
The Impact of Hypertension and Atrial Fibrillation on Cognitive Decline and Subclinical Atherosclerosis


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Clinical Assessment
2.2. Parameters of Subclinical Atherosclerosis
2.2.1. Intima–Media Thickness (IMT)
2.2.2. Ankle Brachial Index (ABI)
2.3. Transthoracic Echocardiography Left Ventricular Parameters Function
2.4. Screening Tools for Cognitive Impairment, Daily Activity, and Depression Scales
2.4.1. Mini-Mental State Examination (MMSE)
2.4.2. Montreal Cognitive Assessment (MoCA)
2.4.3. Activities of Daily Living (ADL)
2.4.4. Instrumental Activities of Daily Living (IADL)
2.4.5. Geriatric Depression Scale (GDS-15)
2.5. CHA₂DS₂-VASc Score for Atrial Fibrillation Stroke Risk
2.6. Statistical Analysis
3. Results
3.1. Study Population
3.2. Comparative Analysis of Biologic Parameters in Hypertensive Patients with/without AF
3.3. IMT, ABI, and Hemodynamic Parameters (SBP, DPB, HR) in Both Groups of Patients
3.4. Comparative Analysis of Echocardiographic Parameters of Left Ventricle Systolic Function in Both Groups of Patients
3.5. Comparative Analysis of Screening Tools for Cognitive Impairment, Daily Activity, and Depression Scalesin Both Groups of Patients
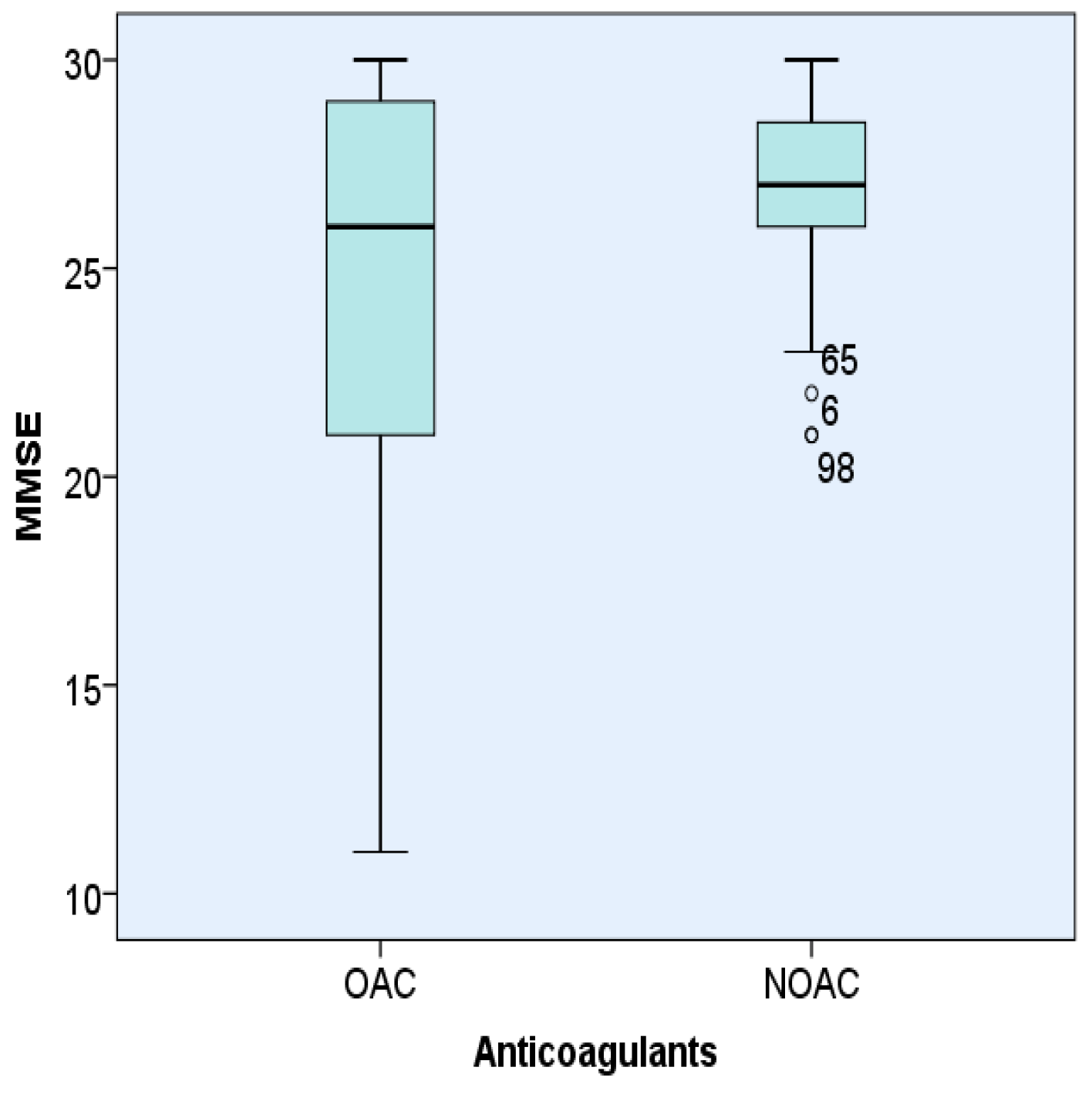
3.6. Comparative Analysis of Types of Anticoagulants Used in Hypertensive Patients with AF Patients on Screening Tools for Cognitive Impairment, Daily Activity, and Depression Scales, Subclinical Atherosclerosis, Hemodynamic and Echocardiographic Parameters
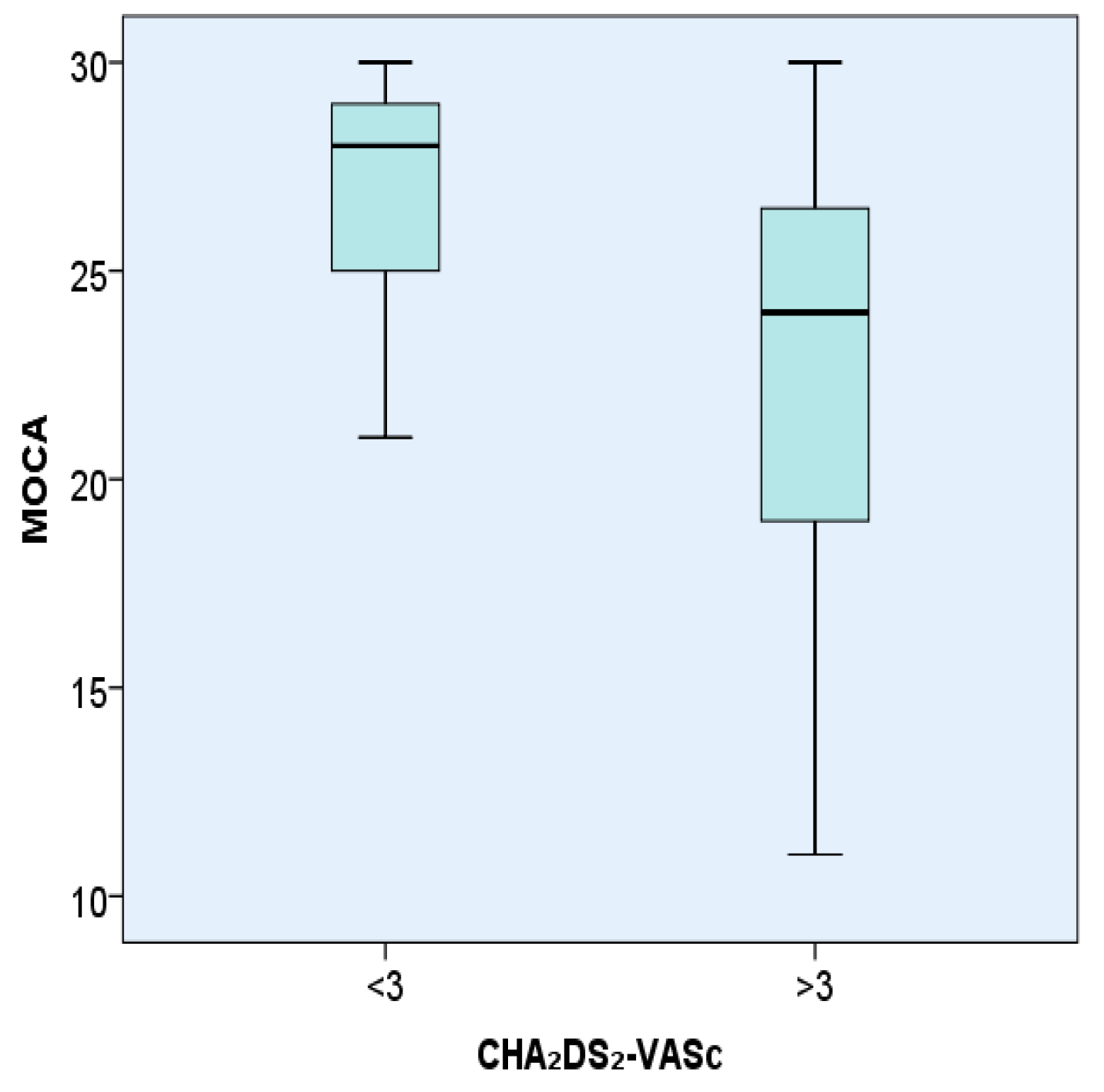
3.7. Comparative Analysis of CHA₂DS₂-VASc Score (</>3) in Patients with AF on Screening Tools for Cognitive Impairment, Daily Activity, and Depression Scales, Subclinical Atherosclerosis, Hemodynamic and Echocardiographic Parameters
3.8. Comparative Analysis of Age </>65 in Hypertensive Patients with AF on Screening Tools for Cognitive Impairment, Daily Activity, and Depression Scales, Subclinical Atherosclerosis, Hemodynamic and Echocardiographic Parameters
3.9. IMT and Screening Tools For Cognitive Impairment, Daily Activity, and Depression Scalesin Both Groups of Patients Adjusted for Age and Sex
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lopez, A.D.; Mathers, C.D.; Ezzati, M.; Jamison, D.T.; Murray, C.J. Global and regional burden of disease and risk factors, 2001: Systematic analysis of population health data. Lancet 2006, 367, 1747–1757. [Google Scholar] [CrossRef]
- Mills, K.T.; Bundy, J.D.; Kelly, T.N.; Reed, J.E.; Kearney, P.M.; Reynolds, K.; Chen, J.; He, J. Global disparities of hypertension prevalence and control: Asystematic analysis of population-based studies from 90 countries. Circulation 2016, 134, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Lewington, S.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R. Prospective Studies Collaboration. Age-specific relevance of usu-al blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002, 360, 1903–1913. [Google Scholar]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.F.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2020, 1125. [Google Scholar] [CrossRef]
