
Anemia and the Risk of Cognitive Impairment: An Updated Systematic Review and Meta-Analysis

 ,
, 
 , ,
, ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Approach
2.2. Search Strategy
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Data Extraction
2.6. Study Quality
2.7. Statistical Analysis
3. Results
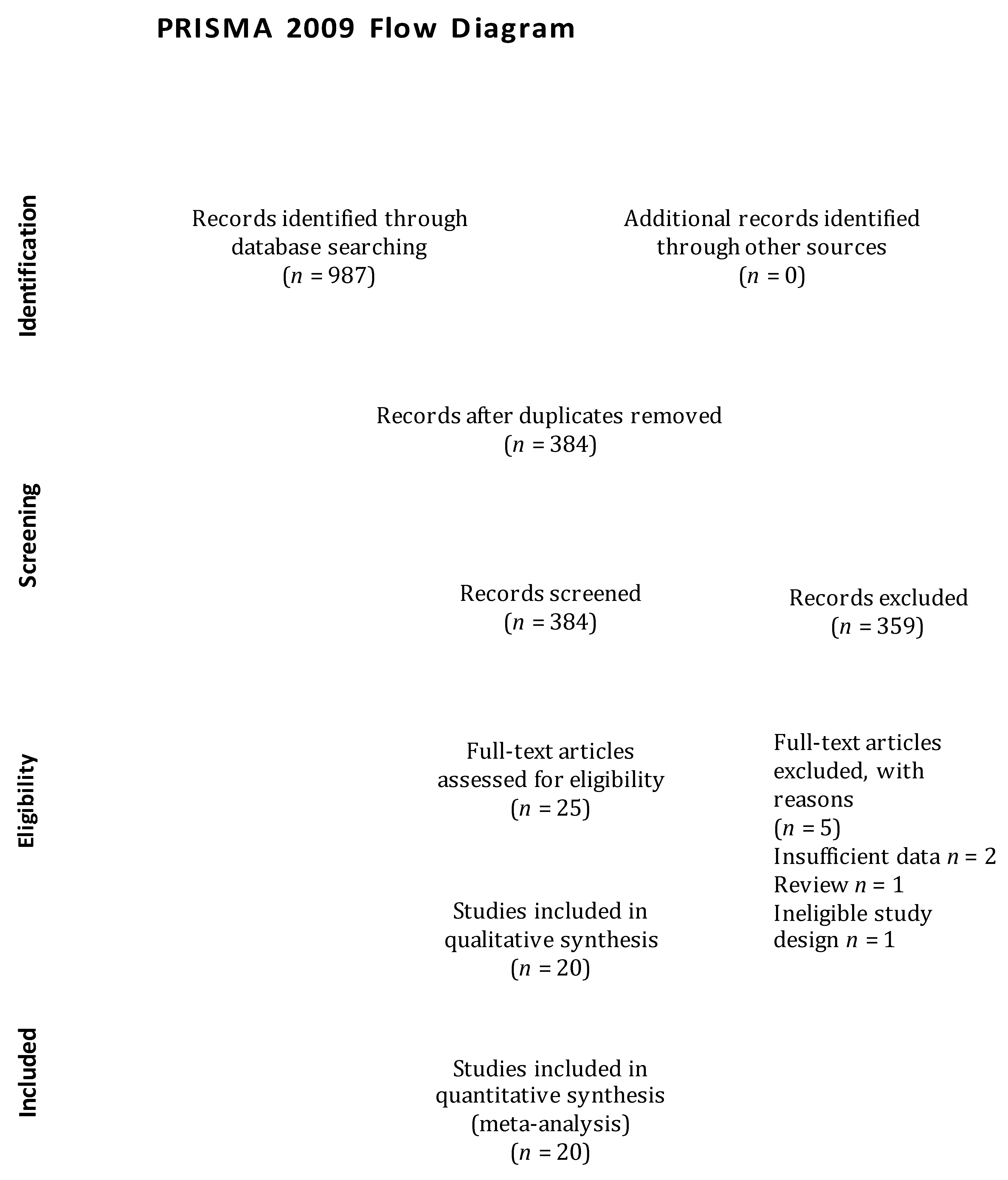
3.1. Study Selection
3.2. Study Characteristics
3.3. Methodological Quality Assessment
3.4. Meta-Analysis
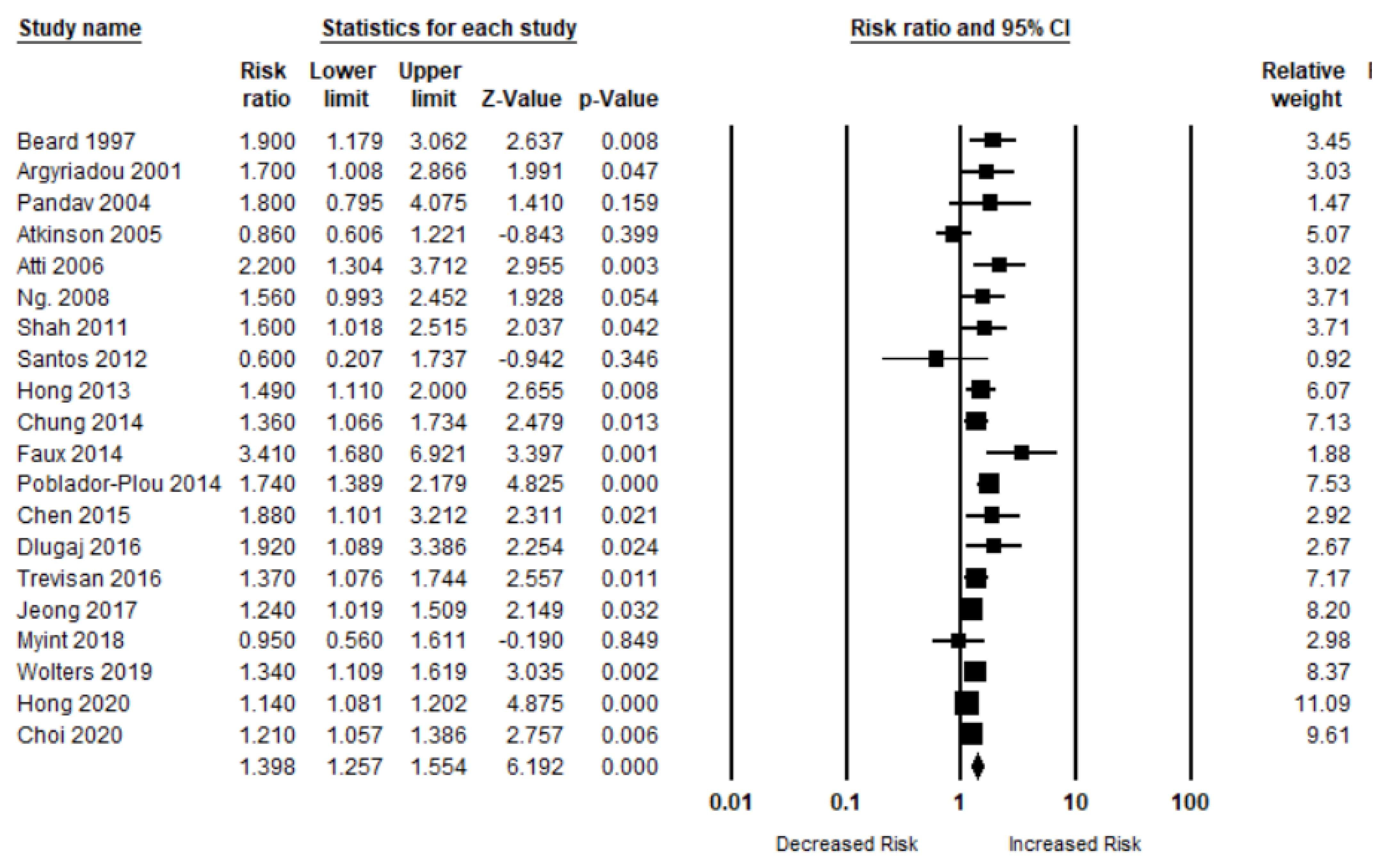
3.4.1. Anemia and Overall Cognitive Impairment
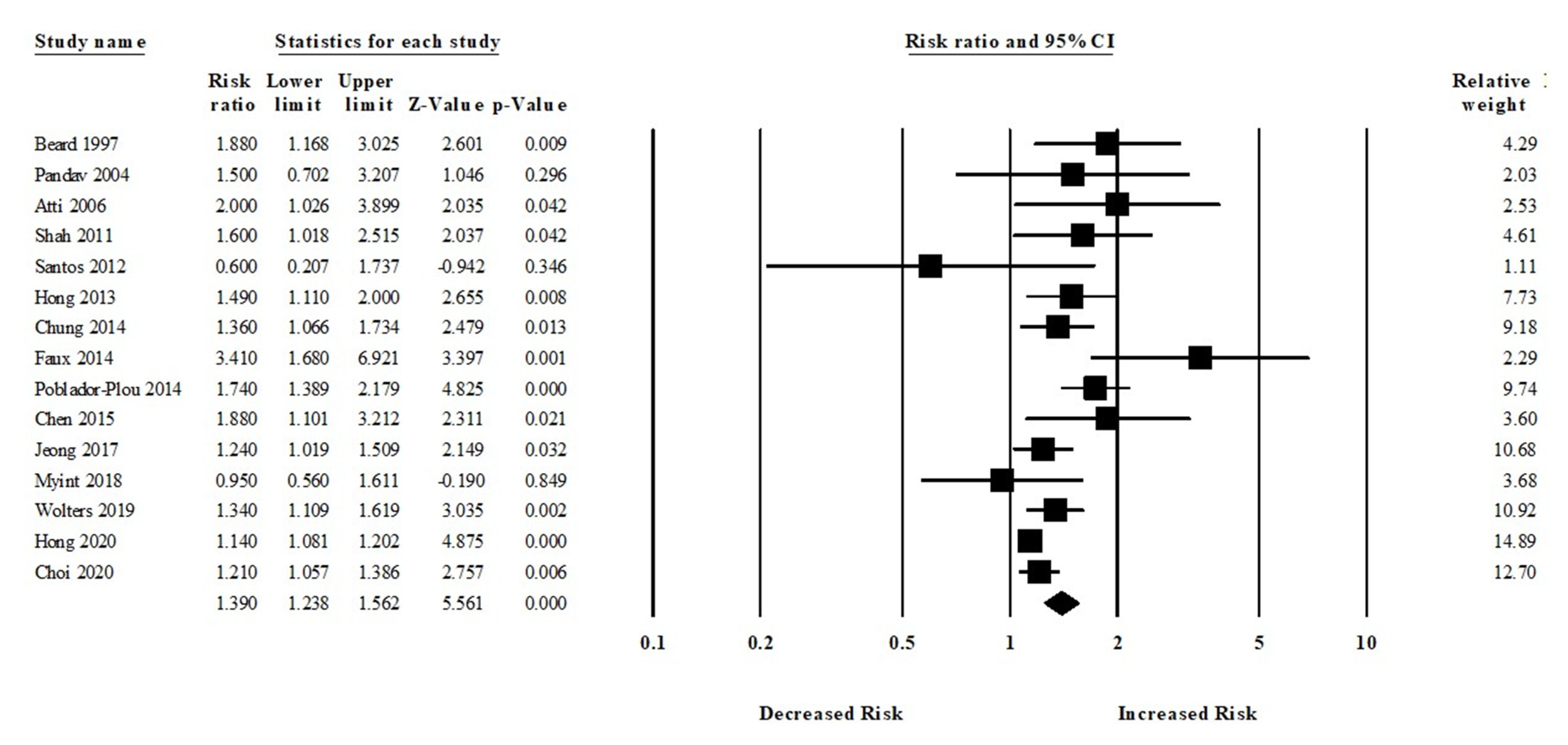
3.4.2. Anemia and All-Cause Dementia Risk
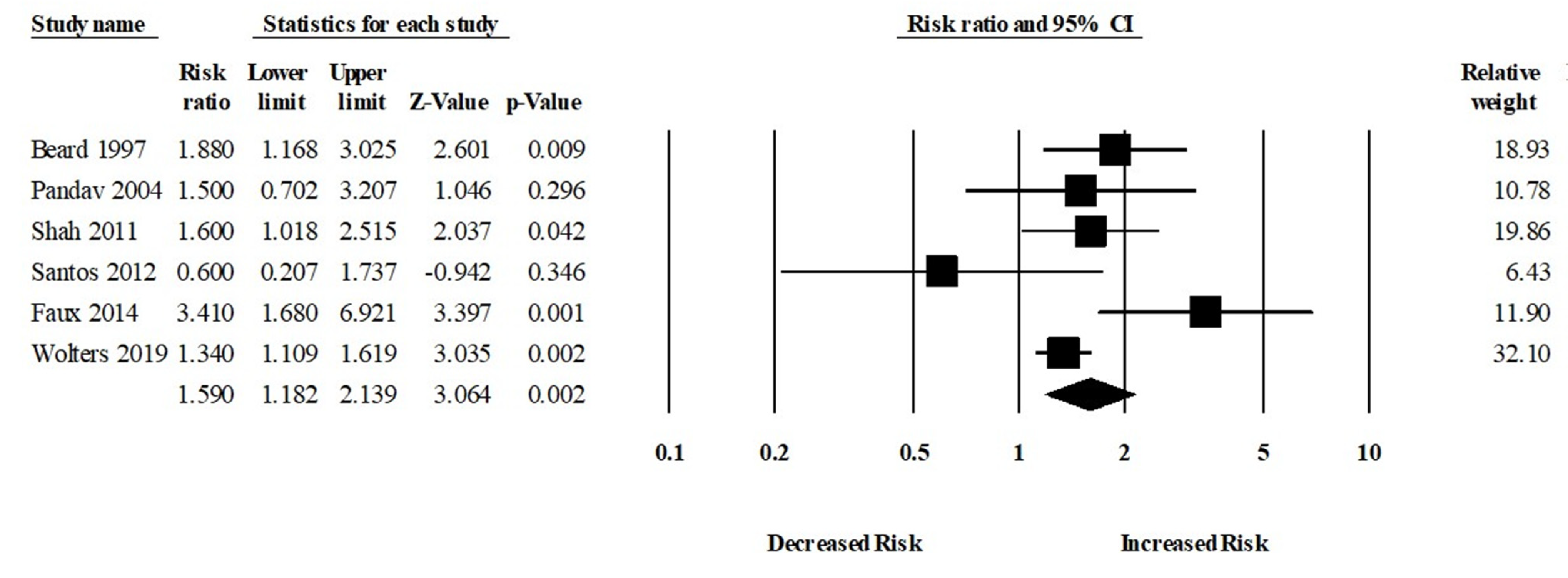
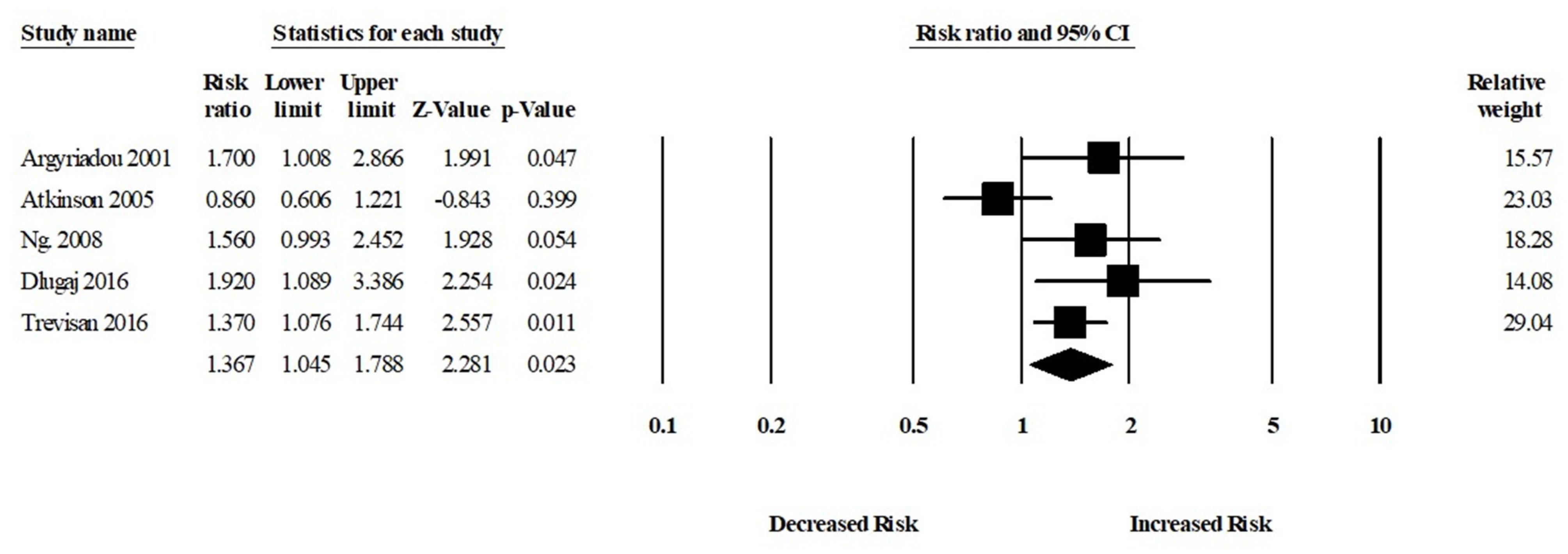
3.4.3. Anemia and MCI Risk
3.5. Subgroup Analysis
3.6. Sensitivity Analysis
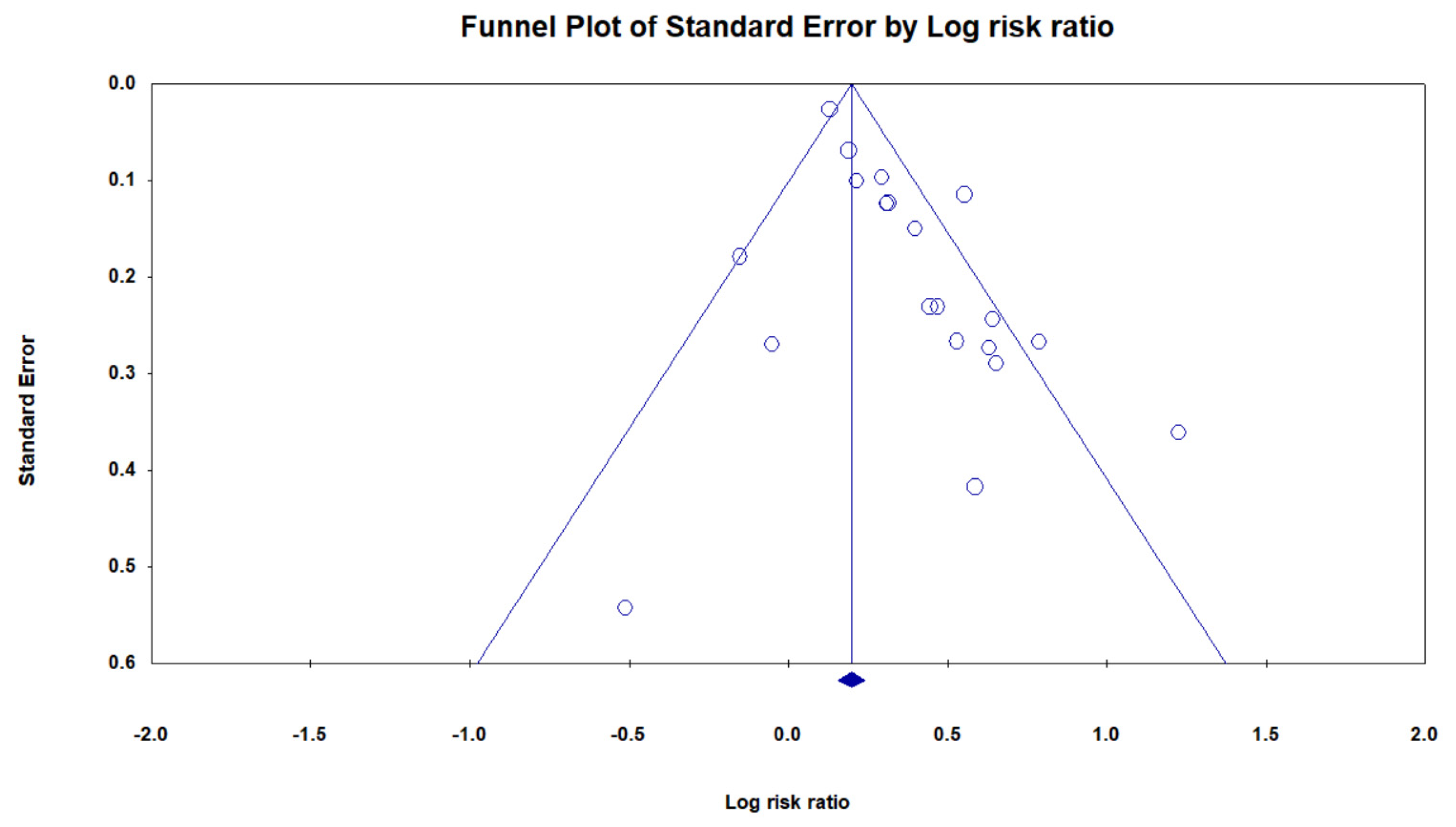
3.7. Publication Bias
4. Discussion
4.1. Main Findings
4.2. Biological Plausibility
4.3. Public Health Implications
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pavisic, I.M.; Suarez-Gonzalez, A.; Pertzov, Y. Translating visual short-term memory binding tasks to clinical practice: From theory to practice. Front. Neurol. 2020, 11, 458. [Google Scholar] [CrossRef]
- Bennett, B.; McDonald, F.; Beattie, E.; Carney, T.; Freckelton, I.; White, B.; Willmott, L. Assistive technologies for people with dementia: Ethical considerations. Bull. World Health Organ. 2017, 95, 749. [Google Scholar] [CrossRef] [PubMed]
- Borisov, A.; Ivanova, N.; Vyazgina, E.; Danilov YuP, B.E. A Modern Approach to the Problem of Cognitive and Motor Impairment in Dementia. J. Alzheimers Neurodegener. Dis. 2020, 6, 035. [Google Scholar]
- Shah, H.; Albanese, E.; Duggan, C.; Rudan, I.; Langa, K.M.; Carrillo, M.C.; Chan, K.Y.; Joanette, Y.; Prince, M.; Rossor, M. Research priorities to reduce the global burden of dementia by 2025. Lancet Neurol. 2016, 15, 1285–1294. [Google Scholar] [CrossRef]
- Nichols, E.; Szoeke, C.E.; Vollset, S.E.; Abbasi, N.; Abd-Allah, F.; Abdela, J.; Aichour, M.T.E.; Akinyemi, R.O.; Alahdab, F.; Asgedom, S.W. Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 88–106. [Google Scholar] [CrossRef]
