Towards Integrated Care for Chronic Patients in Belgium: The Pilot Project, an Instrument Supporting the Emergence of Collaborative Networks

{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Background
- -
- The framework of project management stated by Segrestin pertaining to the sociology of organisations;
- -
- The framework of public policy instruments of Lascoumes and Le Galès belonging to the sociology of public action—this framework has already been used to analyse the specific case of an urban project, but not yet to analyse pilot projects in the health sector;
- -
- The framework of sociology of translation by mobilising the work of several authors—Callon, Latour, Akrich, Monaghan, and Freeman.
1.2. Pilot Project: Two Words for One Single Public Policy Instrument
2. Materials and Methods
- Written documents through a literature study (scientific literature) and a documentary analysis (political, legal, and operational documents);
- Actions and interactions through direct observation (attendance at 67 meetings—148 h in total): 100 h were spent attending and observing meetings (preparatory meetings during the conceptualisation phase, follow up meetings during the execution phase, etc.) of two pilot projects (35 h for the first project and 70 h for the second one). The researcher also attended plenary sessions and intervisions organised by the public authorities (43 h) to observe what was happening through interactions and to observe innovation in action;
- Discourses: the researcher conducted 24 semi-structured interviews, lasting between 33 and 98 min, with different categories of actors—policy-advisers and public officials involved in devising and implementing the new policy, pilot project coordinators, and pilot project stakeholders. Furthermore, this research relies on data collected via seven focus groups (n = 7–16, 5 h) on the topic of governance, the purpose of which was to determine the governance modalities of three projects (the two mentioned above and a third additional project).
3. Results
3.1. Launching Integrated Care Pilot Projects: A Phased Process
- The preparation phase and the conceptualisation phase, which are the two phases of the selection procedure, during which field actors designed their projects together;
- The execution phase, which began in January 2018, which should last for four years, and during which the twelve out of the fourteen selected pilot projects (two pilot projects gave up) are expected to implement their “loco-regional action plan” (see below);
- The expansion phase, which will occur after the four-year execution phase, during which the successful pilot projects will have to evolve to cover the entire Belgian population.
- The preparation phase (first phase of the selection procedure): in February 2016, the authorities launched a call for expressions of interest, which marked the beginning of the four-month preparation phase. Field actors who were interested in creating a pilot project had to constitute multidisciplinary local consortia. By doing so, the political will was to gather a variety of people working with chronic patients so that each consortium properly reflected the care offer of the geographical zone covered by its project. Stakeholders had to submit a joint expression of interest approximately defining their target groups, as well as the geographic area covered by their projects, by May 31, 2016. This expression of interest had to be signed by all of the partners who had joined the pilot project consortium.
- The conceptualisation phase (second phase of the selection procedure): between July 2016 and September 2017, each of the twenty selected pilot project consortia had to write a more detailed application file containing a loco-regional action plan. In this plan, pilot project stakeholders had to describe their common vision, their strategic and operational objectives, as well as the actions they would implement to achieve their objectives if they were selected for the four-year execution stage. These had to be based on an analysis of local needs, of available and missing resources in the pilot zone, as well as a risk stratification pertaining to their respective populations.
