Abstract
An earthquake of magnitude 7.8 MW and 6.8 MW struck Nepal on 25 April and 12 May, 2015, respectively, which caused massive damage. In such crises, understanding the water, sanitation, and hygiene (WASH) situation is of paramount importance. Therefore, we aimed to assess the WASH situation and its impact on health, particularly in the Sindhupalchowk district. A questionnaire survey and microbial analysis of water samples were conducted. Descriptive statistics and parametric and non-parametric statistical tests were employed. The results revealed that 97.1% of water samples from the source during the pre-monsoon season and 98.5% during the monsoon season had fecal contamination. Similarly, 92.8% of water samples during the pre-monsoon season and 96.7% during the monsoon season at point of use (PoU) had fecal contamination. Furthermore, water consumption was comparatively less during the pre-monsoon season. The increase in water consumption improved hygiene behavior and lowered the prevalence of waterborne diseases. Similarly, less water consumption affected water handling behavior; for example, the cleaning interval of storage vessels was less frequent. An increase in cleaning interval resulted in fecal contamination of water at PoU. The findings of this study can be useful in the review of existing WASH policy and plans and integration with the disaster management plan for disaster risk reduction.
1. Background
During humanitarian emergencies engendered by natural disasters such as earthquakes, water, sanitation, and hygiene (WASH) is the most crucial aspect to consider, as it is a major lifeline and immediately needed for consumption, hygiene, support in relief and rescue, and normal activities [1,2]. There is a high possibility of a significant impact on the WASH situation after an earthquake. Some examples are (i) due to the movement of tectonic plates beneath the ground, certain portions of rocks and ground become squeezed while others expand, resulting in a change in the groundwater table, as well as a change in the pathways of springs, which might reduce or stop the water yield at the sources in hilly areas [3]; (ii) damage to water supply infrastructures, which hampers access to improved water [2]; (iii) an increase in the porosity of soil as a result of the earthquake, which accelerates the percolation of pollutants through pores, causing water quality degradation [4]; (iv) damage to sanitation facilities [2]; and (v) reduced hygiene practices [5] in the post-earthquake situation [6,7].
Inadequate WASH services can further increase the risk of cascading events such as epidemics of waterborne diseases and several social problems [8,9]. WASH intervention is important for the prevention of the transmission of bacteria such as Salmonella typhi, E. coli, and Vibrio cholerae, and viruses such as hepatitis A and E are responsible for the transmission of waterborne diseases such as, typhoid, diarrhea, cholera (diarrheal illness), and other hepatitis A and E diseases [10,11,12,13]. The number of people in need of water and sanitation following a disaster is much greater than the number of people killed, injured, displaced, or needing medical attention [2]. For instance, the Haiti earthquake revealed a higher number of cholera outbreaks than those affected by the earthquake because of the lack of priority and sufficient investment given to WASH [14]. These events have further brought attention to the maintenance of health and the importance of WASH during hazards such as earthquakes.
In Nepal, massive earthquakes with a magnitude of 7.6 MW on 25 April and 6.8 MW on 12 May, 2015, led to 8702 deaths and 22,303 injuries. Subsequent aftershocks, resulting landslides, and avalanches caused widespread damage to livelihoods and had a huge impact on water supply, quality, and availability, affecting millions of people across the country. Out of a total of 11,288 water supply systems in the 14 most-affected districts, 1570 sustained major damages, 3663 partial damages, and approximately 220,000 toilets were destroyed [15]. Many water springs, which are major sources of drinking water in mid-hills, also dried up as a consequence of the earthquakes [16]. In addition, several experts have also raised concerns about the risk of a waterborne disease outbreak in Nepal in a post-disaster situation [17]. Furthermore, Nepal lies in a seismically active area due to which there is a greater possibility of the occurrence of earthquakes in the future, posing a huge potential threat to the community and highlighting the urgent need to take pivotal steps [18]. Global goals and several policy documents have also emphasized the consideration of WASH, which should be prioritized in such situations. The target numbers 6.1, 6.2, 6.3, and 6.6 of Sustainable Development Goal (SDG) 6 regarding ‘Clean water and sanitation’ underscores access to adequate WASH and water source protection. The progress of SDG 6 is important to achieving SDG 3 on ‘Health and well-being’ [19]. Moreover, the National Policy for Disaster Risk Reduction 2018 [20] aims to reduce the number of affected people and the risk of damage to basic services, including water, sanitation, and hygiene. The Disaster Risk Reduction National Strategic Action Plan 2018–2030 [21] of the Government of Nepal has also set a target for reducing disaster loss, considering the SDGs to reduce disaster impact substantially by 2030. Moreover, the Sendai Framework for Disaster Risk Reduction emphasizes understanding vulnerabilities and disaster risk as an initial step for risk reduction [22]. Accordingly, the identification of vulnerabilities in the WASH sector during a disaster should be prioritized to reduce the risk.
