
Corticolimbic Modulation via Intermittent Theta Burst Stimulation as a Novel Treatment for Functional Movement Disorder: A Proof-of-Concept Study

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
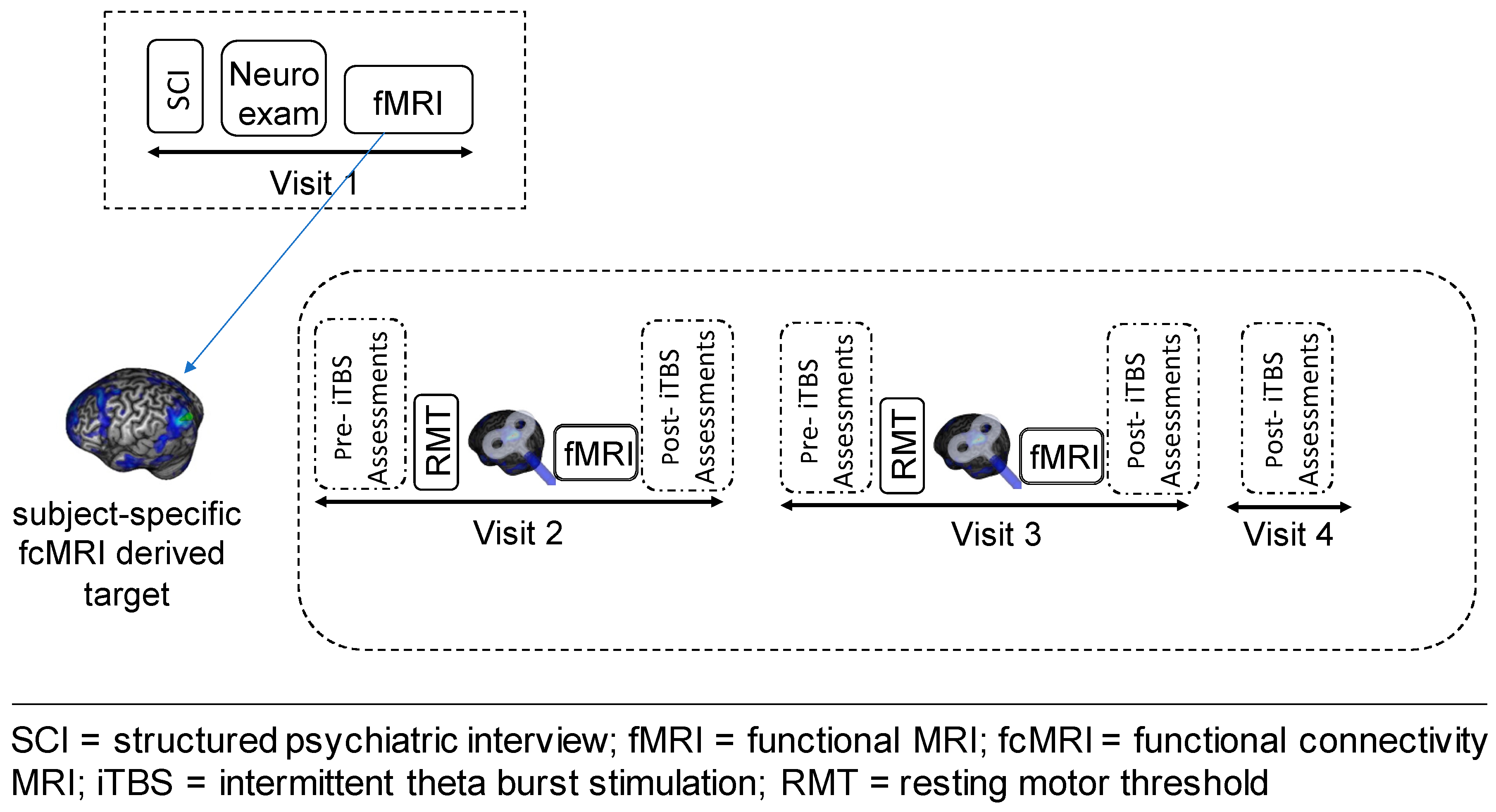
2.2. Study Design
2.3. TMS and iTBS Procedures
2.4. Image Acquisition
2.5. fMRI Task and Stimuli
2.6. Imaging Processing and Data Analysis
2.7. Statistical Analysis
3. Results
3.1. Safety and Tolerability
3.2. Functional MRI
3.3. Valence and Arousal Levels
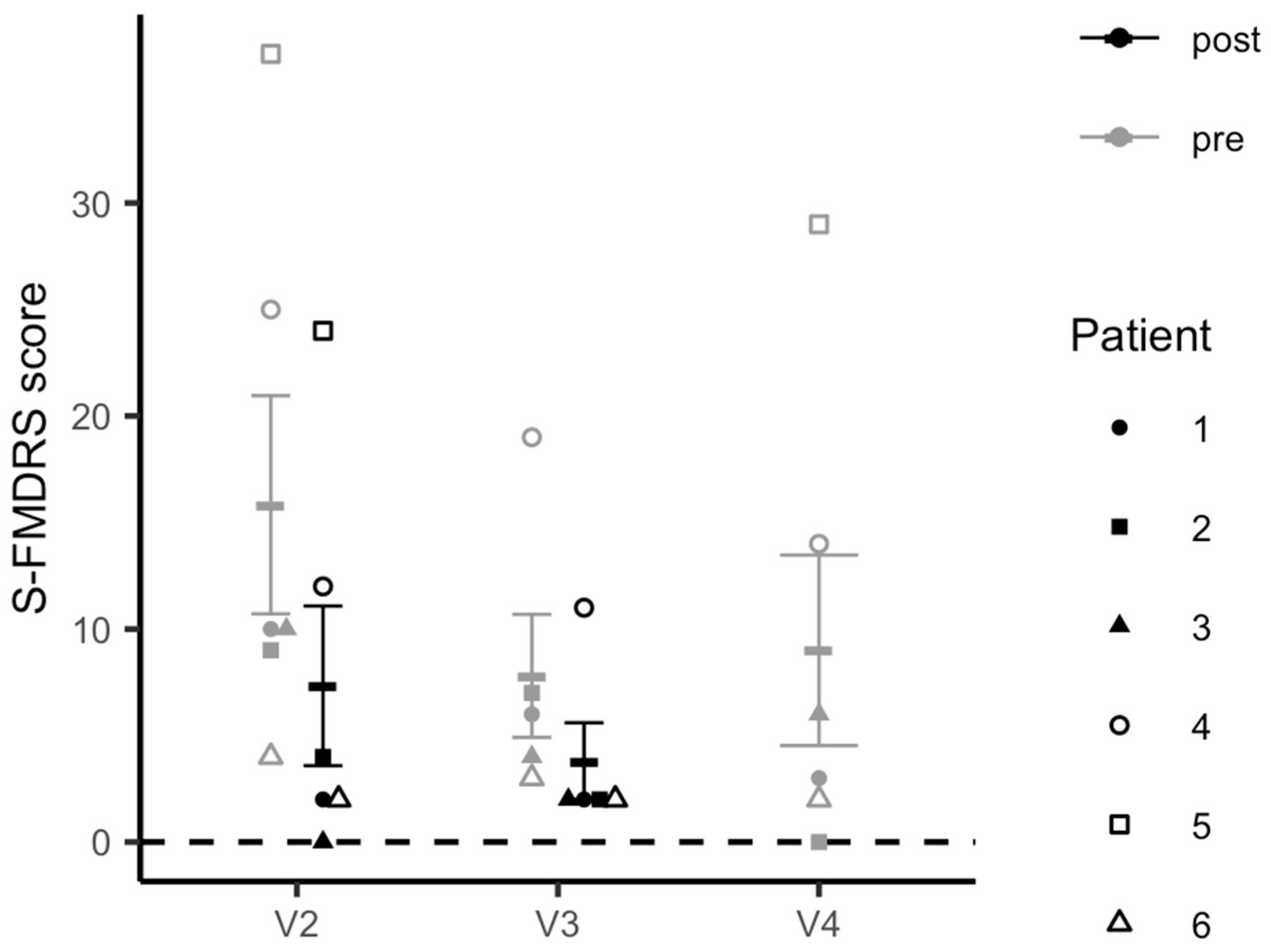
3.4. Simplified-Functional Movement Disorder Rating Scale Scores
3.5. Correlations between Imaging Data and FMD Symptom Severity
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Exclusion/Inclusion Criteria
Appendix A.2. Visit 1–Clinical and Behavioral Assessments
Appendix A.3. Arousal and Valence Rating Procedures
Appendix A.4. MRI Procedures
Appendix A.5. Intermittent TBS Procedures
References
- Stone, J.; Carson, A.; Duncan, R.; Roberts, R.; Warlow, C.; Hibberd, C.; Coleman, R.; Cull, R.; Murray, G.; Pelosi, A.; et al. Who Is Referred to Neurology Clinics?—The Diagnoses Made in 3781 New Patients. Clin. Neurol. Neurosurg. 2010, 112, 747–751. [Google Scholar] [CrossRef]
- Espay, A.J.; Aybek, S.; Carson, A.; Edwards, M.J.; Goldstein, L.H.; Hallett, M.; LaFaver, K.; LaFrance, W.C.; Lang, A.E.; Nicholson, T.; et al. Current Concepts in Diagnosis and Treatment of Functional Neurological Disorders. JAMA Neurol. 2018, 75, 1132–1141. [Google Scholar] [CrossRef]
- Drane, D.L.; Fani, N.; Hallett, M.; Khalsa, S.S.; Perez, D.L.; Roberts, N.A. A Framework for Understanding the Pathophysiology of Functional Neurological Disorder. CNS Spectr. 2020, 1–7. [Google Scholar] [CrossRef]
- Voon, V.; Cavanna, A.E.; Coburn, K.; Sampson, S.; Reeve, A.; LaFrance, W.C. Functional Neuroanatomy and Neurophysiology of Functional Neurological Disorders (Conversion Disorder). J. Neuropsychiatry Clin. Neurosci. 2016, 28, 168–190. [Google Scholar] [CrossRef]
- Perez, D.L.; Dworetzky, B.A.; Dickerson, B.C.; Leung, L.; Cohn, R.; Baslet, G.; Silbersweig, D.A. An Integrative Neurocircuit Perspective on Psychogenic Nonepileptic Seizures and Functional Movement Disorders: Neural Functional Unawareness. Clin. EEG Neurosci. 2015, 46, 4–15. [Google Scholar] [CrossRef]
- Demartini, B.; Nisticò, V.; Edwards, M.J.; Gambini, O.; Priori, A. The Pathophysiology of Functional Movement Disorders. Neurosci. Biobehav. Rev. 2020, 120, 387–400. [Google Scholar] [CrossRef]
