
The Near-Death Experience: A Reality Check?

Abstract
:1. Some Initial Considerations
2. The ND/OBE Experiential Curriculum
2.1. Baseline Features
2.2. How Trustworthy Are NDE Reports?
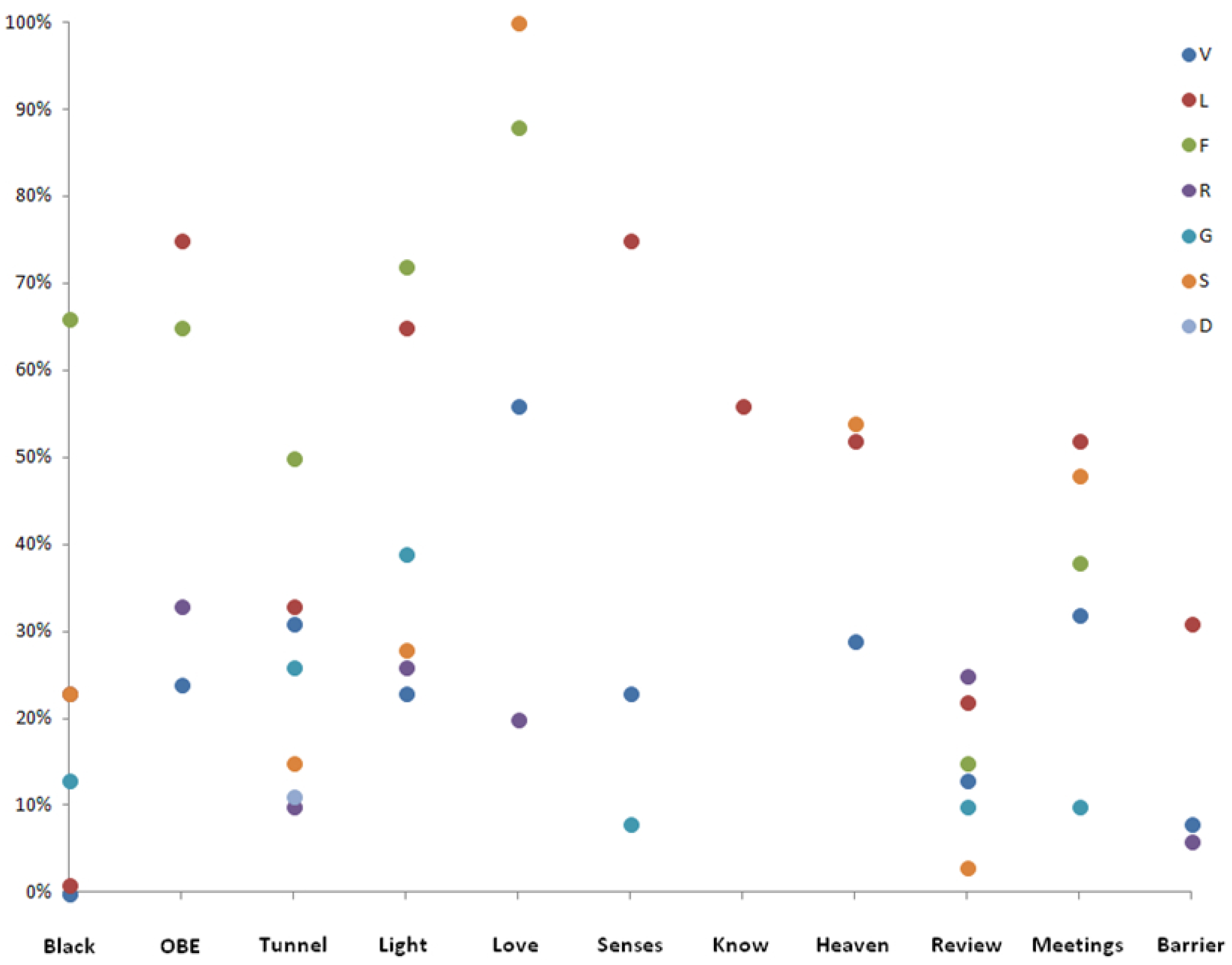
2.3. The Idiosyncratic Nature of NDE
2.4. Hellish Experiences
2.5. The Semantic Content of Experiences Undergone
2.6. The Jesus Characteristics and Geography of Heaven: True Insights—or Not?
“I can see that form now—it had blond-gold hair…and a beard—very light, and a moustache [and] a white garment on—there was a red spot here [points to image of a Sacred Heart on gown]—and a chalice in his hand”.([1], p. 60)
Or: “He was tall—had a white robe on—his face was beautiful—his skin was glowing and absolutely flawless”.([4], p. 49)
And “She [in reference to the subject’s mother] was wearing a long sparkling silver gown—[as] did Christ—he had long hair—long beard”.([4], p. 169)
And: “...I saw Christ. He was incredibly beautiful...his feet were bare. The bosom was open and you could see his chest. He had hair down to his shoulders and a beard. There was light coming out of his head like a star”.([5], p. 229)
3. Neuro(patho)logical Considerations
3.1. The Physical Features of the ND/OBE Body
3.2. Duality of Conscious Awareness during ND/OBE
3.3. The Vestibular System and the Out-of-Body Component
3.4. The Tunnel Phenomenon and the Perceived Light
3.5. How Accurate Are Reports about OBE?—General Comments
3.6. Are OBE Reports Reliably Accurate?—The Non-Contributory Case of Pam Reynolds
3.7. The Neurophysiological Basis of ND/OBE Phenonmenology
“[I came] rushing through a tunnel and snapped back into my body”;“When they put the shocks [electrical defibrillation] on me and I fell back, down to my body, like a dead weight. And the next thing, I was in my body again”;“Then there was sudden confusion—I was upset and scared—something was wrong. I regained my body and felt tremendous pain all over”.
- (1)
- NDE terminate as subjects regain full conscious-awareness—there is no recorded case to the contrary;
- (2)
- it follows that ND/OBE occur in the immediate run-up period to that objective time-point;
- (3)
