Abstract
Clinical practice guidelines (CPGs) are essential for current medical professions since they prevent clinical practice from being based on personal opinions, bias, or individual experience. CPGs are technologies used to govern clinical practice because they guide decision making considering the best available evidence and patients’ values and preferences. In Colombia, studies associated with CPGs and medical professions are scarce; the few available have considered CPGs as a tool for standardization, improving health care efficiency, and quality, and have identified barriers against their implementation. Studies from the medical humanities, sociology, and medical philosophy perspectives are nonexistent. The objective of this study was to analyze the way in which 311 physicians perceive CPGs, the difficulties associated with implementation, the way in which CPGs set and condition individual and collective professional autonomy, and its effect on patient–physician relationships. Our findings revealed that CPGs may be understood as tools used to govern medical judgment and the medical professions with limited implementation in the Colombian health system, but which have become significant mechanisms placing medicine close to the highest scientific, professional, and ethical standards.
1. Introduction
Evidence-based medicine (EBM) uses the best available scientific evidence in a conscious, explicit, and judicious way to improve clinical care and decisions regarding individual patients [1]. It has also been defined as a new paradigm for medical training and practice, which goes beyond the traditional model based on physicians’ authority, by means of three aspects: (i) careful examination of available scientific evidence to help a specific patient; (ii) assessment of available human, technological, and economic resources for health care; and (iii) patients’ values associated with clinical decisions [2,3] This way of reasoning and practicing medicine has been described as the most significant contemporary initiative in biomedical practice [4]. Some authors even consider it as important as the discovery of antibiotics and anesthesia [5].
EBM emerged in the 1990s as a response to the limitations of traditional clinical practice based on anatomical and pathophysiological reasoning and guided by individual medical experience. The latter was considered misguiding since it could result in nonexistent cause-and-effect relationships and inaccurate predictions regarding the performance of diagnostic tests and treatment efficacy. EBM emergence was also favored by other factors, such as the variability of medical interventions by geographical area, a higher likelihood of medical error due to the cognitive limitations of human judgment, and excessive costs derived from inefficient interventions [6,7].
Literature criticizing EBM clearly favors evidence gathered through empiric and probabilistic reasoning and underestimates rationality and knowledge gathered through clinical experience [8]. Despite the importance given to clinical experience in some statements, the formal definition of EBM includes the use of data quantified from large patient populations and produced by clinical epidemiology [9]. As Alvan Feinstein previously stated, medical care is increasingly considered a ‘scientific ideology’ in which the language of likelihood and epidemiological criteria is regarded as important to increase the scientific nature of clinical practice [10].
Clinical practice guidelines (CPGs) became the main EBM mechanism since they are based on the best available evidence and apply standards to confirm the validity of therapies, diagnostic tests, and prognoses. CPGs allow for the application of standards that affect medical behavior in uncertain situations, and include the assessment of health care benefits, damages, and costs. CPGs are guidelines that go beyond most general descriptions, since they aim to address relevant aspects for clinical decision making and any values that may affect such decisions [11].
CPGs were developed in the 1970s after the convergence of expert authority, consensus conferences, strict procedural protocols, and consumer (patients) representatives [12] Besides accepting the development of CPGs, EBM added the classification of different evidence levels so that the type of clinical recommendation could be categorized. CPGs developed as the core of EBM by adopting the aims and means of this new paradigm, such as the following: (i) materializing the initial goal of providing physicians with critical capacity to assess medical literature; (ii) summarizing the most important papers or reviews about specific topics; (iii) having easy-to-use tools, which has resulted in considerable expectations about the possibility of influencing physician’s behavior; and (iv) increasing the scientific nature of medical practice, controlling the variability of clinical decisions, and decreasing errors and excessive costs associated with health care.
Authors criticizing CPGs state that its implementation has had negative consequences on medical professionals and patients. According to some physicians, popularization of CPGs has limited individual professional autonomy [13,14] Telling physicians how to practice medicine is often perceived as a way of weakening clinical experience and exposing the profession to scrutiny, substitution, and interference by other disciplines or political control [15,16,17]. Interpretations by social studies suggest that CPGs do not only emerge from the administrative urge to regulate costs and practices, but are also managed by medical professionals themselves to protect their collective professional autonomy from external interference [12,18]. Recent works even suggest that physicians themselves have helped in the creation of guidelines and standards for medical practice in order to regulate the quality of their practice [12]
CPGs critical analyses can be classified into two groups: (i) Those considering that medical standards based on pathophysiology and the heuristics of experience and clinical judgment are displaced by the standardized and objectivized language of probabilistic, and (ii) those that deny such displacement and claim that new knowledge, ways of reasoning, and techniques are transforming the traditional clinical [19]. According to the latter, the mechanization of medical judgment beclouds the collective experience of specialists associations, the rigorous behavior of consensus conferences and expert panels when developing guidelines [20]. CPGs can alter he patient–physician relationship [20], and patients’ influence on their own health-disease paths is highly limited [21]. Several empirical studies have shown that health professionals believe standardized therapies to be significant obstacles and limitations against the empathy they may feel towards their patients, since they limit the time and space needed to approach the multiple dimensions of disease [22].
Arianne Hanemaayer analyzed CPGs using theoretical resources collected from the works by philosopher Michel Foucault, and showed that CPGs function as political government technologies; she developed a database with disciplinary sanctions by Canadian medical courts and found that CPGs are used to discipline physicians and support sanctions for unprofessional behavior. In these cases, the purpose and effect of the disciplinary action is not the body but the clinical judgment; CPGs act as government technologies since they are conduct codes that determine the clinical or paraclinical evidence related with diagnosis and medical interventions; they guide decision-making behaviors and sanction deviations or lack of adherence [23].
In Colombia, CPGs have not been incorporated as rapidly as in Canada, United States, and European countries, because of the poor development of health technology infrastructure, limited budget for clinical research, problems associated with development and argumentation in general research, separation of medical and epidemiological training, and debates regarding the health system (coverage, access, and quality) that displace and make other topics invisible, such as structural factors. In 2019, the Cochrane collaboration officially opened an office in Colombia; and the Instituto de Evaluación de Tecnologías Sanitarias ([IETS], Institute for the Assessment of Health Technologies) was founded in 2011 with the purpose of assessing health technologies based on scientific evidence, guidelines, and protocols on procedures, drugs, and therapies [24]. Since that year, the Ministry of Health and Social Protection of Colombia has published 58 CPGs, which add to the eleven guidelines published by the IETS, four protocols, and the cost-effectiveness analysis of more than 20 therapeutic options [25]. At the same time, EBM courses have been gradually incorporated into medical curricula, and nowadays it is commonly taught in almost every medical college of Colombia [26].
