
Mindfulness-Based Interventions for Physical and Psychological Wellbeing in Cardiovascular Diseases: A Systematic Review and Meta-Analysis


 ,
, 

Abstract
1. Introduction
2. Materials and Methods
Meta-Analyses
3. Results
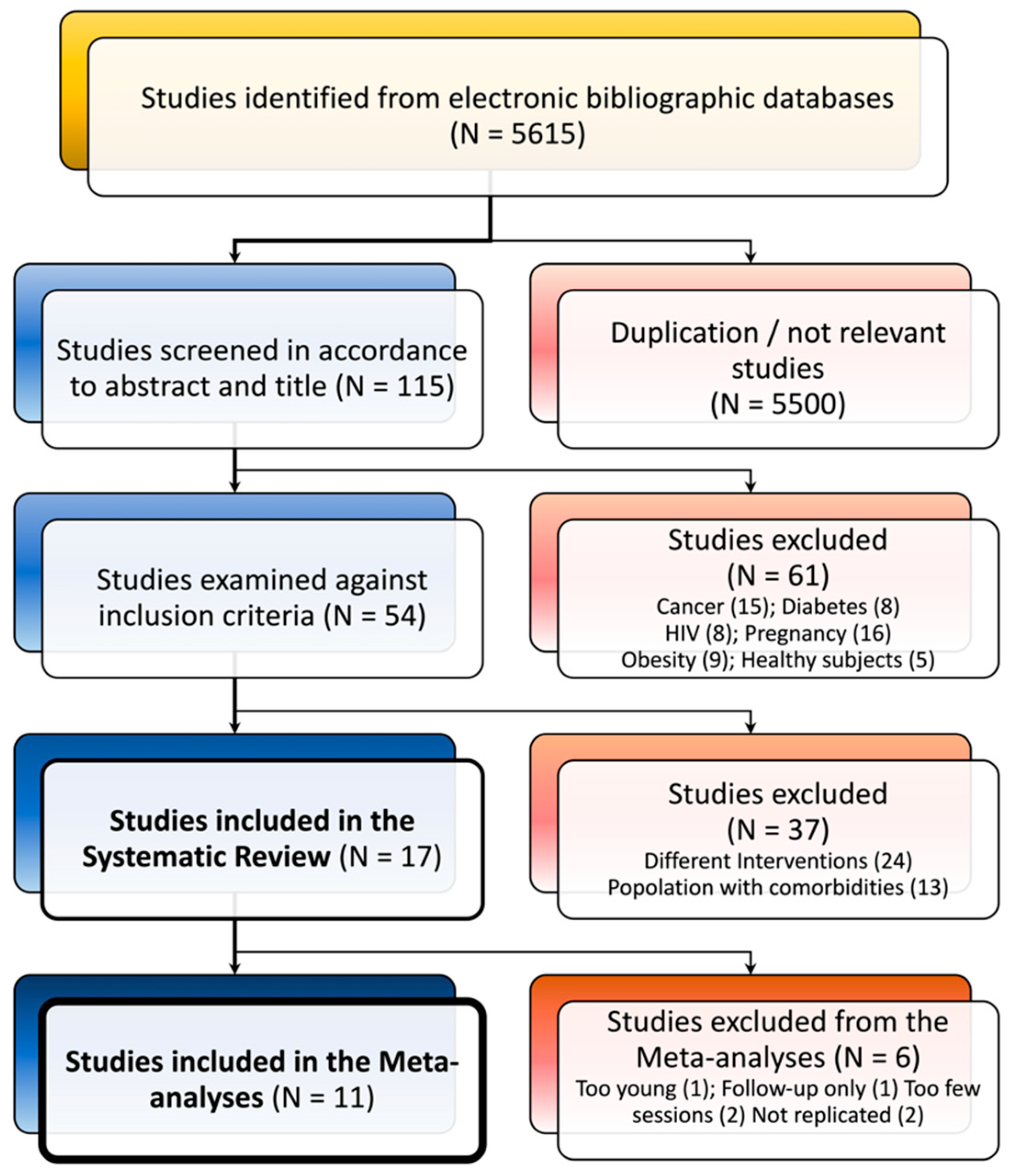
3.1. Study Selection
3.2. Study and Sample Characteristics
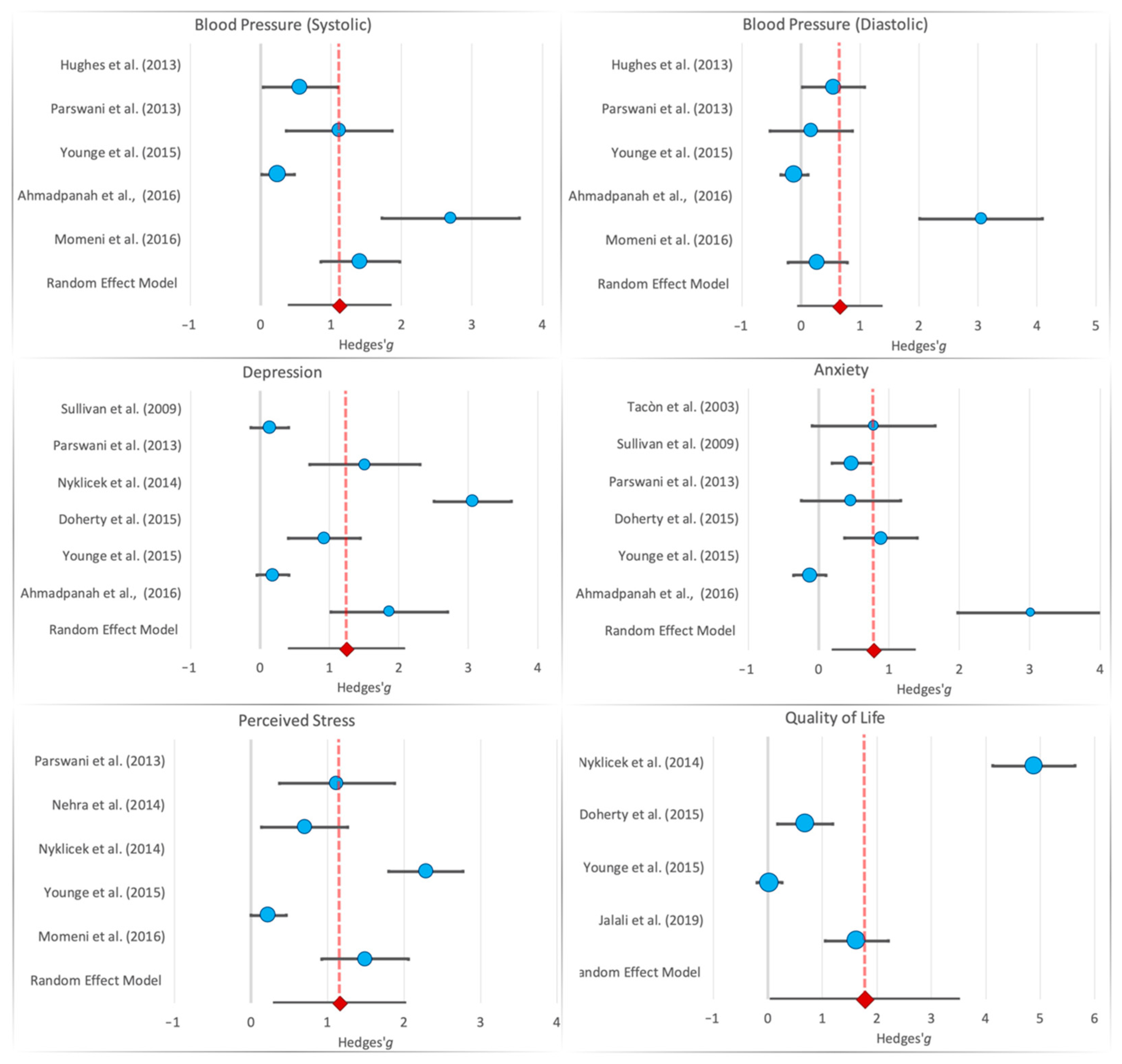
3.3. Mindfulness and Physical Outcomes

{kind=link}
{kind=link}
| Reference | Sample | Country | Intervention | Cardiological Disorders | Physiological Measures | Psychological Measures | Main Findings |
|---|---|---|---|---|---|---|---|
| Ahmadpanah et al. (2016) [9] | MDM (n 15 female; Age: 46.3 year) SMT (n 15 female; Age: 46.5 year) Control Group (n 15 female; Age: 46.5 year) | IRAN | MDM group: 8 weekly sessions; lasting 1 h STM group: 8 weekly sessions, lasting 1 h Control Group: brief medical check once a week for 8 weeks | HT | BP | BDI BAI | MDM and SMT treatments produced improvements in symptoms of anxiety and depression and reduced BP |
| Doherty et al. (2015) [10] | Treatment Group: n 32 (12 women and 19 men; mean age: 57.6 year) Control Group: 30 (8 women and 22 men mean age: 59.6 year) | IRELAND | MBCT group: 8 weekly sessions; each lasted 2 h Control Group: waiting list. Received no psychological intervention until Time 3, when they were offered MBCT. All participants were assessed at baseline (Time 1), 8 weeks later (Time 2), and at 6-month follow-up (Time 3) | CHT | HADS BSI POMS PAIS MAAS PQ CSQ | MCBT showed significant improvement rates in clinical depression. | |
| Freedenberg et al. (2017) * (adolescents) [21] | Treatment group: 26 (18 women and 8 men; mean age: 15.1 year) Video Online Group: 20 (11 women and 9 men; mean Age: 14.5 year) | USA | MBSR group: 6 weekly sessions each lasted an hour and a half Control Group: video online support group met for six consecutive weekly one-hour session | Congenital Cardiac Diagnoses Cardiac device or postural orthostatic tachycardia syndrome | HADS RSQ | MBSR intervention did not induce significant improvements in anxiety and depression scores | |
| Gotink et al. (2017) * (follow-up) [22] | MBSR group: (n 215; 44.2% female and 55.8% male; mean age: 43.2 year) Control Group: (n 109; 50.5% female and 49.5% male; mean Age: 43.2 year) | JAPAN | MBSR group: 12 weekly sessions online Control Group: usual care by their treating cardiologist | Heart disease | BP Heart rate Respiratory rate Cortisol level | SFHS Visual Analogue Scale Hospital Anxiety and Depression scale Perceived Stress Scale Perceived Social Support Scale | Exercise capacity, systolic blood pressure, mental functioning, and depression improved significantly compared to UC |
| Grant et al. (2013) * (not an intervention protocol) [23] | MBI group: 48 (50% female) Control Group: 49 (57.1% female and 42.9% male) | ALBANY | MA: focused-breathing exercise Control Group: no breathing exercise | Hypertension | Systolic and Diastolic BP Heart rate | There were no group differences in reactivity to either stressor. Participants in the mindfulness-analog condition experienced significantly greater latency to systolic blood pressure recovery following the CPT and a tendency toward greater latency to diastolic blood pressure recovery | |