- a financial plan;
- a communication plan;
- a time line taking the form of a Gantt Chart;
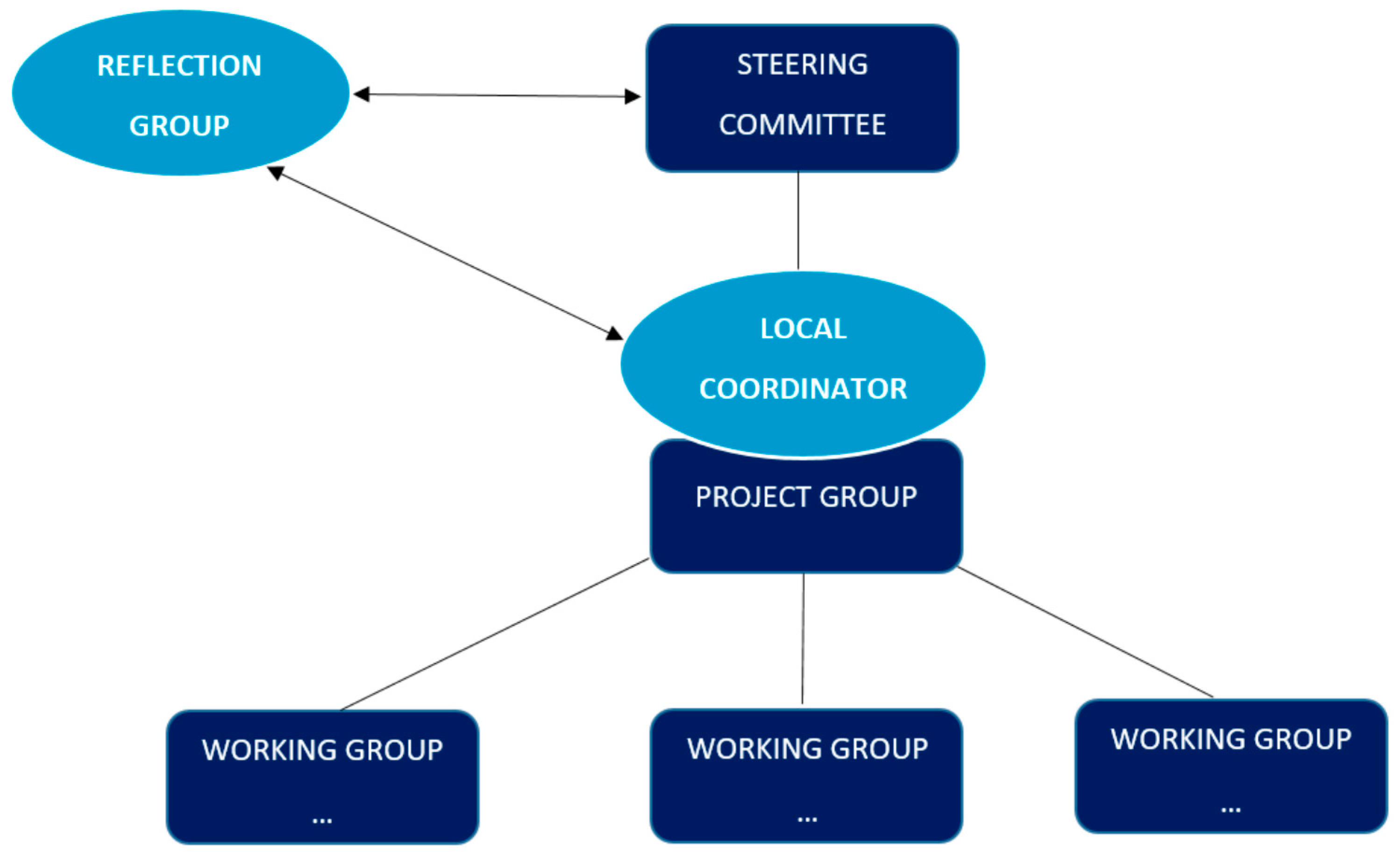
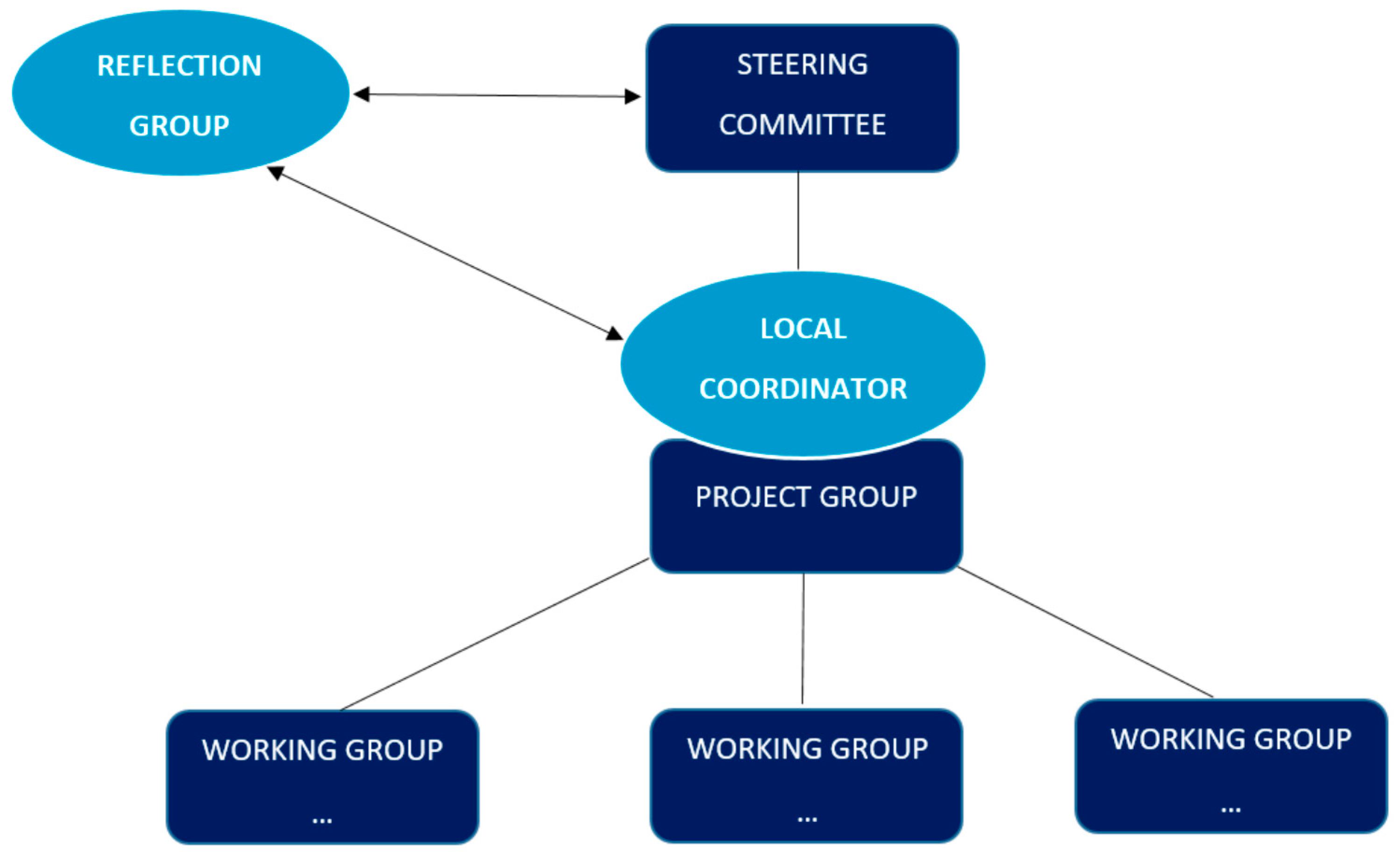
- the description of their future governance structure and legal personality;
- a description of how responsibilities would be distributed among partners during the execution phase [2].
3.2. Financial Aspects
3.3. Building Integrated Care Pilot Projects
“The divisions are different [in the integrated care projects]. In x [name of the project], you can find public and private providers, you have everything. Why would it be this federation instead of this one that would [take the lead]? The conflict resides [in] this pillar logic, i.e., this logic of ideological and confessional division, which has structured the Belgian society since the outset. We would try to evolve towards something more rational in the 21st century, which is not only based on political convictions or beliefs. […] We would try to evolve towards something more rational”(Interview with a pilot project member, 2018).
3.4. Empirical Example: Choosing a Governance Structure and Legal Personality for the Future Execution Phase
- -
- A session for a first project, during which the participants were divided into three focus groups gathering ten to fifteen people and lasting three hours each;
- -
- A joint session for two projects, during which the participants were divided into four focus groups gathering ten to fifteen people and lasting two and a half hours each: these two projects had common stakeholders and considered the possibility of pooling resources, which explains why it was decided to organise a joint session.