- Pick, S.; Goldstein, L.H.; Perez, D.L.; Nicholson, T.R. Emotional Processing in Functional Neurological Disorder: A Review, Biopsychosocial Model and Research Agenda. J. Neurol. Neurosurg. Psychiatry 2019, 90, 704–711. [Google Scholar] [CrossRef] [PubMed]
- Morris, L.S.; To, B.; Baek, K.; Chang-Webb, Y.-C.; Mitchell, S.; Strelchuk, D.; Mikheenko, Y.; Phillips, W.; Zandi, M.; Jenaway, A.; et al. Disrupted Avoidance Learning in Functional Neurological Disorder: Implications for Harm Avoidance Theories. NeuroImage Clin. 2017, 16, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Voon, V.; Brezing, C.; Gallea, C.; Ameli, R.; Roelofs, K.; LaFrance, W.C.; Hallett, M. Emotional Stimuli and Motor Conversion Disorder. Brain 2010, 133, 1526–1536. [Google Scholar] [CrossRef] [PubMed]
- Aybek, S.; Nicholson, T.R.; O’Daly, O.; Zelaya, F.; Kanaan, R.A.; David, A.S. Emotion-Motion Interactions in Conversion Disorder: An FMRI Study. PLoS ONE 2015, 10, e0123273. [Google Scholar] [CrossRef] [PubMed]
- Faul, L.; Knight, L.; Espay, A.; Depue, B.; LaFaver, K. Neural Activity in Functional Movement Disorders after Inpatient Rehabilitation. Psychiatry Res. Neuroimaging 2020, 303, 111125. [Google Scholar] [CrossRef]
- Espay, A.J.; Ries, S.; Maloney, T.; Vannest, J.; Neefus, E.; Dwivedi, A.K.; Allendorfer, J.B.; Wulsin, L.R.; LaFrance, W.C.; Lang, A.E.; et al. Clinical and Neural Responses to Cognitive Behavioral Therapy for Functional Tremor. Neurology 2019, 93, e1787. [Google Scholar] [CrossRef]
- Hallett, M. Transcranial Magnetic Stimulation and the Human Brain. Nature 2000, 406, 147–150. [Google Scholar] [CrossRef]
- Lantrip, C.; Gunning, F.M.; Flashman, L.; Roth, R.M.; Holtzheimer, P.E. Effects of Transcranial Magnetic Stimulation on the Cognitive Control of Emotion: Potential Antidepressant Mechanisms. J. ECT 2017, 33, 73–80. [Google Scholar] [CrossRef]
- Gersner, R.; Kravetz, E.; Feil, J.; Pell, G.; Zangen, A. Long-Term Effects of Repetitive Transcranial Magnetic Stimulation on Markers for Neuroplasticity: Differential Outcomes in Anesthetized and Awake Animals. J. Neurosci. Off. J. Soc. Neurosci. 2011, 31, 7521–7526. [Google Scholar] [CrossRef] [PubMed]
- Taib, S.; Ory-Magne, F.; Brefel-Courbon, C.; Moreau, Y.; Thalamas, C.; Arbus, C.; Simonetta-Moreau, M. Repetitive Transcranial Magnetic Stimulation for Functional Tremor: A Randomized, Double-Blind, Controlled Study. Mov. Disord. Off. J. Mov. Disord. Soc. 2019, 34, 1210–1219. [Google Scholar] [CrossRef] [PubMed]