- Dzeshka, M.S.; Shantsila, A.; Shantsila, E.; Lip, G.Y. Atrial Fibrillation and Hypertension. Hypertension 2017, 70, 854–861. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Himmelfarb, C.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ ASH/ASPC/NMA/PCNA Guideline for the Preven-tion, Detection, Evaluation, and Management of High Blood Pressure in Adults A Report of the American College of Cardi-ology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, e13–e115. [Google Scholar] [CrossRef]
- Gorelick, P.B.; Scuteri, A.; Black, S.; DeCarli, C.; Greenberg, S.M.; Iadecola, C.; Launer, L.J.; Laurent, S.; Lopez, O.L.; Nyenhuis, D.; et al. Vascular Contributions to Cognitive Impairment and Dementia. Stroke 2011, 42, 2672–2713. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Pokorney, S.D.; Hayden, K.M.; Welsh-Bohmer, K.; Newby, L.K. Cognitive Function: Is There More to Anticoagulation in Atrial Fibrillation Than Stroke? J. Am. Heart Assoc. 2015, 4, e001573. [Google Scholar] [CrossRef] [PubMed]
- Dublin, S.; Anderson, M.L.; Haneuse, S.J.; Heckbert, S.R.; Crane, P.K.; Breitner, J.C.S.; McCormick, W.; Bowen, J.D.; Teri, L.; McCurry, S.M.; et al. Atrial Fibrillation and Risk of Dementia: A Prospective Cohort Study. J. Am. Geriatr. Soc. 2011, 59, 1369–1375. [Google Scholar] [CrossRef]
- Alonso, A.; De Larriva, A.P.A. Atrial Fibrillation, Cognitive Decline and Dementia. Eur. Cardiol. Rev. 2016, 11, 49. [Google Scholar] [CrossRef]
- Ma, L. Depression, Anxiety, and Apathy in Mild Cognitive Impairment: Current Perspectives. Front. Aging Neurosci. 2020, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- Polikandrioti, M.; Koutelekos, I.; Vasilopoulos, G.; Gerogianni, G.; Gourni, M.; Zyga, S.; Panoutsopoulos, G. Anxiety and Depression in Patients with Permanent Atrial Fibrillation: Prevalence and Associated Factors. Cardiol. Res. Pract. 2018, 2018, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hugo, J.; Ganguli, M. Dementia and Cognitive Impairment. Clin. Geriatr. Med. 2014, 30, 421–442. [Google Scholar] [CrossRef]
- Aboyans, V.; Criqui, M.H.; Abraham, P.; Allison, M.; Creager, M.A.; Diehm, C.; Fowkes, F.G.R.; Hiatt, W.R.; Jönsson, B.; Lacroix, P.; et al. Measurement and Interpretation of the Ankle-Brachial Index. Circulation 2012, 126, 2890–2909. [Google Scholar] [CrossRef]
- Jozwiak, A.; Guzik, P.; Mathew, A.; Wykretowicz, A.; Wysocki, H. Association of atrial fibrillation and focal neurologic defi-cits with impaired cognitive function in hospitalized patients > or = 65 years of age. Am. J. Cardiol. 2006, 98, 1238–1241. [Google Scholar] [CrossRef]
- Pangman, V.C.; Sloan, J.; Guse, L. An examination of psychometric properties of the Mini-Mental State Examination and the Standardized Mini-Mental State Examination: Implications for clinical practice. Appl. Nurs. Res. 2000, 13, 209–213. [Google Scholar] [CrossRef]
- Tuijl, J.P.; Scholte, E.M.; De Craen, A.J.M.; Van Der Mast, R.C. Screening for cognitive impairment in older general hospital patients: Comparison of the six-item cognitive test with the Mini-Mental Status Examination. Int. J. Geriatr. Psychiatry 2012, 27, 755–762. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bedirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Noelker, L.S.; Browdie, R. Sidney Katz, MD: A New Paradigm for Chronic Illness and Long-Term Care. Gerontologist 2014, 54, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Graf, C. The Lawton Instrumental Activities of Daily Living Scale. AJN Am. J. Nurs. 2008, 108, 52–62. [Google Scholar] [CrossRef]
