
The Quality of Life in Patients with Epilepsy in the Context of Sleep Problems and Sexual Satisfaction

 , , and
, , and
Abstract
1. Introduction
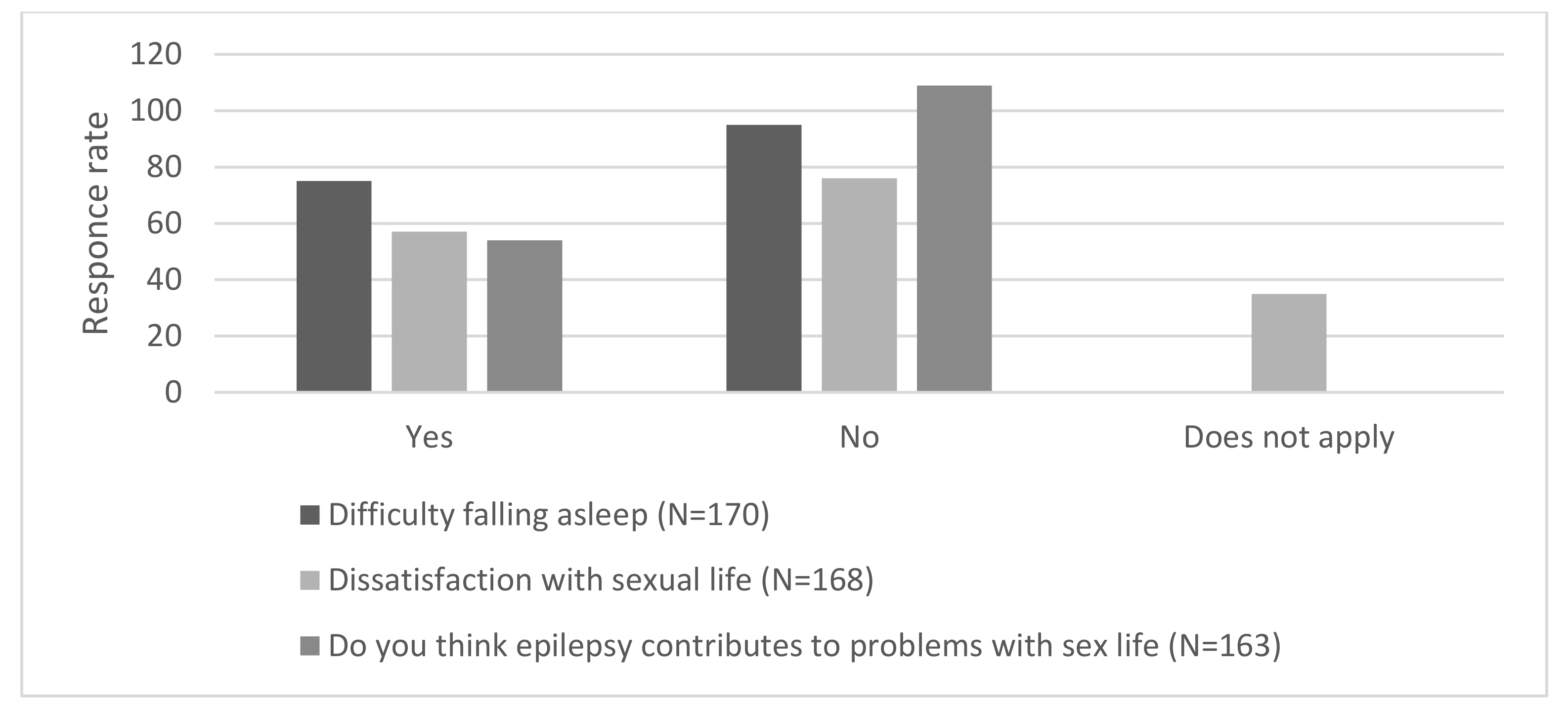
- Do the respondents report problems with sleep initiation?
- Are the respondents satisfied with their sex life?
- Do the respondents think that epilepsy contributes to problems with their sex life?
- What is the correlation between the declared answers (questions 1–3) concerning selected aspects of sexual function and sleep?
- Does the assessment of the quality of life of patients differ between the following groups: those who declare satisfaction vs. no satisfaction with their sex life; those who consider epilepsy to be the cause of sex life problems vs. those who express the opposite opinion; and those who declare sleep initiation problems vs. no sleep initiation problems?
2. Materials and Methods
2.1. Material
2.2. Method
2.2.1. QOLIE-31 Questionnaire
2.2.2. The Authors’ Own Questionnaire
- (1)
- Are you satisfied with your sex life?