- the use of word-counts (as used in dream research) suggests that these events are ephemeral and generally last only a few seconds or minutes: there can be no escape from that conclusion, and is a key issue;
- (4)
- this seems to be a sensible conclusion since, on physiological grounds, memories can only be set down when the brain is not in a moribund state—a fourth vital point needing recognition. Surely the most sensible conclusion is that ND/OBE do occur, and are remembered during those final moments as subjects are rapidly returning to full conscious-awareness;
- (5)
- ND/OBE are therefore brain-originating phenomena, and not trips to “Heaven”, “Hell”, other imagined cosmic spaces, or generated by external agencies.
- (1)
- suicide survivors from the Golden Gate Bridge [46];
- (2)
- (3)
- from military pilots centrifuged to unconsciousness.
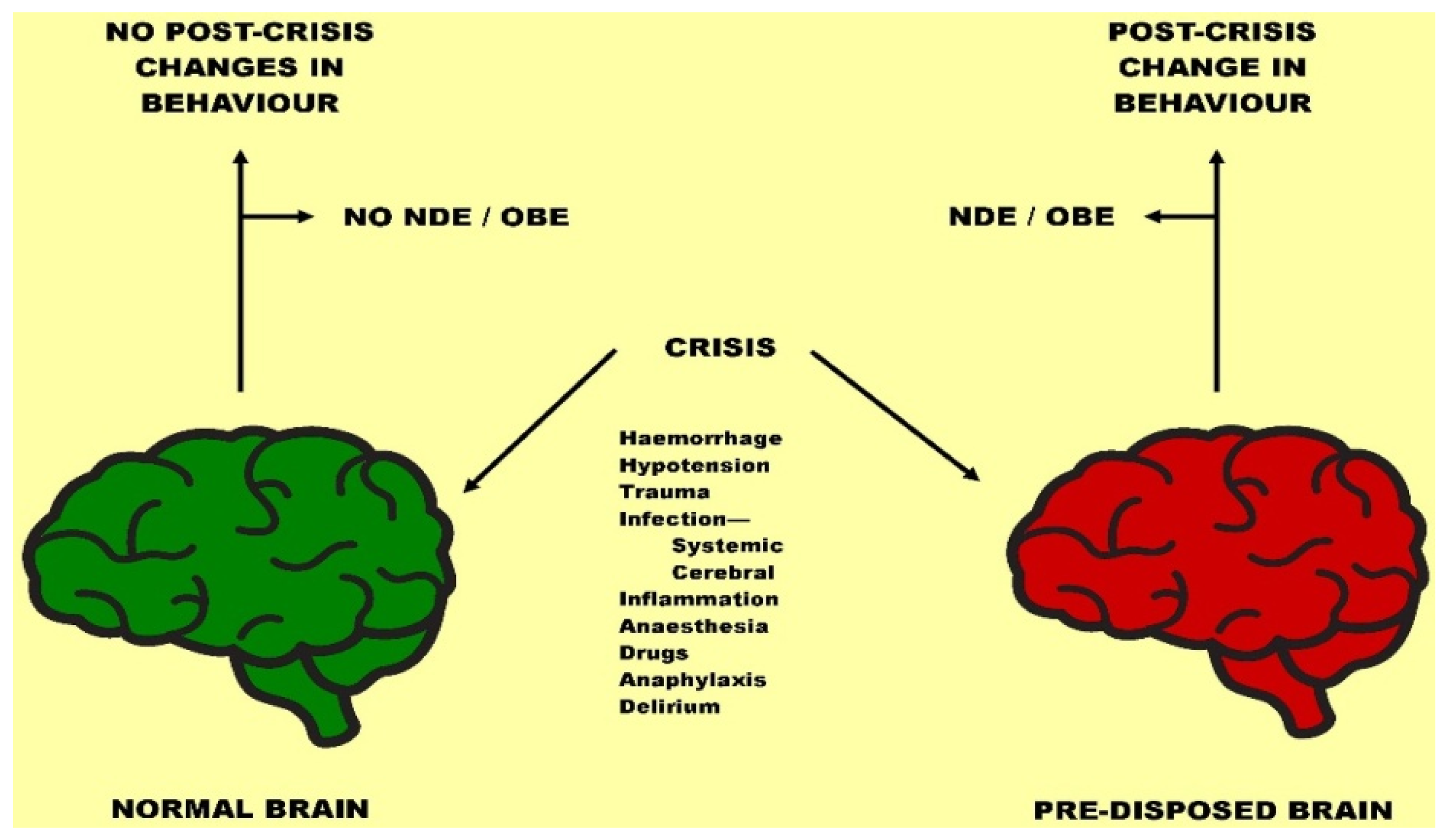
3.8. Is there a Predisposed Brain Underlying ND/OBE Phenomenology?
3.9. REM-Intrusion and the Emergent State of Otherworld Possession
4. Theological Considerations
4.1. Considering the Spiritual Domain of NDE
4.2. Changed Perceptions in Subjects Post-Event
4.3. Comments on So-called Paranormal Outcomes of ND/OBE Phenomena
4.4. Grappling with Those Eternal—Yet Persistent—Key Questions!
5. Summary: Checking Reality
5.1. The Background Perspective
5.2. Some Conceptual Inputs
- (1)
- It seems important to stress again that ND/OBE are non-uniform, extremely heterogeneous events—viewed historically, culturally, or personally. They are heavily overloaded with anthropomorphic and geophysical reference. Their idiosyncratic personally-biased characteristics almost deny definition. Their dreamlike content can be absurd, illogical, and even frankly silly. The juxtaposed occurrence of “hellish” as well as “heavenly” reports, and their inter-conversions, seriously undermines the possibility of sensibly belonging to, or even representing, another presumed non-physical realm. That difficulty, to my knowledge, has not been fully acknowledged by the ND fraternity.
- (2)