- Sheikh, J.I.; Yesavage, J.A. Geriatric Depression Scale [GDS]: Recent evidence and development of a shorter version. Clin. Gerontol. 1986, 5, 165–173. [Google Scholar]
- Lesher, E.L.; Berryhill, J.S. Validation of the geriatric depression scale-short form among inpatients. J. Clin. Psychol. 1994, 50, 256–260. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Akl, E.A.; Crowther, M.; Gutterman, D.D.; Schuünemann, H.J. Executive Summary. Chest 2012, 141, 7S–47S. [Google Scholar] [CrossRef] [PubMed]
- Verdecchia, P.; Angeli, F.; Reboldi, G. Hypertension and Atrial Fibrillation, Doubts and Certainties from Basic and Clinical Studies. Circ. Res. 2018, 122, 352–368. [Google Scholar] [CrossRef]
- Verdecchia, P.; Mazzotta, G.; Angeli, F.; Reboldi, G. Above which blood pressure level does the risk of atrial fibrillation in-crease? Hypertension 2012, 59, 184–185. [Google Scholar] [CrossRef]
- Thomas, M.C.; Dublin, S.; Kaplan, R.C.; Glazer, N.; Lumley, T.; Longstreth, W.T.; Smith, N.L.; Psaty, B.M.; Siscovick, D.S.; Heckbert, S.R. Blood Pressure Control and Risk of Incident Atrial Fibrillation. Am. J. Hypertens. 2008, 21, 1111–1116. [Google Scholar] [CrossRef]
- Verdecchia, P.; Angeli, F.; Gentile, G.; Reboldi, G. More versus less intensive blood pressure-lowering strategy: Cumulative evidence and trial sequential analysis. Hypertension 2016, 68, 642–653. [Google Scholar] [CrossRef] [PubMed]
- Annoura, M.; Ogawa, M.; Kumagai, K.; Zhang, B.; Saku, K.; Arakawa, K. Cholesterol Paradox in Patients with Paroxysmal Atrial Fibrillation. Cardiology 1999, 92, 21–27. [Google Scholar] [CrossRef]
- Li, Z.Z.; Du, X.; Guo, X.X.; Tang, R.B.; Jiang, C.; Nian Liu, N.; Chang, S.S.; Yu, R.H.; Long, D.-y.; Bai, R.; et al. Association Between Blood Lipid Profiles and Atrial Fibrillation: A Case-Control Study. Med. Sci. Monit. 2018, 24, 3903–3908. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Bigger, J.T.; Hickey, K.T.; Chen, H.; Lopez-Jimenez, C.; Banerji, M.A.; Evans, G.; Fleg, J.L.; Papademetriou, V.; Thomas, A.; et al. Effect of Intensive Blood Pressure Lowering on Incident Atrial Fibrillation and P-Wave Indices in the ACCORD Blood Pressure Trial. Am. J. Hypertens. 2015, 29, 1276–1282. [Google Scholar] [CrossRef]
- Martínez-González, M.Á.; Toledo, E.; Arós, F.; Fiol, M.; Corella, D.; Salas-Salvadó, J.; Ros, E.; Covas, M.I.; Fernández-Crehuet, J.; Lapetra, J.; et al. Extra-virgin olive oil consumption reduces risk of atrial fibrillation: The PREDIMED trial. Circulation 2014, 130, 18–26. [Google Scholar] [CrossRef]
- Ramdas, G.P.; Padmini, V. Prognostic significance of atrial fibrillation is a function of left ventricular ejection fraction. Clin. Cardiol. 2007, 30, 349–354. [Google Scholar]
- Benjamin, E.J.; Levy, D.; Vaziri, S.M.; D’Agostino, R.B.; Belanger, A.J.; Wolf, P.A. Independent risk factors for atrial fibrillation in a population-based cohort. The Framingham Heart Study. JAMA 1994, 271, 840–844. [Google Scholar] [CrossRef] [PubMed]
- Cha, Y.-M.; Redfield, M.M.; Shen, W.-K.; Gersh, B.J. Atrial Fibrillation and Ventricular Dysfunction. Circulation 2004, 109, 2839–2843. [Google Scholar] [CrossRef]
- Polak, J.F.; Pencina, M.J.; O’Leary, D.H.; D’Agostino, R.B. Common Carotid Artery Intima-Media Thickness Progression as a Predictor of Stroke in Multi-Ethnic Study of Atherosclerosis. Stroke 2011, 42, 3017–3021. [Google Scholar] [CrossRef] [PubMed]