Studies associated with CPGs and medical professions are scarce in Colombia, as it was found through the following search strategy applied in the PubMed database (Colombia [Title/Abstract]) AND (“clinical practice guidelines” [Title/Abstract]). The few available studies have considered CPGs as a tool for increasing standardization and improving health care efficiency and quality, and have identified barriers against their implementation [27,28,29,30]. In these publications, lack of critical analysis by social and humanistic studies can be confirmed. In Colombia, studying CPGs from social, philosophical, and critical approaches may help to (i) reduce, to a certain extent, the considerable research gap in this field; (ii) clarify whether EBM has been incorporated as a way of governing medical practice uncertainties and the patient–physician relationship; and (iii) reveal situations in which CPGs implementation results in non-observance of ethical aspects associated with health care considering the increasing trend towards medical practice standardization.
The objective of this study was to analyze CPGs as a government technology of the medical professions in Medellín, Colombia.
2. Materials and Methods
Type of Study: Cross-Sectional
Study location: Colombia has 65 medicine schools, 33 of which have a high-quality certification [31]. In Medellín there are six medicine schools which graduate around 250 doctors and specialists each year, in the areas of surgery, gynecology, internal medicine, neurology, psychiatry, orthopedics, and rheumatology [32].
Study population: A total of 311 physicians working in the city of Medellín, Colombia, were selected. The number of physicians was defined considering an expected standard deviation of 25 points (0–100 scale) in the data collection instrument, 3% accuracy, 95% confidence, 15% sampling correction, and a reference population of 13,168 physicians [33]. Snowball sampling and maximum variation (by age, professional experience, etc.) was conducted until 313 participants were obtained.
In the recruitment of participants two methods were used: E-mail invitations using lists collected from the databases of medical graduates, medical associations, and health service provider organizations (HPOs) with the prior approval of their coordinators and in-person meetings in the HPOs. During the in-person meeting, the project was explained to those professionals who agreed to participate in the study; in both cases, the instrument (CPGs scale) was self-applied. Interviewer, instrument, and interviewee bias were monitored during data collection. The interviewer received training that included a protocol with operational variable definitions and guidelines on field work. A pilot test was conducted to ensure the reproducibility and psychometric validity of the instrument (as it will be described below), and interviewee’s responses were confidential and anonymous. Data was collected between September 2020 and April 2021.
Design of the data collection instrument: A CPGs scale was designed for data collection follow the procedure describe in the Figure 1. The scale consists of four constructs: (i) Perception of CPGs; (ii) favoring factors and barriers against their implementation; (iii) implications of CPGs on professional autonomy; and (iv) effects of CPGs on the patient–physician relationship. There was an initial section with questions on demographic aspects (age and sex), professional education, work experience, and CPGs use. Responses to each index item were based on a 5-level Likert scale, and together form a scale of 0–100 points according to the following formula:
([Score obtained − minimum possible score]/[maximum score − minimum]) × 100
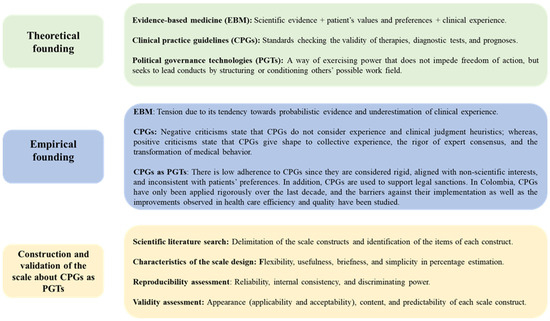
Figure 1.
Description of the construction and validation process of a CPGs scale with government technology.
Results were interpreted considering that the higher the score, the better the perceptions on CPGs in each construct (The scale was made up of four independent constructs for the following reasons: (i) They may be used as independent constructs by other researchers without affecting their reproducibility and validity (they do not need to use the four dimensions of the scale); (ii) according to the level of CPGs development and implementation in other contexts, new items could be added to each construct, and the score of such construct may be recalculated, which adds flexibility and versatility if the construct was to be investigated in other places or institutions; and (iii) a general score of the four dimensions can also be generated by applying the formula mentioned above to all items.
The first construct focuses on aspects that have been repeatedly mentioned both in the literature against and those in favor of CPGs and which are about their usefulness for diagnosis confirmation, treatment initiation, complication management, treatment quality improvement, and medical error reduction [6,34]. The second construct is based on different studies analyzing barriers such as difficulties associated with CPGs interpretation, finding information in CPGs, lack of time, and financial limitations in their application [35,36,37]. The third construct includes aspects found in literature such as legal and labor conflicts associated with non-adherence to the guidelines, regulation of the medical profession by non-medical areas, and reduction of individual autonomy and clinical discretion [18,34]. Finally, the fourth construct measures perceptions of how CPGs affect the patient–physician relationship [38]
Psychometric assessment of the instrument: In terms of reproducibility, reliability was determined with Cronbach’s alpha (satisfactory >0.70), internal consistency or correlation between each item and its construct (satisfactory Spearman’s rho ≥0.30), and discriminatory power by obtaining Spearman’s rho correlation between each item and the construct to which they do not belong (a rho <1 for internal consistency was considered satisfactory). Regarding validity, we assessed appearance, content, and prediction criteria; for appearance, applicability was determined considering the criteria of five experts (epidemiologists, medical ethic professors, and EBM professors) and acceptability was determined by applying the scale to ten study subjects. Content validity was determined through an exploratory factor analysis (main component extraction method) with λ coefficients or factor loads (satisfactory ≥0.30). Finally, predictability was determined with the variance percentage explained by the items of each construct.
Analysis of information: Qualitative variables were described by estimating absolute (n) and relative frequencies (%) with their 95% confidence intervals (CI); whereas, quantitative variables were expressed as median and interquartile range (IQR) since they were not adjusted to normal distribution. Comparison of demographic aspects (age group and sex), professional education, work experience, and CPGs use with the four scale constructs was made with Mann–Whitney U Test and Kruskal–Wallis H test after checking non-compliance of the normality assumption with Lilliefors-corrected Kolmogorov–Smirnov test. A linear regression model was developed to identify confounding variables and factors potentially explaining the score of each construct. Analyses were conducted on SPSS software version 27.0 and p-values <0.05 were considered significant.