- Another threat, excluding willful dishonesty, is that some of the reported happenings are factually incorrect. Yet these aberrations are glossed over in the attempt to assert often with considerable force that the ones which are supposedly not incorrect indelibly point to existence away from, and independent of, the body. The current trend is based mainly on cardiac patients who may represent particular, and possibly biased, kinds of ND experiences. Apart from their employment in supporting the "consciousness-exists-outside-a-dead-brain" mantra, they cannot be made to generalize upon, or even promote, those proposals advanced.
- (3)
- And while a few people have apparently learned all knowledge, and amassed the information residing in large (earth-like, it should be noted) libraries, these revelations are never capable of disclosure on return to earth. There has never been one, single revelatory report bringing to our attention something never before witnessed throughout the annals of recorded history on this planet. All we are served with are blue skies, fluffy white clouds, beautiful flowers, and so on (see Section 4.4, above). To me that sounds rather locally suspicious, and not the ideal programmatic material with which to usher in the new “Omega” or “Millennium”, or whatever else we are headed for.
- (4)
- Another major problem that requires addressing is how the memory for these events is put down. It should be obvious to everyone that our memories require defined neural process for their capture, thus to facilitate subsequent expression. The increasingly ravaging effects of dementia severely remind us of that. However, “cosmic consciousness” seems very reluctant to relieve us of our failures to remember things on earth, neither those, it seems, having had the privileged luxury of travel to other-world destinations. This critically applies to all those experts who insist that some form of non-neural mentation can exist alone, or as part of the “Big Mind” somewhere out there. If it were insisted that the memories recollected were not due to neural function, then why are these same subjects incapable of bringing back remembered aspects of their experiences while away from earth, notably answers to the important questions about knowledge, life and existence? In that respect, there has been a consistent, miserable failure.