- Argyriadou, S.; Vlachonikolis, I.; Melisopoulou, H.; Katachanakis, K.; Lionis, C. In what extent anemia coexists with cognitive impairment in elderly: A cross-sectional study in Greece. BMC Fam. Pract. 2001, 2, 5. [Google Scholar] [CrossRef] [PubMed]
- Sousa, N.D.S.; Menezes, T.N.d.; Silva, N.d.A.; Eulálio, M.d.C.; Paiva, A.d.A. Prevalence of anemia and correlation between the concentration of hemoglobin and cognitive factors among the elderly. Cienc. Saude Coletiva 2018, 23, 935–944. [Google Scholar] [CrossRef]
- Macedo, B.G.; Dias, P.P.; Camara, H.S.; Antunes, C.M.F. Anemia in the Elderly: Neuropsychiatric Repercussions. Adv. Aging Res. 2017, 6, 11. [Google Scholar] [CrossRef]
- Kim, H.-B.; Park, B.; Shim, J.-Y. Anemia in association with cognitive impairment: A systematic review and meta-analysis. J. Alzheimer’s Dis. 2019, 72, 803–814. [Google Scholar] [CrossRef]
- Peters, R.; Burch, L.; Warner, J.; Beckett, N.; Poulter, R.; Bulpitt, C. Haemoglobin, anaemia, dementia and cognitive decline in the elderly, a systematic review. BMC Geriatr. 2008, 8, 18. [Google Scholar] [CrossRef]
- Zhang, X.; Le, W. Pathological role of hypoxia in Alzheimer’s disease. Exp. Neurol. 2010, 223, 299–303. [Google Scholar] [CrossRef]
- Park, S.E.; Kim, H.; Lee, J.; Lee, N.K.; Hwang, J.W.; Yang, J.-j.; Ye, B.S.; Cho, H.; Kim, H.J.; Kim, Y.J. Decreased hemoglobin levels, cerebral small-vessel disease, and cortical atrophy: Among cognitively normal elderly women and men. Int. Psychogeriatr. 2016, 28, 147. [Google Scholar] [CrossRef]
- Youdim, M.B. Brain iron deficiency and excess; cognitive impairment and neurodegenration with involvement of striatum and hippocampus. Neurotox. Res. 2008, 14, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Poly, T.N.; Islam, M.M.; Walther, B.A.; Yang, H.-C.; Wu, C.-C.; Lin, M.-C.; Li, Y.-C. Association between use of statin and risk of dementia: A meta-analysis of observational studies. Neuroepidemiology 2020, 54, 214–226. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Beard, C.M.; Kokmen, E.; O’Brien, P.C.; Anía, B.J.; Melton III, L.J. Risk of Alzheimer’s disease among elderly patients with anemia: Population-based investigations in Olmsted County, Minnesota. Ann. Epidemiol. 1997, 7, 219–224. [Google Scholar] [CrossRef]