| Hughes et al. (2013) [26] | MBSR Group (n 28; 61% women; mean age: 51.2 year Control Group: (n 28; 54% women; mean age: 49.5 year) | UK | MBSR Group: 8 weekly sessions; each lasted 2.5 h Control Group: progressive muscle relaxation (PMR) 8 weekly sessions; each lasted 2.5 h | Prehypertension | Systolic and Diastolic BP | MBSR is effective in lowering Systolic and Diastolic BPe in prehypertensive individuals. | |
| Jalali et al. (2019) [30] | MBSR group: (n 30; 50% female) Control group (n 30, 50% female) | IRAN | MBSR group: 8 weekly sessions each lasted 2 h Control Group: routine medical care | Cardiovascular disease | Self-Efficacy (General Self-Efficacy Scale) Quality of life (Short Form Survey) | MBSR program led to a stable improvement of the scores of self-efficacy and quality of life in the experimental group | |
| Momeni et al. (2016) [28] | MBRS group (n 30 13 female and 17 male Age: 49.2 year) Control Group (n 30 12 female and 18 male; Age: 46.2 year | IRAN | MBSR group: 8 weekly sessions lasting 2.5 h Control Group: receive no psychological therapy, waiting list | Cardiovascular disease | BP AOBP | PSS-14 STAI-X | MBSR helps people to deal with stress, pain, and illness more effectively and play a more active role in their lives and recovery. MBSR was also effective in reducing cardiac patients’ BP, perceived stress, and anger. |
| Nehra et al. (2014) [13] | MBRS group (n 25) Control Group (n 25) | INDIA | MBSR group: 8 weekly sessions lasting 2 h Control Group: Standard treatment | Coronary heart disease | PSS HCS | MBSR is highly effective in reducing perceived stress and health complaints in CHD patients. | |
| Norman et al. (2018) [29] * (not yet replicated measures) | MBI group: n 22 (11 female and 11 male; Mean Age: 76.5 year) Control Group: n 18 (6 female and 12 male; Mean Age: 75.0 year) | Sweden | MBI group: 8-weekly educational and training sessions lasting 2 h Control group: received usual care comprising standard health care for patients with CHF | CHF | Heart rate Respiratory rate Fatigue severity scale Karolinska Sleep Questionnaire Unsteadiness/dizziness | MBI is effective in reducing the self-reported impact of fatigue on daily living, unsteadiness/dizziness, and breathlessness/tiredness related to physical function | |
| Nyklıcek et al. (2014) [31] | MBRS group n 55 (10 female and 45 male; Mean Age: 55.4 year) Mindfulness Self-Help Control Group n 52 (9 female and 43 male; Mean Age: 56.3 year) | USA | MBSR: group: 3 weekly meetings (lasting 90–120 min) with an additional evaluation session 2 weeks later). Mindfulness Self-Help Control Group: Participants receiving the self-help booklet were asked to thoroughly read the theory and to practice exercises daily | PCI | SAD-4 PSS GMS The World Health Organization Quality of Life-Brief Questionnaire SAQ FMI-s | The group mindfulness intervention reduced perceived stress and symptoms of anxiety and depression more strongly than the control group in the relatively younger subsample. | |
| Owens et al. (2016) [25] * (not yet replicated measures) | 17 female and 3 male; Mean Age: 49.4 year | USA | MBSR group: 8 weekly sessions lasting 2.5 h Control Group: Waiting list control | Palpitations | Heart palpitations | MBSR participants reported a significant reduction in heart palpitations, and this improvement in the MBSR participants was sustained at 1-month follow-up. | |