- (5)
- In addition, there must be some resonances to the fact that for many subjects, their experience ends precisely when conscious-awareness returns, reminding us of the abrupt return when our last period of nocturnal REM sleep finishes—so-called hypnopompic re-awakenings. Since this implies that ND/OBE occur during that period as conscious-awareness is being resumed, there is no problem concerning how memory for the event is set down. That period of resumed conscious-awareness can be quite rapid. That, for example, was demonstrated by scientists carrying out laboratory-timed observations with unconscious military aircrew as they came back to life. Their recollections occurred within 40 laboratory-timed seconds.
- (6)
- Some post-experiential subjects undergo profound changes in their lives and outlooks. Unfortunately, we still do not know what percentage of experients are so involved. But these life-changing reversals, although of great personal significance, are not unique to ND/OBE, since they frequently occur as a result of a profound life stress, an acutely fearful occurrence, childhood abuse, or the result of taking drugs, such as LSD. We do not have a clear picture why only a few ND/OBE subjects experience these changes, yet it is a phenomenon which could be empirically investigated through use of appropriate questionnaires and neurophysiological investigations. There must be discernible differences between those subjects affected, and those not. I have alluded to genetic, structural, and psychological differences that could be relevant: those ideas need follow up.
- (7)
- On a wider front, we need some answers as to why 90+% (cardiac) subjects never have ND/OBE. Investigative techniques could be employed to attempt to find differences. It must be asked why these are not being employed to find solutions to these remaining uncertainties. Far better to devote time and money updating those unknowns rather than to continue the vain, dogged attempt to see whether subjects out-of-body can report on played videos or marked boards distributed around intensive care settings.
- (8)
- Neurophysiological data are rapidly transforming the ND/OBE scene. Work on the temporo-parietal junction gives insights about the self, and of its projections into peri-personal space (OBE) and the sensing of other presences. The concept of REM intrusion, elucidated in context of sleep paralysis, lucid dreaming, and narcolepsy offers profound insights into the apparent loss of selfhood when the switching between the relevant neural loci in upper brainstem is disturbed. In that “no-man’s land”, the resulting experience does become ineffable, such that the subject feels entirely separated from reality and thus in the presence of God, or “Absolute Being”, etc. The third neurophysiological prong concerns possible developmental abnormalities in left-right bodily orientation, and the resulting propensity to extend towards the paranormal, magical ideation, fantasy proneness, and so on.
Conflicts of Interest
References
- Kenneth Ring. Life at Death: A Scientific Investigation of the Near-Death Experience. New York: Coward, McCann & Geoghegan, 1980. [Google Scholar]
- Raymond Moody. Life after Life. Covington: Mockingbird Books, 1975. [Google Scholar]
- Bruce Greyson. “A typology of near-death experiences.” American Journal of Psychiatry 142 (1985): 967–69. [Google Scholar] [PubMed]
- Michael Sabom. Recollections of Death. New York: Harper Row, 1982. [Google Scholar]
- Peter Fenwick, and Elizabeth Fenwick. The Truth in the Light. New York: Berkeley Books, 1998. [Google Scholar]
- Margot Grey. Return from Death. Boston: Arkana, 1985. [Google Scholar]
- Pim Van Lommel, Ruud van Wees, Vincent Meyers, and Ingrid Elfferich. “Near-death experience in survivors of cardiac arrest: A prospective study in the Netherlands.” Lancet 358 (2001): 2039–45. [Google Scholar]
- Pim Van Lommel. Consciousness beyond Life: The Science of the Near-Death Experience. New York: Harper One, 2010. [Google Scholar]
- Kenneth Drab. “The tunnel experience: Reality or hallucination? ” Journal of Near-Death Studies 1 (1981): 126–52. [Google Scholar]
- Olaf Blanke, and Sebastian Dieguez. “Leaving Body and Life Behind: Out-of-Body and Near-Death Experience.” In The Neurology of Consciousness. Edited by Steven Laureys and Giulio Tonini. San Diego: Academic Press, 2009. [Google Scholar]
- William Cash. “Did atheist philosopher see God when he ‘died’? ” The Washington Post, 3 March 2001. [Google Scholar]