4. Discussion
4.1. The Case of Integrated Care Pilot Projects: Emerging Collaborative Networks
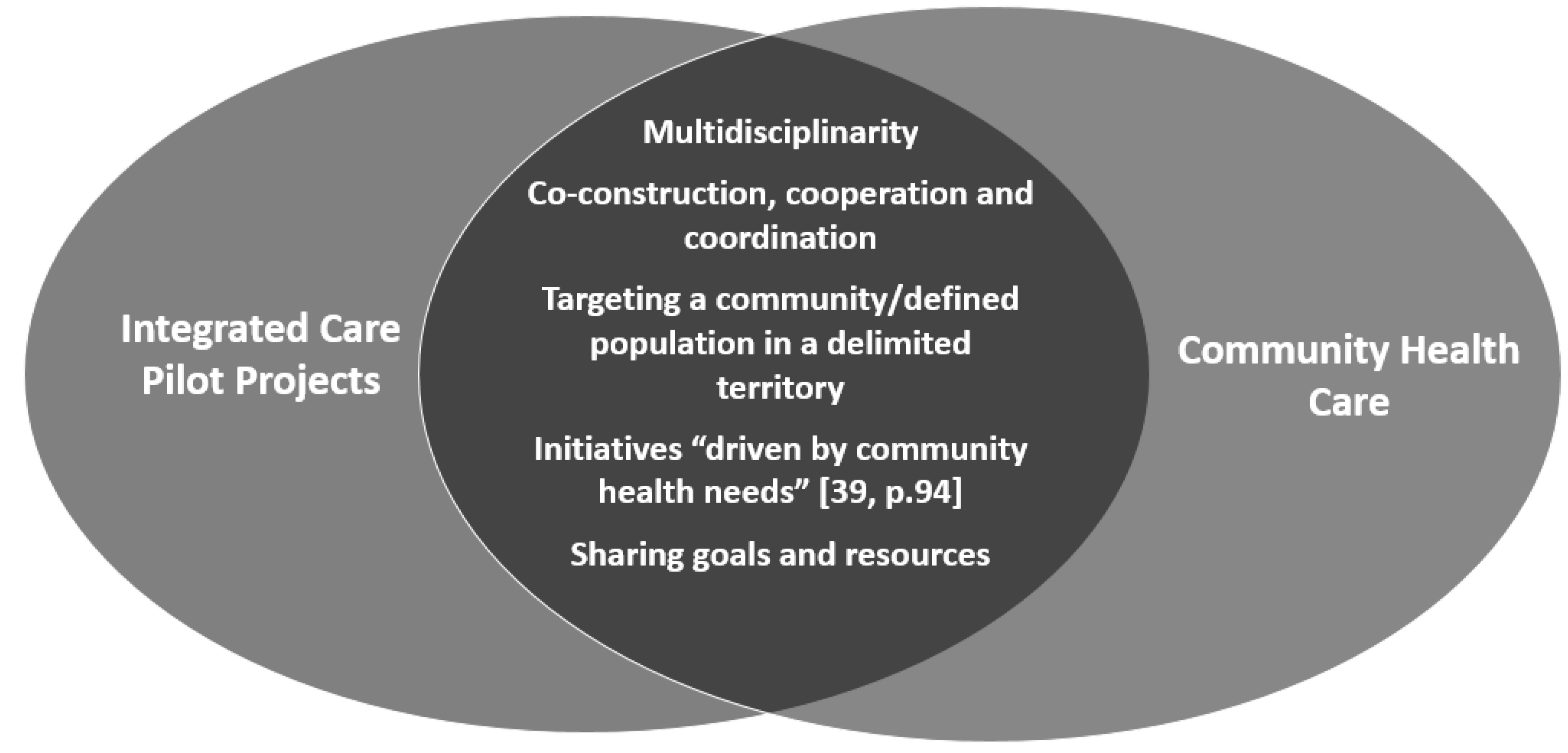
4.2. Collaboration as a Means, Collaboration as an End to Integrating Care
5. Conclusions
Funding
Conflicts of Interest
References
- Amelung, V.; Stein, V.; Goodwin, N.; Balicer, R.; Nolte, E.; Suter, E. (Eds.) Handbook Integrated Care; Springer International Publishing: Cham, Switzerland, 2017; Available online: http://link.springer.com/10.1007/978-3-319-56103-5 (accessed on 19 September 2018).
- Belgian Ministry of Social Affairs and Public Health. Plan Conjoint en Faveur des Malades Chroniques: «Des Soins Intégrés Pour Une Meilleure Santé». 2015. Available online: http://www.integreo.be/sites/default/files/public/content/plan_fr.pdf (accessed on 4 December 2018).
- Riley, L.; Gouda, H.; Cowan, M. Noncommunicable Diseases Progress Monitor; World Health Organization: Geneva, Switzerland, 2017; Available online: http://apps.who.int/iris/bitstream/10665/258940/1/9789241513029-eng.pdf (accessed on 12 September 2018).
- Paulus, D.; Van den heede, K.; Mertens, R. Organisation Des Soins Pour Les Malades Chroniques en Belgique: Développement d’un Position Paper (Report No. 190B); Centre Fédéral d’Expertise des Soins de Santé (KCE)-Health Services Research (HSR): Bruxelles, Belgium, 2012; Available online: https://kce.fgov.be/sites/default/files/page_documents/KCE_190B_organisation_soin_malades_chroniques_0.pdf (accessed on 16 January 2017).