- Nambi, V.; Chambless, L.; Folsom, A.R.; He, M.; Hu, Y.; Mosley, T.; Volcik, K.; Boerwinkle, E.; Ballantyne, C.M. Carotid in-tima-media thickness and presence or absence of plaque improves prediction of coronary heart disease risk: The ARIC (Ath-erosclerosis Risk In Communities) study. J. Am. Coll. Cardiol. 2010, 55, 1600–1607. [Google Scholar] [CrossRef] [PubMed]
- Tran, L.T.T.; Park, H.-J.; Kim, H.-D. Is the carotid intima-media thickness really a good surrogate marker of atherosclerosis? J. Atheroscler. Thromb. 2012, 19, 680–690. [Google Scholar] [CrossRef]
- Eryd, S.A.; Östling, G.; Rosvall, M.; Persson, M.; Smith, J.G.; Melander, O.; Hedblad, B.; Engström, G. Carotid intima-media thickness is associated with incidence of hospitalized atrial fibrillation. Atherosclerosis 2014, 233, 673–678. [Google Scholar] [CrossRef]
- Kokubo, Y.; Watanabe, M.; Higashiyama, A.; Nakao, Y.M.; Nakamura, F.; Miyamoto, Y. Impact of Intima-Media Thickness Progression in the Common Carotid Arteries on the Risk of Incident Cardiovascular Disease in the Suita Study. J. Am. Heart Assoc. 2018, 7, e007720. [Google Scholar] [CrossRef]
- Willeit, K.; Kiechl, S. Atherosclerosis and atrial fibrillation—Two closely intertwined diseases. Atherosclerosis 2014, 233, 679–681. [Google Scholar] [CrossRef]
- Chen, L.Y.; Foo, D.C.; Wong, R.C.; Seow, S.-C.; Gong, L.; Benditt, D.G.; Ling, L.H. Increased carotid intima-media thickness and arterial stiffness are associated with lone atrial fibrillation. Int. J. Cardiol. 2013, 168, 3132–3134. [Google Scholar] [CrossRef]
- Heeringa, J.; Van Der Kuip, D.A.M.; Hofman, A.; Kors, J.A.; Van Rooij, F.J.A.; Greg, Y.; Lip, H.; Wirreman, J.C.M. Subclinical Atherosclerosis and Risk of Atrial Fibrillation the Rotterdam Study. Arch. Intern. Med. 2007, 167, 382–387. [Google Scholar] [CrossRef]
- Dąbrowski, M.; Lewandowski, J.; Abramczyk, P.; Łoń, I.; Gaciong, Z.; Siński, M. Atrial fibrillation does not affect an-kle-brachial index measured using the Doppler method. Hypertens. Res. 2018, 41, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Ricco, J.-B.; Bartelink, M.-L.E.L.; Björck, M.; Brodmann, M.; Cohnert, T.; Collet, J.-P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2017, 39, 763–816. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-S.; Tung, T.-H.; Wang, J.; Chen, Y.-F.; Chen, T.-H.; Lin, M.-S.; Chi, C.-C.; Chen, M.-C. Peripheral arterial disease and atrial fibrillation and risk of stroke, heart failure hospitalization and cardiovascular death: A nationwide cohort study. Int. J. Cardiol. 2016, 203, 204–211. [Google Scholar] [CrossRef]
- Bekwelem, W.; Norby, F.L.; Agarwal, S.K.; Matsushita, K.; Coresh, J.; Alonso, A.; Chen, L. Association of Peripheral Artery Disease With Incident Atrial Fibrillation: The ARIC (Atherosclerosis Risk in Communities) Study. J. Am. Heart Assoc. 2018, 7, e007452. [Google Scholar] [CrossRef] [PubMed]
- Proietti, M.; Farcomeni, A. Association Between Peripheral Artery Disease and Incident Risk of Atrial Fibrillation: Strong Evidence Coming From Population-Based Cohort Studies. J. Am. Heart Assoc. 2018, 7, e009126. [Google Scholar] [CrossRef] [PubMed]
- O’Neal, W.T.; Efird, J.T.; Nazarian, S.; Alonso, A.; Heckbert, S.R.; Soliman, E.Z. Peripheral Arterial Disease and Risk of Atrial Fibrillation and Stroke: The Multi-Ethnic Study of Atherosclerosis. J. Am. Heart Assoc. 2014, 3, e001270. [Google Scholar] [CrossRef]