Limited information on exposure to hazards, its effect on the WASH situation, and the subsequent impact on health among concerned authorities and communities can further aggravate the risk. Therefore, to improve the understanding, our study aimed to examine the status of WASH and its impact on health in the aftermath of an earthquake in the pre-monsoon and monsoon seasons. We considered two seasons in this study for two reasons. First, water availability drastically decreases in the pre-monsoon season, and, second, water quality also varies significantly in these two seasons. As a result, the WASH situation and its impact could vary [23,24]. Understanding the existing vulnerabilities in the WASH sector after an earthquake will further guide the reviewing, updating, and/or formulating of disaster management policy and plans on earthquake preparedness, mitigation, response, and recovery to ultimately establish a disaster-resilient community.
2. Methodology
2.1. Study Area
The study was conducted in the Sindhupalchowk district of Nepal. The area of the district is 2542 km2, with three urban municipalities and nine rural municipalities. There are 66,635 households and a population of 287,798 in the district. The district was one of the most affected by the earthquake on the basis of per-capita disaster effects among the severely affected 14 districts, as stated by the National Planning Commission [15].
The administration division was redefined within the Sindhupalchowk district during the project period. We planned and used the previous administrative division (with 2 municipalities and 77 village development committees (VDCs).
2.2. Sampling
Sampling was performed using the 30 × 7 cluster sampling method used in humanitarian emergencies [25,26,27,28]. It was a two-stage sampling method based on probability proportional to size (PPS). In the first stage, we selected 30 clusters, and 1 ward was considered as a cluster. A ‘ward’ is the smallest administrative unit of the local government of Nepal, i.e., village-level or municipality-level governments. In the second stage, seven households were selected in each cluster. The total sample size was 210 households. The nine municipalities and VDCs selected for sampling were Tatopani VDC (Wards 1, 3, and 4), Ramche VDC (Wards 5 and 7), Mankha VDC (Wards 1, 4, 6, 7, and 9), Chautara Municipality (Wards 1–4 and 7), Irkhu VDC (Wards 1 and 5), Selang VDC (Ward 7), Bhimtar VDC (Wards 1 and 4), Melamchi Municipality (Wards 3–7), and Helambu VDC (Ward 1) (Figure 1).
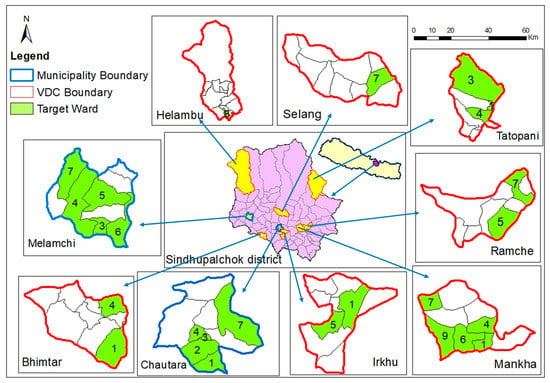
Figure 1.
Wards of the municipalities and village development committees (VDCs) selected for sampling in Sindhupalchowk district.
2.3. Data Collection
2.3.1. Questionnaire Survey
Trained enumerators visited the selected clusters and interviewed household family members. A structured questionnaire with a specific set of questions was used to collect data on water supply, sanitation, and hygiene and health status for the quantitative survey. The questionnaire was included in Appendix A (Table A1). Before conducting the survey, written informed consent was provided to all respondents. The survey was conducted in the pre-monsoon (April–May) and monsoon seasons (August–September). The duration of the pre-monsoon season is from March to May, and the monsoon season is from June to September.
2.3.2. Water Sampling
Sampling of water from sources and PoU was conducted to identify whether the water was safe for drinking or not. For this, two types of kits were used. The first type was the Coliforms P/A (H2S) Test Vial, and the second type was the HiSelectiveTM H2S Medium Kit with the vial. The suppliers of these kits are Eco Concern Pvt. Ltd., Lalitpur, Nepal, and HiMedia Laboratories Pvt. Ltd., Maharashtra, India, respectively. These kits do not provide quantitative information on microbial water quality but only qualitative information through changes in color and turbidity, thus indicating microbial contamination.
The caps of these vials are sealed air-tight and opened when placing the water sample. Then, the caps are kept air-tight after placing the water sample. The amount of water sample to be placed in these vials is indicated by a mark, which is 30 mL in the first type and 20 mL in the second type.
The water samples were collected directly into the vials from the water sources and the surveyed households at their PoU. In the case of difficulty in water sample collection and placing the water samples in the vials, a sterilized polyethylene beaker (50 mL) was used. The water samples were stored in an ice box transported to the field base within 2 to 4 h, and incubated in a portable incubator.
