Abstract
Children placed with kinship foster parents can experience less disruption and stronger family ties than children in non-kinship placements. However, financial hardship can restrict kinship caregivers from taking in relatives’ children. This study investigated (1) kinship caregivers’ financial standing compared to a national subsample of caregivers and (2) whether certain factors moderate the likelihood that a kinship caregiver will be able to provide care for additional non-relative children without additional financial assistance from the Department of Social Services (DSS). This study utilized primary data from 345 relatives across North Carolina and nationally representative secondary data on 6394 individuals’ financial circumstances. One-sample t-tests and chi-square goodness-of-fit tests revealed that caregivers who participated in our study generally fared better financially than caregivers at the national level. Model-based recursive partitioning results showed that if an additional child is placed in the home, the caregiver’s perceived capacity to provide care without extra DSS support decreased by approximately 19%, with a greater decrease (35%) among a subgroup of caregivers with low financial well-being status. The heterogeneity in caregivers’ experiences, capacities, and financial needs buttresses the need for nuanced interventions and programs targeting these caregivers, enabling them to provide more stable care for children placed in their homes.
1. Introduction
Kinship care is the preferred placement option when it is determined that moving a child from their family’s home is necessary due to child abuse and/or neglect. However, notwithstanding kinship care being the preferred choice by families and child welfare professionals, the prohibitive costs associated with caring for a child can be particularly challenging [1]. Programs such as the Kinship Guardianship Assistance Program (KinGAP) are designed partly to mitigate this financial burden and serve as a permanency option for children, but there are limitations to who qualifies for KinGAP to receive payments for caregiving. For example, the North Carolina Department of Health and Human Services (NCDHHS) names several eligibility requirements for KinGAP, including requirements around the age of the child in care (i.e., 14 years old), license status of the home, and the amount of time the child must be in the licensed home of a caregiver [2]. Because of the requirements of many existing programs, vast disparities remain in the financial assistance provided to kinship caregivers compared to non-relative foster parents. Indeed, decades of evidence highlight the significant number of unlicensed kinship caregivers who have lower incomes and limited access to resources and support, including financial assistance, potentially creating financial hardship as they engage in caregiving responsibilities [3,4,5,6,7].
The experience of financial hardship can significantly impact a child’s well-being, including their physical and mental health [8,9,10]. The impact of financial hardship on the caregiver has also been considered previously [11,12,13,14], but less is known about the impact that financial hardship has on a caregiver’s current caregiving choices or plans to provide support to additional non-relative children as a licensed foster parent. One situation where the decision to support an additional child can arise is when considering placement for the sibling of a relative who is already living with a kinship caregiver. The benefits related to placing siblings together, including prevention of an additional loss and an increased sense of connection and fulfillment for each child [15,16,17], are substantial enough that states must attempt to keep siblings together when out-of-home placement is deemed necessary [18]. However, the decision to take on multiple children has important financial implications, and it is crucial to understand the impact of these financial implications on caregiver capacities and intentions. Thus, this study addresses three questions: (a) How does the financial standing of kinship caregivers compare to individuals caring for another child in the general population in the United States? (b) What is the relationship between the number of children from DSS living with a kinship caregiver and the caregiver’s perceived financial capacity to care for the children? (c) What distinct subgroups can be identified based on how caregivers’ financial considerations inform their decisions to take care of relatives’ children? Findings from this study could highlight groups within kinship caregivers who could benefit from targeted financial support to help them continue serving or begin to serve as resources for some of our youngest, most vulnerable populations.
1.1. The State of Kinship Care
There are three types of kinship care: formal, in which the child lives with a relative, but the child is in the legal custody of the state; informal, in which a relative or fictive kin has taken on the role of guardian without legal involvement from the state; and diversion kinship care, in which a child protective agency assists in placing a child in a relative’s care [19]. Over the years, kinship placements have grown continuously as the preferred placement option for children [6,20,21]. Currently, over 2.5 million children in the United States are in some type of kinship foster arrangement [19]. From 2011 to 2021, the number of children in formal or informal kinship care placements rose from 27% to 35%, and there are an estimated 100,000–300,000 children in diversion kinship care [19].
Compared with other out-of-home placement options, kinship care is considered better for a child’s well-being for numerous reasons. Kinship placement allows children to maintain ties with family members and close friends, preserving relationships that may otherwise be lost in alternative placement types [22,23,24,25]. Placement with a relative or fictive kin also increases the potential for a child to remain connected to customs and traditions, which may foster a sense of belonging [24,26,27]. Furthermore, children in kinship placements experience more placement stability and are less likely to have placement disruptions compared to children in placements with non-relatives [24,28,29,30,31].
One of the primary ways kinship caregivers receive financial assistance to provide care for children of relatives is through foster care payments [32]. However, many kinship caregivers cannot benefit from this type of assistance due to foster care licensing requirements [33,34]. Even when these caregivers can receive foster care payments, there is evidence that the payment amounts in all but four states in the U.S. are insufficient when considering the financial demands associated with meeting the needs of children in their care [35]. The potential for financial hardship ultimately falls on the kinship caregiver, who is responsible for making up for the difference. This study examines whether statistically identifiable heterogeneity exists in how finances drive kinship caregivers’ decisions to support other relative’s children. Such insights could inform the appropriate contextualization and targeting of interventions.
1.2. Financial Hardship and Adverse Outcomes
Financial hardship, which often manifests as a lack of financial resources to cover the costs of essential items (e.g., housing, food, and transportation), constitutes a major stressor for many individuals and households [36,37]. The family stress model (FSM), which has been considered previously when exploring the relationship between kinship caregivers, finances, and family outcomes [38,39], posits that financial hardship can have a negative impact on family relationships, thereby increasing the risk of family instability [9,40].