- Griffin, W.F.; Salahuddin, T.; O’Neal, W.T.; Soliman, E.Z. Peripheral arterial disease is associated with an increased risk of atrial fibrillation in the elderly. Europace 2016, 18, 794–798. [Google Scholar] [CrossRef] [PubMed]
- Naranjoa, I.C.; Portilla Cuenca, J.C.; Duque De San Juana, B.; Garcia, A.F.; Sevillaa, R.R.; Serrano Cabreraa, A.; Camara Hijonb, C.; Romero Chalab, S.; Fuentesc, J.M.; Ramirez Morenod, J.M. Association of Vascular Factors and Amnestic Mild Cognitive Impairment: A Comprehensive Approach. J. Alzheimers Dis. 2015, 44, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Alonso, A.; Knopman, D.S.; Gottesman, R.F.; Soliman, E.Z.; Shah, A.J.; O’Neal, W.T.; Norby, F.; Mosley, T.H.; Chen, L. Correlates of Dementia and Mild Cognitive Impairment in Patients with Atrial Fibrillation: The Atherosclerosis Risk in Communities Neurocognitive Study (ARIC-NCS). J. Am. Heart Assoc. 2017, 6, 006014. [Google Scholar] [CrossRef] [PubMed]
- Mizrahi, E.H.; Waitzman, A.; Marina, A.M.; Adunsky, A. Atrial Fibrillation Predicts Cognitive Impairment in Patients With Ischemic Stroke. Am. J. Alzheimers Dis. Other Dement. 2011, 26, 623–626. [Google Scholar] [CrossRef] [PubMed]
- De Bruijn, R.F.A.G.; Heeringa, J.; Wolters, F.J.; Franco, O.H.; Stricker, B.H.C.; Hofman, A.; Koudstaal, P.J.; Ikram, M.A. Association Between Atrial Fibrillation and Dementia in the General Population. JAMA Neurol. 2015, 72, 1288–1294. [Google Scholar] [CrossRef]
- Rivard, L.; Khairy, P. Mechanisms, Clinical Significance, and Prevention of Cognitive Impairment in Patients with Atrial Fibrillation. Can. J. Cardiol. 2017, 33, 1556–1564. [Google Scholar] [CrossRef] [PubMed]
- Kalantarian, S.; Stern, T.A.; Mansour, M.; Ruskin, J.N. Cognitive impairment associated with atrial fibrillation: A meta-analysis. Ann. Intern. Med. 2013, 158, 338–346. [Google Scholar] [CrossRef]
- Zulkifly, M.F.M.; Ghazali, S.E.; Din, N.C.; Singh, D.K.A.; Subramaniam, P. A Review of Risk Factors for Cognitive Impairment in Stroke Survivors. Sci. World J. 2016, 2016, 1–16. [Google Scholar] [CrossRef]
- Thacker, E.L.; McKnight, B.; Psaty, B.M.; Longstreth, W.T.; HColeen, J.R.; Sitlani, M.; Dublin, S.; Arnold, A.M.; Fitzpatrick, A.L.; Gotterman, R.F.; et al. Atrial fibrillation and cognitive decline, A longitudinal cohort study. Neurology 2013, 81, 119–125. [Google Scholar] [CrossRef]
- Alosco, M.L.; Spitznagel, M.B.; Sweet, L.H.; Josephson, R.; Hughes, J.; Gunstad, J. Atrial Fibrillation Exacerbates Cognitive Dysfunction and Cerebral Perfusion in Heart Failure. Pacing Clin. Electrophysiol. 2015, 38, 178–186. [Google Scholar] [CrossRef]
- Knecht, S.; Oelschläger, C.; Duning, T.; Lohmann, H.; Albers, J.; Stehling, C.; Heindel, W.; Breithardt, G.; Berger, K.; Ringelstein, E.B.; et al. Atrial fibrillation in stroke-free patients is associated with memory impairment and hippocampal atrophy. Eur. Heart J. 2008, 29, 2125–2132. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.S.; Morley, J.E.; Mikolajczak, P.C.; Lee, R. Atrial fibrillation: A major risk factor for cognitive decline. Am. Heart J. 2015, 169, 448–456. [Google Scholar] [CrossRef] [PubMed]
- Amaricăi, E.; Poenaru, D.V. The post-stroke depression and its impact on functioning in young and adult stroke patients of a rehabilitation unit. J. Ment. Health 2015, 25, 137–141. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depres-sion screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Cahn-Weiner, D.A.; Farias, S.T.; Julian, L.; Harvey, D.J.; Kramer, J.H.; Reed, B.R.; Mungas, D.; Wetzel, M.; Chui, H. Cognitive and neuroimaging predictors of instrumental activities of daily living. J. Int. Neuropsychol. Soc. 2007, 13, 747–757. [Google Scholar] [CrossRef]