- Pandav, R.S.; Chandra, V.; Dodge, H.H.; DeKosky, S.T.; Ganguli, M. Hemoglobin levels and Alzheimer disease: An epidemiologic study in India. Am. J. Geriatr. Psychiatry 2004, 12, 523–526. [Google Scholar] [CrossRef]
- Atkinson, H.H.; Cesari, M.; Kritchevsky, S.B.; Penninx, B.W.; Fried, L.P.; Guralnik, J.M.; Williamson, J.D. Predictors of combined cognitive and physical decline. J. Am. Geriatr. Soc. 2005, 53, 1197–1202. [Google Scholar] [CrossRef]
- Atti, A.R.; Palmer, K.; Volpato, S.; Zuliani, G.; Winblad, B.; Fratiglioni, L. Anaemia increases the risk of dementia in cognitively intact elderly. Neurobiol. Aging 2006, 27, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Ng, T.-P.; Feng, L.; Niti, M.; Yap, K.B. Albumin, haemoglobin, BMI and cognitive performance in older adults. Age Ageing 2008, 37, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.; Buchman, A.; Wilson, R.; Leurgans, S.; Bennett, D. Hemoglobin level in older persons and incident Alzheimer disease: Prospective cohort analysis. Neurology 2011, 77, 219–226. [Google Scholar] [CrossRef]
- Santos, I.S.; Scazufca, M.; Lotufo, P.A.; Menezes, P.R.; Bensenor, I.M. Anemia and dementia among the elderly: The São Paulo Ageing & Health Study. Int. Psychogeriatr. 2012, 24, 74. [Google Scholar]
- Hong, C.H.; Falvey, C.; Harris, T.B.; Simonsick, E.M.; Satterfield, S.; Ferrucci, L.; Metti, A.L.; Patel, K.V.; Yaffe, K. Anemia and risk of dementia in older adults: Findings from the Health ABC study. Neurology 2013, 81, 528–533. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.-D.; Sheu, J.-J.; Kao, L.-T.; Lin, H.-C.; Kang, J.-H. Dementia is associated with iron-deficiency anemia in females: A population-based study. J. Neurol. Sci. 2014, 346, 90–93. [Google Scholar] [CrossRef]
- Faux, N.G.; Rembach, A.; Wiley, J.; Ellis, K.A.; Ames, D.; Fowler, C.J.; Martins, R.N.; Pertile, K.K.; Rumble, R.L.; Trounson, B. An anemia of Alzheimer’s disease. Mol. Psychiatry 2014, 19, 1227–1234. [Google Scholar] [CrossRef]
- Poblador-Plou, B.; Calderón-Larrañaga, A.; Marta-Moreno, J.; Hancco-Saavedra, J.; Sicras-Mainar, A.; Soljak, M.; Prados-Torres, A. Comorbidity of dementia: A cross-sectional study of primary care older patients. BMC Psychiatry 2014, 14, 84. [Google Scholar] [CrossRef]