Studies have reported several adverse effects of financial hardship on different members of the family system. Among adults, financial hardship has been found to contribute to caregiver depression [11,12], increased psychological distress [41], relational conflicts [14], decreased self-efficacy [13], increased aggression [42], and reduced positive parenting techniques [12,14]. The heightened stress experienced by caregivers facing financial hardship can affect their behaviors, parenting satisfaction, and, ultimately, their ability to engage in sensitive parenting [13,43,44]. Preoccupation with addressing pressing family economic needs affects a caregiver’s ability to fully invest in the long-term social, health, and educational needs of a child in their care [45].
Children in general (i.e., even children who are not in kinship placements) also bear the weight of financial hardship. The experience of financial hardship among children has been associated with decreased levels of hope [37], increased loneliness [41], challenges in literacy achievement and academic participation [43,46,47,48], food insecurity [44], internalizing behaviors, such as withdrawal and anxiety [42,49], and externalizing behaviors, such as aggression and defiance [11,14]. The adverse effects of financial stressors on a child’s health, education, and well-being are partly the result of stress experienced by caregivers in situations such as work instability and loss of income [40,50].
Previous studies have examined the financial hardship experienced by kinship caregivers in comparison to non-relatives, noting that kinship caregivers often fare worse financially than non-relatives [39,51,52,53,54,55]. Evidence suggests that there may be differences in the potential to experience financial hardship based on factors such as age [23,56,57,58]. In fact, kinship caregivers, especially grandparents serving as kinship resources, have a greater likelihood of dealing with other life circumstances (e.g., medical challenges, unemployment, fixed income) as they get older, which can affect their financial well-being more than caregivers in other age groups [23,56,57,58]. Thus, this study sought to build on existing evidence, investigating the possible thresholds at which caregivers’ ages interact with their financial circumstances to influence their caregiving decisions. This nuanced intersectionality has yet to be extensively addressed in the literature.
Despite the financial hardship some kinship caregivers face, many continue to step up and provide caregiving support for children in need, highlighting their altruism. The concept of altruism and its impact on behavior and decision making are rooted in evolutionary theory. Ultimately, individuals are often inclined to engage in prosocial behaviors, including providing care for others, even if this comes at a personal cost to the individual [59,60,61]. Evidence suggests that individuals are more likely to act altruistically for those who are related to them [62,63]. However, there are limits to the cost that even the most altruistic caregivers are willing to pay, and as the cost to the caregiver increases, altruistic behavior can decline [62]. Testa [63] also emphasizes this point, stating that unless some form of extrinsic motivation is incorporated, especially in the case of kinship care, there are lengths to which intrinsic motivation will continue to influence an individual’s behavior. These findings suggest the need to explore ways to extend the financial support to caregivers beyond what is currently offered.
Given the impact of financial hardship on caregiver distress, parenting, and outcomes for children, it is necessary to understand at which point the experience of financial hardship impacts caregiver capacities and intentions for various subgroups in order to design appropriately tailored assistance to improve the financial stability of kinship foster parents. Addressing financial pressures among kinship families has the potential to increase their caregiving capacity, potentially impacting their decision to support more children of relatives in their homes.
2. Methods
2.1. Data Source
This study used data from the National Financial Well-Being Survey (NFWBS) and the Harvey Kinship Project. The NFWBS is a nationally representative cross-sectional survey administered by the Consumer Financial Protection Bureau (CFPB) [64] to individuals aged 18 years and older across all 50 states (N = 6394). The Harvey Kinship Project is an evaluation study conducted in North Carolina from 2018 to 2023 to evaluate a kin-specific foster care training program to help eligible kinship caregivers qualify to receive financial support under KinGAP. Standard foster care licensure training and processes were adapted for kinship caregivers to increase the number of licensed kinship caregivers serving as foster parents in the state. The kinship training and support services, such as assistance with transportation and child care, were provided to caregivers online due to the COVID-19 health crisis. This study uses the pretest survey from the participants who enrolled in the online program from 2020 to 2023 (N = 345). This pretest survey prompted participants to respond to questions related to their experience in training to become licensed as a foster parent, knowledge about permanency options, and financial well-being and behavior.
2.2. Measures
2.2.1. Outcome Variable
The outcome variable was the perceived financial ability to support a relative child. Caregivers were asked to respond to the statement, “I cannot afford to care for the child without getting help from social services”, using a 5-point Likert-type scale with responses ranging from completely (coded 1) to not at all (coded 5). The responses were collapsed into a binary response scale where those who indicated completely (1) to very little (4) were collapsed into 0 (No), and those who selected not at all were coded 1 (Yes). The variable was renamed perceived ability to support a child to ensure an intuitive interpretation of the new response scale.
2.2.2. Predictor
For a subset of research questions about the predictive influence of the number of children in care, the main predictor is the number of children, measured as the number of children currently placed in a participant’s home by the Department of Social Services (DSS).