| Parswani et al. (2013) [27] | MBSR group (n 15; male mean age = 47.3 year) TAU group (n 15 male mean age = 50.6 year) | INDIA | MBS group: eight weekly sessions, lasting 1–1.5 h Control Group: health education session | CHD | BP BMI | Hospital Anxiety and Depression Scale PSS | MBSR treatment produces significant reduction in symptoms of anxiety and depression, perceived stress, BP, and BMI in CHD patients |
| Steffen et al. (2015) [24] * (not an intervention protocol) | MBI group: n 30 (47% female and 53% male Age: 19.9 year) Control Group: n 32 (53% female and 47% male Age: 20.6 year) | USA | MBI group: Brief 1-day passive listening of two tracks from CD + Mindfulness of Breathing exercise Control Group: Brief 1-day passive listening of two tracks from CD | Cardiovascular reactivity | BP Heart rate | BDI STAI PASAT Working memory and auditory attention | Mindfulness participants showed lower systolic blood pressure and decreased systolic during cognitively stressing activity, whereas no significant effects were detected for mood levels. |
| Sullivan et al. [32] (2009) | MBSR group: n 108 (66.7% male and 33.3% female Age: 61.5 year) Control Group: n 100 (73% male and 27% female Age: 61.1 year) | UK | MBSR group: once a week for 2.25 h for 8 consecutive weeks. Control Group: Usual care treatment | CHF | KCCQ 23-item | CES-D 10-item POMS | MBSR significantly reduced depression and anxiety, while improving overall quality of life and clinical symptoms in patients with CHF when compared to control patients. |
| Tacòn et al. (2003) [33] | MBSR group: n 10 (female Age: 60.5 year Control Group: n 10 female Age: 60.5 year | USA | MBSR group: 8 weeks-2 h each week Control Group: Participants were placed on a waiting list and offered the opportunity to participate in the program after the study was completed. | Angina, hypertension, cardiovascular disease, and cardiac valve disorders. | STAI Courtauld Emotional Control Scale Problem-Focused Styles of Coping Multidimensional Health Locus of Control scale | Women in the intervention group showed improvement in anxiety scores and decrease in the control of negative emotions. | |
| Younge et al. (2015) [17] | MBI group: n 215 (44.2% female and 55.8% male Age:43.2 year) Control Group: n 109 (50.5% female and 49.5 male Age: 43.2 year) | UK | MBI group: 12-week session lasting 1 h Control group: usual care by their treating cardiologist. Treatment and frequency differ between patients | Heart disease | Heart rate BP Respiratory rate NT-proBNP | The Dutch version of the Perceived Stress Scale Social Support Scale 12 Blumenthal | Online mindfulness training shows positive effects on heart rate, systolic and diastolic blood pressure. Whereas no significant effect was found on psychological outcomes. |
| Construct | Study | MBI Group | Control Group | Cohen’s d | Hedges’ g | Weight (%) Fixed Model | Weight (%) Random Model | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | MD | SD | N | MD | SD | g | SE | 95% CI | ||||||
| Anxiety | Tacòn et al. (2003) [33] | 10 | −8.77 | 9.31 | 10 | 0.330 | 12.8 | 0.814 | 0.779 | 0.446 | −0.094 | 1.65 | 3.26 | 14.1 |
| Sullivan et al. (2009) [32] | 108 | −1.25 | 8.16 | 100 | 1.80 | 4.14 | 0.466 | 0.464 | 0.140 | 0.190 | 0.739 | 33.0 | 19.8 | |
| Parswani et al. (2013) [27] | 15 | −1.74 | 3.30 | 15 | −0.140 | 3.49 | 0.471 | 0.458 | 0.360 | −0.248 | 1.16 | 5.00 | 15.8 | |