3. Results
The four constructs of the scale about CPGs as a government technology showed satisfactory reproducibility and validity (Table 1).

Table 1.
Analysis of the reliability, internal consistency, and discriminatory power of the scale.
In the study group, the mean age was 37 years (IQR 29–46); 43.7% (95% CI = 38.3–49.3) of participants were women and 24.4% (95% CI = 19.9–29.4) were specialized physicians, mainly from the Internal Medicine (4.8%), Emergency Medicine (4.5%), Obstetrics and Gynecology (4.5%), and Pediatrics (3.9%) areas. 16.4% (95% CI = 12.6–20.8) had one year of working experience; regarding CPGs use, 84.9% (95% CI = 80.6–88.5) said that they always or almost always used them in medical practice (Table 2).
Table 2.
Description of demographics, professional education, work experience, and CPGs use.
In general, CPGs were positively perceived, with a median of 70.0 points (IQR 65.0–80.0). 90.7% of participants think CPGs are based on the best available evidence; 88.4% believe that they are useful to confirm diagnoses, initiate treatments, and manage complications; and 71.1% state that they reduce medical error (Figure 2). The score for this construct was lower among women (p-value < 0.001), among those who never use CPGs (p-value = 0.003 **), and among those who knew the lowest number of CPGs (p-value < 0.001 **) (Table 3). In the facilitators and barriers construct, the score was also good, with a median of 70.0 (IQR 55–80), suggesting that not many barriers are perceived against CPGs use. It is worth mentioning that 46.9% of physicians state that they do not have time to consult the CPGs during medical consultations, and 19.9% describe them as difficult to interpret the information contained in them (Figure 2). The greatest barriers were perceived by women (p-value = 0.035 **), physicians that never or seldom use CPGs (p-value = 0.002 **), and physicians knowing between one and four CPGs (p-value < 0.001 **) (Table 3).
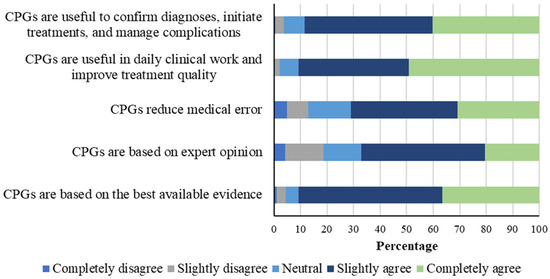
Figure 2.
Relative frequency of general perceptions of CPGs.
Table 3.
Comparison of general perceptions, facilitators and barriers, professional autonomy, and patient–physician relationship based on demographic characteristics, professional education, work experience, and CPGs use.
In the construct of facilitators and barriers, the score was also good with a median of 70.0 (IQR 55-80), indicating that there are not perceived many barriers to their use (Figure 3). It is noteworthy that 46.9% of the physicians assert that there is not enough time during medical appointments to consult the Clinical Practice Guidelines (CPGs), and 19.9% agree that interpreting the information contained in them is challenging (Figure 2). Those who perceive greater barriers include women (p-value = 0.035 **), physicians who never use them or do so infrequently (p-value = 0.002 **), and those who are familiar with between one and four CPGs (p-value < 0.001 **). See Table 3 for details.
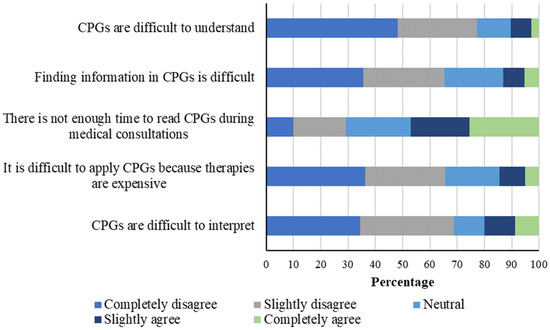
Figure 3.
Relative frequency of CPGs facilitators and barriers.
Professional autonomy was the worst-perceived construct, with a score of 60 (IQR 50–75). It can be highlighted that only 9% of participants agreed when asked directly whether CPGs reduce autonomy; 47.6% considered that non-adherence to CPGs may cause labor problems and 54% indicated that it could lead to legal conflict (Figure 4). In this construct, scores were low for all participants, a worse result being observed among those seldom using CPGs (p-value = 0.027 **) and those who were familiar with one or two CPGs (p-value = 0.026 **) (Table 3).
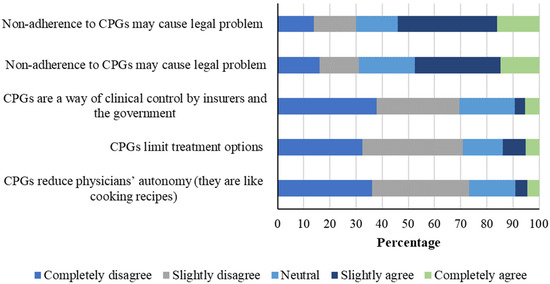
Figure 4.
Relative frequency of the professional autonomy construct.
The construct describing the way in which CPGs affect the patient–physician relationship yielded a score of 65.0 (IQR 55–80) (Figure 5). Herein, it was observed that 29.9% think that CPGs and standardized formats are an obstacle to develop empathy toward patients, and 16.1% state that CPGs hinder individualized patient approach. The worst perception was found among those never using CPGs (p-value = 0.002**) and those knowing between one and four CPGs (Table 3).
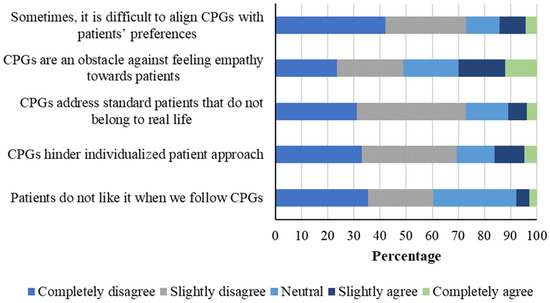
Figure 5.
Relative frequency of the patient–physician relationship construct.