- Chen, Y.-G.; Lin, T.-Y.; Chen, H.-J.; Dai, M.-S.; Ho, C.-L.; Kao, C.-H. Thalassemia and risk of dementia: A nationwide population-based retrospective cohort study. Eur. J. Intern. Med. 2015, 26, 554–559. [Google Scholar] [CrossRef]
- Dlugaj, M.; Winkler, A.; Weimar, C.; Duerig, J.; Broecker-Preuss, M.; Dragano, N.; Moebus, S.; Joeckel, K.-H.; Erbel, R.; Eisele, L. Anemia and mild cognitive impairment in the German general population. J. Alzheimer’s Dis. 2016, 49, 1031–1042. [Google Scholar] [CrossRef]
- Trevisan, C.; Veronese, N.; Bolzetta, F.; De Rui, M.; Maggi, S.; Zambon, S.; Musacchio, E.; Sartori, L.; Perissinotto, E.; Crepaldi, G. Low hemoglobin levels and the onset of cognitive impairment in older people: The PRO. VA Study. Rejuvenation Res. 2016, 19, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.-M.; Shin, D.W.; Lee, J.E.; Hyeon, J.H.; Lee, J.; Kim, S. Anemia is associated with incidence of dementia: A national health screening study in Korea involving 37,900 persons. Alzheimer’s Res. Ther. 2017, 9, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Myint, P.K.; Owen, S.; McCarthy, K.; Pearce, L.; Moug, S.J.; Stechman, M.J.; Hewitt, J.; Carter, B. Is anemia associated with cognitive impairment and delirium among older acute surgical patients? Geriatr. Gerontol. Int. 2018, 18, 1025–1030. [Google Scholar] [CrossRef]
- Wolters, F.J.; Zonneveld, H.I.; Licher, S.; Cremers, L.G.; Ikram, M.K.; Koudstaal, P.J.; Vernooij, M.W.; Ikram, M.A.; Group, H.B.C.C.R. Hemoglobin and anemia in relation to dementia risk and accompanying changes on brain MRI. Neurology 2019, 93, e917–e926. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.-T.; Hsieh, Y.-C.; Liu, H.-Y.; Chiou, H.-Y.; Chien, L.-N. Association Between Anemia and Dementia: A Nationwide, Population-based Cohort Study in Taiwan. Curr. Alzheimer Res. 2020, 17, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.W.; Kim, T.H.; Han, E. Anemia and incidence of dementia in patients with new-onset type 2 diabetes: A nationwide population-based cohort study. BMJ Open Diabetes Res. Care 2020, 8, e001289. [Google Scholar] [CrossRef]
- Duffin, J.; Hare, G.M.; Fisher, J.A. A mathematical model of cerebral blood flow control in anaemia and hypoxia. J. Physiol. 2020, 598, 717–730. [Google Scholar] [CrossRef]