- World Health Organization. Noncommunicable Diseases (NCD) Country Profiles—Belgium; World Health Organization: Geneva, Switzerland, 2018; Available online: http://www.who.int/nmh/countries/2018/bel_en.pdf?ua=1 (accessed on 4 February 2019).
- Ording, A.; Sørensen, H. Concepts of comorbidities, multiple morbidities, complications, and their clinical epidemiologic analogs. Clin. Epidemiol. 2013, 5, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Schokkaert, E.; Van de Voorde, C. Belgium’s Healthcare System. Should the Communities/Regions Take It Over? Or the Sickness Funds? 2011. Available online: http://www.rethinkingbelgium.eu/rebel-initiative-ebooks/ebook-10-belgium-healthcare-system-communities-regions-take-over-sickness-funds (accessed on 6 February 2017).
- OECD.stat. Health Expenditure and Financing. 2017. Available online: https://stats.oecd.org/viewhtml.aspx?datasetcode=SHA&lang=en (accessed on 14 August 2018).
- Van der Heyden, J.; Charafeddine, R. Enquête de Santé 2013. Rapport 1: Santé et Bien- Être. Résumé Des Principaux Résultats D/2014/2505/53—Référence Interne: PHS Report 2014-031. 2014. Available online: https://his.wiv-isp.be/fr/Documents%20partages/summ_HS_FR_2013.pdf (accessed on 20 August 2018).
- Baszanger, I. Les maladies chroniques et leur ordre négocié. Revue Française de Sociologie 1986, 27, 3–27. [Google Scholar] [CrossRef]
- Czernichow, P. Un système de santé plus intégré pour mieux prendre en charge les maladies chroniques. Santé Publique 2015, 1, 7–8. [Google Scholar] [CrossRef] [PubMed]
- Thunus, S. The system for addressing personal problems. In From Medicalisation to Socialisation: Shifts in Belgian Mental Health and Psychiatric Institutions; Université de Liège: Liège, Belgium, 2015. [Google Scholar]
- Mangez, E. Global Knowledge-based Policy in Fragmented Societies: The case of curriculum reform in French-speaking Belgium: European Journal of Education, Part, I. Eur. J. Educ. 2010, 45, 60–73. [Google Scholar] [CrossRef]
- De Troyer, M.; Krzeslo, E. Assurance maladie, soins de santé et sécurité sociale: Trois éléments indissociables. Chronique Internationale de l’IRES 2004, 91, 113–122. [Google Scholar]
- WHO. Global Status Report on Noncommunicable Diseases 2014: Attaining the Nine Global Noncommunicable Diseases Targets; a Shared Responsibility; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- WHO. Integrated Health Services—What and Why? Technical Brief No.1.2008; World Health Organization: Geneva, Switzerland, 2008; Available online: http://www.who.int/healthsystems/service_delivery_techbrief1.pdf (accessed on 23 January 2017).
- Berwick, D.M.; Nolan, T.W.; Whittington, J. The Triple Aim: Care, Health, and Cost. Health Aff. 2008, 27, 759–769. [Google Scholar] [CrossRef]
- Buttard, A.; Santos, C.D.; Tizio, S. Networking Healthcare. From a competitive call to a medical cooperation as a guarantee of a found confidence. Recherches en Sciences de Gestion 2012, 6, 21–43. [Google Scholar] [CrossRef]
- Hall, P.A. Policy Paradigms, Social Learning, and the State: The Case of Economic Policymaking in Britain. Comp. Polit. 1993, 25, 275–296. [Google Scholar] [CrossRef]
- Lascoumes, P.; Le Galès, P. (Eds.) Gouverner par les Instruments; Presses de la Fondation Nationale des Sciences Politiques: Paris, France, 2004; 370p. [Google Scholar]
- Vreugdenhil, H.; Ker Rault, P. Pilot Projects for Evidence-Based Policy-Making: Three Pilot Projects in the Rhine Basin. In German Policy Studies; EBSCO Industries, Inc.: Birmingham, AL, USA, 2010; pp. 115–151. [Google Scholar]
- Zurlo, F.; dos Nunes, V.G.A. Designing Pilot Projects as Boundary Objects; Springer International Publishing: Cham, Switzerland, 2016; Available online: http://link.springer.com/10.1007/978-3-319-23141-9 (accessed on 14 December 2017).