2.4. Measurement
The types of water sources used were identified by asking the households to choose the source of water used for household purposes. Responses were categorized as improved source (treated water supply), unimproved source (spring sources with protection not ensured), and surface water source (river water) [29]. The total water consumption of households in liters per day for drinking, cooking, and hygiene purposes was based on self-reported data. Then, the amount was divided by the number of family members in the household to calculate the water consumption in liters per capita per day (L/c/d). The water consumption data were further categorized as households using <50 L/c/d of water and those using 50 L/c/d or more of water. According to the definition of WHO, 50 L/c/d of water is required for consumption, hygiene, and laundry [30]. The cleaning interval of the storage vessel was determined by asking ‘When did you cleaned the storage vessel last time?’ The prevalence of waterborne disease was determined by asking ‘Did you or any of your family member have any of following diseases last month?’ The responses included diarrhea, hepatitis (A or E), and typhoid. If any of the family members had the aforementioned waterborne diseases, then they were categorized as a household having the waterborne disease. Moreover, solid waste was considered as any non-liquid waste generated from households, such as degradable waste, packaging materials, plastics, metals, glasses, furniture, textiles, electronics, batteries from VDCs, and municipalities. Data on solid waste handling practices by households were collected by asking ‘How do you dispose solid waste?’, and the answers included burn, bury, and throw outside. Similarly, information on toilet use was also collected to determine if they had access to toilets or not. Furthermore, personal hygiene was measured using a 4-point Likert-scale questionnaire comprising 10 questions on activities related to hygiene. The score of the questionnaire ranges from never (1) to most of the time (4), with a total score of 40.
2.5. Analysis
2.5.1. Water Quality Analysis
The Coliforms P/A (H2S) Test Vial was filled with a 30 mL water sample and incubated at 44 °C for 48 h. The detection of black color after incubation indicated the presence of fecal contamination. Similarly, the HiSelectiveTM H2S Medium Kit contains a sterile bottle with powder medium. The bottle was filled with a water sample up to the arrow mark (20 mL) and swirled to dissolve the powder completely. The sample was incubated at 35 °C for 48 h. After incubation, we observed the following colors with turbidity, indicating the presence of given microorganisms: dark purple color (Klebsiella species, Enterobacter species), bluish-green color (Escherichia coli, Shigella species, and Streptococcus species, Pseudomonas species), bluish-purple color (Vibrio species), or black color (Citrobacter species and Salmonella species). The water was considered as not fit for drinking if any of these colors were observed.
2.5.2. Statistical Analysis
Descriptive statistics such as frequency, proportion, mean, and median of different variables were calculated. McNemar’s test and Fisher’s exact test were used for categorical variables. Pearson’s correlation coefficient, Wilcoxon test, Mann–Whitney U-test, and independent samples t-test were used for continuous variables. The significance level was set at p < 0.05 for all statistical tests. Chronbach’s alpha was used to evaluate the reliability of the hygiene questionnaire.
3. Results
3.1. Water Use and Sanitation
The proportion of households using unimproved water sources was 167 (80%) and improved sources 42 (20%) in the pre-monsoon season. Similarly, the proportion of households using unimproved sources, improved sources, and surface water sources was 163 (78%), 42 (20%), and 4 (2%), respectively, in the monsoon season (Figure 2). Regarding water consumption, 64 (31.7%) households in the pre-monsoon season and 75 (37.1%) in the monsoon season used 50 L/c/d or more of water for domestic purposes. The proportion of households using water <50 L/c/d was higher in the pre-monsoon season (138) (68.3%) compared to the monsoon season (127) (62.9%), with a statistically significant relationship (p = 0.01). The median values of water consumption were 26.6 L/c/d in the pre-monsoon season and 33.3 L/c/d in the monsoon season. The amount was less in the pre-monsoon season than in the monsoon season, with statistical significance (p < 0.001) (Table 1).
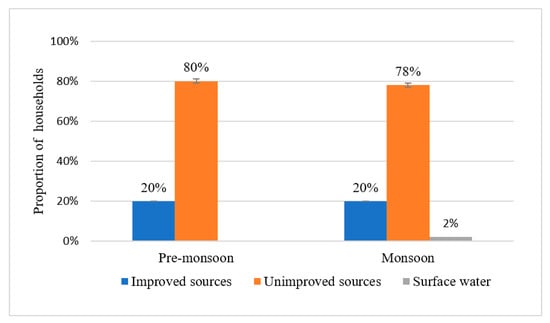
Figure 2.
Proportion of households with types of water source used during pre-monsoon (N = 209) and monsoon seasons (N = 209).

Table 1.
Household characteristics with water use.