| Doherty et al. (2015) [10] | 32 | −5.37 | 4.07 | 30 | −1.63 | 4.30 | 0.894 | 0.883 | 0.263 | 0.367 | 1.40 | 9.36 | 17.8 | |
| Younge et al. (2015) [17] | 215 | −0.500 | 3.20 | 109 | −0.900 | 3.00 | −0.128 | −0.127 | 0.117 | −0.357 | 0.103 | 47.0 | 20.1 | |
| Ahmadpanah et al. (2016) [9] | 15 | −6.20 | 4.57 | 15 | 7.87 | 4.54 | 3.09 | 3.01 | 0.526 | 1.98 | 4.04 | 2.34 | 12.5 | |
| Depression | Sullivan et al. (2009) [32] | 108 | −1.74 | 17.3 | 100 | 0.46 | 14.24 | 0.139 | 0.138 | 0.138 | −0.133 | 0.409 | 32.0 | 17.8 |
| Parswani et al. (2013) [27] | 15 | −2.80 | 1.82 | 15 | 0.54 | 2.44 | 1.55 | 1.51 | 0.405 | 0.714 | 2.30 | 3.74 | 15.5 | |
| Nyklicek et al. (2014) [31] | 55 | −1.61 | 0.450 | 52 | −0.210 | .460 | 3.08 | 3.06 | 0.284 | 2.51 | 3.62 | 7.61 | 16.7 | |
| Doherty et al. (2015) [10] | 32 | −5.49 | 3.67 | 30 | −1.73 | 4.36 | 0.936 | 0.924 | 0.264 | 0.406 | 1.44 | 8.79 | 16.9 | |
| Younge et al. (2015) [17] | 215 | −0.50 | 2.90 | 109 | 0.000 | 2.30 | 0.184 | 0.184 | 0.118 | −0.047 | 0.414 | 44.5 | 17.7 | |
| Ahmadpanah et al. (2016) [9] | 15 | −8.00 | 4.52 | 15 | 1.33 | 5.22 | 1.91 | 1.86 | 0.429 | 1.02 | 2.70 | 3.34 | 15.2 | |
| Perceived Stress | Parswani et al. (2013) [27] | 15 | −10.5 | 4.13 | 15 | −2.74 | 8.58 | 1.16 | 1.13 | 0.384 | 0.373 | 1.88 | 5.68 | 18.6 |
| Nehra et al. (2014) [13] | 25 | −3.16 | 2.62 | 25 | −0.920 | 3.60 | 0.712 | 0.701 | 0.287 | 0.138 | 1.26 | 10.1 | 19.9 | |
| Nyklicek et al. (2014) [31] | 55 | −4.5 | 1.04 | 52 | −2.05 | 1.05 | 2.30 | 2.29 | 0.248 | 1.80 | 2.77 | 13.7 | 20.3 | |
| Younge et al. (2015) [17] | 215 | −2.40 | 6.30 | 109 | −0.900 | 6.80 | 0.232 | 0.231 | 0.118 | 0.001 | 0.462 | 6.47 | 21.4 | |
| Momeni et al. (2016) [28] | 30 | −13.5 | 7.57 | 30 | −4.04 | 4.60 | 1.51 | 1.49 | 0.289 | 0.926 | 2.06 | 10.0 | 19.8 | |
| Quality of Life | Nyklicek et al. (2014) [31] | 55 | −2.55 | 0.370 | 52 | −0.630 | .410 | 4.92 | 4.88 | 0.385 | 4.13 | 5.64 | 6.37 | 24.4 |
| Doherty et al. (2015) [10] | 32 | −10.3 | 16.15 | 30 | 1.90 | 18.9 | 0.693 | 0.685 | 0.258 | 0.178 | 1.191 | 14.2 | 25.1 | |
| Younge et al. (2015) [17] | 215 | 0.40 | 10.40 | 109 | 0.700 | 9.30 | 0.030 | 0.030 | 0.117 | −0.200 | 0.260 | 68.6 | 25.5 | |
| Jalali et al. (2019) [30] | 30 | −13.0 | 8.35 | 30 | 0.970 | 8.59 | 1.65 | 1.63 | 0.295 | 1.05 | 2.21 | 10.8 | 24.9 | |
| Blood Pressure | Hughes et al. (2013) [26] | 28 | −2.40 | 5.30 | 28 | 1.10 | 7.11 | 0.558 | 0.550 | 0.269 | 0.024 | 1.08 | 12.3 | 20.9 |
| (Diastolic) | Parswani et al. (2013) [27] | 15 | −2.56 | 5.34 | 15 | −1.60 | 5.50 | 0.177 | 0.172 | 0.356 | −0.525 | 0.870 | 6.98 | 19.2 |
| Younge et al. (2015) [17] | 215 | −2.34 | 8.90 | 109 | −3.39 | 10.1 | −0.113 | −0.112 | 0.117 | −0.342 | 0.118 | 64.2 | 23.1 | |
| Ahmadpanah et al. (2016) [9] | 15 | −21.5 | 10.7 | 15 | 9.69 | 9.17 | 3.14 | 3.051 | 0.530 | 2.01 | 4.09 | 3.14 | 15.6 | |
| Momeni et al. (2016) [28] | 30 | −1.66 | 8.39 | 30 | 0.50 | 6.65 | 0.285 | 0.282 | 0.256 | −0.220 | 0.784 | 13.48 | 21.15 | |
| Blood Pressure | Hughes et al. (2013) [26] | 28 | −4.90 | 6.87 | 28 | −0.70 | 7.83 | 0.570 | 0.562 | 0.269 | 0.035 | 1.089 | 12.68 | 20.98 |
| (Systolic) | Parswani et al. (2013) [27] | 15 | −11.20 | 11.40 | 15 | 10.14 | 23.77 | 1.145 | 1.114 | 0.383 | 0.363 | 1.865 | 6.24 | 18.78 |