The potentially explanatory factors for the attitudes observed towards CPGs in the study group were sex, number of CPGs known, constructs of facilitators and barriers, professional autonomy, and patient–physician relationship. For the facilitators and barriers construct, potential explanatory factors are years of experience, frequency of CPGs use, the constructs of attitude towards CPGs, facilitators and barriers, and patient–physician relationship. In the case of professional autonomy, the results of the remaining three constructs (general attitude towards CPGs, facilitators and barriers, and patient–physician relationship) were significant. Regarding the patient–physician relationship construct, explanatory factors included number of CPGs known and the scores in attitude towards CPGs, facilitators, barriers, and professional autonomy (Table 4).
Table 4.
Linear regression analysis conducted with the potential explanatory factors for scores of each construct.
4. Discussion
Herein, results are interpreted according to theoretical approaches by social studies of medicine, governability studies, and medicine philosophy. Our findings are extremely useful for scholars, researchers, managers, and other professionals focused on education, medical ethics, and social studies of medicine, since they offer a reinterpretation of essential concepts such as professional autonomy, clinical freedom, and discretion based on experience and clinical judgment in the light of empirical data.
4.1. General Perception of CPGs
The fact that 84.9% of participants always or almost always use CPGs reflects their presence in decision making and their efforts to follow professional, institutional, and scientific decrees. The high score observed in this construct demonstrates that the study subjects approve CPGs use, so a subsequent implementation of interventions based on the best available evidence may be assumed. This is a significant finding given the slow development of CPGs in Colombia, which were introduced in the 1990s by resources such as the Normas y Guías de Atención de las Acciones del Plan Obligatorio de Salud (Health Care Rules and Guidelines for the Mandatory Health Plan Actions) in 1998 and resolution no. 412 in 2000 [39]. These mechanisms have played an important role since they have set forth activities, procedures, and cost-effective interventions whose implementation was mandatory, reflecting the intention to communicate some of the EBM goals.
CPGs acceptance by the study physicians was not consistent with the resistance observed in other countries, where it has been said that CPGs negatively affect physicians’ autonomy, annul their clinical judgment, deviate them from traditional professional goals, hinder individualized patient approach, etc. This nonconformity is reflected by the low adherence to CPGs use reported in different studies. For example, a study showed that only 55% of physicians apply CPGs recommendations [40]. Specifically, in the case of CPGs for septic patients, a study showed that, in spite of a wide media campaign, less than 20% of the indications were followed. After a significant educational effort was made, the percentage only increased to 38% [41]. Besides logistics (time, space, and resources), reasons for rejecting CPGs include that they are conceived as ‘cook recipes’, they are not practical, they protect interests that go beyond science, they are too rigid, and, sometimes, they go against patients’ preferences [42,43].
Therefore, significant efforts have been made over the last twenty years to promote CPGs and EBM worldwide [44]. These guidelines have been institutionalized and incorporated into physicians’ daily routine with the intention of improving the quality of medicine and increasing its scientific nature, increasing the authority of medical professionals by establishing their practice on scientific criteria, reducing the gaps between research and clinical practice, and minimizing variation. More specifically, the website of the Ministerio de Salud y Protección Social of Colombia describes the guidelines as informative documents with recommendations focused on patients’ health care and based on systematic evidence reviews as well as on benefits and damages assessments. The purpose of these ‘texts’ is to state what should and should not be done in terms of prevention, diagnosis, and treatment. Guidelines are designed to decrease the “unexplainable variability of clinical practice,” outdated knowledge, intervention inefficiency, and health care issues [25], which reflects their significant role in the management of different and frequent events and issues observed in professional practice.
The fact that most study participants regard CPGs as a reliable tool that can be continuously used also reflects an institutional effort to control and govern professional uncertainty. CPGs function is supported by ‘devices’, which are sets with a practical reasoning structure that are governed by quite conscious objectives that include instruments, people, judgment systems, buildings, and spaces “with programmatic support by certain presumptions and assumptions on human beings” [45]. In this sense, we should remember that CPGs development in Colombia has depended on the assembly and alliance of different public administration and academic agencies, given that CPGs configuration and creation in Colombia took place thanks to the efforts by university groups of Universidad de Antioquia, Pontificia Universidad Javeriana, and Universidad Nacional de Colombia, who originally created the Alianza Centro de Investigaciones en Evaluaciones de Tecnologías en Salud (Center of Research on Health Technologies Assessment Alliance) in 2009 and who have worked together with the IETS and the Ministry itself to offer rigorous and academic analyses regarding the efficacy, efficiency, cost-effectiveness, and cost-utility of different health technologies [46].
Positive perceptions of CPGs by participants can also be interpreted as physicians acknowledging professional and even legal ‘game rules’ that regulate the medical professions in Colombia. These ‘rules’ entail consideration of the different mechanisms used by institutions to ensure guideline compliance, which range from educating general physicians on clinical epidemiology and EBM to audits and ‘surveillance’ mechanisms to ensure guideline compliance [47].
4.2. CPGs Facilitators and Barriers
The CPGs facilitators and barriers construct showed that participants do not perceive many barriers against the use of guidelines given that the result obtained was 70 points (IQR 55–80). Most of the participants stated that CPGs were not difficult to understand, they facilitate their search for specific information, and they can be easily interpreted, which is not consistent with the usual complaints reported for other instruments such as protocols [34,48]. This also reflects the efforts made to simplify guidelines and promote the pedagogical instrument network of EBM. However, perceptions regarding the time limitations for patient health care should be highlighted, since 46.9% of physicians report not having time to read CPGs during medical consultations, which hinders their integration into clinical practice. According to the Colombian health system regulations, consultations should not last more than 20 min, and some health care institutions have shortened and manipulated these standards in order to increase productivity, setting this threshold as the maximum time for each patient. For this reason, CPGs are not negative on their own, but certain structural and external aspects limit their use. One of the keys to understanding this is the implementation of “neoliberal government technologies” in health care [49]. In Colombia, health service organization, administration, funding, and supply are based on ‘structured pluralism’, which proposes an adjustment between public and private insurance companies and operating health institutions within a regulated market [50]. As some governability scholars state [51], it is a form of governing health ‘at a distance’, regulated by a market logic in which different actors compete against each other to cover population needs in terms of insurance, adapted to the new institutional business culture where values such as profitability and self-sustainability are favored [52,53].
