss, L.; Sleigh, J.W. Emergence from general anesthesia and the sleep-manifold. Front. Syst. Neurosci. 2014, 8, 146. [Google Scholar] [CrossRef][Green Version]
- Fleischmann, A.; Pilge, S.; Kiel, T.; Kratzer, S.; Schneider, G.; Kreuzer, M. Substance-Specific Differences in Human Electroencephalographic Burst Suppression Patterns. Front. Hum. Neurosci. 2018, 12, 368. [Google Scholar] [CrossRef]
- Bandt, C.; Pompe, B. Permutation Entropy: A Natural Complexity Measure for Time Series. Phys. Rev. Lett. 2002, 88, 174102. [Google Scholar] [CrossRef] [PubMed]
- Tunstall, M.E. Detecting wakefulness during general anaesthesia for caesarean section. Br. Med. J. 1977, 1, 1321. [Google Scholar] [CrossRef]
- Schnider, T.W.; Minto, C.F.; Shafer, S.L.; Gambus, P.L.; Andresen, C.; Goodale, D.B.; Youngs, E.J. The Influence of Age on Propofol Pharmacodynamics. Anesthesiology 1999, 90, 1502–1516. [Google Scholar] [CrossRef]
- Stockmanns, G.; Ningler, M.; Omerovic, A.; Kochs, E.F.; Schneider, G. NeuMonD: A tool for the development of new indicators of anaesthetic effect. Biomed. Tech./Biomed. Eng. 2007, 52, 96–101. [Google Scholar] [CrossRef]
- Berger, S.; Schneider, G.; Kochs, E.F.; Jordan, D. Permutation Entropy: Too Complex a Measure for EEG Time Series? Entropy 2017, 19, 692. [Google Scholar] [CrossRef]
- Jordan, D.; Stockmanns, G.; Kochs, E.F.; Pilge, S.; Schneider, G. Electroencephalographic Order Pattern Analysis for the Separation of Consciousness and Unconsciousness: An Analysis of Approximate Entropy, Permutation Entropy, Recurrence Rate, and Phase Coupling of Order Recurrence Plots. Anesthesiology 2008, 109, 1014–1022. [Google Scholar] [CrossRef]
- Olofsen, E.; Sleigh, J.W.; Dahan, A. Permutation entropy of the electroencephalogram: A measure of anaesthetic drug effect. Br. J. Anaesth. 2008, 101, 810–821. [Google Scholar] [CrossRef]
- Pilge, S.; Blum, J.; Kochs, E.F.; Schoniger, S.A.; Kreuzer, M.; Schneider, G. Does the cerebral state index separate consciousness from unconsciousness? Anesth. Analg. 2011, 113, 1403–1410. [Google Scholar] [CrossRef]
- Schneider, G.; Hollweck, R.; Ningler, M.; Stockmanns, G.; Kochs, E.F. Detection of consciousness by electroencephalogram and auditory evoked potentials. Anesthesiology 2005, 103, 934–943. [Google Scholar] [CrossRef]
- Hentschke, H.; Stüttgen, M.C. Computation of measures of effect size for neuroscience data sets. Eur. J. Neurosci. 2011, 34, 1887–1894. [Google Scholar] [CrossRef]
- Jordan, D.; Steiner, M.; Kochs, E.F.; Schneider, G. A Program for Computing the Prediction Probability and the Related Receiver Operating Characteristic Graph. Anesth. Analg. 2010, 111, 1416–1421. [Google Scholar] [CrossRef] [PubMed]
- Cardillo, G. Dunn’s Test. 2021. Available online: https://github.com/dnafinder/dunn (accessed on 25 November 2021).