- (2)
- Do you have problems with falling asleep?
- (3)
- Do you think epilepsy contributes to problems with sex life?
2.3. Statistics
- -
- Responses not satisfied vs. satisfied with sexual life: Those selected on the scale from “often” to “always” were treated as positive (YES), while those from “rarely” to “never” were negative (NO).
- -
- Respondents having vs. not having problems with sleep initiation: Responses selected on the scale from “sometimes” to “always” were treated as positive (YES), while those from “rarely” to “never” were negative (NO).
- -
- Respondents declaring that epilepsy was vs. was not the cause of difficulties in their sex life: Responses selected on the scale from “rarely” to “always” were treated as positive (YES), while those from “very rarely” to “never” were negative (NO).
3. Results
3.1. Sociodemographic Data
3.2. Medical History Data
3.3. The Frequency of Sleep Initiation Problems
3.4. Satisfaction with Sex Life
3.5. The Quality of Life in the Context of the Quality of Sleep and Sex Life
4. Discussion
4.1. Limitations of the Study
4.2. Strengths of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Hand, C. Measuring health-related quality of life in adults with chronic conditions in primary care settings: Critical review of concepts and 3 tools. Can. Fam. Physician 2016, 62, 375–383. [Google Scholar]
- Røysamb, E.; Nes, R.B.; Czajkowski, N.O.; Vassend, O. Genetics, personality and wellbeing. A twin study of traits, facets and life satisfaction. Sci. Rep. 2018, 8, 12298. [Google Scholar] [CrossRef]
- Etxeberria, I.; Urdaneta, E.; Galdona, N. Factors associated with health-related quality of life (HRQoL): Differential patterns depending on age. Qual. Life Res. 2019, 28, 2221–2231. [Google Scholar] [CrossRef] [PubMed]
- De Weerd, A.; de Haas, S.; Otte, A.; Trenite, D.K.-N.; van Erp, G.; Cohen, A.; de Kam, M.; van Gerven, J. Subjective sleep disturbance in patients with partial epilepsy: A questionnaire-based study on prevalence and impact on quality of life. Epilepsia 2004, 45, 1397–1404. [Google Scholar] [CrossRef] [PubMed]
- Peterson, C.L.; Walker, C.; Coleman, H.; Shears, G. Reported service needs at diagnosis of epilepsy and implications for quality of life. Epilepsy Behav. 2019, 100, 106527. [Google Scholar] [CrossRef] [PubMed]
- Tombini, M.; Assenza, G.; Quintiliani, L.; Ricci, L.; Lanzone, J.; Ulivi, M.; Di Lazzaro, V. Depressive symptoms and difficulties in emotion regulation in adult patients with epilepsy: Association with quality of life and stigma. Epilepsy Behav. 2020, 107, 107073. [Google Scholar] [CrossRef]
- Stauder, M.; Vogel, A.C.; Nirola, D.K.; Tshering, L.; Dema, U.; Dorji, C.; Dorji, L.; Mateen, F.J. Depression, sleep quality, and social isolation among people with epilepsy in bhutan: A cross-sectional study. Epilepsy Behav. 2020, 112, 107450. [Google Scholar] [CrossRef]
- Shen, Y.; Zhang, M.; Wang, Y.; Wang, L.; Xu, X.; Xiao, G.; Chen, J.; Zhang, T.; Zhou, N. Subjective Sleep Disturbance in Chinese Adults with Epilepsy: Associations with Affective Symptoms. Epilepsy Res. 2017, 135, 150–157. [Google Scholar] [CrossRef]
- Lee, S.-A.; No, Y.-J.; Jo, K.-D.; Kwon, J.-H.; Kim, J.Y.; Shin, D.-J. Factors contributing to excessive daytime sleepiness in korean adults with epilepsy: A sleep questionnaire-based study. Epilepsy Behav. 2019, 90, 61–65. [Google Scholar] [CrossRef]