2.2.3. Hypothesized Moderators
This study assessed nine potential moderators: Financial well-being is a widely used scale developed by the CFPB [64] to measure an individual’s financial situation and financial capability. Items on the scale cover four major areas of financial well-being: (1) sense of control over one’s resources, (2) ability to handle unpredictable financial changes, (3) being on track to meet one’s financial objectives, and (4) economic freedom to enjoy one’s life [64]. To validate the CFPB financial well-being scale, comparisons were made to other measures of financial well-being (e.g., credit rating, presence of savings for three months of expenses, material hardship, etc.). A comparison of these measures and the CFPB’s financial well-being scale showed statistically significant relationships in both magnitude and direction [64]. Additionally, scores on the CFPB financial well-being scale show high correlation with widely used socio-economic status indicators, such as income and education level [64], further confirming the validity of the scale. For the current study, four items were averaged to obtain the overall financial well-being score (Cronbach’s α = 0.97), with low scores indicating low financial well-being and high scores indicating higher financial well-being. Age was a continuous variable measured in years. Sex was measured as male (coded 1) and non-male (coded 0). The highest level of education was originally measured by asking the caregivers to indicate their highest education level. The responses were collapsed into “high school and below” (coded as 1) and post-high school (coded as 0). Median household income was originally measured in five income groups: $20,000 or less, $20,001–$40,000, $40,001–$60,000, $60,001–$80,000, $80,001–$100,000, and $100,001 or more. The North Carolina (NC) median household income threshold ($62,891 as of 2021) was used as a benchmark to collapse the income groups into “less than NC median household income” for $60,000 and below (coded as 0) and above $60,000 (coded as 1). Grandparent was used to characterize the relationship between a caregiver and a child, where “grandmother or grandfather” was coded 1, and all others were coded 0. The caregiver’s marital status, originally measured as a six-level variable, was collapsed into married, coded 1, and not married, coded 0. Employment status was measured by asking the caregivers to indicate their current work situation. Responses for “employed” were coded 0, while responses for “unemployed” were coded as 1. Finally, the presence of biological children currently living at home with caregivers was measured as a categorical variable, with “yes” coded 1 and “no” coded 0.
2.3. Data Analysis
2.3.1. Comparisons to Population
Using Stata 18, two types of threshold analyses were performed to investigate the financial standing of kinship caregivers (i.e., financial well-being score and income groups) compared to the general population and a subset of caregivers in the United States (i.e., Question 1). First, a one-sample t-test was performed to determine whether the mean financial well-being score of the kinship caregiver sample was comparable to the NFWBS national sample’s mean of 2.83 at the 0.05 significance level. A sensitivity analysis was performed using the mean financial well-being scores for a subsample of the NFWBS datasets, namely 214 individuals from across all nine census divisions caring for another child in their household. This subsample was chosen to ensure comparative samples of caregivers in both the Harvey project data and the national data. Second, a chi-square goodness-of-fit test was used to assess whether the observed distribution of income and employment groupings in the kinship caregiver sample aligns with the expected distribution based on the national income grouping from the NFWBS data. The analyses were repeated using the subset of 214 individuals from the national dataset caring for another child in their household.
2.3.2. Model-Based Recursive Partitioning
To address Questions 2 and 3, this study utilized model-based recursive partitioning (MOB), a machine learning algorithm, and the “partykit” package for R version 4.3.1 to identify subgroups of caregivers based on the relationship between the number of DSS children that caregivers already had and their perceived ability to support them without additional DSS financial assistance. Other child welfare outcome studies have employed this tree-based machine learning method to identify smaller subgroups [65,66].
The MOB analysis assessed whether nine caregiver characteristics served as moderators, allowing us to identify subgroups that exhibited varying relationships between the number of DSS children in one’s care and their financial capacity to support them. The MOB algorithm fits a logistic regression model to the caregiver data, given the binary outcome variable (i.e., ability to support financially or not). Our data-driven analytic approach was tested for parameter stability across nine partitioning variables (i.e., hypothesized moderators). If the algorithm found substantial between-group differences (i.e., parameter instability based on a 0.05 significance level), it repeatedly split the sample based on the variable that had the highest instability (i.e., lowest p-value), thus enabling subgroups to emerge, if any [65]. A minimum sample size of 10 per subgroup was specified to ensure a reasonable number of respondents per group and allow for meaningful between-group comparisons. The Bonferroni corrected p-value was used to limit the family-wise error rate (FWER) and minimize Type I error probability (i.e., false positive error).
3. Results
3.1. Descriptive Results
Table 1 shows the demographic characteristics of the sample (N = 345). More than half of caregivers (58%, n = 159) reported that they were unable to support children in their care financially, and the average number of children placed in participants’ homes by DSS was 1.28 (SD = 0.98). The mean financial well-being score reported among the caregivers was 3.43 (SD = 0.58). The reported mean age of caregivers was 44.26 (SD = 12.43, median = 43), while the mean age for grandparent caregivers only was 57.41 (SD = 9.01, median = 57). The sample comprised 82 (29%) males and 205 (71%) non-males. Of the respondents, 124 (43%) had a high school education or lower, while 163 (57%) had a post-high school education. The majority of the respondents reported annual household income less than the North Carolina state median (60%). A total of 94 (33%) respondents were Black/African American, 169 (60%) were White, and 21 (7%) identified as another race. Fifty-one (18%) respondents with a child in their home identified as a grandparent. Regarding the marital status of the respondents, 192 (66.21%) reported that they were married, while 98 (34%) were not. Most respondents reported being employed (84%), while 48 (16%) were unemployed. Of the respondents, 139 (51%) reported having a biological child living in their home. Lastly, 235 (81%) respondents indicated that they had at least one child in their home who had been placed with them by DSS.

Table 1.
Descriptive characteristics of caregivers in the study sample (N = 345).
3.2. Comparisons to Population
The results of the one-sample t-test indicated that the 3.43 financial well-being mean score for the kinship caregiver sample was higher than the United States mean score of 2.83 (t = 17.07, p < 0.001) as well as the 2.95 average score for the national subsample of individuals who are caring for another child (t = 13.44, p < 0.001). These results suggest that the kinship caregiver sample had better self-reported financial well-being than the general public. Results of the chi-square goodness-of-fit tests indicated statistically significant differences in the middle to higher income group between the kinship caregiver sample and the national [x2 (3) = 50.03, p < 0.001]. A comparison of employment status between the kinship caregiver sample and a subsample (N = 214) from the national dataset revealed more equivalent employment patterns based on full-time employment, part-time employment, and retirement. The only significant employment differences pertained to the distribution of unemployment (x2 = 3.73, p < 0.001), self-employment (x2 = 4.10, p < 0.001), and student status (x2 = 8.78, p < 0.05). Overall, these findings suggest that the observed financial well-being, income, and employment distribution of the kinship caregiver sample is statistically different from the broader United States population.