- Juttukonda, M.R.; Donahue, M.J.; Waddle, S.L.; Davis, L.T.; Lee, C.A.; Patel, N.J.; Pruthi, S.; Kassim, A.A.; Jordan, L.C. Reduced oxygen extraction efficiency in sickle cell anemia patients with evidence of cerebral capillary shunting. J. Cereb. Blood Flow Metab. 2021, 41, 546–560. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, C.; Correia, S.C.; Santos, R.X.; Cardoso, S.; Moreira, P.I.; Clark, T.A.; Zhu, X.; Smith, M.A.; Perry, G. Role of mitochondrial-mediated signaling pathways in Alzheimer disease and hypoxia. J. Bioenerg. Biomembr. 2009, 41, 433. [Google Scholar] [CrossRef]
- Kawahara, M.; Kuroda, Y. Molecular mechanism of neurodegeneration induced by Alzheimer’s β-amyloid protein: Channel formation and disruption of calcium homeostasis. Brain Res. Bull. 2000, 53, 389–397. [Google Scholar] [CrossRef]
- Zheng, W.-H.; Bastianetto, S.; Mennicken, F.; Ma, W.; Kar, S. Amyloid β peptide induces tau phosphorylation and loss of cholinergic neurons in rat primary septal cultures. Neuroscience 2002, 115, 201–211. [Google Scholar] [CrossRef]
- Stenvinkel, P. Anaemia and inflammation: What are the implications for the nephrologist? Nephrol. Dial. Transplant. 2003, 18 (Suppl. 8), viii17–viii22. [Google Scholar] [CrossRef]
- Weuve, J.; Ridker, P.M.; Cook, N.R.; Buring, J.E.; Grodstein, F. High-sensitivity C-reactive protein and cognitive function in older women. Epidemiology 2006, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Eagan, D.E.; Gonzales, M.M.; Tarumi, T.; Tanaka, H.; Stautberg, S.; Haley, A.P. Elevated serum C-reactive protein relates to increased cerebral myoinositol levels in middle-aged adults. Cardiovasc. Psychiatry Neurol. 2012, 2012, 120540. [Google Scholar] [CrossRef]
- Marsland, A.L.; Gianaros, P.J.; Abramowitch, S.M.; Manuck, S.B.; Hariri, A.R. Interleukin-6 covaries inversely with hippocampal grey matter volume in middle-aged adults. Biol. Psychiatry 2008, 64, 484–490. [Google Scholar] [CrossRef]
- Wu, D.-X.; Feng, L.; Yao, S.-Q.; Tian, X.-F.; Mahendran, R.; Kua, E.-H. The early dementia prevention programme in Singapore. Lancet Psychiatry 2014, 1, 9–11. [Google Scholar] [CrossRef]