- Larry Dossey. Recovering the Soul: A Scientific and Spiritual Search. New York: Bantam Books, 1989. [Google Scholar]
- Francis Walker. “A nowhere near-death experience: Heavenly choirs interrupt myelo-graphy.” Journal of American Medical Association 261 (1989): 3245–46. [Google Scholar] [CrossRef]
- Kevin Malarkey. The Boy Who Came Back from Heaven. Carol Stream: Tyndale House Publishing, 2011. [Google Scholar]
- Alan Kellehear. “Culture, biology and the near-death experience.” The Journal of Mental and Nervous Disease 181 (1993): 148–56. [Google Scholar] [CrossRef]
- Bede. A History of the English Church & People. London: Penguin Classics, 1968. [Google Scholar]
- Satwant Pasricha, and Ian Stevenson. “Near-death experiences in India.” The Journal of Mental and Nervous Disease 174 (1986): 165–70. [Google Scholar] [CrossRef]
- Dorothy Counts. “Near-death and out-of-body experiences in a Melanesian society.” Journal of Near-Death Studies 3 (1983): 115–35. [Google Scholar]
- Jeffery Long. Evidence of the Afterlife. New York: Harper One, 2010. [Google Scholar]
- Eben Alexander. Proof of Heaven. London: Piatkus, 2012. [Google Scholar]
- Ian Wilson. Life after Death. London: Pan Books, 1997. [Google Scholar]
- Bruce Greyson, and Nancy Bush. “Distressing Near-Death Experiences.” Psychiatry 55 (1992): 95–110. [Google Scholar] [PubMed]
- Kenneth Ring. “Solving the riddle of frightening near-death experiences.” Journal of Near-Death Studies 13 (1994): 5–23. [Google Scholar]
- Silvio Ionta, Lukas Heydrich, Bigna Lenggenhager, Michael Mouthon, Eleonora Fornari, Dominique Chapuis, Roger Gassert, and Olaf Blanke. “Multisensory mechanisms in temporo-parietal cortex support self-locationand first-person perspective.” Neuron 70 (2011): 363–74. [Google Scholar] [CrossRef] [PubMed]
- Caro Lippman. “Hallucinations of physical duality in migraine.” American Journal of Psychiatry 117 (1953): 345–50. [Google Scholar] [CrossRef]
- Richard Andersen. “Multimodal integration for the representation of space in the posterior parietal cortex.” Philosophical Transactions of the Royal Society of London 352 (1997): 1421–28. [Google Scholar] [CrossRef] [PubMed]
- Thomas Brandt, and Marianne Dieterich. “The vestibular cortex: Its locations, functions, and disorders.” Annals of the New York Academy of Science 871 (1999): 293–312. [Google Scholar] [CrossRef]
- James Lackner. “Some proprioceptive influences on the perceptual representation of body shape and orientation.” Brain 111 (1988): 281–97. [Google Scholar] [CrossRef] [PubMed]
- Horst Mittelstaedt. “The role of the otoliths in the perception of the orientation of self and world to the vertical.” Zoologische Jahrbucher Physiology 95 (1991): 419–25. [Google Scholar]
- Ernest Dunbar. “The light thrown on psychological processes by the action of drugs.” Proceedings of the Society for Psychical Research 19 (1905): 62–77. [Google Scholar]
- T. Lempert, M. Bauer, and D. Schmidt. “Syncope: A videometric analysis of 56 episodes of transient cerebral hypoxia.” Annals of Neurology 36 (1994): 233–37. [Google Scholar] [CrossRef] [PubMed]
- P. Howard, G. L. Leathart, A. C. Dornhorst, and E. P. Sharpey-Schafer. “The ‘mess trick’ and the ‘fainting lark’.” British Medical Journal 3 (1951): 382–84. [Google Scholar] [CrossRef]
- Th. Els, J. Kassubek, R. Kubalek, and J. Klisch. “Diffusion-weighted MRI during early global cerebral hypoxia: A predictor for clinical outcome? ” Acta neurologica Scandinavica 110 (2004): 361–67. [Google Scholar] [CrossRef] [PubMed]
- G. Schneider, A. W. Gelb, B. Schmeller, R. Tschakert, and E. Kochs. “Detection of awareness in surgical patients with EEG-based indices—Bispectral index and patient state index.” British Journal of Anaesthesia 91 (2003): 329–35. [Google Scholar] [CrossRef] [PubMed]
- Logan Voss. “Monitoring consciousness: The current status of EEG-based depth of anaesthesia monitors.” Best Practice & Research Clinical Anaesthesiology 21 (2007): 313–25. [Google Scholar] [CrossRef]
- Sam Parnia, Ken Spearpoint, Gabriele de Vos, Peter Fenwick, Diana Goldberg, Jie Yang, Jiawen Zhu, Katie Baker, Hayley Killingback, Paula McLean, and et al. “AWARE—Awareness during Resuscitation—A prospective study.” Resuscitation 85 (2014): 1799–805. [Google Scholar] [CrossRef] [PubMed]
- Crislip Mark. “Near Death Experiences & the Medical Literature.” Available online: http://www.skeptic.com/eskeptic/08-06-18 (accessed on 21 October 2015).
- Sebastian Dieguez. “NDEs Redux: Skeptics Need to Reclaim, Redefine and Embrace Near Death Experiences.” Available online: http://www.skeptic.com/eskeptic/08-08-13 (accessed on 21 October 2015).