3.3. Subgroup Identification
The MOB model assessing the moderated relationship between the perceived financial ability to support a child and the number of children currently placed in the caregiver’s home produced a decision tree which is shown in Figure 1. The parameters for each decision node of the decision tree are provided in Table 2. All participants in this study were included in Node 1. The participants were then partitioned into two subgroups based on their average scores on the financial well-being measure. The parameter stability test indicated that the parameters of the model were significantly different between caregivers with low (score ≤ 3.33) and high financial well-being (score > 3.33, p < 0.001).
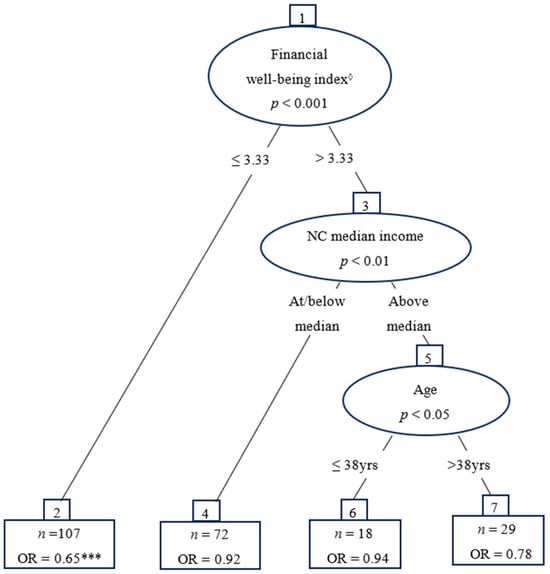
Figure 1.
Odds ratio differences in perceived financial ability to support childcare between subgroups of financial well-being, income level, and age. Note: *** p < 0.001; ◊ Range 1–5.
Table 2.
Logistic regression of caregivers’ perceived ability to financially support a child and the number of children placed in their homes by DSS.
Node 2 is a terminal node for kinship caregivers whose average financial well-being score is 3.33 or lower. The odds ratio for this subgroup (OR = 0.65, p < 0.001) suggests that among kinship caregivers with low financial well-being status, as the number of children in the caregiver’s home increases by 1, the perceived ability to support a child without additional financial assistance from DSS goes down by 35%. The subgroup of caregivers with higher financial well-being scores (Node 3) was further partitioned based on the caregiver’s income in relation to the median household income for North Carolina. This additional partition revealed a second subgroup (Node 4) that represented kinship caregivers who had a high average financial well-being score (i.e., >3.33) but earned less than the North Carolina median household income (i.e., <$60,000). For this subgroup, the odds ratio (OR = 0.92) suggests that these caregivers’ ability to support children without additional financial support decreases by 8% as the number of children in the caregiver’s home increases by 1.
The subgroup of kinship caregivers with an average financial well-being above 3.33 and an income above North Carolina’s median household income (Node 5) is further partitioned based on the age of the kinship caregiver. Node 6 represents kinship caregivers who are 38 years old or younger, with an above-average financial well-being score (>3.33) and an income above North Carolina’s median household income. The odds ratio for this subgroup (OR = 0.94) suggests that a caregiver has 6% lower odds of indicating that they could support another child without additional financial assistance as the number of children in the caregiver’s home increases by 1.
Finally, Node 7 represents kinship caregivers older than 38 years with an above-average financial well-being score (>3.33) and an income above North Carolina’s median household income. Based on the odds ratio for this subgroup (OR = 0.78), a kinship caregiver has 22% lower odds of indicating that they could support another child placed by DSS without additional financial assistance as the number of children in the caregiver’s home increases by 1. Nodes 6 and 7 are terminal nodes.
In summary, the decision tree visualized three moderators (i.e., financial well-being average score, NC median household income, and caregiver age) that produced four subgroups of participants with varying abilities to serve as kinship caregivers for a child. The subgroups are as follows: (1) kinship caregivers with below-average financial well-being status; (2) kinship caregivers with an above-average financial well-being status and living on a household income below the median for North Carolina; (3) kinship caregivers aged 38 years or younger with an above-average financial well-being status and living above the North Carolina median household income; and (4) kinship caregivers older than 38 with above-average financial well-being status and living on household income above the median for North Carolina.
4. Discussion
This study aimed to contrast the financial status of kinship caregivers with the general population and determine whether certain financial and personal factors moderate the odds of a kinship caregiver’s perceived ability to support the child in their care without additional financial assistance from DSS. One-sample t-tests and chi-square goodness-of-fit tests revealed that the caregivers who participated in our study generally fared better financially than their counterparts at the national level as well as in the South Atlantic Division and Southern Region. The MOB results also revealed an inverse relationship between the number of children placed by DSS and the perceived ability of a caregiver to provide care for a child in their care without financial support. The model results suggest that financial well-being status is the primary moderator of caregivers’ perceived ability to support children, with caregivers who report a below-average financial well-being status having a greater need for DSS financial support for additional children in their care.
Several subgroups emerged from the MOB analysis, although the odds ratios for these subgroups were not significant at a 0.05 significance level. However, the interactive role of age is intriguing, given the emergence of 38 years as a possible splitting point. (i.e., caregivers older than 38 years and those who were 38 years and younger). Caregivers older than 38 years, despite having a high average financial well-being score and a household income over the median in NC, still appear to have lower odds of reporting the ability to support a child as the number of children placed in their homes by DSS increases. Caregivers who were 38 years old or younger with high financial well-being scores and a median household income greater than the NC average also had lower odds of reporting an ability to provide financial support for a child as the number of children placed in their home increased, though they had higher odds of reporting the ability to do so when compared to their counterparts above the age of 38. The age split point at 38 years observed in these data suggests that families with caregivers approaching middle adulthood may have particular financial demands that limit their capacity to provide kinship care without additional support, suggesting an area for further research.