| Younge et al. (2015) [17] | 215 | −5.17 | 14.50 | 109 | −1.50 | 15.50 | 0.247 | 0.247 | 0.118 | 0.016 | 0.477 | 66.14 | 23.10 | |
| Ahmadpanah et al. (2016) [9] | 15 | −36.33 | 15.59 | 15 | 9.53 | 17.46 | 2.771 | 2.696 | 0.497 | 1.721 | 3.671 | 3.70 | 16.46 | |
| Momeni et al. (2016) [28] | 30 | −15.83 | 7.73 | 30 | −2.83 | 10.25 | 1.432 | 1.413 | 0.286 | 0.854 | 1.973 | 11.23 | 20.68 | |
| Construct | N Studies | Model | Hedges’ g | Heterogeneity | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| g | SE | 95% CI | z-Score | p-Value | I2 | χ2 | τ2 | df | ||||
| Anxiety | 6 | Fixed | 0.295 | 0.081 | 0.137 | 0.453 | 3.66 | <0.001 * | 0.894 | 47.34 | - | 5 |
| Random | 0.780 | 0.294 | 0.204 | 1.38 | 2.65 | 0.008 * | 0.890 | - | 0.42 | - | ||
| Depression | 6 | Fixed | 0.559 | 0.078 | 0.405 | 0.713 | 7.13 | <0.001 * | 0.956 | 113.6 | - | 5 |
| Random | 1.24 | 0.421 | 0.419 | 2.07 | 2.96 | 0.003 | 0.966 | - | 0.98 | - | ||
| Perceived Stress | 5 | Fixed | 0.737 | 0.091 | 0.557 | 0.916 | 8.05 | <0.001 * | 0.939 | 65.47 | - | 4 |
| Random | 1.16 | 0.435 | 0.306 | 2.01 | 2.66 | 0.007 * | 0.939 | - | 0.87 | - | ||
| Quality of Life | 4 | Fixed | 0.605 | 0.097 | 0.415 | 0.796 | 6.23 | <0.001 * | 0.981 | 159.6 | - | 3 |
| Random | 1.78 | 0.878 | 0.060 | 3.500 | 2.03 | 0.043 | 0.981 | - | 3.0 | - | ||
| Blood Pressure | 5 | Fixed | 0.141 | 0.094 | −0.043 | 0.325 | 1.50 | 0.133 | 0.893 | 37.38 | . | 4 |
| (Diastolic) | Random | 0.657 | 0.357 | −0.043 | 1.36 | 1.84 | 0.066 | 0.893 | - | 0.54 | - | |
| Blood Pressure | 5 | Fixed | 0.563 | 0.096 | 0.375 | 0.750 | 5.88 | <0.001 * | 0.891 | 36.54 | - | 4 |
| (Systolic) | Random | 1.12 | 0.365 | 0.404 | 1.84 | 3.07 | 0.002 * | 0.891 | - | 0.56 | - | |
3.4. Mindfulness and Psychological Outcomes
3.5. Risk of Bias
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; De Ferranti, S.; Després, J.P.; Fullerton, H.J.; Howard, V.J.; et al. Heart Disease and Stroke Statistics-2015 Update: A Report from the American Heart Association. Circulation 2015, 131, e29–e322. [Google Scholar] [CrossRef]
- Loucks, E.B.; Britton, W.B.; Howe, C.J.; Eaton, C.B.; Buka, S.L. Positive Associations of Dispositional Mindfulness with Cardiovascular Health: The New England Family Study. Int. J. Behav. Med. 2015, 22, 540–550. [Google Scholar] [CrossRef]
- Tunstall-Pedoe, H.; Kuulasmaa, K.; Mähönen, M.; Tolonen, H.; Ruokokoski, E.; Amouyel, P. Contribution of trends in survival and coronary-event rates to changes in coronary heart disease mortality: 10-year results from 37 WHO MONICA Project populations. Lancet 1999, 353, 1547–1557. [Google Scholar] [CrossRef]
- Lawrence, M.; Booth, J.; Mercer, S.; Crawford, E. A systematic review of the benefits of mindfulness-based interventions following transient ischemic attack and stroke. Int. J. Stroke 2013, 8, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Mars, T.S.; Abbey, H. Mindfulness meditation practise as a healthcare intervention: A systematic review. Int. J. Osteopath. Med. 2010, 13, 56–66. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Wherever You Go, There You Are: Mindfulness Meditation for Everyday Life; Hyperion: New York, NY, USA, 1994. [Google Scholar]