- Garcin, B.; Mesrati, F.; Hubsch, C.; Mauras, T.; Iliescu, I.; Naccache, L.; Vidailhet, M.; Roze, E.; Degos, B. Impact of Transcranial Magnetic Stimulation on Functional Movement Disorders: Cortical Modulation or a Behavioral Effect? Front. Neurol. 2017, 8, 338. [Google Scholar] [CrossRef] [PubMed]
- Shah, B.B.; Chen, R.; Zurowski, M.; Kalia, L.V.; Gunraj, C.; Lang, A.E. Repetitive Transcranial Magnetic Stimulation plus Standardized Suggestion of Benefit for Functional Movement Disorders: An Open Label Case Series. Parkinsonism Relat. Disord. 2015, 21, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Pollak, T.A.; Nicholson, T.R.; Edwards, M.J.; David, A.S. A Systematic Review of Transcranial Magnetic Stimulation in the Treatment of Functional (Conversion) Neurological Symptoms. J. Neurol. Neurosurg. Psychiatry 2014, 85, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Dumitru, A.; Rocchi, L.; Saini, F.; Rothwell, J.C.; Roiser, J.P.; David, A.S.; Richieri, R.M.; Lewis, G.; Lewis, G. Influence of Theta-Burst Transcranial Magnetic Stimulation over the Dorsolateral Prefrontal Cortex on Emotion Processing in Healthy Volunteers. Cogn. Affect. Behav. Neurosci. 2020, 20, 1278–1293. [Google Scholar] [CrossRef] [PubMed]
- Ironside, M.; Browning, M.; Ansari, T.L.; Harvey, C.J.; Sekyi-Djan, M.N.; Bishop, S.J.; Harmer, C.J.; O’Shea, J. Effect of Prefrontal Cortex Stimulation on Regulation of Amygdala Response to Threat in Individuals with Trait Anxiety: A Randomized Clinical Trial. JAMA Psychiatry 2019, 76, 71–78. [Google Scholar] [CrossRef]
- Balconi, M.; Ferrari, C. Emotional Memory Retrieval. RTMS Stimulation on Left DLPFC Increases the Positive Memories. Brain Imaging Behav. 2012, 6, 454–461. [Google Scholar] [CrossRef] [PubMed]
- De Raedt, R.; Leyman, L.; Baeken, C.; Van Schuerbeek, P.; Luypaert, R.; Vanderhasselt, M.-A.; Dannlowski, U. Neurocognitive Effects of HF-RTMS over the Dorsolateral Prefrontal Cortex on the Attentional Processing of Emotional Information in Healthy Women: An Event-Related FMRI Study. Biol. Psychol. 2010, 85, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Vanderhasselt, M.-A.; De Raedt, R.; Leyman, L.; Baeken, C. Acute Effects of Repetitive Transcranial Magnetic Stimulation on Attentional Control Are Related to Antidepressant Outcomes. J. Psychiatry Neurosci. 2009, 34, 119–126. [Google Scholar] [PubMed]