Because there is ample literature on the role of grandparents as kinship caregivers and how financial support is needed for this subgroup [23,56,57], we anticipated that an age split point would be higher. In general, there was a low percentage of caregivers identifying as grandparents represented in this study (i.e., 18%). One potential reason for the lower age of caregivers in our study may be due to the online administration of the program and the survey. While this online modification was adopted due to the restrictions caused by COVID-19, the format may have impacted the involvement of caregivers of different ages.
The study results reinforce that helping kinship caregivers access financial resources remains central to children’s outcomes. The average family is estimated to spend approximately $12,980 per year raising a child [67], which is approximately 22% of the NC median household income. The daily costs associated with raising a child may make it difficult for caregivers to support more children even if they desire to do so. While the chi-square goodness-of-fit tests revealed that caregivers in our study reported higher average financial well-being scores than caregivers in other regions of the nation, there were still downward trends in their perceived ability to support a child placed by DSS without financial assistance. This finding suggests that despite the seemingly high financial well-being of some, concerns remain about the costs associated with child-rearing. This finding is additional evidence of the hardship that child-rearing has on caregivers who are effectively low-income, suggesting that they will also have concerns related to the ability to support more than one child without assistance.
At the time of this study, most caregivers had a child placed in their home by DSS (81%), but 60% of the sample reported an income below the NC median household income. It is clear that kinship caregivers genuinely want to serve in their role. However, their willingness and altruism alone are not enough. If a child needing an out-of-home placement cannot go to a kinship caregiver, that child misses the opportunity to maintain familial connections and may not achieve optimal development. Therefore, increasing the financial assistance available to kinship caregivers is in the child’s and their siblings’ best interest.
While this study contributes to our understanding of differences in caregiver capacity to support children from DSS, it has some limitations. The first relates to the generalizability of the results. This study used data from caregivers living in more than 90 counties in North Carolina. However, these data may be different from populations in other states. Additionally, the study design limits the ability to infer causality between the number of children placed in the home and the ability to financially support the children. Another limitation lies in the information not available in this study regarding potential income sources for kinship caregivers who report being unemployed, such as social security or disability. We also did not have information on whether families received financial support from Temporary Assistance to Needy Families (TANF). This information could provide a deeper understanding of the families’ financial circumstances in our sample and account for some of this study’s findings. Finally, this study utilizes the financial well-being score of caregivers based on a self-report measure. While the CFPB financial well-being measure is comprehensive and validated [64], self-report measures can be affected by social desirability or recall bias [68].
Despite these limitations, this study utilized unique data to provide information regarding the distinct experiences of this group of kinship caregivers who support children who are unable to remain in the care of their family of origin. Another strength of this study lies in the use of nationally representative data from the NFWBS to draw comparisons between the financial status of caregivers in our study and the general population. Furthermore, the use of machine learning methods like MOB allowed us to draw out relationships reflecting the experiences of these caregivers. The MOB results highlight the intersectionality of unique age thresholds in ways not previously examined.
The results of this study have several policy implications. There are still barriers that kinship caregivers face that can contribute to the disparities between payments they receive in comparison to foster parents. As noted earlier, current restrictions under KinGAP limit the financial resources that kinship caregivers can access when acting in service of the children of family members. The Harvey Kinship Project is an example of an intervention that seeks to support financial equity by increasing the number of licensed kinship caregivers, enabling them to receive payments as they provide support for the children who need it. Increasing access to financial assistance, whether through reevaluation of KinGAP requirements or expansion of interventions such as the Harvey Kinship Project, is necessary to address the disparities between kinship caregivers and foster parents who receive foster care payments. Additionally, this study highlights the importance of continued exploration of the diverse needs of kinship groups to specify other types of support that would benefit these caregivers.
5. Conclusions
This study explored the financial and personal factors that may moderate the odds of a kinship resource providing care for children without additional financial assistance from DSS. While this study’s findings are not surprising, the use of a machine learning technique assists in identifying certain caregivers who may need more support than previously realized. The benefits of keeping children with relatives are clear, but this may be more challenging in certain instances, such as when families have multiple children who need an out-of-home placement (e.g., sibling groups). It is ideal for keeping these children together, but the findings from this study suggest that this could present financial hardship for some kinship caregivers who report lower financial well-being. The intersectionality of caregiver characteristics, such as age and socio-economic status, must be considered to truly understand the most crucial support for this population. Kinship caregivers are not monolithic. There is heterogeneity in their experiences, capacities, and, ultimately, their financial needs. Thus, interventions and policies targeting these caregivers must be sufficiently nuanced to account for their unique experiences. Reliance on caregiver altruism alone is insufficient. The well-being of children requiring out-of-home placement is paramount, and caregivers continue to show a desire to support such children. However, the costs associated with raising children are substantial. Therefore, caregivers’ willingness to provide care to relatives must be met with financial means to do so.