- Brown, E.N.; Lydic, R.; Schiff, N.D. General Anesthesia, Sleep, and Coma. N. Engl. J. Med. 2010, 363, 2638–2650. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, N.; Lockhart, S.H.; Eger, E.I., II; Weiskopf, R.B.; Liu, J.; Laster, M.; Taheri, S.; Peterson, N.A. Comparison of kinetics of sevoflurane and isoflurane in humans. Anesth. Analg. 1991, 72, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.S.; Yoon, S.W.; Choi, S.L.; Choi, S.H.; Lee, B.Y.; Jeong, M.A. Comparison of emergence times with different fresh gas flow rates following desflurane anaesthesia. J. Int. Med. Res. 2014, 42, 1285–1293. [Google Scholar] [CrossRef] [PubMed]
- Luppi, A.I.; Spindler, L.R.B.; Menon, D.K.; Stamatakis, E.A. The Inert Brain: Explaining Neural Inertia as Post-anaesthetic Sleep Inertia. Front. Neurosci. 2021, 15, 174. [Google Scholar] [CrossRef] [PubMed]
- Alkire, M.T.; Hudetz, A.G.; Tononi, G. Consciousness and Anesthesia. Science 2008, 322, 876–880. [Google Scholar] [CrossRef]
- Kratzer, S.; Mattusch, C.; Garcia, P.S.; Schmid, S.; Kochs, E.; Rammes, G.; Schneider, G.; Kreuzer, M.; Haseneder, R. Propofol and sevoflurane differentially modulate cortical depolarization following electric stimulation of the ventrobasal thalamus. Front. Comput. Neurosci. 2017, 11, 109. [Google Scholar] [CrossRef] [PubMed]
- Hannivoort, L.N.; Absalom, A.R.; Struys, M. The role of pharmacokinetics and pharmacodynamics in clinical anaesthesia practice. Curr. Opin. Anaesthesiol. 2020, 33, 483–489. [Google Scholar] [CrossRef]
- Raz, A.; Grady, S.M.; Krause, B.M.; Uhlrich, D.J.; Manning, K.A.; Banks, M.I. Preferential effect of isoflurane on top-down vs. bottom-up pathways in sensory cortex. Front. Syst. Neurosci. 2014, 8, 191. [Google Scholar] [CrossRef]
- Kenny, J.D.; Westover, M.B.; Ching, S.; Brown, E.N.; Solt, K. Propofol and sevoflurane induce distinct burst suppression patterns in rats. Front. Syst. Neurosci. 2014, 8, 237. [Google Scholar] [CrossRef]
- Boisseau, N.; Madany, M.; Staccini, P.; Armando, G.; Martin, F.; Grimaud, D.; Raucoules-Aime, M. Comparison of the effects of sevoflurane and propofol on cortical somatosensory evoked potentials. Br. J. Anaesth. 2002, 88, 785–789. [Google Scholar] [CrossRef] [PubMed]
- Vijayan, S.; Ching, S.; Purdon, P.L.; Brown, E.N.; Kopell, N.J. Thalamocortical mechanisms for the anteriorization of alpha rhythms during propofol-induced unconsciousness. J. Neurosci. 2013, 33, 11070–11075. [Google Scholar] [CrossRef] [PubMed]
- Boncompte, G.; Medel, V.; Cortínez, L.I.; Ossandón, T. Brain activity complexity has a non-linear relation to the level of propofol sedation. Br. J. Anaesth. 2021, 127, 254–263. [Google Scholar] [CrossRef] [PubMed]
- Sepúlveda, P.O.; Tapia, L.F.; Monsalves, S. Neural inertia and differences between loss of and recovery from consciousness during total intravenous anaesthesia: A narrative review. Anaesthesia 2019, 74, 801–809. [Google Scholar] [CrossRef]
- Pilge, S.; Blum, J.; Kreuzer, M.; Schneider, G.; Kochs, E. Does the Cerebral State Index differentiate between consciousness and unconsciousness. A prospective patient study. Eur. J. Anaesthesiol. 2006, 23, 28. [Google Scholar] [CrossRef]
- Revuelta, M.; Paniagua, P.; Campos, J.M.; Fernandez, J.A.; Martinez, A.; Jospin, M.; Litvan, H. Validation of the index of consciousness during sevoflurane and remifentanil anaesthesia: A comparison with the bispectral index and the cerebral state index. Br. J. Anaesth. 2008, 101, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Pilge, S.; Kreuzer, M.; Kochs, E.F.; Zanner, R.; Paprotny, S.; Schneider, G. Monitors of the hypnotic component of anesthesia—correlation between bispectral index and cerebral state index. Minerva Anestesiol. 2012, 78, 636–645. [Google Scholar] [PubMed]
- Bonhomme, V.; Hans, P. Muscle relaxation and depth of anaesthesia: Where is the missing link? Br. J. Anaesth. 2007, 99, 456–460. [Google Scholar] [CrossRef]
- Kreuzer, M.; Zanner, R.; Pilge, S.; Paprotny, S.; Kochs, E.F.; Schneider, G. Time delay of monitors of the hypnotic component of anesthesia: Analysis of state entropy and index of consciousness. Anesth. Analg. 2012, 115, 315–319. [Google Scholar] [CrossRef]