- Scott-Sheldon, L.A.J.; Gathright, E.C.; Donahue, M.L.; Balletto, B.; Feulner, M.M.; Decosta, J.; Cruess, D.G.; Wing, R.R.; Carey, M.P.; Salmoirago-Blotcher, E. Mindfulness-Based Interventions for Adults with Cardiovascular Disease: A Systematic Review and Meta-Analysis. Ann. Behav. Med. 2020, 54, 67–73. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness; Random House Publishing Group: New York, NY, USA, 2013. [Google Scholar]
- Ahmadpanah, M.; Paghale, S.J.; Bakhtyari, A.; Kaikhavani, S.; Aghaei, E.; Nazaribadie, M.; Holsboer-Trachsler, E.; Brand, S. Effects of psychotherapy in combination with pharmacotherapy, when compared to pharmacotherapy only on blood pressure, depression, and anxiety in female patients with hypertension. J. Health Psychol. 2016, 21, 1216–1227. [Google Scholar] [CrossRef] [PubMed]
- O’Doherty, V.; Carr, A.; McGrann, A.; O’Neill, J.O.; Dinan, S.; Graham, I.; Maher, V. A Controlled Evaluation of Mindfulness-Based Cognitive Therapy for Patients with Coronary Heart Disease and Depression. Mindfulness 2015, 6, 405–416. [Google Scholar] [CrossRef]
- Fogarty, F.A.; Booth, R.J.; Gamble, G.D.; Dalbeth, N.; Consedine, N.S. The effect of mindfulness-based stress reduction on disease activity in people with rheumatoid arthritis: A randomised controlled trial. Ann. Rheum. Dis. 2015, 74, 472–474. [Google Scholar] [CrossRef]
- Labelle, L.E.; Campbell, T.S.; Faris, P.; Carlson, L.E. Mediators of Mindfulness-Based Stress Reduction (MBSR): Assessing the Timing and Sequence of Change in Cancer Patients. J. Clin. Psychol. 2015, 71, 21–40. [Google Scholar] [CrossRef]
- Nehra, D.K.; Sharma, N.; Kumar, P.; Nehra, S. Efficacy of mindfulness-based stress reduction programme in reducing perceived stress and health complaints in patients with coronary heart disease. Dysphrenia 2014, 5, 19–25. [Google Scholar]
- Morgan, D. Mindfulness-Based Cognitive Therapy for Depression: A New Approach to Preventing Relapse. Psychother. Res. 2003, 13, 123–125. [Google Scholar] [CrossRef]
- Abbott, R.A.; Whear, R.; Rodgers, L.R.; Bethel, A.; Thompson Coon, J.; Kuyken, W.; Stein, K.; Dickens, C. Effectiveness of mindfulness-based stress reduction and mindfulness based cognitive therapy in vascular disease: A systematic review and meta-analysis of randomised controlled trials. J. Psychosom. Res. 2014, 76, 341–351. [Google Scholar] [CrossRef] [PubMed]
- Alsubaie, M.; Abbott, R.; Dunn, B.; Dickens, C.; Keil, T.F.; Henley, W.; Kuyken, W. Mechanisms of action in mindfulness-based cognitive therapy (MBCT) and mindfulness-based stress reduction (MBSR) in people with physical and/or psychological conditions: A systematic review. Clin. Psychol. Rev. 2017, 55, 74–91. [Google Scholar] [CrossRef]
- Younge, J.O.; Wery, M.F.; Gotink, R.A.; Utens, E.M.W.J.; Michels, M.; Rizopoulos, D.; Van Rossum, E.F.C.; Hunink, M.G.M.; Roos-Hesselink, J.W. Web-based mindfulness intervention in heart disease: A randomized controlled trial. PLoS ONE 2015, 10, e0143843. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Grp, P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement (Reprinted from Annals of Internal Medicine). Phys. Ther. 2009, 89, 873–880. [Google Scholar] [CrossRef]
- Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M.; Whiting, P.F.; Rutjes, A.W.S.S.; Westwood, M.E.; Mallet, S.; Deeks, J.J.; Reitsma, J.B.; et al. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar]
- Jonathan, J.; Deeks, J.P.H.; Altman, D.G. 9 Analysing Data and Undertaking Meta-Analyses; Jonathan, J., Deeks, J., Higgins, P.T., Altman, D.G., on behalf of the Cochrane Statistical Methods Group, Eds.; Wiley-Blackwell, John Wiley & Sons Ltd.: Chichester, UK, 2008; ISBN 9780470699515. [Google Scholar]