- Michael Sabom. Light and Death. Grand Rapids: Zondervan, 1998. [Google Scholar]
- Robert F. Spetzler, Mark N. Hadley, Daniele Rigamonti, L. Philip Carter, Peter A. Raudzens, Steven A. Shedd, and Elizabeth Wilkinson. “Aneurysms of the basilar artery treated with circulatory arrest, hypothermia, and barbiturate cerebral protection.” Journal of Neurosurgery 68 (1988): 868–79. [Google Scholar] [CrossRef] [PubMed]
- Mary Ann Liebert. “Use of barbiturates in the control of intracranial hypertension.” Journal of Neurotrauma 17 (2000): 527–30. [Google Scholar]
- J.-O. Trelles, and Daniel Lagache. “Intoxication barbiturique recidivante s’accompagnant d’hallucinose pedoculaire.” Annales Medico-Psychologiques 16 (1932): 565–72. [Google Scholar]
- Jean L’Hermitte. “Syndrome de la calotte du peduncle cerebral: Les troubles psycholo-sensoriels dans les lesions du mesocephale.” Review of Neurology (Paris) 38 (1922): 1359–65. [Google Scholar]
- Michael N. Marsh. Out-of-Body & Near-Death Experiences: Brain State Phenomena or Glimpses of Immortality? Oxford: Oxford University Press, 2010. [Google Scholar]
- Olaf Blanke, and Christine Mohr. “Out-of-body experience, heautoscopy, and autoscopic hallucinations of neurological origins: Implications for neurocognitive mechanisms of corporeal awareness and self-consciousness.” Brain Research Reviews 50 (2005): 184–99. [Google Scholar] [CrossRef] [PubMed]
- David Rosen. “Suicide survivors: A follow-up study of persons who survived jumping from the Golden gate and San Francisco-Oakland bridges.” Western Journal of Medicine 122 (1975): 289–94. [Google Scholar] [PubMed]
- Estelle Forster, and James E. Winnery. “Recovery from Gz-Induced loss of consciousness: Psychological considerations.” Aviation Space, and Environmental Medicine 59 (1988): 517–22. [Google Scholar]
- Divya Mehta, Torsten Klengel, Karen N. Conneely, Alicia K. Smithc, André Altmann, Thaddeus W. Pace, Monika Rex-Haffner, Anne Loeschner, Mariya Gonik, Kristina B. Mercer, and et al. “Childhood maltreatment is associated with distinct genomic and epigenetic profiles in posttraumatic stress disorder.” Proceedings of the National Academy of Sciences USA 110 (2013): 8302–7. [Google Scholar] [CrossRef] [PubMed]
- M. C. Craig, M. Catani, Q. Deeley, R. Latham, E. Daly, R. Kanaan, M. Picchioni, P. K. McGuire, T. Fahy, and D. G. M. Murphy. “Altered connections on the road to psychopathy.” Molecular Psychiatry 14 (2009): 946–53. [Google Scholar] [CrossRef] [PubMed]
- Andreas Meyer-Lindenberg, Joshua W. Buckholtz, Bhaskar Kolachana, Ahmad R. Hariri, Lukas Pezawas, Giuseppe Blasi, Ashley Wabnitz, Robyn Honea, Beth Verchinski, Joseph Callicott, and et al. “Neural mechanisms of genetic risk for impulsivity and violence in humans.” Proceedings of the National Academy of Sciences USA 103 (2006): 6269–74. [Google Scholar] [CrossRef] [PubMed]
- Martin H. Teicher, and Jacqueline Samson. “Childhood maltreatment and psychology: A case for ecophenotypic variants as clinically and neurobiologically distinct subtypes.” American Journal of Psychiatry 170 (2013): 1114–33. [Google Scholar] [CrossRef] [PubMed]
- David E. Comings, Nancy Gonzales, Gerard Saucier, Patrick J. Johnson, and James P. MacMurray. “The DR4 gene and the spiritual transcendence scale of the character temperament scale.” Psychiatric Genetics 10 (2000): 185–89. [Google Scholar] [CrossRef] [PubMed]
- Lorenzi Cristina, Serretti Alessandro, Mandelli Laura, Tubazio Viviana, Ploia Cristina, and Smeraldi Enrico. “5-HT 1A polymorphisms and self-transcendence in mood disorders.” American Journal of Medical Genetics Part B Neuropsychiatric Genetics 137 (2005): 33–35. [Google Scholar]
- Cosimo Urgesi, Salvatore M. Aglioti, Miran Skrap, and Franco Fabbro. “The spiritual brain: Selective cortical lesions modulate human self-transcendence.” Neuron 65 (2010): 309–19. [Google Scholar] [CrossRef] [PubMed]