This suggests that the neoliberal mechanisms for health legislation and management, boosted by financial sustainability and demands for productivity, “prevail over semiologic analysis, algorithms, or CPGs” [50]. The guidelines challenge other mechanisms or devices exclusively focused on productivity demands, costs control, etc.; even though administrative, economic, and financial viewpoints seem to include CPGs use into economic and productivity obligations, our findings highlight that physicians are aware of a certain degree of individual and collective autonomy against interferences or influences that are external to the medical profession, and limitations that may affect health care and its standards, which may be partially solved by means of guidelines.
For most participants, CPGs are a professional and scientific instrument that simplifies medical practice, but whose full implementation is limited by other types of external regulations. This is consistent with the findings by Weisz et al., who stated that not only should cost control be considered when developing CPGs, but also the fact that they have become significant mechanisms for professionalization and protection of collective autonomy against funders and patients. Furthermore, CPGs reflect physicians’ efforts to regulate medical care and follow scientific standards [12].
4.3. Clinical Practice Guidelines and Professional Autonomy
According to the results in the professional autonomy construct, few participants considered that CPGs limit autonomy given that the score was 60 (IQR 50–75). Even though it is not believed that CPGs reduce autonomy, participants consider that their non-compliance or non-use may cause labor and legal problems. Participants do not perceive CPGs as negatively affecting professional autonomy, but as mechanisms that exercise power over professionals, since they guide their performance by establishing professional and even legal limits. The fact that CPGs are not understood as obstacles against professional autonomy reflects that they have been somehow settled in medical practice, and they have been ‘incorporated’ into medical professions supported by medical auditors and the administrative regulations of health institutions.
Historically, after guidelines were popularized in the United States in the 1970s, different criticizing sectors described the emergence of an intention to deteriorate professional autonomy and physicians’ discretion. After World War II, medicine was considered an autonomous profession in the United States and Europe [7]. However, as of the 1960s, medical elites of scientific journals and universities, as well as non-medical agents such as the government or insurance companies, started to question a series of events that were affecting physicians’ social legitimacy [54]. As Timmermans and Kolker highlighted, extensive clinical autonomy may have decreased trust in medical professionals due to a lack of external controls, which increased costs with inefficient and incompetent care [55]. At the same time, a culture of lawsuits and claims against physicians was emerging: The number of claims due to medical negligence increased 300% from 1965 to 1970 in the United States [56]. Likewise, gaps between scientific research and clinical practice, an increase in the power of medical interventions, human judgment limitations, and a huge geographical variation of professional practice were observed [57]. In this context, guidelines were established as a way of professionalizing medicine and managing these problems [12].
Similarly, in specialized literature there are some studies highlighting that guidelines have been regarded as instruments that decrease health professionals’ medical autonomy, since the latter feel increasingly limited by guidelines created by big corporations or government strategies, frequently with the aim of controlling costs instead of strictly controlling medical care [47,58]. Several experts have stated that even though EBM had initially focused on text publication with pedagogical ends, non-medical agents have profited from guidelines to ‘punish’ physicians’ autonomy by making the latter financially and legally liable for inadequate or incorrect interventions [34].
In our study, CPGs recommendations include scientific statements approaching facts based on probabilistic criteria. Likewise, they guide clinicians through the path of science, compliance with certain professional standards, and the wariness of defensive medicine. We should thus acknowledge that the concept of government and the act of governing itself do not limit and coerce but achieve their goal by guiding and directing behavior toward specific ends. Some works published by social studies have shown that the use of EBM and guidelines to manage uncertainty does not necessarily replace physicians’ knowledge and skills and does not affect their autonomy and freedom. Moreover, different publications state that evidence and experience have jointly become complementary resources [55].
4.4. Effects of CPGs on the Patient–Physician Relationship
Regarding the patient–physician relationship, results showed that 70.1% of physicians do not regard CPGs as an obstacle against feeling empathy, and only 16.1% stated that they hinder individualized approach. These findings are consistent with the efforts undertaken in the last 20 years by EBM advocates to govern the patient–physician relationship toward models increasing patient individualization and a liberal conception of the medical profession, where patients are perceived as autonomous agents and consumers capable of making decisions during the clinical consultation.
Literature reveals that, since the emergence of EBM, the tension between EBM and individual-centered approaches, two professionalization models, has gradually disappeared [38]. The most recent statements by the EBM professional elites suggest an epidemiological approach that enhances individualization by means of a population-based perspective filter. The emphasis given to patients’ values and preferences in decision making and the initiatives to make this process a shared experience reflects a change toward putting patients at the center of the patient–physician relationship. Guyatt and his group emphasized that evidence is never enough, encouraging professionals to consider the patient’s circumstances and values [2].
This kind of ideas has been followed by statements seeking to integrate EBM and shared decision making. Incorporating CPGs into clinical consultations seeks to provide a space for discussion between physicians and patients; in which the construction of informed preferences can be possible by means of the evidence-based deliberation [59]. Physicians are expected to be able to communicate medical information in a clear way and, at the same time, understand the values and preferences described by their patients [60]. Even though most guidelines do not consider patients’ preferences in their recommendations, recent ones have gradually incorporated this aspect as essential within health care. An example of this is the CPGs on prevention, diagnosis, treatment, and rehabilitation of heart failure developed by the Ministerio de Salud y Protección Social of Colombia [61]. This document was designed using a survey conducted on 106 participants with heart failure in order to “identify how they perceive possible outcomes and to approach the local context in order to address their decision-making expectations regarding the management of their disease” [62]. Likewise, the CPG for the management of primary hypertension included surveys conducted on patient groups and focused on the identification of values and preferences.
Participants’ perceptions may be interpreted in view of this significant ethical change that has taken place in medical education over the last 20 years. The development of a patient-centered medicine and evidence-based approach reflects a type of relationship consistent with the characteristics of liberal societies. Acknowledging patients’ values and preferences and engaging them in their health and disease process goes in line with a society centered in choice and risk self-management. In this sense, medical professionals and public and private institutions use guidelines to improve health care quality, to increase physicians’ professionalism, and to regulate costs, as well to govern the patient–physician relationship toward a liberal and individualized model.
4.5. Limitations and Strengths of the Study
The main limitations include the following: (i) it was not possible to perform a probability sampling, to remedy this, a sampling with maximum variation was achieved for central variables of the study such as age, years of professional experience, among others that show the breadth of subjects to which the results can be extrapolated; (ii) the evaluation of some psychometric properties such as sensitivity to change was not included, which was controlled during the pilot test applying the construct in two moments (range four weeks) to 5% of subjects to control changes in the scores intra-participants; and (iii) some results could not be stratified by structural variables of the Colombian health system such as the level of complexity of the clinics in which the doctors work, which are factors that should be investigated in subsequent studies.