- Owczarek, K.; Rozenek, H.; Michalak, L. Some aspects of quality of life in epilepsy. Postępy Psychiatrii I Neurologii 2007, 16, 63–68. [Google Scholar]
- Cramer, J.A.; Perrine, K.; Devinsky, O.; Bryant-Comstock, L.; Meador, K.; Hermann, B. Development and cross-cultural translations of a 31-item quality of life in epilepsy inventory. Epilepsia 1998, 39, 81–88. [Google Scholar] [CrossRef]
- Coleman, H.; Peterson, C.; Walker, C. Examining quality of life in an Australian cohort of people with epilepsy over six years—Understanding the role of stigma and mood. Epilepsy Behav. 2020, 113, 107473. [Google Scholar] [CrossRef]
- Merz, C.J. Contribution of stress and sex hormones to memory encoding. Psychoneuroendocrinology 2017, 82, 51–58. [Google Scholar] [CrossRef]
- Schenck, C.H.; Arnulf, I.; Mahowald, M.W. Sleep and sex: What can go wrong? A review of the literature on sleep related disorders and abnormal sexual behaviors and experiences. Sleep 2007, 30, 683–702. [Google Scholar] [CrossRef]
- Henning, O.; Johannessen Landmark, C.; Traeen, B.; Svendsen, T.; Farmen, A.; Nakken, K.O.; Lossius, M. Sexual function in people with epilepsy: Similarities and differences with the general population. Epilepsia 2019, 60, 1984–1992. [Google Scholar] [CrossRef] [PubMed]
- Bossini, L.; Fortini, V.; Casolaro, I.; Caterini, C.; Koukouna, D.; Cecchini, F.; Benbow, J.; Fagiolini, A. Sexual dysfunctions, psychiatric diseases and quality of life: A review. Psychiatr. Pol. 2014, 48, 715–726. [Google Scholar] [PubMed]
- Henning, O.J.; Nakken, K.O.; Træen, B.; Mowinckel, P.; Lossius, M. Sexual problems in people with refractory epilepsy. Epilepsy Behav. 2016, 61, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Atif, M.; Sarwar, M.R.; Scahill, S. The relationship between epilepsy and sexual dysfunction: A review of the literature. Springerplus 2016, 5, 2070. [Google Scholar] [CrossRef] [PubMed]
- Dawson, E.; Stutzman, S.E.; Olson, D.M.; Hays, R.S. Performance of the international index of erectile function tool in men with epilepsy. Epilepsy Behav. 2019, 94, 78–81. [Google Scholar] [CrossRef]
- Zhao, S.; Tang, Z.; Xie, Q.; Wang, J.; Luo, L.; Liu, Y.; Zhu, Z.; Luo, J.; Zhao, Z. Association between epilepsy and risk of sexual dysfunction: A meta-analysis. Seizure 2019, 65, 80–88. [Google Scholar] [CrossRef]
- Rathore, C.; Henning, O.J.; Luef, G.; Radhakrishnan, K. Sexual dysfunction in people with epilepsy. Epilepsy Behav. 2019, 100, 106495. [Google Scholar] [CrossRef] [PubMed]
- Holka-Pokorska, J.; Wichniak, A.; Wierzbicka, A.; Lew Starowicz, M.; Jarkiewicz, M.; Jernajczyk, W.; Jarema, M. Sexual dysfunctions in patients referred to sleep disorders center. J. Sex. Med. 2017, 14, e304. [Google Scholar] [CrossRef]
- Çilliler, A.E.; Güven, B. Sleep quality and related clinical features in patients with epilepsy: A preliminary report. Epilepsy Behav. 2020, 102, 106661. [Google Scholar] [CrossRef]
- Bergmann, M.; Prieschl, M.; Stefani, A.; Heidbreder, A.; Walser, G.; Frauscher, B.; Unterberger, I.; Högl, B. A prospective controlled study about sleep disorders in drug resistant epilepsy. Sleep Med. 2020, 75, 434–440. [Google Scholar] [CrossRef]
- Giuliano, L.; Mainieri, G.; Cicero, C.E.; Battaglia, G.; Guccione, A.; Salomone, S.; Drago, F.; Nicoletti, A.; Sofia, V.; Zappia, M. Parasomnias, sleep-related movement disorders and physiological sleep variants in focal epilepsy: A polysomnographic study. Seizure 2020, 81, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Hackett, M.L.; Nikpour, A.; Somerville, E.; Bleasel, A.; Ireland, C.; Ghougassian, D.F.; Anderson, C.S.; Glozier, N. Course and impact of sleep disturbance in newly diagnosed epilepsy: A prospective registry study. Clin. Neurol. Neurosurg. 2020, 195, 105963. [Google Scholar] [CrossRef] [PubMed]