- Freedenberg, V.A.; Hinds, P.S.; Friedmann, E. Mindfulness-Based Stress Reduction and Group Support Decrease Stress in Adolescents with Cardiac Diagnoses: A Randomized Two-Group Study. Pediatr. Cardiol. 2017, 38, 1415–1425. [Google Scholar] [CrossRef] [PubMed]
- Gotink, R.A.; Younge, J.O.; Wery, M.F.; Utens, E.M.W.J.; Michels, M.; Rizopoulos, D.; Van Rossum, L.F.C.; Roos-Hesselink, J.W.; Hunink, M.M.G. Online mindfulness as a promising method to improve exercise capacity in heart disease: 12-month follow-up of a randomized controlled trial. PLoS ONE 2017, 12, 0175923. [Google Scholar] [CrossRef]
- Grant, C.; Hobkirk, A.; Persons, E.; Hwang, V.; Danoff-Burg, S. Cardiovascular reactivity to and recovery from stressful tasks following a mindfulness analog in college students with a family history of hypertension. J. Altern. Complement. Med. 2013, 19, 341–346. [Google Scholar] [CrossRef]
- Steffen, P.R.; Larson, M.J. A Brief Mindfulness Exercise Reduces Cardiovascular Reactivity During a Laboratory Stressor Paradigm. Mindfulness 2015, 6, 803–811. [Google Scholar] [CrossRef]
- Owens, J.E.; Schorling, J.; Plews-Ogan, M.; Goodman, M.; Moorman, R.; Zaklin, R.; Dent, J. A randomized controlled trial evaluating Mindfulness-Based Stress Reduction (MBSR) for the treatment of palpitations: A pilot study. Int. J. Cardiol. 2016, 223, 25–27. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.W.; Fresco, D.M.; Myerscough, R.; Van Dulmen, M.H.M.; Carlson, L.E.; Josephson, R. Randomized controlled trial of mindfulness-based stress reduction for prehypertension. Psychosom. Med. 2013, 75, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Parswani, M.; Sharma, M.; Iyengar, S. Mindfulness-based stress reduction program in coronary heart disease: A randomized control trial. Int. J. Yoga 2013, 6, 111. [Google Scholar] [CrossRef]
- Momeni, J.; Omidi, A.; Raygan, F.; Akbari, H. The effects of mindfulness-based stress reduction on cardiac patients’ blood pressure, perceived stress, and anger: A single-blind randomized controlled trial. J. Am. Soc. Hypertens. 2016, 10, 763–771. [Google Scholar] [CrossRef]
- Norman, J.; Fu, M.; Ekman, I.; Björck, L.; Falk, K. Effects of a mindfulness-based intervention on symptoms and signs in chronic heart failure: A feasibility study. Eur. J. Cardiovasc. Nurs. 2018, 17, 54–65. [Google Scholar] [CrossRef] [PubMed]
- Jalali, D.; Abdolazimi, M.; Alaei, Z.; Solati, K. Effectiveness of mindfulness-based stress reduction program on quality of life in cardiovascular disease patients. IJC Heart Vasc. 2019, 23, 100356. [Google Scholar] [CrossRef]
- Nyklíček, I.; Dijksman, S.C.; Lenders, P.J.; Fonteijn, W.A.; Koolen, J.J. A brief mindfulness based intervention for increase in emotional well-being and quality of life in percutaneous coronary intervention (PCI) patients: The MindfulHeart randomized controlled trial. J. Behav. Med. 2014, 37, 135–144. [Google Scholar] [CrossRef]
- Sullivan, M.J.; Wood, L.; Terry, J.; Brantley, J.; Charles, A.; McGee, V.; Johnson, D.; Krucoff, M.W.; Rosenberg, B.; Bosworth, H.B.; et al. The Support, Education, and Research in Chronic Heart Failure Study (SEARCH): A mindfulness-based psychoeducational intervention improves depression and clinical symptoms in patients with chronic heart failure. Am. Heart J. 2009, 157, 84–90. [Google Scholar] [CrossRef]