- Singh, A.; Erwin-Grabner, T.; Sutcliffe, G.; Paulus, W.; Dechent, P.; Antal, A.; Goya-Maldonado, R. Default Mode Network Alterations after Intermittent Theta Burst Stimulation in Healthy Subjects. Transl. Psychiatry 2020, 10, 75. [Google Scholar] [CrossRef] [PubMed]
- Iwabuchi, S.J.; Raschke, F.; Auer, D.P.; Liddle, P.F.; Lankappa, S.T.; Palaniyappan, L. Targeted Transcranial Theta-Burst Stimulation Alters Fronto-Insular Network and Prefrontal GABA. NeuroImage 2017, 146, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Liston, C.; Chen, A.C.; Zebley, B.D.; Drysdale, A.T.; Gordon, R.; Leuchter, B.; Voss, H.U.; Casey, B.J.; Etkin, A.; Dubin, M.J. Default Mode Network Mechanisms of Transcranial Magnetic Stimulation in Depression. Biol. Psychiatry 2014, 76, 517–526. [Google Scholar] [CrossRef]
- Dunlop, K.; Woodside, B.; Olmsted, M.; Colton, P.; Giacobbe, P.; Downar, J. Reductions in Cortico-Striatal Hyperconnectivity Accompany Successful Treatment of Obsessive-Compulsive Disorder with Dorsomedial Prefrontal RTMS. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2016, 41, 1395–1403. [Google Scholar] [CrossRef]
- Williams, D.T.; Ford, B.; Fahn, S. Phenomenology and Psychopathology Related to Psychogenic Movement Disorders. Adv. Neurol. 1995, 65, 231–257. [Google Scholar]
- Lefaucheur, J.-P.; André-Obadia, N.; Antal, A.; Ayache, S.S.; Baeken, C.; Benninger, D.H.; Cantello, R.M.; Cincotta, M.; de Carvalho, M.; De Ridder, D.; et al. Evidence-Based Guidelines on the Therapeutic Use of Repetitive Transcranial Magnetic Stimulation (RTMS). Clin. Neurophysiol. Off. J. Int. Fed. Clin. Neurophysiol. 2014, 125, 2150–2206. [Google Scholar] [CrossRef] [PubMed]
- Rossi, S.; Hallett, M.; Rossini, P.M.; Pascual-Leone, A. Safety of TMS Consensus Group Safety, Ethical Considerations, and Application Guidelines for the Use of Transcranial Magnetic Stimulation in Clinical Practice and Research. Clin. Neurophysiol. Off. J. Int. Fed. Clin. Neurophysiol. 2009, 120, 2008–2039. [Google Scholar] [CrossRef]
- First, M.; Spitzer, R.; Gibbon, M.; Williams, J. Structured Clinical Interview for DSM-IV-TR Axis I Disorders, Research Version, Patient Edition (SCID-I/P); NYBiometrics Research, New York State Psychiatric Institute: New York, NY, USA, 2002. [Google Scholar]