- Owczarek, K.; Michalak, L. Assessing quality of life study in epileptic patients. Analise of some diagnostic methods. Epileptologia 2006, 14, 225–231. [Google Scholar]
- Quigg, M.; Gharai, S.; Ruland, J.; Schroeder, C.; Hodges, M.; Ingersoll, K.S.; Thorndike, F.P.; Yan, G.; Ritterband, L.M. Insomnia in epilepsy is associated with continuing seizures and worse quality of life. Epilepsy Res. 2016, 122, 91–96. [Google Scholar] [CrossRef]
- Gutter, T.; Callenbach, P.M.C.; Brouwer, O.F.; de Weerd, A.W. Prevalence of sleep disturbances in people with epilepsy and the impact on quality of life: A survey in secondary care. Seizure 2019, 69, 298–303. [Google Scholar] [CrossRef]
- Wichniak, A.; Wierzbicka, A.; Jernajczyk, W. Zasady rozpoznawania i leczenia bezsenności. Psychiatria W Praktyceklinicznej 2008, 1, 1–10. [Google Scholar]
- Fisher, R.S.; Vickrey, B.G.; Gibson, P.; Hermann, B.; Penovich, P.; Scherer, A.; Walker, S. The impact of epilepsy from the patient’s perspective ii: Views about therapy and health care. Epilepsy Res. 2000, 41, 53–62. [Google Scholar] [CrossRef]
- Sprecher, S. Sexual satisfaction in premarital relationships: Associations with satisfaction, love, commitment, and stability. J. Sex. Res. 2002, 39, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Izdebski, Z. Sexuality of Poles in the Early 21 Century. Research Analysis, 1st ed.; WUJ Press: Kraków, Poland, 2012. (In Polish) [Google Scholar]
- Leidy, N.K.; Elixhauser, A.; Vickrey, B.; Means, E.; Willian, M.K. Seizure frequency and the health-related quality of life of adults with epilepsy. Neurology 1999, 53, 162. [Google Scholar] [CrossRef] [PubMed]
- Birbeck, G.L.; Hays, R.D.; Cui, X.; Vickrey, B.G. Seizure reduction and quality of life improvements in people with epilepsy. Epilepsia 2002, 43, 535–538. [Google Scholar] [CrossRef] [PubMed]
- Zelená, V.; Kuba, R.; Soška, V.; Rektor, I. Depression as a prominent cause of sexual dysfunction in women with epilepsy. Epilepsy Behav. 2011, 20, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Heersink, M.; Kocovski, N.L.; MacKenzie, M.B.; Denomme, K.; Macrodimitris, S. Social anxiety and its psychosocial impact on the lives of people with epilepsy. Epilepsy Behav. 2015, 51, 286–293. [Google Scholar] [CrossRef]
- Stefanidou, M.; Montouris, G. Reproductive and sexual health concerns in transition-age adolescents and young adults with epilepsy. Semin. Pediatric Neurol. 2020, 36, 100855. [Google Scholar] [CrossRef]
- Zambrelli, E.; Turner, K.; Vignoli, A.; La Briola, F.; Dionisio, S.; Malanchini, S.; Galli, F.; Canevini, M.P. Sleep disturbances in italian children and adolescents with epilepsy: A questionnaire study. Epilepsy Behav. 2020, 106, 107014. [Google Scholar] [CrossRef]
- Furuichi, Y.; Sakakibara, T.; Nezu, S.; Saeki, K.; Obayashi, K.; Kurumatani, N.; Hoshida, T.; Doi, T.; Miki, N.; Kinoshita, S.; et al. Analysis of factors related to low health-related quality of life in children with epilepsy using a self-assessed japanese version of the KIDSCREEN-52. Brain Dev. 2021, 43, 78–88. [Google Scholar] [CrossRef]