Author Contributions
Conceptualization, D.A. and I.C.J.; methodology, D.A., I.C.J. and S.H.A.; software, D.A. and S.H.A.; validation, D.A. and K.C.B.; formal analysis, D.A. and S.H.A.; investigation, D.A. and K.C.B.; data curation, D.A., K.C.B. and I.C.J.; writing—original draft preparation, I.C.J., S.H.A. and D.A.; writing—review and editing, I.C.J., D.A. and K.C.B.; visualization, D.A. and S.H.A.; supervision, D.A. and K.C.B.; project administration, I.C.J.; funding acquisition, D.A. and K.C.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the University of North Carolina at Chapel Hill’s C. Felix Harvey Award to Advance Institutional Priorities.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the University of North Carolina at Chapel Hill (protocol code 18-1043, 8 May 2018).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The Harvey project data presented in this study are available upon request from the corresponding author. The CFPB data are publicly available at https://www.consumerfinance.gov/data-research/financial-well-being-survey-data/, accessed on 20 February 2024.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Cox, C.B. Grandparent-headed families: Needs and implications for social work interventions and advocacy. Fam. Soc. 2007, 88, 561–566. [Google Scholar] [CrossRef]
- North Carolina Department of Health and Human Services. Foster Care and Beyond: Kinship Foster Care and Guardianship Assistance. 2018. Available online: https://www.ncdhhs.gov/cws2122a4/download?attachment (accessed on 2 October 2023).
- Bass, S.; Shields, M.K.; Behrman, R.E. Children, families, and foster care: Analysis and recommendations. Futur. Child. 2004, 14, 5–29. [Google Scholar] [CrossRef]
- Berrick, J.D.; Barth, R.P.; Needell, B. A comparison of kinship foster homes and foster family homes: Implications for kinship foster care as family preservation. Child. Youth Serv. Rev. 1994, 16, 33–63. [Google Scholar] [CrossRef]
- Fruhauf, C.A.; Pevney, B.; Bundy-Fazioli, K. The needs and use of programs by service providers working with grandparents raising grandchildren. J. Appl. Gerontol. 2015, 34, 138–157. [Google Scholar] [CrossRef] [PubMed]
- Stene, K.L.; Dow-Fleisner, S.J.; Ermacora, D.; Agathen, J.; Falconnier, L.; Stager, M.; Wells, S.J. Measuring the quality of care in kinship foster care placements. Child. Youth Serv. Rev. 2020, 116, 105136. [Google Scholar] [CrossRef]
- Xu, Y.; Bright, C.L.; Ahn, H.; Huang, H.; Shaw, T. A new kinship typology and factors associated with receiving financial assistance in kinship care. Child. Youth Serv. Rev. 2020, 110, 104822. [Google Scholar] [CrossRef]
- Ashiabi, G.S.; O’Neal, K.K. Children’s health status: Examining the associations among income poverty, material hardship, and parental factors. PLoS ONE 2007, 2, e940. [Google Scholar] [CrossRef]
- Masarik, A.S.; Conger, R.D. Stress and child development: A review of the Family Stress Model. Curr. Opin. Psychol. 2017, 13, 85–90. [Google Scholar] [CrossRef]
- Zilanawala, A.; Pilkauskas, N.V. Low-Income Mothers’ Material Hardship and Children’s Socioemotional Well-Being. Fragile Families Working Paper WP11-02-FF. Princeton University, School of Public and International Affairs, Center for Research on Child Wellbeing. 2011. Available online: https://ffcws.princeton.edu/sites/g/files/toruqf4356/files/wp11-02-ff.pdf (accessed on 26 September 2023).
- Saasa, S.; Ward, K.P.; Sandberg, S.; Jacobson, J. Financial hardship, neighborhood cohesion and child externalizing behaviors: An extension of the family stress model among immigrant mothers. Child. Youth Serv. Rev. 2021, 128, 106153. [Google Scholar] [CrossRef]
- Shelleby, E.C. Economic stress in fragile families: Pathways to parent and child maladjustment. J. Child Fam. Stud. 2018, 27, 3877–3886. [Google Scholar] [CrossRef]
- Gómez, A.; Karimli, L.; Holguin, M.; Chung, P.; Szilagyi, P.; Schickedanz, A. Bills, babies, and (language) barriers: Associations among economic strain, parenting, and primary language during the newborn period. Fam. Relat. 2022, 71, 352–370. [Google Scholar] [CrossRef] [PubMed]
- Neppl, T.K.; Senia, J.M.; Donnellan, M.B. Effects of economic hardship: Testing the family stress model over time. J. Fam. Psychol. 2016, 30, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Affronti, M.; Rittner, B.; Semanchin Jones, A.M. Functional adaptation to foster care: Foster care alumni speak out. J. Public Child Welf. 2015, 9, 1–21. [Google Scholar] [CrossRef]
- Sting, S. Sibling relations in alternative child care results of a study on sibling relations in sos children’s villages in Austria. Kriminol. I Soc. Integr. 2013, 21, 119–128. [Google Scholar]
- Wojciak, A.S. ‘It’s complicated.’ exploring the meaning of sibling relationships of youth in foster care. Child Fam. Soc. Work 2017, 22, 1283–1291. [Google Scholar] [CrossRef]
- Fostering Connections to Success and Increasing Adoptions Act, Public Law 110-351, 110th Congress, 122 STAT. 3949. 2008. Available online: https://www.govinfo.gov/content/pkg/PLAW-110publ351/pdf/PLAW-110publ351.pdf (accessed on 2 October 2023).
- Annie, E.; Casey Foundation. What Is Kinship Care? 2023. Available online: https://www.aecf.org/blog/what-is-kinship-care (accessed on 25 September 2023).