- Segrestin, D. Les Chantiers du Manager; Colin: Paris, France, 2004; 343p. [Google Scholar]
- Dumoulin, P.; Dumont, R.; Bross, N.; Masclet, G. Travailler en Réseau: Méthodes et Pratiques en Intervention Sociale; Dunod: Paris, France, 2015. [Google Scholar]
- March, J.G. Exploration and Exploitation in Organizational Learning. Organ. Sci. 1991, 2, 71–87. [Google Scholar] [CrossRef]
- Engström, S.; Lidelöw, S. From the Pilot Project to the Mainstream Practice—Learning Explored in Planning and Design of a Low-Energy Quarter. Procedia Econ. Financ. 2015, 21, 288–296. [Google Scholar] [CrossRef]
- Vreugdenhil, H.; Taljaard, S.; Slinger, J.H. Pilot projects and their diffusion: A case study of integrated coastal management in South Africa. Int. J. Sustain. Dev. 2012, 15, 148–172. [Google Scholar] [CrossRef]
- Callon, M. Some Elements of a Sociology of Translation: Domestication of the Scallops and the Fishermen of St Brieuc Bay. Sociol. Rev. 1984, 32 (Suppl. 1), 196–233. [Google Scholar] [CrossRef]
- Freeman, R. What is ‘translation’? Evid. Policy 2009, 5, 429–447. [Google Scholar] [CrossRef]
- Musselin, C. Sociologie de l’action organisée et analyse des politiques publiques: Deux approches pour un même objet? Revue Française de Science Politique 2005, 55, 51. [Google Scholar] [CrossRef]
- Jick, T.D. Mixing Qualitative and Quantitative Methods: Triangulation in Action. Adm. Sci. Q. 1979, 24, 602–611. [Google Scholar] [CrossRef]
- Contandriopoulos, A.-P.; Denis, J.-L.; Touati, N.; Rodriguez, R. Intégration de soins: Dimensions et mise en oeuvre. Ruptures Revue Transdisciplinaire en Santé 2001, 8, 38–52. [Google Scholar]
- WHO. Integrated Care Models: An Overview. 2016. Available online: http://www.euro.who.int/__data/assets/pdf_file/0005/322475/Integrated-care-models-overview.pdf (accessed on 13 March 2017).
- Schweyer, F.-X.; Levasseur, G.; Pawlikowska, T. Créer et Piloter un Réseau de Santé: Un Outil de Travail Pour Les Équipes; de L’ecole Nationale de la Santé Publique: Rennes, France, 2002.
- Akrich, M.; Callon, M.; Latour, B.; Monaghan, A. The key to success in innovation part II: The art of choosing good spokespersons. Int. J. Innov. Manag. 2002, 6, 207–225. [Google Scholar] [CrossRef]
- Prévot, M. L’approche Communautaire: Un Liant Interdisciplinaire? Santé Conjuguée. 2016. Available online: File:///C:/Users/M%C3%A9lanie/Downloads/sc74_def_prevost_approche_com.pdf (accessed on 12 September 2017).
- Powell, W. Neither Market nor Hierarchy; Network Forms of Organization. In Research in Organizational Behavior; Staw, B.M., Cummings, L.L., Eds.; JAI Press: Greenwich, UK, 1990; pp. 295–336. [Google Scholar]
- Plochg, T.; Klazinga, N.S. Community-based integrated care: Myth or must? Int. J. Qual. Health Care 2002, 14, 91–101. [Google Scholar] [CrossRef] [PubMed]

© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Winter, M. Towards Integrated Care for Chronic Patients in Belgium: The Pilot Project, an Instrument Supporting the Emergence of Collaborative Networks. Societies 2019, 9, 28. https://doi.org/10.3390/soc9020028
De Winter M. Towards Integrated Care for Chronic Patients in Belgium: The Pilot Project, an Instrument Supporting the Emergence of Collaborative Networks. Societies. 2019; 9(2):28. https://doi.org/10.3390/soc9020028
Chicago/Turabian StyleDe Winter, Mélanie. 2019. "Towards Integrated Care for Chronic Patients in Belgium: The Pilot Project, an Instrument Supporting the Emergence of Collaborative Networks" Societies 9, no. 2: 28. https://doi.org/10.3390/soc9020028
APA StyleDe Winter, M. (2019). Towards Integrated Care for Chronic Patients in Belgium: The Pilot Project, an Instrument Supporting the Emergence of Collaborative Networks. Societies, 9(2), 28. https://doi.org/10.3390/soc9020028