- Lin, C.-Y.; Potenza, M.N.; Broström, A.; Blycker, G.R.; Pakpour, A.H. Mindfulness-based cognitive therapy for sexuality (MBCT-S) improves sexual functioning and intimacy among older women with epilepsy: A multicenter randomized controlled trial. Seizure 2019, 73, 64–74. [Google Scholar] [CrossRef]
- Paardekooper, D.; Thayer, Z.; Miller, L.; Nikpour, A.; Gascoigne, M.B. Group-based cognitive behavioral therapy program for improving poor sleep quality and quality of life in people with epilepsy: A pilot study. Epilepsy Behav. 2020, 104, 106884. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Ding, X.; Guo, Y.; Chen, Q.; Wang, W.; Zheng, Y.; Wang, S.; Ding, Y.; Ding, M. Multidisciplinary management improves anxiety, depression, medication adherence, and quality of life among patients with epilepsy in Eastern China: A prospective study. Epilepsy Behav. 2019, 100, 106400. [Google Scholar] [CrossRef] [PubMed]
- Do, J.; Webster, R.J.; Longmuir, P.E.; Ieradi, S.; Reddy, D.; Whiting, S.; Pohl, D. Physically active children with epilepsy have good objective sleep duration and efficiency despite subjective reports of fatigue and sleep problems. Epilepsy Behav. 2020, 104, 106853. [Google Scholar] [CrossRef] [PubMed]
- Ayala-Guerrero, F.; Mexicano, G.; Gutiérrez-Chávez, C.A.; Lazo, L.A.; Mateos, E.L. Effect of gabapentin on sleep patterns disturbed by epilepsy. Epilepsy Behav. 2019, 92, 290–296. [Google Scholar] [CrossRef]
- Rocamora, R.; Álvarez, I.; Chavarría, B.; Principe, A. Perampanel effect on sleep architecture in patients with epilepsy. Seizure 2020, 76, 137–142. [Google Scholar] [CrossRef]
- Pavlova, M.K.; Wang, W.; Pham, J.; Ramel, J.; Latreille, V. Objectively measured sleep–wake patterns in patients with drug-resistant epilepsy–interaction with quality of life and antiepileptic treatment. Epilepsy Behav. 2020, 112, 107316. [Google Scholar] [CrossRef] [PubMed]
- Deleo, F.; Quintas, R.; Pastori, C.; Pappalardo, I.; Didato, G.; Di Giacomo, R.; de Curtis, M.; Villani, F. Quality of life, psychiatric symptoms, and stigma perception in three groups of persons with epilepsy. Epilepsy Behav. 2020, 110, 107170. [Google Scholar] [CrossRef]


{kind=link}
| Data | N = Number of Subjects | % | |
|---|---|---|---|
| Marital status | Married Unmarried Divorced/separated Widowed Domestic partnership | 75 68 15 4 7 | 44.4% 40.2% 8.9% 2.4% 4.1% |
| Number of Children | 0 1 2 3 4 5 | 80 41 29 12 3 1 | 48.2% 24.7% 17.5% 7.2% 1.8% 0.6% |
| Education | Tertiary Secondary Vocational Primary | 28 84 38 20 | 16.5% 49.4% 22.4% 11.8% |
| Place of Residence | Village Town < 10,000 inhabit. Big town > 10,000 < 100,000 inhabit. City > 100,000 inhabit. | 52 27 44 46 | 30.6% 15.9% 25.9% 27.1% |
| Type of Seizure | Generalized Tonic-Clonic Seizures | Complex Partial Seizures | Simple Partial Seizures | Absence Seizures | Myoclonic Seizures | Unclassified Seizures | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Frequency of Seizures | C | % | C | % | C | % | C | % | C | % | C | % |
| No seizures over the past 6 months | 53 | 50 | 32 | 32.3 | 17 | 48.6 | 8 | 57.1 | 3 | 33.3 | 3 | 1.8 |
| 1–2 seizures over the past 6 months | 29 | 27.4 | 23 | 23.2 | 6 | 17.1 | 2 | 14.3 | ||||
| 3–5 seizures over the past 6 months | 10 | 9.4 | 10 | 10.1 | 3 | 8.6 | 1 | 7.1 | 1 | 11.1 | ||
| 1 or more seizures per month | 8 | 7.5 | 21 | 21.2 | 5 | 14.3 | ||||||
| 1 or more seizures per week | 6 | 5.7 | 12 | 12.1 | 4 | 11.4 | 2 | 14.3 | 2 | 22.2 | ||
| 1 or more seizures per day | 1 | 1.0 | 1 | 7.1 | 3 | 33.3 | ||||||