- Bradley, M.M.; Lang, P.J. Measuring Emotion: The Self-Assessment Manikin and the Semantic Differential. J. Behav. Ther. Exp. Psychiatry 1994, 25, 49–59. [Google Scholar] [CrossRef]
- Nielsen, G.; Ricciardi, L.; Meppelink, A.M.; Holt, K.; Teodoro, T.; Edwards, M. A Simplified Version of the Psychogenic Movement Disorders Rating Scale: The Simplified Functional Movement Disorders Rating Scale (S-FMDRS). Mov. Disord. Clin. Pract. 2017, 4, 710–716. [Google Scholar] [CrossRef]
- Tran, V. Positive Affect Negative Affect Scale (PANAS). In Encyclopedia of Behavioral Medicine; Gellman, M.D., Turner, J.R., Eds.; Springer: New York, NY, USA, 2013; pp. 1508–1509. ISBN 978-1-4419-1005-9. [Google Scholar]
- Young, R.C.; Biggs, J.T.; Ziegler, V.E.; Meyer, D.A. A Rating Scale for Mania: Reliability, Validity and Sensitivity. Br. J. Psychiatry J. Ment. Sci. 1978, 133, 429–435. [Google Scholar] [CrossRef]
- Awiszus, F. TMS and Threshold Hunting. Suppl. Clin. Neurophysiol. 2003, 56, 13–23. [Google Scholar] [CrossRef]
- Tse, N.Y.; Goldsworthy, M.R.; Ridding, M.C.; Coxon, J.P.; Fitzgerald, P.B.; Fornito, A.; Rogasch, N.C. The Effect of Stimulation Interval on Plasticity Following Repeated Blocks of Intermittent Theta Burst Stimulation. Sci. Rep. 2018, 8, 8526. [Google Scholar] [CrossRef]
- Fox, M.D.; Buckner, R.L.; White, M.P.; Greicius, M.D.; Pascual-Leone, A. Efficacy of Transcranial Magnetic Stimulation Targets for Depression Is Related to Intrinsic Functional Connectivity with the Subgenual Cingulate. Biol. Psychiatry 2012, 72, 595–603. [Google Scholar] [CrossRef]
- Cox, R.W. AFNI: Software for Analysis and Visualization of Functional Magnetic Resonance Neuroimages. Comput. Biomed. Res. Int. J. 1996, 29, 162–173. [Google Scholar] [CrossRef]
- Amunts, K.; Kedo, O.; Kindler, M.; Pieperhoff, P.; Mohlberg, H.; Shah, N.J.; Habel, U.; Schneider, F.; Zilles, K. Cytoarchitectonic Mapping of the Human Amygdala, Hippocampal Region and Entorhinal Cortex: Intersubject Variability and Probability Maps. Anat. Embryol. 2005, 210, 343–352. [Google Scholar] [CrossRef]
- To, W.T.; De Ridder, D.; Hart, J.; Vanneste, S. Changing Brain Networks Through Non-Invasive Neuromodulation. Front. Hum. Neurosci. 2018, 12, 128. [Google Scholar] [CrossRef] [PubMed]
- Beynel, L.; Campbell, E.; Naclerio, M.; Galla, J.T.; Ghosal, A.; Michael, A.M.; Kimbrel, N.A.; Davis, S.W.; Appelbaum, L.G. The Effects of Functionally Guided, Connectivity-Based RTMS on Amygdala Activation. Brain Sci. 2021, 11, 494. [Google Scholar] [CrossRef]