Despite these limitations, this research has the following strengths: design and validation of a psychometrically robust construct; inclusion of a large sample of physicians; determination of some dimensions related to the CPGs that are poorly perceived; identification of subgroups that rated the use and impacts of the CPGs with different scores. These elements are decisive to guide the critical application and appropriation of CPGs and improve medical education programs, biomedical ethics, medical practice, and research on different topics.
5. Conclusions
Based on the perceptions analyzed, CPGs may be understood as devices for the government of medical judgment profession with limited implementation in the Colombian health system. They have become significant mechanisms that place medicine closer to the highest scientific, professional, and ethical standards. According to Foucault’s heuristics, the notion of government conveys an idea of power relationships that does not hinder freedom of action, but seeks the ‘conduction of behaviors’ and the prevalence of “some people’s action model over others” [63], where governing means structuring or conditioning others’ possible field of action. In our study, guidelines were perceived as scientific, professional, and administrative mechanisms governing practice, patients, professional autonomy, and the production of evidence-based statements. Understanding guidelines as merely coercive mechanisms that negatively affect physicians’ individual criteria or that standardize patients does not exploit their powerful influence on medical professions. Moreover, our findings revealed the significant epistemological, ontological, and ethical changes in medical professions over the last twenty years in Colombia, which were triggered by the incorporation of EBM and CPGs into medical practice.
As a result of the incursion and deployment of evidence-based guidelines, government of the production and application of medical knowledge has changed. Governing epistemology through the guidelines means considering the effect of clinical epidemiology on the consensus conferences where guidelines are created, the influence of evidence hierarchies in guideline development, and the progressive displacement of knowledge originating from pathophysiological reasoning and accumulated experience in patient care toward a secondary scale in decision-making. Governing knowledge based on epidemiological criteria also entails a change in the image from which patients are governed; whereas, traditional clinical objectivity approaches implied a patient–physician relationship based on immediate experience and individualized knowledge; clinical epidemiological perspectives state that judgment should be filtered in order to minimize interpretations limited by experience by using data based on population criteria. Patients are no longer individual organisms for physicians; their existence is assumed from population data, which has resulted in a new objectification. However, guidelines have also been regarded as government mechanisms interfering with professional ethos, which has been associated with the development of a new way of regarding and approaching the patient–physician relationship.
Author Contributions
Conceptualization, D.A.E.-M. and L.F.H.-G.; methodology, D.A.E.-M., L.F.H.-G. and J.A.C.-A.; validation, D.A.E.-M., L.F.H.-G. and J.A.C.-A.; formal analysis, D.A.E.-M., L.F.H.-G. and J.A.C.-A.; investigation, D.A.E.-M., L.F.H.-G. and J.A.C.-A.; resources, D.A.E.-M., L.F.H.-G. and J.A.C.-A.; D.A.E.-M.; writing—original draft preparation, D.A.E.-M.; writing—review and editing, D.A.E.-M., L.F.H.-G. and J.A.C.-A.; visualization, D.A.E.-M., L.F.H.-G. and J.A.C.-A.; supervision, D.A.E.-M., L.F.H.-G. and J.A.C.-A.; project administration, D.A.E.-M.; funding acquisition, D.A.E.-M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Universidad Cooperativa de Colombia, grant number INV3032.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Universidad Cooperativa de Colombia protocol code No. 027-2020.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data were not deposited in a public repository. Anonymized data are available upon reasonable quest.
Conflicts of Interest
The authors report no conflict of interest in relation to this work and declare no potential conflicts of interest with respect to the research and publication of this article.
References
- Sackett, D.L.; Rosenberg, W.M.C.; Gray, J.A.M.; Haynes, R.B.; Richardson, W.S. Evidence based medicine: What it is and what it isn’t. BMJ 1996, 312, 71–72. [Google Scholar] [CrossRef]
- Montori, V.M.; Guyatt, G.H. What is evidence-based medicine? Endocrinol. Metab. Clin. N. Am. 2002, 31, 521–526. [Google Scholar] [CrossRef]
- Guyatt, G.; Cairns, J.; Churchill, D.; Cook, D.; Haynes, B.; Hirsh, J.; Irvine, J.; Levine, M.; Levine, M.; Nishikawa, J.; et al. Evidence-Based Medicine: A new approach to teaching the practice of medicine. JAMA 1992, 268, 2420. [Google Scholar] [CrossRef]
- Mykhalovskiy, E.; Weir, L. The problem of evidence-based medicine: Directions for social science. Soc. Sci. Med. 2004, 59, 1059–1069. [Google Scholar] [CrossRef]
- Dickersin, K.; Straus, S.E.; Bero, L.A. Evidence based medicine: Increasing, not dictating, choice. BMJ 2007, 334 (Suppl. 1), s10. [Google Scholar] [CrossRef]
- Timmermans, S.; Berg, M. The Gold Standard. The Challenge of Evidence Based Medicine and Standardization in Health Care; Temple University Press: Philadelphia, NY, USA, 2003. [Google Scholar]