- Bramlett, M.D.; Radel, L.F.; Chow, K. Health and well-being of children in kinship care: Findings from the national survey of children in nonparental care. Child Welf. 2017, 95, 41–60. [Google Scholar] [CrossRef]
- Brisebois, K.; Lee, S. Foster and kinship care: An examination of the legislation that aims to improve permanency and continuity of care in Ontario. Can. J. Humanit. Soc. Sci. 2012, 3, 101–114. [Google Scholar]
- Bunch, S.G.; Eastman, B.J.; Griffin, L.W. Examining the perceptions of grandparents who parent in formal and informal kinship care. J. Hum. Behav. Soc. Environ. 2007, 15, 93–105. [Google Scholar] [CrossRef]
- Connolly, M.; Kiraly, M.; McCrae, L.; Mitchell, G. A kinship care practice framework: Using a life course approach. Br. J. Soc. Work 2017, 47, 87–105. [Google Scholar] [CrossRef]
- Pitcher, D. Inside Kinship Care: Understanding Family Dynamics and Providing Effective Support; Jessica Kingsley Publishers: London, UK, 2014. [Google Scholar]
- Wu, Q.; Zhu, Y.; Ogbonnaya, I.; Zhang, S.; Wu, S. Parenting intervention outcomes for kinship caregivers and child: A systematic review. Child Abus. Negl. 2020, 106, 104524. [Google Scholar] [CrossRef]
- Crumbley, J.; Little, R.L. Relatives Raising Children: An Overview of Kinship Care; Child Welfare League of America: Washington, DC, USA, 1997. [Google Scholar]
- Llosada-Gistau, J.; Casas, F.; Montserrat, C. The subjective well-being of children in kinship care. Psicothema 2019, 31, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Koh, E. Permanency outcomes of children in kinship and non-kinship foster care: Testing the external validity of kinship effects. Child. Youth Serv. Rev. 2010, 32, 389–398. [Google Scholar] [CrossRef]
- Koh, E.; Testa, M.F. Children discharged from kin and non-kin foster homes: Do the risks of foster care re-entry differ? Child. Youth Serv. Rev. 2011, 33, 1497–1505. [Google Scholar] [CrossRef]
- Perry, G.; Daly, M.; Kotler, J. Placement stability in kinship and non-kin foster care: A canadian study. Child. Youth Serv. Rev. 2012, 34, 460–465. [Google Scholar] [CrossRef]
- Rubin, D.M.; Downes, K.J.; O’Reilly, A.L.; Mekonnen, R.; Luan, X.; Localio, R. Impact of kinship care on behavioral well-being for children in out-of-home care. Arch. Pediatr. Adolesc. Med. 2008, 162, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Hernández, J.; Berrick, J.D. Kinship Probate Guardianship: An Important Permanency Option for Children. Fam. Soc. J. Contemp. Soc. Serv. 2019, 100, 34–51. [Google Scholar] [CrossRef]
- Ansong, D.; Brevard, K.; Gibbs, D.; Childs, S.; Francis, A.M. Harvey Kinship Project Report: Helping Abused and Neglected Children Find Permanent Homes with Their Grandparents and Other Relatives; The Group on Evidence Building in Child Welfare, UNC-Chapel Hill School of Social Work: Chapel Hill, NC, USA, 2020. [Google Scholar]
- Gibbs, D.; Ansong, D.; Brevard, K.; Francis, A.M.; Childs, S. Improving parenting competency and permanency awareness for kinship foster parents through in-service licensure training. Child Adolesc. Soc. Work J. 2022, 39, 595–606. [Google Scholar] [CrossRef] [PubMed]
- Ahn, H.; DePanfilis, D.; Frick, K.; Barth, R.P. Estimating minimum adequate foster care costs for children in the United States. Child. Youth Serv. Rev. 2018, 84, 55–67. [Google Scholar] [CrossRef]
- Mirowsky, J.; Ross, C.E. Age and the effect of economic hardship on depression. J. Health Soc. Behav. 2001, 42, 132–150. [Google Scholar] [CrossRef]
- Wen, D.; Goh, E.C.L.; Hsu, C. Hope in Low-Income Families—A study of family hardiness in Singapore. Fam. Relat. 2022, 71, 513–525. [Google Scholar] [CrossRef]
- Xu, Y.; Bright, C.L.; Barth, R.P.; Ahn, H. Poverty and economic pressure, financial assistance, and Children’s behavioral health in kinship care. Child Maltreatment 2021, 26, 28–39. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Zhao, Q.; Schuler, B.R.; Levkoff, S.E. Material hardship among custodial grandparents in COVID-19 and its associations with Grandchildren’s physical and mental health: A latent class analysis. Child. Youth Serv. Rev. 2022, 132, 106340. [Google Scholar] [CrossRef]
- Conger, R.D.; Conger, K.J.; Martin, M.J. Socioeconomic status, family processes, and individual development. J. Marriage Fam. 2010, 72, 685–704. [Google Scholar] [CrossRef] [PubMed]
- Low, N.; Mounts, N.S. Economic stress, parenting, and adolescents’ adjustment during the COVID-19 pandemic. Fam. Relat. 2022, 71, 90–107. [Google Scholar] [CrossRef]
- Liu, Y.; Merritt, D.H. Familial financial stress and child internalizing behaviors: The roles of caregivers’ maltreating behaviors and social services. Child Abus. Negl. 2018, 86, 324–335. [Google Scholar] [CrossRef]
- Iruka, I.U.; LaForett, D.R.; Odom, E.C. Examining the validity of the family investment and stress models and relationship to children’s school readiness across five cultural groups. J. Fam. Psychol. 2012, 26, 359–370. [Google Scholar] [CrossRef]
- McCurdy, K.; Gorman, K.S.; Metallinos-Katsaras, E. From poverty to food insecurity and child overweight: A family stress approach. Child Dev. Perspect. 2010, 4, 144–151. [Google Scholar] [CrossRef]