- Baas, D.; Aleman, A.; Kahn, R.S. Lateralization of Amygdala Activation: A Systematic Review of Functional Neuroimaging Studies. Brain Res. Brain Res. Rev. 2004, 45, 96–103. [Google Scholar] [CrossRef]
- Stujenske, J.M.; Likhtik, E. Fear from the Bottom Up. Nat. Neurosci. 2017, 20, 765–767. [Google Scholar] [CrossRef]
- Blakemore, R.L.; Sinanaj, I.; Galli, S.; Aybek, S.; Vuilleumier, P. Aversive Stimuli Exacerbate Defensive Motor Behaviour in Motor Conversion Disorder. Neuropsychologia 2016, 93, 229–241. [Google Scholar] [CrossRef]
- Balderston, N.L.; Beydler, E.M.; Roberts, C.; Deng, Z.-D.; Radman, T.; Lago, T.; Luber, B.; Lisanby, S.H.; Ernst, M.; Grillon, C. Mechanistic Link between Right Prefrontal Cortical Activity and Anxious Arousal Revealed Using Transcranial Magnetic Stimulation in Healthy Subjects. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2020, 45, 694–702. [Google Scholar] [CrossRef] [PubMed]
- Philip, N.S.; Barredo, J.; van ’t Wout-Frank, M.; Tyrka, A.R.; Price, L.H.; Carpenter, L.L. Network Mechanisms of Clinical Response to Transcranial Magnetic Stimulation in Posttraumatic Stress Disorder and Major Depressive Disorder. Biol. Psychiatry 2018, 83, 263–272. [Google Scholar] [CrossRef]
- Moreno-Ortega, M.; Kangarlu, A.; Lee, S.; Perera, T.; Kangarlu, J.; Palomo, T.; Glasser, M.F.; Javitt, D.C. Parcel-Guided RTMS for Depression. Transl. Psychiatry 2020, 10, 283. [Google Scholar] [CrossRef]
- Hamilton, M. The Assessment of Anxiety States by Rating. Br. J. Med. Psychol. 1959, 32, 50–55. [Google Scholar] [CrossRef]
- Gonzalez, J.S.; Shreck, E.; Batchelder, A. Hamilton Rating Scale for Depression (HAM-D). In Encyclopedia of Behavioral Medicine; Gellman, M.D., Turner, J.R., Eds.; Springer: New York, NY, USA, 2013; pp. 887–888. ISBN 978-1-4419-1005-9. [Google Scholar]
- McNair, D.M.; Lorr, M.; Droppleman, L.F. Educational and Industrial Testing Service. In Profile of Mood States; Educational and Industrial Testing Service: San Diego, CA, USA, 1971. [Google Scholar]
- Posner, K.; Brown, G.K.; Stanley, B.; Brent, D.A.; Yershova, K.V.; Oquendo, M.A.; Currier, G.W.; Melvin, G.A.; Greenhill, L.; Shen, S.; et al. The Columbia-Suicide Severity Rating Scale: Initial Validity and Internal Consistency Findings from Three Multisite Studies with Adolescents and Adults. Am. J. Psychiatry 2011, 168, 1266–1277. [Google Scholar] [CrossRef] [PubMed]