- Britton Willoughby, and Richard R. Bootzin. “Near-death experiences and the temporal lobe.” Psychological Science 15 (2004): 254–58. [Google Scholar]
- Richard J. Roberts, Nils R. Varney, James R. Hulbert, Jane S. Paulsen, Emily D. Richardson, Jane A. Springer, Janet Smith Shepherd, Cynthia M. Swan, Joseph A. Legrand, John H. Harvey, and et al. “The neuropathology of everyday life: The frequency of partial seizure symptoms among normals.” Neuropscychology 4 (1990): 65–85. [Google Scholar] [CrossRef]
- Michael Persinger, and Makarec Katherine. “Complex partial epileptic signs as a continuum from normals to epileptics: Normative data and clinical populations.” Journal of Clinical Psychology 49 (1993): 33–45. [Google Scholar] [CrossRef]
- Craig Murray, and Jezz Fox. “The out-of-body experience and body image: Difference between experients and non experients.” The Journal of Mental and Nervous Disease 193 (2005): 70–72. [Google Scholar] [CrossRef]
- M. N. Marsh. “Near-Death & Out-of-Body Experiences.” In The Springer Encyclopedia of Sciences and Religions. Edited by Anne Runehov and Luis Oviedo. Berlin: Springer Verlag, 2013. [Google Scholar]
- Kevin R. Nelson, Michelle Mattingly, Sherman A. Lee, and Frederick A. Schmitt. “Does the arousal system contribute to near death experience? ” Neurology 66 (2006): 1003–9. [Google Scholar] [CrossRef] [PubMed]
- Kevin R. Nelson, Mattingly Michelle, and Schmitt Frederick. “Out-of-body experience and arousal.” Neurology 68 (2007): 794–95. [Google Scholar] [CrossRef] [PubMed]
- Kevin R. Nelson. The Spiritual Doorway into the Brain. New York: Plume Books, 2012. [Google Scholar]
- Giorgio Buzzi. “Near-death experiences.” Lancet 359 (2002): 2116–17. [Google Scholar] [CrossRef]
- Tracey L. Kahan, and Stephen LaBerge. “Lucid dreaming as metacognition: Implications for cognitive science.” Consciousness and Cognition 3 (1994): 246–64. [Google Scholar] [CrossRef]
- Ursula Voss, Romain Holzmann, Inka Tuin, and J. Allan Hobson. “Lucid dreaming: A state of consciousness with features of both waking and non-lucid dreaming.” Sleep 32 (2009): 1191–200. [Google Scholar] [PubMed]
- Ling Lin, Juliette Faraco, Robin Li, Hiroshi Kadotani, William Rogers, Xiaoyan Lin, Xiaohong Qiu, Pieter J. de Jong, Seiji Nishino, and Emmanuel Mignot. “The sleep disorder canine narcolepsy is caused by a mutation in the hypocretin (orexin) receptor 2 gene.” Cell 98 (1999): 365–76. [Google Scholar] [CrossRef]
- Thomas C. Thannickal, Robert Y. Moore, Robert Nienhuis, Lalini Ramanathan, Seema Gulyani, Michael Aldrich, Marsha Cornford, and Jerome M. Siegel. “Reduced numbers of hypocretin neurons in human narcolepsy.” Neuron 27 (2000): 469–74. [Google Scholar] [CrossRef]
- Kaur Satvinder, Thankachan Stephen, Begum Ssuraiya, Liu Meng, Blanco-Centurion Carlos, and Shiromani Priyattam. “Hypocretin-2 saporin lesions of the ventrolateral periaquaductal gray (vlPAG) increase REM sleep in hypocretin knockout mice.” PLoS ONE 4 (2009): E6346. [Google Scholar]
- Gary Aston-Jones, Janusz Rajkowski, and Jonathan Cohen. “Role of Locus Coeruleus in attention and behavioural flexibility.” Biological Psychiatry 46 (1999): 1309–20. [Google Scholar] [CrossRef]
- Jun Lu, David Sherman, Marshall Devor, and Clifford B. Saper. “A putative flip-flop switch for control of REM sleep.” Nature 441 (2006): 589–94. [Google Scholar] [CrossRef] [PubMed]
- J. Puizillout, and A. S. Foutz. “Vago-aortic nerves and REM sleep: Evidence for a REM-triggering and a REM-maintenance factor.” Brain Research 111 (1976): 181–84. [Google Scholar] [CrossRef]
- D. J. Vagg, R. Bandler, and K. A. Keay. “Hypovolemic shock: Critical involvement of a projection from the ventrolateral periaquaductal gray to the caudal midline medulla.” Neuroscience 152 (2008): 1099–109. [Google Scholar] [CrossRef] [PubMed]
- William Alston. Perceiving God: The Epistemology of Religious Experience. Ithaca: Cornell University Press, 1993. [Google Scholar]