- Berg, M. Turning a Practice into a Science: Reconceptualizing Postwar Medical Practice. Soc. Stud. Sci. 1995, 25, 437–476. [Google Scholar] [CrossRef]
- Tonelli, M.R. The challenge of evidence in clinical medicine. J. Eval. Clin. Pract. 2010, 16, 384–389. [Google Scholar] [CrossRef]
- Knaapen, L. Being ‘evidence-based’ in the absence of evidence: The management of non-evidence in guideline development. Soc. Stud. Sci. 2013, 43, 681–706. [Google Scholar] [CrossRef]
- Feinstein, A.R. Clinical Judgment Revisited: The Distraction of Quantitative Models. Ann. Intern. Med. 1994, 120, 799. [Google Scholar] [CrossRef]
- Hayward, R.S.; Wilson, M.C.; Tunis, S.R.; Bass, E.B.; Guyatt, G. Users’ guides to the medical literature. VIII. How to use clinical practice guidelines. A. Are the recommendations valid? The Evidence-Based Medicine Working Group. JAMA J. Am. Med. Assoc. 1995, 274, 570–574. [Google Scholar] [CrossRef]
- Weisz, G.; Cambrosio, A.; Keating, P.; Knaapen, L.; Schlich, T.; Tournay, V.J. The Emergence of Clinical Practice Guidelines. Milbank Q. 2007, 85, 691–727. [Google Scholar] [CrossRef]
- Willis, E.; White, K. Evidence-Based Medicine, the Medical Profesión and Health Policy; Oxford University Press: Melbourne, Australia, 2003. [Google Scholar]
- Rodwin, M.A. The Politics of Evidence-Based Medicine. J. Health Politics Policy Law 2001, 26, 439–446. [Google Scholar] [CrossRef]
- Holmes, D.; Murray, S.J.; Perron, A.; Rail, G. Deconstructing the evidence-based discourse in health sciences: Truth, power and fascism. Int. J. Evid.-Based Healthc. 2006, 4, 180–186. [Google Scholar] [CrossRef]
- Frankford, D.M. Scientism and Economism in the Regulation of Health Care. J. Health Politics Policy Law 1994, 19, 773–799. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D. Clinical sense and clinical science. Soc. Sci. Med. 1977, 11, 599–601. [Google Scholar] [CrossRef]
- Armstrong, D. Clinical autonomy, individual and collective: The problem of changing doctors’ behaviour. Soc. Sci. Med. 2002, 55, 1771–1777. [Google Scholar] [CrossRef]
- Parker, M. Whither our art? Clinical wisdom and evidence-based medicine. Med. Health Care Philos. 2002, 5, 273–280. [Google Scholar] [CrossRef]
- Mykhalovskiy, E. Evidence-Based Medicine: Ambivalent Reading and the Clinical Recontextualization of Science. Health Interdiscip. J. Soc. Study Health Illn. Med. 2003, 7, 331–352. [Google Scholar] [CrossRef]
- Lambert, H. Accounting for EBM: Notions of evidence in medicine. Soc. Sci. Med. 2006, 62, 2633–2645. [Google Scholar] [CrossRef]
- Derksen, F.; Bensing, J.; Kuiper, S.; van Meerendonk, M.; Lagro-Janssen, A. Empathy: What does it mean for GPs? A qualitative study. Fam. Pract. 2015, 32, 94–100. [Google Scholar] [CrossRef]
- Hanemaayer, A. The Impossible Clinic. A Critical Sociology of Evidence-Based Medicine; UBC Press: Vancouver, BC, Canada, 2019. [Google Scholar]
- Congreso de Colombia. Ley 1438. 2023. Available online: www.minsalud.gov.co/Normatividad_Nuevo/LEY%201438%20DE%202011.pdf (accessed on 1 March 2025).
- Ministerio de Salud y Protección Social—República de Colombia. Clinical practice guidelines CPGs [Guías de práctica clínica GPC]. Available online: http://gpc.minsalud.gov.co/gpc/SitePages/buscador_gpc.aspx (accessed on 1 March 2025).
- Sánchez-Duque, J.; Méndez-Hernández, P.; Mendieta, G.; Rodríguez, J.; Gómez-González, J. Educación en salud basada en la evidencia: Una perspectiva de estudiantes de medicina colombianos. RHCS 2020, 3, 159–160. [Google Scholar]
- Patiño-Lugo, D.F.; Pastor Durango, M.d.P.; Lugo-Agudelo, L.H.; Posada Borrero, A.M.; Ciro Correa, V.; Plata Contreras, J.A.; Vera Giraldo, C.Y.; Aguirre-Acevedo, D.C. Implementation of the clinical practice guideline for individuals with amputations in Colombia: A qualitative study on perceived barriers and facilitators. BMC Health Serv. Res. 2020, 20, 538. [Google Scholar] [CrossRef] [PubMed]
- Sánchez Díaz, N.; Duarte Osorio, A.; Gómez Restrepo, C.; Bohórquez Peñaranda, A.P. Implementacion de la guía de práctica clínica para el manejo de adultos con esquizofrenia en Colombia. Rev. Colomb. De Psiquiatr. 2016, 45, 60–66. [Google Scholar] [CrossRef]
- Gómez-Díaz, O.L.; Esparza-Bohórquez, M.; Jaimes-Valencia, M.L.; Granados-Oliveros, L.M.; Bonilla-Marciales, A.; Medina-Tarazona, C. Experiencia en la implantación y consolidación de las Guías de buenas prácticas de la Registered Nurses’ Association of Ontario (RNAO) en el ámbito clínico y académico en Colombia. Enfermería Clínica 2020, 30, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez Moreno, J.H.; Romero Vergara, A.J.; de Alba De Moya, D.D.J.; Jaramillo Rojas, H.J.; Díaz Rojas, C.M.; Ciapponi, A. Evaluación de herramientas de implementación de la Guía de Práctica Clínica de infecciones de transmisión sexual. Rev. Panam. De Salud Pública 2017, 41, 1. [Google Scholar] [CrossRef]
- ASCOFAME. Facultades Afiliadas. 2023. Available online: https://ascofame.org.co/web/facultades-afiliadas/ (accessed on 1 March 2025).
- Ministerio de Educación Nacional. Bases Consolidadas. 2023. Available online: https://snies.mineducacion.gov.co/portal/ESTADISTICAS/Bases-consolidadas/ (accessed on 1 March 2025).
- Ministerio de Salud y Protección Social. Indicadores Básicos de Talento Humano. 2020. Available online: https://www.sispro.gov.co/observatorios/ontalentohumano/Paginas/Observatorio-de-Talento-Humano-en-Salud.aspx (accessed on 1 March 2025).