- Islam, M.M.; Iqbal, U.; Walther, B.; Atique, S.; Dubey, N.K.; Nguyen, P.-A.; Poly, T.N.; Masud, J.H.B.; Li, Y.-C.J.; Shabbir, S.-A. Benzodiazepine use and risk of dementia in the elderly population: A systematic review and meta-analysis. Neuroepidemiology 2016, 47, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Dannhauser, T.M.; Cleverley, M.; Whitfield, T.J.; Fletcher, B.C.; Stevens, T.; Walker, Z. A complex multimodal activity intervention to reduce the risk of dementia in mild cognitive impairment–ThinkingFit: Pilot and feasibility study for a randomized controlled trial. BMC Psychiatry 2014, 14, 129. [Google Scholar] [CrossRef]
- Kivipelto, M.; Mangialasche, F.; Ngandu, T. Lifestyle interventions to prevent cognitive impairment, dementia and Alzheimer disease. Nat. Rev. Neurol. 2018, 14, 653–666. [Google Scholar] [CrossRef] [PubMed]
- Tamura, M.K.; Vittinghoff, E.; Yang, J.; Go, A.S.; Seliger, S.L.; Kusek, J.W.; Lash, J.; Cohen, D.L.; Simon, J.; Batuman, V. Anemia and risk for cognitive decline in chronic kidney disease. BMC Nephrol. 2016, 17, 13. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author Year | Country | Study Design | Female Patients (%) | Mean Age | Criteria for Anemia Patients’ Inclusion | Criteria for Dementia/Cognitive Impairment Patients’ Inclusion | Number of Dementia Patients | OR/HR | NOS |
|---|---|---|---|---|---|---|---|---|---|
| Beard, 1997 [18] | USA | C-C | 77.3 | 82.5 | WHO | DSM | 191 | 1.91 (1.19–3.09) | 5 |
| Argyriadou, 2001 [6] | Greece | C-C | 54.3 | 65~ | Mean hematocrit (Hct): Men < 38%, Women ≤ 36% | MMSE < 24 | 213 | 1.70 (1.02–2.90) | 6 |
| Pandav, 2004 [19] | India | Co | 56.6 | 69.6 | WHO | DSM | 26 | 1.80 (0.8–4.10) | 8 |
| Atkinson, 2005 [20] | USA | Co | 100 | 78 | WHO | MMSE < 24 | 68 | 0.86 (0.60–1.21) | 6 |
| Atti, 2006 [21] | Sweden | Co | 72 | 81.5 | WHO | DSM | 108 | 2.20 (1.30–3.70) | 6 |
| Ng., 2008 [22] | Singapore | C-C | 63.2 | 65.8 | Lowest Hb quintile Men: Hb < 13.3 g/dL, Women: Hb < 12.2 g/dL | MMSE < 24 | 298 | 1.56 (1.00–2.47) | 8 |
| Shah, 2011 [23] | USA | Co | 74.7 | 80.8 | WHO | NINCD-ADRDA | 113 | 1.60 (1.02–2.52) | 7 |
| Santos, 2012 [24] | Brazil | C-C | 60.4 | 70.4 | WHO | DSM | 99 | 0.60 (0.21–1.76) | 7 |
| Hong, 2013 [25] | USA | Co | 51.8 | 76.1 | WHO | 3MS | 455 | 1.49 (1.11–2.00) | 8 |