- Hayashi, K.; Sawa, T. The fundamental contribution of the electromyogram to a high bispectral index: A postoperative observational study. J. Clin. Monit. Comput. 2019, 33, 1097–1103. [Google Scholar] [CrossRef]
- Kamata, K.; Aho, A.; Hagihira, S.; Yli-Hankala, A.; Jäntti, V. Frequency band of EMG in anaesthesia monitoring. Br. J. Anaesth. 2011, 107, 822–823. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.H.; Min, K.T.; Lee, J.R.; Choi, K.W.; Han, K.H.; Kim, E.H.; Oh, H.J.; Lee, J.H. Determination of EC95 of remifentanil for smooth emergence from propofol anesthesia in patients undergoing transsphenoidal surgery. J. Neurosurg. Anesthesiol. 2015, 27, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Schwender, D.; Daunderer, M.; Klasing, S.; Finsterer, U.; Peter, K. Power spectral analysis of the electroencephalogram during increasing end-expiratory concentrations of isoflurane, desflurane and sevoflurane. Anaesthesia 1998, 53, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Mhuircheartaigh, R.N.; Warnaby, C.; Rogers, R.; Jbabdi, S.; Tracey, I. Slow-wave activity saturation and thalamocortical isolation during propofol anesthesia in humans. Sci. Transl. Med. 2013, 5, ra148–ra208. [Google Scholar] [CrossRef] [PubMed]
- Lysakowski, C.; Dumont, L.; Pellégrini, M.; Clergue, F.; Tassonyi, E. Effects of fentanyl, alfentanil, remifentanil and sufentanil on loss of consciousness and bispectral index during propofol induction of anaesthesia. BJA Br. J. Anaesth. 2001, 86, 523–527. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Propofol Group n = 15 | Sevoflurane Group n = 15 | Isoflurane Group n = 15 | p-Value | |
|---|---|---|---|---|
| Age (y) | 57 (45 67) | 43 (38.5 63.5) | 40 (33 46.5) | * p = 0.1008 |
| Size (cm) | 168 (161 178.5) | 173 (167 179) | 180 (173 185.5) | * p = 0.1059 |
| Weight (kg) | 71 (68 77) | 75 (69.5 79.5) | 90 (81 100) | * p = 0.0021 |
| BMI | 25.4 (23.2 31.2) | 25.8 (23.8 36.6) | 28.4 (25.8 34.1) | * p = 0.1474 |
| LOC to ROC (min) | 107 (89 115) | 109 (93 182) | 129 (103 142) | * p = 0.221 |
| Sufentanil (µg) | n/a | 25.0 (20.0 37.5) | 30.0 (27.5 40.0) | † p = 0.391 |
| Remifentanil (µg) | 992 (867 1408) | |||
| Gender (m/f) | 7/8 | 9/6 | 11/4 | §p = 0.3296 |
| ASA (I/II) | 10/5 | 8/7 | 10/5 | §p = 0.6839 |
| −15 s | +30 s | p-Value | Hedge’s g | AUC | |
|---|---|---|---|---|---|
| LOR: CSI | 74 [62 86] | 59 [52 65] | p < 0.001 | 1.13 [0.85 1.51] | 0.78 [0.67 0.87] |
| LOR: PeEn | 2.29 [2.23 2.35] | 2.22 [2.19 2.16] | p < 0.001 | 0.94 [0.65 1.8] | 0.74 [0.63 0.84] |
| ROR-isoflurane: CSI | 88 (48 to 93) | 87 (81 to 96) | 0.234 | n.s. | 0.50 [0.28 0.74] |
| ROR-sevoflurane: CSI | 87 (49 to 97) | 88 (59 to 96) | 0.445 | n.s. | 0.59 [0.36 0.81] |
| ROR-propofol: CSI | 85.5 (41 to 99) | 87 (78 to 100) | 0.023 | −0.71 [−1.20 −0.33] | 0.63 [0.17 0.58] |
| ROR-isoflurane: PeEn | 2.36 [2.33 2.43] | 2.41 [2.39 2.44] | 0.057 | 0.52 [−1.22 −0.03] | 0.63 [0.40 0.85] |
| ROR-sevoflurane: PeEn | 2.43 [2.25 2.48] | 2.43 [2.41 2.46] | 0.216 | n.s. | 0.56 [0.32 0.78] |
| ROR-propofol: PeEn | 2.40 [2.28 2.44] | 2.44 [2.39 2.48] | 0.058 | −0.68 [−1.32 −0.17] | 0.68 [0.44 0.85] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kreuzer, M.; Kiel, T.; Ernst, L.; Lipp, M.; Schneider, G.; Pilge, S. Evaluation of Anesthetic Specific EEG Dynamics during State Transitions between Loss and Return of Responsiveness. Brain Sci. 2022, 12, 37. https://doi.org/10.3390/brainsci12010037
Kreuzer M, Kiel T, Ernst L, Lipp M, Schneider G, Pilge S. Evaluation of Anesthetic Specific EEG Dynamics during State Transitions between Loss and Return of Responsiveness. Brain Sciences. 2022; 12(1):37. https://doi.org/10.3390/brainsci12010037
Chicago/Turabian StyleKreuzer, Matthias, Tobias Kiel, Leonie Ernst, Marlene Lipp, Gerhard Schneider, and Stefanie Pilge. 2022. "Evaluation of Anesthetic Specific EEG Dynamics during State Transitions between Loss and Return of Responsiveness" Brain Sciences 12, no. 1: 37. https://doi.org/10.3390/brainsci12010037
APA StyleKreuzer, M., Kiel, T., Ernst, L., Lipp, M., Schneider, G., & Pilge, S. (2022). Evaluation of Anesthetic Specific EEG Dynamics during State Transitions between Loss and Return of Responsiveness. Brain Sciences, 12(1), 37. https://doi.org/10.3390/brainsci12010037