- Hurwitz, B. Clinical Guidelines and the Law. Negligence, Discretion, and the Judgment; CRC Press: Boca Raton, FL, USA, 1998. [Google Scholar]
- Haynes, B.; Haines, A. Getting research findings into practice: Barriers and bridges to evidence based clinical practice. BMJ 1998, 317, 273–276. [Google Scholar] [CrossRef]
- Taba, P.; Rosenthal, M.; Habicht, J.; Tarien, H.; Mathiesen, M.; Hill, S.; Bero, L. Barriers and facilitators to the implementation of clinical practice guidelines: A cross-sectional survey among physicians in Estonia. BMC Health Serv. Res. 2012, 12, 455. [Google Scholar] [CrossRef]
- Jin, Y.; Li, Z.; Han, F.; Huang, D.; Huang, Q.; Cao, Y.; Weng, H.; Zeng, X.-T.; Wang, X.; Shang, H.-C. Barriers and enablers for the implementation of clinical practice guidelines in China: A mixed-method study. BMJ Open 2019, 9, e026328. [Google Scholar] [CrossRef]
- Ishikawa, H.; Hashimoto, H.; Kiuchi, T. The evolving concept of “patient-centeredness” in patient–physician communication research. Soc. Sci. Med. 2013, 96, 147–153. [Google Scholar] [CrossRef]
- Gomez Sanchez, P.; Gaitan, H. Guías de práctica clínica en Colombia. Rev. Colomb. De Obstet. Y Ginecol. 2013, 64, 214–217. [Google Scholar] [CrossRef]
- McGlynn, E.A.; Asch, S.M.; Adams, J.; Keesey, J.; Hicks, J.; DeCristofaro, A.; Kerr, E.A. The Quality of Health Care Delivered to Adults in the United States. N. Engl. J. Med. 2003, 348, 2635–2645. [Google Scholar] [CrossRef]
- Levy, M.M.; Dellinger, R.P.; Townsend, S.R.; Linde-Zwirble, W.T.; Marshall, J.C.; Bion, J.; Schorr, C.; Artigas, A.; Ramsay, G.; Beale, R.; et al. The Surviving Sepsis Campaign: Results of an international guideline-based performance improvement program targeting severe sepsis. Intensive Care Med. 2010, 36, 222–231. [Google Scholar] [CrossRef]
- Aldugieman, T.; Alanezi, R.; Alshammari, W.M.G.; Al-Shamary, Y.W.Z.; Alqahtani, M.; Alreshidi, F. Knowledge, attitude and perception toward evidence-based medicine among medical students in Saudi Arabia: Analytic cross-sectional study. J. Fam. Med. Prim. Care 2018, 7, 1026. [Google Scholar] [CrossRef]
- Shafiei, K.; Sedaghati, F. Knowledge, attitude, and practices among Iranian neurologists toward evidence-based medicine. Iran J. Neurol. 2017, 16, 26–29. [Google Scholar]
- Djulbegovic, B.; Guyatt, G.H. Progress in evidence-based medicine: A quarter century on. Lancet 2017, 390, 415–423. [Google Scholar] [CrossRef]
- Rose, N. Políticas de Vida. Biomedicine, Poder y Subjetividad en el Siglo XXI; Editorial Universitaria: La Plata, Argentina, 2012. [Google Scholar]
- Palacio, A.C.A. Editorial. Iatreia. 2017. 29(4-S). Palacio-Acosta CA. Editorial. Iatreia [Internet]. 15 de mayo de 2017 [citado 3 de marzo de 2025]; 29(4-S2). Available online: https://revistas.udea.edu.co/index.php/iatreia/article/view/327830 (accessed on 1 March 2025).
- Timmermans, S. From Autonomy to Accountability: The role of clinical practice guidelines in professional power. Perspect. Biol. Med. 2005, 48, 490–501. [Google Scholar] [CrossRef]
- Berg, M. Problems and promises of the protocol. Soc. Sci. Med. 1997, 44, 1081–1088. [Google Scholar] [CrossRef]
- Petersen, A. Risk, government and the new public health. In Petersen y Robin Bunton. Foucault, Health and Medicine; Routledge: London, UK, 1997. [Google Scholar]
- Ardila-Sierra, A.; Abadía-Barrero, C. Medical labour under neoliberalism: An ethnographic study in Colombia. Int. J. Public Health 2020, 65, 1011–1017. [Google Scholar] [CrossRef]
- Rose, N.; Miller, P. Political power beyond the State: Problematics of government. Br. J. Sociol. 2010, 61 (Suppl. 1), 271–303. [Google Scholar] [CrossRef]
- Mendieta Gonzalez, D.; Jaramillo, C.E. El Sistema general de seguridad social en salud en Colombia. Universal, pero ineficiente: A propósito de los veinticinco años de su creación. Rev. Latinoam. Derecho Soc. 2019, 201–218. [Google Scholar] [CrossRef]
- García, C. El hospital como empresa: Nuevas práticas, nuevos trabajadores. Univ. Psychol. 2007, 6, 143–154. [Google Scholar]
- Armstrong, D. Professionalism, Indeterminacy and the EBM Project. BioSocieties 2007, 2, 73–84. [Google Scholar] [CrossRef]
- Timmermans, S.; Kolker, E.S. Evidence-based medicine and the reconfiguration of medical knowledge. J. Health Soc. Behav. 2004, 45, 177–193. [Google Scholar] [PubMed]
- Hershey, N. The defensive practice of medicine. Myth or reality. Milbank Mem. Fund Q. 1972, 50, 69–98. [Google Scholar] [CrossRef]
- Timmermans, S.; Mauck, A. The Promises and Pitfalls of Evidence-Based Medicine. Health Aff. 2005, 24, 18–28. [Google Scholar] [CrossRef]
- Elstein, A.S. On the origins and development of evidence-based medicine and medical decision making. Inflamm. Res. 2004, 53, S184–S189. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Légaré, F.; Simmons, M.B.; McNamara, K.; McCaffery, K.; Trevena, L.J.; Hudson, B.; Glasziou, P.P.; del Mar, C.B. Shared decision making: What do clinicians need to know and why should they bother? Med. J. Aust. 2014, 201, 35–39. [Google Scholar] [CrossRef]
- Forrow, L.; Wartman, S.A.; Brock, D.W. Science, ethics, and the making of clinical decisions. Implications for risk factor intervention. JAMA 1988, 259, 3161–3167. [Google Scholar] [CrossRef]
- Ministerio de Salud y Protección Social. Departamento Administrativo de Ciencia Tecnología e Innovación—Colciencias. Guía de Práctica Clínica Para la Prevención, Diagnóstico, Tratamiento y Rehabilitación de la Falla Cardíaca en Población Mayor de 18 años Clasificación B, C y D. Guía Completa. 2016. Guía No. 53. 2023. Available online: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/DE/CA/gpc-rehabilitacion-falla-cardiaca-poblacion-mayor-18-anos-b-c-d.pdf (accessed on 1 March 2025).
- Ministerio de Salud y Protección Social—Colciencias Guía de Práctica Clínica. Hipertensión Arterial Primaria (HTA)—2013 Guía No. 18. 2023. Available online: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/INEC/IETS/GPC_Completa_HTA.pdf (accessed on 1 March 2025).
- Foucault, M. El sujeto y el poder. Rev. Mex. Sociol. 1988, 50, 3–20. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).