- Steenland, K.; Karnes, C.; Seals, R.; Carnevale, C.; Hermida, A.; Levey, A. Late-life depression as a risk factor for mild cogni-tive impairment or Alzheimer’s disease in 30 US Alzheimer’s disease centers. J. Alzheimers Dis. 2012, 31, 265–275. [Google Scholar] [CrossRef]
- Richard, E.; Reitz, C.; Honing, L.H.; Sschupf, N.; Tang, M.X.; Mantly, J.J.; Mayeux, R.; Devanand, D.; Luchsinger, J.A. Late-life depression, mild cognitive impairment, and dementia. JAMA Neurol. 2013, 70, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.Y.; Agarwal, S.K.; Norby, F.L.; Gottesman, R.F.; Loehr, L.R.; Soliman, E.Z.; Mosley, T.H.; Folsom, A.R.; Coresh, J.; Alonso, A. Persistent but not paroxysmal atrial fibrillation is independently associated with lower cognitive function: The Atherosclerosis Risk in Communities [ARIC] Study. J. Am. Coll. Cardiol. 2016, 67, 1379–1380. [Google Scholar] [CrossRef]
- Jacobs, V.; Woller, S.C.; Stevens, S.M.; May, H.T.; Bair, T.L.; Crandall, B.G.; Cutler, M.; Day, J.D.; Weiss, J.P.; Osborn, J.S.; et al. Percent Time With a Supratherapeutic INR in Atrial Fibrillation Patients Also Using an Antiplatelet Agent Is Associated With Long-Term Risk of Dementia. J. Cardiovasc. Electrophysiol. 2015, 26, 1180–1186. [Google Scholar] [CrossRef]
- Ball, J.; Carrington, M.J.; Stewart, S. On behalf of the SAFETY investigators, Mild cognitive impairment in high-risk patients with chronic atrial fibrillation: A forgotten component of clinical management? Heart 2013, 99, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Poels, M.M.; Vernooij, M.W.; Ikram, M.A.; Hofman, A.; Krestin, G.P.; van der Lugt, A.; Breteler, M.M. Prevalence and risk factors of cerebral microbleeds: An update of the Rotter-dam scan study. Stroke 2010, 41, S103–S106. [Google Scholar] [CrossRef] [PubMed]
- Akoudad, S.; Darweesh, S.K.; Leening, M.J.; Koudstaal, P.J.; Hofman, A.; Van Der Lugt, A.; Stricker, B.H.; Ikram, M.A.; Vernooij, M.W. Use of Coumarin Anticoagulants and Cerebral Microbleeds in the General Population. Stroke 2014, 45, 3436–3439. [Google Scholar] [CrossRef] [PubMed]
- Ott, A.; Breteler, M.M.; De Bruyne, M.C.; Van Harskamp, F.; Grobbee, D.E.; Hofman, A. Atrial fibrillation and dementia in a population-based study: The Rotterdam Study. Stroke 1997, 28, 316–321. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patients Demographic Data | All Patients Included in the Study | 84 Hypertensive Patients with AF | 71 Hypertensive Patients without AF |
|---|---|---|---|
| Number of patients/% Mean ± SD | Number of patients/% Mean ± SD | Number of patients/% Mean ± SD | |
| Age | 155/69.98 ± 9.89 | 84/54.2/73.88 ± 9.78 | 71/45.80/68.00 ± 9.23 |
| Age < 65 | 45/29.0/59.38 ± 5.78 | 18/21.4/59.61 ± 5.82 | 27/38.0/59.22 ± 5.86 |
| Age > 65 | 110/71.0/76.02 ± 6.72 | 66/78.6/77.77 ± 6.45 | 44/62.0/73.39 ± 72.0 |
| Sex/Male/Age | 72/46.5/69.82 ± 10.00 | 36/42.9/72.61 ± 10.08 | 36/50.7/67.03 ± 9.24 |
| Sex/Female/Age | 83/53.5/72.37 ± 9.80 | 48/57.1/74.83 ± 9.54 | 35/49.3/69.00 ± 9.25 |
| Diabetes mellitus | 46/29.7 | 21/25.0 | 25/35.2 |
| Smoking | 49/31.6 | 24/28.6 | 25/35.2 |