- Tacón, A.M.; McComb, J.; Caldera, Y.; Randolph, P. Mindfulness meditation, anxiety reduction, and heart disease: A pilot study. Fam. Community Health 2003, 26, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Freedenberg, V.A.; Thomas, S.A.; Friedmann, E. A Pilot Study of a Mindfulness Based Stress Reduction Program in Adolescents with Implantable Cardioverter Defibrillators or Pacemakers. Pediatr. Cardiol. 2015, 36, 786–795. [Google Scholar] [CrossRef] [PubMed]
- Keyworth, C.; Knopp, J.; Roughley, K.; Dickens, C.; Bold, S.; Coventry, P. A mixed-methods pilot study of the acceptability and effectiveness of a brief meditation and mindfulness intervention for people with diabetes and coronary heart disease. Behav. Med. 2014, 40, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Cullen, M. Mindfulness-Based Interventions: An Emerging Phenomenon. Mindfulness 2011, 2, 186–193. [Google Scholar] [CrossRef]


| MeSH Terms | PubMed | Science Direct | Scholar |
|---|---|---|---|
| “Heart Diseases” AND “mindfulness” | 11/15 | 4/1187 | 7/35,900 |
| “Cardiovascular Diseases” AND “Mindfulness” | 23/33 | 0/1934 | 23/34,900 |
| “Heart Failure” AND “Mindfulness” | 1/2 | 9/2168 | 1/36,500 |
| “Cardiovascular failure and Mindfulness” | ----- | 6/1123 | 5/24,200 |
| “Congestive heart failure and Mindfulness” | 3 | 3/444 | 2/6510 |
| “Coronary Disease” AND “Mindfulness” | 3/3 | 0/79 | 11/20,500 |
| “Cardiovascular Abnormalities” AND “Mindfulness”; Congenital Abnormalities” AND “Mindfulness”; “Heart Defects, Congenital” AND “Mindfulness;” Cardiovascular Infections” AND “Mindfulness” | ------ | 3/621 | ------ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marino, F.; Failla, C.; Carrozza, C.; Ciminata, M.; Chilà, P.; Minutoli, R.; Genovese, S.; Puglisi, A.; Arnao, A.A.; Tartarisco, G.; et al. Mindfulness-Based Interventions for Physical and Psychological Wellbeing in Cardiovascular Diseases: A Systematic Review and Meta-Analysis. Brain Sci. 2021, 11, 727. https://doi.org/10.3390/brainsci11060727
Marino F, Failla C, Carrozza C, Ciminata M, Chilà P, Minutoli R, Genovese S, Puglisi A, Arnao AA, Tartarisco G, et al. Mindfulness-Based Interventions for Physical and Psychological Wellbeing in Cardiovascular Diseases: A Systematic Review and Meta-Analysis. Brain Sciences. 2021; 11(6):727. https://doi.org/10.3390/brainsci11060727
Chicago/Turabian StyleMarino, Flavia, Chiara Failla, Cristina Carrozza, Maria Ciminata, Paola Chilà, Roberta Minutoli, Sara Genovese, Alfio Puglisi, Antonino A. Arnao, Gennaro Tartarisco, and et al. 2021. "Mindfulness-Based Interventions for Physical and Psychological Wellbeing in Cardiovascular Diseases: A Systematic Review and Meta-Analysis" Brain Sciences 11, no. 6: 727. https://doi.org/10.3390/brainsci11060727
APA StyleMarino, F., Failla, C., Carrozza, C., Ciminata, M., Chilà, P., Minutoli, R., Genovese, S., Puglisi, A., Arnao, A. A., Tartarisco, G., Corpina, F., Gangemi, S., Ruta, L., Cerasa, A., Vagni, D., & Pioggia, G. (2021). Mindfulness-Based Interventions for Physical and Psychological Wellbeing in Cardiovascular Diseases: A Systematic Review and Meta-Analysis. Brain Sciences, 11(6), 727. https://doi.org/10.3390/brainsci11060727