| Sleep Initiation Problems | N | Average | Standard Deviation | t | p | |
|---|---|---|---|---|---|---|
| SW | yes | 75 | 41.27 | 24.40 | −5.181 | 0.0001 |
| no | 95 | 61.77 | 26.45 | |||
| yes | 75 | 48.50 | 22.18 | −2.836 | 0.005 | |
| no | 95 | 58.96 | 25.75 | |||
| EWB | yes | 75 | 40.51 | 6.52 | −2.140 | 0.034 |
| no | 95 | 42.47 | 5.07 | |||
| EF | yes | 75 | 41.20 | 8.63 | −0.687 | 0.493 |
| no | 95 | 42.07 | 7.88 | |||
| COG | yes | 75 | 32.73 | 13,46 | −4.820 | 0.0001 |
| no | 95 | 43,25 | 14.58 | |||
| ME | yes | 75 | 45.11 | 26.65 | −3.616 | 0.0001 |
| no | 95 | 61.23 | 30.40 | |||
| SF | yes | 75 | 47.37 | 20.78 | −3.939 | 0.0001 |
| no | 95 | 60.28 | 21.46 | |||
| QOLIE-31 | yes | 75 | 41.25 | 11.30 | −5.175 | 0.0001 |
| no | 95 | 50.79 | 12.36 |
| Satisfaction with Sex Life | N | Average | Standard Deviation | t | p | |
|---|---|---|---|---|---|---|
| SW | Yes | 76 | 57.64 | 29.60 | 2.27 | 0.024 |
| No | 57 | 46.24 | 26.03 | |||
| yes | 76 | 60.60 | 25.04 | 2.83 | 0.005 | |
| no | 57 | 48.46 | 23.51 | |||
| EWB | yes | 76 | 41.76 | 5.02 | 1.56 | 0.121 |
| no | 57 | 40.25 | 5.87 | |||
| EF | yes | 76 | 43.77 | 7.67 | 4.08 | 0.0001 |
| no | 57 | 38.38 | 7.30 | |||
| COG | yes | 76 | 42.20 | 13.92 | 2.24 | 0.027 |
| no | 57 | 36.31 | 16.26 | |||
| ME | yes | 76 | 51.85 | 31.08 | −1.35 | 0.179 |
| no | 57 | 59.11 | 30.00 | |||
| SF | yes | 76 | 59.52 | 23.29 | 2.62 | 0.010 |
| no | 57 | 49.58 | 20.20 | |||
| QOLIE-31 | yes | 76 | 50.06 | 13.00 | 3.08 | 0.003 |
| no | 57 | 43.12 | 12.01 |
| Epilepsy as the Cause of Problems with Sex Life | N | Average | Standard Deviation | t | p | |
|---|---|---|---|---|---|---|
| SW | yes | 54 | 39.08 | 25.23 | −4.591 | 0.0001 |
| no | 109 | 59.10 | 26.61 | |||
| yes | 54 | 45.37 | 23.77 | −3.397 | 0.001 | |
| no | 109 | 58.87 | 23.86 | |||
| EWB | yes | 54 | 39.63 | 6.33 | −2.617 | 0.010 |
| no | 109 | 42.22 | 5.10 | |||
| EF | yes | 54 | 38.80 | 7.08 | −3.300 | 0.001 |
| no | 109 | 43.19 | 8.41 | |||
| COG | yes | 54 | 31.85 | 13.31 | −4.301 | 0.0001 |
| no | 109 | 41.95 | 14.46 | |||
| ME | yes | 54 | 46.40 | 29.69 | −2.394 | 0.018 |
| no | 109 | 58.20 | 29.54 | |||
| SF | yes | 54 | 44.61 | 20.66 | −4.403 | 0.0001 |
| no | 109 | 59.85 | 20.83 | |||
| QOLIE-31 | yes | 54 | 39.44 | 10.98 | −5.498 | 0.0001 |
| no | 109 | 50.13 | 11.99 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rozenek, H.; Zaręba, K.; Banasiewicz, J.; Wójtowicz, S.; Krasuski, T.; Owczarek, K. The Quality of Life in Patients with Epilepsy in the Context of Sleep Problems and Sexual Satisfaction. Brain Sci. 2021, 11, 778. https://doi.org/10.3390/brainsci11060778
Rozenek H, Zaręba K, Banasiewicz J, Wójtowicz S, Krasuski T, Owczarek K. The Quality of Life in Patients with Epilepsy in the Context of Sleep Problems and Sexual Satisfaction. Brain Sciences. 2021; 11(6):778. https://doi.org/10.3390/brainsci11060778
Chicago/Turabian StyleRozenek, Hanna, Kornelia Zaręba, Jolanta Banasiewicz, Stanisław Wójtowicz, Tomasz Krasuski, and Krzysztof Owczarek. 2021. "The Quality of Life in Patients with Epilepsy in the Context of Sleep Problems and Sexual Satisfaction" Brain Sciences 11, no. 6: 778. https://doi.org/10.3390/brainsci11060778
APA StyleRozenek, H., Zaręba, K., Banasiewicz, J., Wójtowicz, S., Krasuski, T., & Owczarek, K. (2021). The Quality of Life in Patients with Epilepsy in the Context of Sleep Problems and Sexual Satisfaction. Brain Sciences, 11(6), 778. https://doi.org/10.3390/brainsci11060778