| Hyperlipemia | 83/53.5 | 42/50.0 | 41/57.7 |
| Obesity | 25/16.1 | 10/11.9 | 15/21.1 |
| Chronic kidney disease | 38/24.5 | 26/31.0 | 12/16.9 |
| Peripheral arterial disease | 10/6.5 | 4/4.6 | 6/8.5 |
| Coronary disease | 68/43.9 | 38/45.2 | 30/42.3 |
| Heart failure | 68/43.9 | 41/48.8 | 27/38.0 |
| Lacunar stroke | 51/32.9 | 26/31.0 | 25/35.2 |
| Minor stroke | 22/14.2 | 15/17.9 | 7/9.9 |
| Biologic Parameter | All Patients | 84 Hypertensive Patients with AF | 71 Hypertensive Patients without AF | p-Value * | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| Hemoglobin (g/dL) | 13.85 | 1.94 | 13.57 | 2.07 | 14.18 | 1.72 | 0.049 |
| Hematocrit (%) | 41.47 | 5.18 | 40.78 | 5.69 | 2.29 | 4.42 | 0.066 |
| ESR (mm/h) | 22.03 | 15.89 | 21.75 | 16.09 | 22.38 | 15,76 | 0.807 |
| Thrombocytes x103/µL | 227.29 | 58.90 | 222.83 | 60.15 | 232.56 | 57.36 | 0.037 |
| APTT(s) | 27.74 | 6.70 | 28.87 | 7.97 | 26.41 | 4.46 | 0.017 |
| INR | 1.95 | 0.78 | 1.86 | 0.86 | 2.05 | 0.68 | 0.135 |
| PT (s) | 24.63 | 10.69 | 24.17 | 11.09 | 25.17 | 10.26 | 0.564 |
| PT (%) | 57.46 | 29.43 | 60.72 | 29.87 | 53.60 | 28.63 | 0.134 |
| Total Cholesterol (mg/dL) | 183.86 | 60.48 | 170.17 | 54.50 | 200.05 | 63.51 | 0.002 |
| LDL Cholesterol (mg/dL) | 131.30 | 52.52 | 121.30 | 47.06 | 143.14 | 56.39 | 0.011 |
| HDL Cholesterol (mg/dL) | 47.98 | 18.14 | 45.90 | 12.06 | 50.43 | 23.24 | 0.141 |
| TG (mg/dL)I | 130.91 | 56.98 | 123.29 | 47.62 | 139.92 | 65.58 | 0.078 |
| Glycemia (mg/dL) | 110.02 | 30.34 | 109.25 | 35.68 | 110.94 | 22.67 | 0.730 |
| Urea (mg/dL) | 41.85 | 17.93 | 43.58 | 20.97 | 39.80 | 13.33 | 0.176 |
| Creatinine (mg/dL) | 0.98 | 0.24 | 1.04 | 0.23 | 0.91 | 0.23 | 0.001 |
| ALT (U/L) | 29.89 | 20.74 | 32.77 | 26.23 | 26.49 | 10.44 | 0.046 |
| AST (U/L) | 26.05 | 17.80 | 29.22 | 22.91 | 22.30 | 6.97 | 0.010 |
| CKMB (U/L) | 17.03 | 8.98 | 18.59 | 11.02 | 15.18 | 5.22 | 0.013 |
| K (mmol/L) | 4.11 | 0.43 | 4.05 | 0.48 | 4.18 | 0.35 | 0.065 |
| Na (mmol/L) | 140.77 | 2.58 | 140.87 | 2.64 | 140.64 | 2.51 | 0.583 |
| Uric acid (mg/dL) | 6.26 | 1.56 | 6.38 | 1.64 | 6.11 | 1.45 | 0.280 |
| Hemodynamic Parameters | All Patients | 84 Hypertensive Patients with AF | 71 Hypertensive Patients without AF | p-Value* | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||||
| SBP (mmHg) | 132.06 | 19.97 | 136.31 | 22.61 | 127.04 | 14.96 | 0.003 |
| DBP (mmHg) | 78.16 | 14.32 | 80.71 | 14.16 | 75.14 | 14.01 | 0.015 |
| HR (b/min) | 74.93 | 15.44 | 76.68 | 17.50 | 72.86 | 12.38 | 0.115 |
| IMT (mm)left | 0.69 | 0.27 | 0.75 | 0.27 | 0.63 | 0.26 | 0.005 |
| IMT (mm) right | 0.67 | 0.30 | 0.75 | 0.32 | 0.59 | 0.26 | 0.001 |
| ABI left | 1.10 | 0.14 | 1.09 | 0.10 | 1.11 | 0.17 | 0.434 |
| ABI right | 1.10 | 0.14 | 1.09 | 0.16 | 1.08 | 0.12 | 0.625 |
| Echocardiographic Parameters | All Patients | 84 Hypertensive Patients with AF | 71 Hypertensive Patients without AF | p-Value * | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| IVS (mm) | 11.99 | 2.11 | 12.26 | 1.90 | 11.68 | 2.31 | 0.087 |
| LA (mm) | 41.37 | 6.25 | 43.25 | 6.50 | 39.15 | 5.15 | <0.001 |
| LVPW (mm) | 12.08 | 2.50 | 11.95 | 2.34 | 12.24 | 2.70 | 0.509 |
| LVESD (mm) | 24.29 | 6.67 | 23.96 | 7.18 | 24.67 | 6.04 | 0.510 |
| LVEDD (mm) | 46.51 | 5.33 | 47.83 | 5.84 | 44.95 | 4.19 | 0.001 |
| LVESV (mL) | 35.83 | 13.81 | 37.76 | 15.02 | 33.56 | 11.94 | 0.059 |