- Derogatis, L.R.; Unger, R. Symptom Checklist-90-Revised. In The Corsini Encyclopedia of Psychology; American Cancer Society: Atlanta, GA, USA, 2010; pp. 1–2. ISBN 978-0-470-47921-6. [Google Scholar]
- Bernstein, D.P.; Fink, L.; Handelsman, L.; Foote, J.; Lovejoy, M.; Wenzel, K.; Sapareto, E.; Ruggiero, J. Initial Reliability and Validity of a New Retrospective Measure of Child Abuse and Neglect. Am. J. Psychiatry 1994, 151, 1132–1136. [Google Scholar] [CrossRef] [PubMed]
- Kubany, E.S.; Leisen, M.B.; Kaplan, A.S.; Watson, S.B.; Haynes, S.N.; Owens, J.A.; Burns, K. Development and Preliminary Validation of a Brief Broad-Spectrum Measure of Trauma Exposure: The Traumatic Life Events Questionnaire. Psychol. Assess. 2000, 12, 210–224. [Google Scholar] [CrossRef] [PubMed]
- Lundqvist, D.; Flykt, A.; Öhman, A. The Karolinska Directed Emotional Faces—KDEF, CD ROM from Department of Clinical Neuroscience, Psychology Section; Karolinska Institute: Solnavagen, Sweden, 1998. [Google Scholar]
- Shirer, W.R.; Ryali, S.; Rykhlevskaia, E.; Menon, V.; Greicius, M.D. Decoding Subject-Driven Cognitive States with Whole-Brain Connectivity Patterns. Cereb. Cortex 2012, 22, 158–165. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spagnolo, P.A.; Parker, J.; Horovitz, S.; Hallett, M. Corticolimbic Modulation via Intermittent Theta Burst Stimulation as a Novel Treatment for Functional Movement Disorder: A Proof-of-Concept Study. Brain Sci. 2021, 11, 791. https://doi.org/10.3390/brainsci11060791
Spagnolo PA, Parker J, Horovitz S, Hallett M. Corticolimbic Modulation via Intermittent Theta Burst Stimulation as a Novel Treatment for Functional Movement Disorder: A Proof-of-Concept Study. Brain Sciences. 2021; 11(6):791. https://doi.org/10.3390/brainsci11060791
Chicago/Turabian StyleSpagnolo, Primavera A., Jacob Parker, Silvina Horovitz, and Mark Hallett. 2021. "Corticolimbic Modulation via Intermittent Theta Burst Stimulation as a Novel Treatment for Functional Movement Disorder: A Proof-of-Concept Study" Brain Sciences 11, no. 6: 791. https://doi.org/10.3390/brainsci11060791
APA StyleSpagnolo, P. A., Parker, J., Horovitz, S., & Hallett, M. (2021). Corticolimbic Modulation via Intermittent Theta Burst Stimulation as a Novel Treatment for Functional Movement Disorder: A Proof-of-Concept Study. Brain Sciences, 11(6), 791. https://doi.org/10.3390/brainsci11060791