| Chung, 2014 [26] | Taiwan | C-C | 54.7 | 76.4 | ICD-9-CM | ICD-9-CM | 8300 | 1.36 (1.07–1.74) | 8 |
| Faux, 2014 [27] | Australia | C-C | N/R | 35~79 | WHO | NINCD-ADRDA | 211 | 3.41 (1.68–6.92) | 7 |
| Poblador-Plou, 2014 [28] | Spain | C-C | 59.7 | 75.8 | ICD-9-CM | ICD-9-CM | 3971 | 1.74 (1.39–2.18) | 7 |
| Chen, 2015 [29] | Taiwan | Co | 57.5 | 38.9 | ICD-9-CM | ICD-9-CM | 871 | 1.88 (1.10–3.21) | 7 |
| Dlugaj, 2016 [30] | Germany | C-C | 50.8 | 64.4 | WHO | IWG | 579 | 1.92 (1.09–3.39) | 8 |
| Trevisan, 2016 [31] | Italy | Co | 58.4 | 72.1 | Gender-specific Hb tertiles; Men: 13.9–14.9 g/dL, Women: 12.8–13.7 g/dL | MMSE < 24 | 403 | 1.37 (1.08–1.75) | 8 |
| Jeong, 2017 [32] | S. Korea | Co | 51 | 66 | WHO | ICD-9-CM | 859 | 1.24 (1.02–1.51) | 8 |
| Myint, 2018 [33] | UK | Co | 53 | 76.5 | Hb < 12.9 g/dL | MoCA | 655 | 0.95 (0.56–1.61) | 8 |
| Wolters, 2019 [34] | Netherland | Co | 64.6 | 57.7 | WHO | MMSE < 26 | 1520 | 1.34 (1.11–1.62) | 8 |
| Hong, 2020 [35] | Taiwan | Co | 60.6 | 70.4 | ICD-9 | ICD-9 | N/R | 1.14 (1.08–1.21) | 8 |
| Choi, 2020 [36] | S. Korea | Co | 55.8 | 57.1 | WHO | ICD-10 | 1682 | 1.21 (1.06–1.39) | 8 |
| Subgroup | Pooled Estimate | Test of Heterogeneity | |||||
|---|---|---|---|---|---|---|---|
| N | aRR | p-Value | τ2 | I2 | Q | p-Value | |
| Outcomes | |||||||
| Overall cognitive impairment (OCI) | |||||||
| Study design | |||||||
| Cohort | 12 | 1.25 (1.14–1.37) | <0.001 | 0.008 | 41.63 | 18.84 | 0.06 |
| Case-control | 8 | 1.65 (1.37–2.00) | <0.001 | 0.02 | 34.91 | 10.74 | 0.15 |
| Study quality | |||||||
| High | 11 | 1.25 (1.16–1.35) | <0.001 | 0.004 | 29.39 | 14.16 | 0.16 |
| Low | 9 | 1.60 (1.23–2.08) | <0.001 | 0.09 | 62.71 | 21.45 | 0.006 |
| Location | |||||||
| Asia | 9 | 1.29 (1.13–1.47) | <0.001 | 0.01 | 56.11 | 18.22 | 0.02 |
| Europe | 7 | 1.48 (1.28–1.71) | <0.001 | 0.009 | 24.98 | 7.99 | 0.23 |
| USA | 4 | 1.37 (0.98–1.92) | 0.06 | 0.07 | 67.31 | 9.17 | 0.02 |
| Adjustment | Pooled Estimate | Test of Heterogeneity | |||||
|---|---|---|---|---|---|---|---|
| N | aRR | p-Value | τ2 | I2 | Q | p-Value | |
| Overall Cognitive Impairment | |||||||
| Diabetes | 13 | 1.37 (1.22–1.54) | <0.001 | 0.02 | 61.02 | 30.79 | 0.002 |
| Education | 11 | 1.38 (1.20–1.59) | <0.001 | 0.01 | 26.04 | 13.52 | 0.19 |