- Bradley, R.H.; Corwyn, R.F. Socioeconomic status and child development. Annu. Rev. Psychol. 2002, 53, 371–399. [Google Scholar] [CrossRef]
- Ansong, D.; Koomson, I.; Okumu, M.; Alhassan, M.; Makubuya, T.; Abreh, M.K. Private supplementary tutoring expenditures and children’s learning outcomes: Gender and locational evidence from Ghana. Stud. Educ. Eval. 2023, 76, 101232. [Google Scholar] [CrossRef]
- Ansong, D.; Okumu, M.; Nyoni, T.; Appiah-Kubi, J.; Amoako, E.O.; Koomson, I.; Conklin, J. The effectiveness of financial capability and asset building interventions in improving youth’s educational well-being: A systematic review. Adolesc. Res. Rev. 2023, 1–16. [Google Scholar] [CrossRef]
- Ansong, D.; Chowa, G.; Masa, R.; Despard, M.; Sherraden, M.; Wu, S.; Osei-Akoto, I. Effects of youth savings accounts on school attendance and academic performance: Evidence from a youth savings experiment. J. Fam. Econ. Issues 2019, 40, 269–281. [Google Scholar] [CrossRef]
- Rapee, R.M.; Schniering, C.A.; Hudson, J.L. Anxiety disorders during childhood and adolescence: Origins and treatment. Annu. Rev. Clin. Psychol. 2009, 5, 311–341. [Google Scholar] [CrossRef] [PubMed]
- Conger, R.D.; Conger, K.J. Resilience in midwestern families: Selected findings from the first decade of a prospective, longitudinal study. J. Marriage Fam. 2002, 64, 361. [Google Scholar] [CrossRef]
- Berrick, J.D.; Boyd, R. Financial well-being in family-based foster care: Exploring variation in income supports for kin and non-kin caregivers in California. Child. Youth Serv. Rev. 2016, 69, 166–173. [Google Scholar] [CrossRef][Green Version]
- Breman, R. Peeling Back the Layers: Kinship Care in Victoria ‘Complexity in Kinship Care’—Research Report, Melbourne, Baptcare Research Unit in Partnership with OzChild and Anchor. 2014. Available online: https://core.ac.uk/download/pdf/30673587.pdf (accessed on 19 September 2023).
- Ehrle, J.; Geen, R. Kin and Non-Kin Foster Care—Findings from a National Survey. Child. Youth Serv. Rev. 2002, 24, 15–35. [Google Scholar] [CrossRef]
- Musil, C.M.; Standing, T. Grandmothers’ diaries: A glimpse at daily lives. Int. J. Aging Hum. Dev. 2005, 60, 317–329. [Google Scholar] [CrossRef] [PubMed]
- Nandy, S.; Selwyn, J. Kinship care and poverty: Using census data to examine the extent and nature of kinship care in the UK. Br. J. Soc. Work 2012, 43, 1649–1666. [Google Scholar] [CrossRef]
- Dunifon, R.E.; Ziol-Guest, K.M.; Kopko, K. Grandparent Coresidence and Family Well-Being. Ann. Am. Acad. Pol. Soc. Sci. 2014, 654, 110–126. [Google Scholar] [CrossRef]
- Pilkauskas, N.V.; Dunifon, R.E. Understanding grandfamilies: Characteristics of grandparents, nonresident parents, and children: Understanding grandfamilies. J. Marriage Fam. 2016, 78, 623–633. [Google Scholar] [CrossRef]
- Purcal, C.; Brennan, D.; Cass, B.; Jenkins, B. Grandparents raising grandchildren: Impacts of lifecourse stage on the experiences and costs of care. Aust. J. Soc. Issues 2014, 49, 467–487. [Google Scholar] [CrossRef]
- Bourke, A.F.G. Hamilton’s rule and the causes of social evolution. Philos. Trans. R. Soc. B Biol. Sci. 2014, 369, 20130362. [Google Scholar] [CrossRef]
- Fehr, E.; Fischbacher, U. Social norms and human cooperation. Trends Cogn. Sci. 2004, 8, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Madsen, E.A.; Tunney, R.J.; Fieldman, G.; Plotkin, H.C.; Dunbar, R.I.M.; Richardson, J.; McFarland, D. Kinship and altruism: A cross-cultural experimental study. Br. J. Psychol. 2007, 98, 339–359. [Google Scholar] [CrossRef] [PubMed]
- Fehr, E.; Gächter, S. Altruistic punishment in humans. Nature 2002, 415, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Testa, M.F. Introduction: Kinship care policy and practice: (Second issue). Child Welf. 2016, 95, 13–39. [Google Scholar]
- Consumer Financial Protection Bureau. CFPB Financial Well-Being Scale: Scale Development Technical Report; CFPB: Washington, DC, USA, 2017. [Google Scholar]
- Chung, G.; Ansong, D.; Brevard, K.C.; Chen, D.G. Identifying treatment moderators of a trauma-informed parenting intervention with children in foster care: Using model-based recursive partitioning. Child Abus. Negl. 2021, 117, 105065. [Google Scholar] [CrossRef] [PubMed]
- Shepherd-Banigan, M.; Smith, V.A.; Lindquist, J.H.; Cary, M.P.; Miller, K.E.M.; Chapman, J.G.; Van Houtven, C.H. Identifying treatment effects of an informal caregiver education intervention to increase days in the community and decrease caregiver distress: A machine-learning secondary analysis of subgroup effects in the HI-FIVES randomized clinical trial. Trials 2020, 21, 189. [Google Scholar] [CrossRef]
- Lino, M.; Kuczynski, K.; Rodriguez, N.; Schap, T. Expenditures on Children by Families, 2015; Miscellaneous Publication No. 1528-2015; U.S. Department of Agriculture, Center for Nutrition Policy and Promotion: Alexandria, VA, USA, 2017. [Google Scholar]
- Althubaiti, A. Information bias in health research: Definition, pitfalls, and adjustment methods. J. Multidiscip. Healthc. 2016, 9, 211–217. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).