| LVEDV (mL) | 76.75 | 19.28 | 78.35 | 19.88 | 74.85 | 18.51 | 0.262 |
| LVEF (%) | 57.51 | 6.92 | 56.29 | 7.77 | 58.95 | 5.45 | 0.014 |
| E (m/s) | 0.71 | 0.18 | 0.74 | 11.820.19 | 0.69 | 0.17 | 0.084 |
| PSAP (mmHg) | 39.13 | 11.66 | 42.23 | 35.46 | 10.41 | <0.001 | |
| Screening Tools for Cognitive Impairment, Daily Activity and Depression Scales | All Patients | 84 Hypertensive Patients with AF | 71 Hypertensive Patients without AF | p-Value* | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| MMSE | 26.29 | 4.47 | 25.15 | 4.92 | 27.63 | 3.46 | <0.001 |
| MoCA | 24.35 | 5.37 | 23.44 | 5.50 | 25.42 | 5.04 | 0.022 |
| ADL | 9.42 | 1.03 | 9.69 | 0.78 | 9.19 | 1.18 | 0.002 |
| IADL | 6.72 | 1.77 | 7.18 | 1.34 | 6.33 | 1.99 | 0.002 |
| GDS-15 | 6.65 | 2.30 | 7.08 | 2.29 | 6.15 | 2.23 | 0.012 |
| Hypertensive and AF Patients | Patients with CHA₂DS₂-VASc <3 | Patients with CHA₂DS₂-VASc >3 | p |
|---|---|---|---|
| Screening tools for cognitive impairment, daily activity, and depression scales | Mean ± SD | Mean ± SD | |
| MMSE | 27.81 ± 2.04 | 24.27 ± 5.28 | <0.001 |
| MoCA | 26.81 ± 2.78 | 22.32 ± 5.73 | <0.001 |
| ADL | 8.95 ± 1.27 | 9.90 ± 0.30 | 0.001 |
| IADL | 6.08 ± 2.16 | 7.10 ± 1.04 | 0.006 |
| GDS-15 | 5.76 ± 2.02 | 7.52 ± 2.22 | 0.002 |
| Variable Analyzed Adjusted for Age and Sex | 84 Hypertensive Patients with AF | 71 Hypertensive Patients without AF | p-Value* | ||
|---|---|---|---|---|---|
| Mean | Std.Error | Mean | Std. Error | ||
| IMT (mm) left adjusted for age IMT (mm) left adjusted for sex | 0.740 0.750 | 0.030 0.030 | 0.650 0.630 | 0.030 0.030 | 0.009 0.842 |
| IMT (mm) right adjusted for age IMT (mm) right adjusted for sex | 0.730 0.750 | 0.030 0.030 | 0.610 0.590 | 0.030 0.040 | 0.015 0.205 |
| MMSE adjusted for age MMSE adjusted for sex | 25.567 25.132 | 0.455 0.472 | 27.147 27.661 | 0.496 0.472 | <0.001 0.363 |
| MoCA adjusted for age MoCA adjusted for sex | 23.764 23.403 | 0.578 0.578 | 25.040 25.467 | 0.631 0.629 | 0.007 0.223 |
| ADL adjusted for age ADL adjusted for sex | 9.602 9.691 | 0.119 0.120 | 9.265 9.190 | 0.109 0.111 | 0.001 0.911 |
| IADL adjusted for age IADL adjusted for sex | 7.036 7.202 | 0.204 0.204 | 6.458 6.318 | 0.187 0.188 | 0.001 0.121 |
| GDS-15 adjusted for age GDS-15 adjusted for sex | 6.873 7.095 | 0.239 0.248 | 6.404 6.141 | 0.261 0.270 | <0.001 0.378 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Militaru, M.; Rachieru, C.; Lighezan, D.F.; Militaru, A.G. The Impact of Hypertension and Atrial Fibrillation on Cognitive Decline and Subclinical Atherosclerosis. Brain Sci. 2021, 11, 752. https://doi.org/10.3390/brainsci11060752
Militaru M, Rachieru C, Lighezan DF, Militaru AG. The Impact of Hypertension and Atrial Fibrillation on Cognitive Decline and Subclinical Atherosclerosis. Brain Sciences. 2021; 11(6):752. https://doi.org/10.3390/brainsci11060752
Chicago/Turabian StyleMilitaru, Marius, Ciprian Rachieru, Daniel Florin Lighezan, and Anda Gabriela Militaru. 2021. "The Impact of Hypertension and Atrial Fibrillation on Cognitive Decline and Subclinical Atherosclerosis" Brain Sciences 11, no. 6: 752. https://doi.org/10.3390/brainsci11060752
APA StyleMilitaru, M., Rachieru, C., Lighezan, D. F., & Militaru, A. G. (2021). The Impact of Hypertension and Atrial Fibrillation on Cognitive Decline and Subclinical Atherosclerosis. Brain Sciences, 11(6), 752. https://doi.org/10.3390/brainsci11060752