| Hypertension | 10 | 1.33 (1.19–1.49) | <0.001 | 0.01 | 62.60 | 24.06 | 0.004 |
| Smoking | 9 | 1.28 (1.13–1.45) | <0.001 | 0.01 | 39.54 | 13.23 | 0.10 |
| Depression | 6 | 1.33 (1.17–1.51) | <0.001 | 0.005 | 21.71 | 6.38 | 0.27 |
| Stroke | 5 | 1.42 (1.18–1.71) | <0.001 | 0.01 | 34.52 | 6.10 | 0.19 |
| APOE e4 | 3 | 1.40 (1.20–1.63) | 0.06 | 0 | 0 | 0.58 | <0.001 |
| CRP | 2 | 1.38 (1.17–1.63) | <0.001 | 0 | 0 | 0.34 | 0.55 |
| Dementia | |||||||
| Diabetes | 10 | 1.34 (1.17–1.54) | <0.001 | 0.02 | 65.11 | 25.79 | 0.002 |
| Education | 6 | 1.41 (1.22–1.63) | <0.001 | 0 | 0 | 4.25 | 0.51 |
| Hypertension | 8 | 1.32 (1.16–1.49) | <0.001 | 0.01 | 67.42 | 21.49 | 0.003 |
| Smoking | 6 | 1.28 (1.16–1.41) | <0.001 | 0.002 | 11.59 | 5.65 | 0.34 |
| Depression | 4 | 1.28 (1.13–1.45) | <0.001 | 0.003 | 19.77 | 3.74 | 0.29 |
| Stroke | 3 | 1.36 (1.10–1.70) | 0.05 | 0.01 | 45.42 | 3.66 | 0.16 |
| APOE e4 | 2 | 1.38 (1.17–1.63) | <0.001 | 0 | 0 | 0.34 | 0.55 |
| CRP | 2 | 1.38 (1.17–1.63) | <0.001 | 0 | 0 | 0.34 | 0.55 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kung, W.-M.; Yuan, S.-P.; Lin, M.-S.; Wu, C.-C.; Islam, M.M.; Atique, S.; Touray, M.; Huang, C.-Y.; Wang, Y.-C. Anemia and the Risk of Cognitive Impairment: An Updated Systematic Review and Meta-Analysis. Brain Sci. 2021, 11, 777. https://doi.org/10.3390/brainsci11060777
Kung W-M, Yuan S-P, Lin M-S, Wu C-C, Islam MM, Atique S, Touray M, Huang C-Y, Wang Y-C. Anemia and the Risk of Cognitive Impairment: An Updated Systematic Review and Meta-Analysis. Brain Sciences. 2021; 11(6):777. https://doi.org/10.3390/brainsci11060777
Chicago/Turabian StyleKung, Woon-Man, Sheng-Po Yuan, Muh-Shi Lin, Chieh-Chen Wu, Md. Mohaimenul Islam, Suleman Atique, Musa Touray, Chu-Ya Huang, and Yao-Chin Wang. 2021. "Anemia and the Risk of Cognitive Impairment: An Updated Systematic Review and Meta-Analysis" Brain Sciences 11, no. 6: 777. https://doi.org/10.3390/brainsci11060777
APA StyleKung, W.-M., Yuan, S.-P., Lin, M.-S., Wu, C.-C., Islam, M. M., Atique, S., Touray, M., Huang, C.-Y., & Wang, Y.-C. (2021). Anemia and the Risk of Cognitive Impairment: An Updated Systematic Review and Meta-Analysis. Brain Sciences, 11(6), 777. https://doi.org/10.3390/brainsci11060777