- William James. The Varieties of Religious Experience. London: Longman, Green & Company, 1902. [Google Scholar]
- Peter Berger. “A Rumour of Angels.” In Modern Society and the Rediscovery of the Supernatural. Garden City: Doubleday, 1969. [Google Scholar]
- Alister Hardy. The Spiritual Nature of Man. Oxford: Oxford University Press, 1979. [Google Scholar]
- David C. Van Essen, Heather A. Drury, Sarang Joshi, and Michael I. Miller. “Functional and structural mapping of human cerebral cortex: Solutions are in the surfaces.” Proceedings of the National Academy of Sciences USA 95 (1998): 788–95. [Google Scholar] [CrossRef]
- Kenneth Ring. Heading Towards Omega. New York: Morrow, 1985. [Google Scholar]
- Colin Ross, and Shaun Joshi. “Paranormal experiences in the general population.” The Journal of Mental and Nervous Disease 180 (1992): 357–61. [Google Scholar] [CrossRef]
- G. Gallup, and F. Newport. “Belief in the paranormal among adult Americans.” Skeptical Enquirer 15 (1991): 137–46. [Google Scholar]
- Peter Brugger, and Mohr Christine. “The paranormal mind: How the study of anomalous experiences and beliefs may inform cognitive neuroscience.” Cortex 44 (2008): 1291–98. [Google Scholar] [CrossRef] [PubMed]
- Christopher C. French, Julia Santomauro, Victoria Hamilton, Rachel Fox, and Michael Thalbourne. “Psychological aspects of the alien contact experience.” Cortex 44 (2008): 1387–95. [Google Scholar] [CrossRef] [PubMed]
- Jessica I. Fleck, Deborah L. Green, Jennifer L. Stevenson, Lisa Payne, Edward M. Bowden, Mark Jung-Beeman, and John Kounios. “The transliminal brain at rest: Baseline EEG, unusual experiences, and access to unconscious mental activity.” Cortex 44 (2008): 1353–63. [Google Scholar] [CrossRef] [PubMed]
- Günter Schulter, and Ilona Papousek. “Believing in paranormal phenomena: Relations to asymmetry of body and brain.” Cortex 44 (2008): 1326–35. [Google Scholar] [CrossRef] [PubMed]
- Deborah Blum. Ghost Hunters. London: Century (Random House Publications), 2007. [Google Scholar]
- Michael N. Marsh. On Being Human: Distinctiveness, Dignity, Disability, Disposal. New York: IFF Books (JHHunt), 2015. [Google Scholar]
- Michael N. Marsh. “Above the Bright Blue Sky.” Antonianum 2 (2015): 3289–318. [Google Scholar]
- Michael N. Marsh. “Hey! What’s that Gorilla doing over there? On the illusory-hallucinatory nature of everyday living.” European Review 23 (2015): 455–72. [Google Scholar] [CrossRef]
- Ring Kenneth, and Sharon Cooper. Mindsight: Near-Death & Out-of-Body Experiences in the Blind. Kearney: Morris Publishing, 2008. [Google Scholar]
- Ring Kenneth, and Sharon Cooper. “Near-death and out-of-body experiences in the blind: A study of apparent eyeless vision.” Journal of Near-Death Studies 16 (1997): 101–47. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| NDE: Early & Late Phase | |
|---|---|
| ● No pain | ● Increased pain perception |
| ● Ability to traverse physical objects | ● Hearing real voices |
| ● Absence of gravity—floating/weightless | ● “Moral” imperative to assume earthly responsibilities |
| ● Sense of motion—acceleration/gyration | ● Unable/unwilling to cross physical barriers |
| ● Seeing light & people | ● Bumpy return to body—weight/pain |
| ● No “moral” qualms when leaving family | |
© 2016 by the author; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marsh, M.N. The Near-Death Experience: A Reality Check? Humanities 2016, 5, 18. https://doi.org/10.3390/h5020018
Marsh MN. The Near-Death Experience: A Reality Check? Humanities. 2016; 5(2):18. https://doi.org/10.3390/h5020018
Chicago/Turabian StyleMarsh, Michael N. 2016. "The Near-Death Experience: A Reality Check?" Humanities 5, no. 2: 18. https://doi.org/10.3390/h5020018
APA StyleMarsh, M. N. (2016). The Near-Death Experience: A Reality Check? Humanities, 5(2), 18. https://doi.org/10.3390/h5020018