The proportion of households with fecal contamination at the source was 204 (97.1%) and at PoU was 195 (92.8%) in the pre-monsoon season (Figure 3). Similarly, the proportion of households with fecal contamination at the source was 206 (98.5%) and at PoU was 202 (96.7%) in the monsoon season (Figure 4). Regarding waste handling practice, most of the households buried waste 199 (95.2%), followed by burning (157) (75.1%) and throwing outside (111) (53.1%). Moreover, 201 (96.1%) of them used toilets (Figure 5).
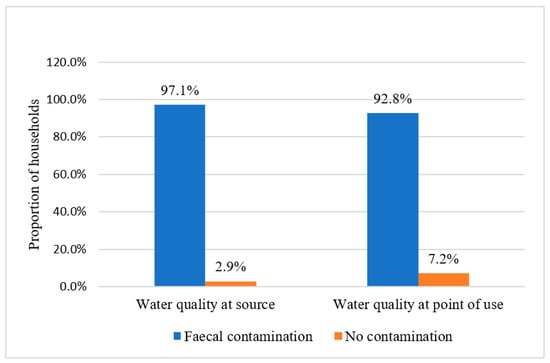
Figure 3.
Fecal contamination of water at source and point of use during pre-monsoon season (N = 210).
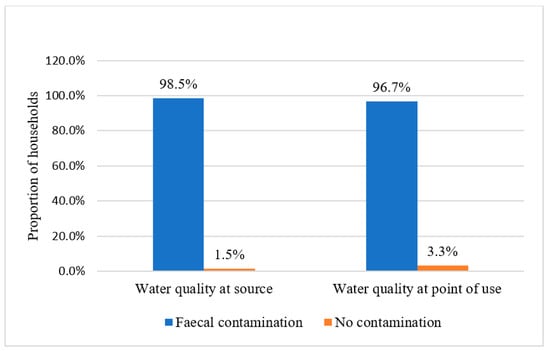
Figure 4.
Fecal contamination of water at source and point of use during monsoon season (N = 209).
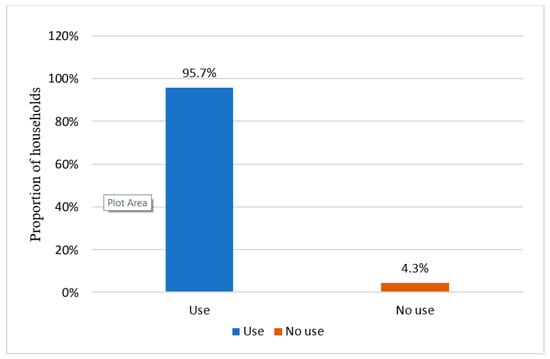
Figure 5.
Proportion (N = 210) of households with toilet use.
3.2. Water Use and Waterborne Diseases
The proportion of households with waterborne diseases was higher (20) (9.5%) during the pre-monsoon season compared to the monsoon season (18) (8.6%), though this relationship was statistically insignificant (Table 2).
Table 2.
Proportion of households with waterborne diseases.
The proportion of households having waterborne diseases was highest among those that consumed less than 50 L/c/d of water in both the pre-monsoon season (18) (13%) (p = 0.02) and the monsoon season (16) (12%) (p = 0.02), with statistically significant relationships (Table 3). Chronbach’s alpha value of the Likert-scale questionnaire for measuring personal hygiene was 0.8. The independent samples t-test showed that there was a statistically significant relationship between water consumption and hygiene behavior (p < 0.001) and higher mean values of hygiene behavior observed among households that had access to 50 L/c/d or more of water (m = 36.5) than those using less water (m = 30.2) in the pre-monsoon season. In the monsoon season, the mean value of hygiene behavior was m = 35.3 among the households using 50 L/c/d or more of water, and the value was m = 31 among those using less water, with a statistically significant relationship (p < 0.001). The result further depicted the statistically significant relationship between households having waterborne diseases and hygiene behavior (p < 0.001), with higher mean values of hygiene behavior among the households without the prevalence of disease (m = 32.7) than those with the prevalence of disease (m = 27.9) in the pre-monsoon season. Likewise, in the monsoon season, the mean value of hygiene behavior was higher among the households without the prevalence of waterborne disease (m = 33) compared to those with waterborne diseases (m = 29.6), and the relationship was statistically significant (p < 0.001).
Table 3.
Relationship between water consumption and waterborne disease.
The proportion of households with waterborne diseases was higher among households with fecal contamination at point of use in the monsoon season. During the pre-monsoon season, among the households (n = 195) having fecal contamination of water at PoU, 17 (8.7%) had waterborne diseases. Among the households (n = 15) not having fecal contamination at PoU, 3 (20%) had waterborne diseases. Similarly, during the monsoon season, among the households (n = 202) having fecal contamination at PoU, 18 (9.2%) had waterborne diseases, and among the households (n = 7) without fecal contamination at PoU, none of the waterborne diseases were recognized (Figure 6).
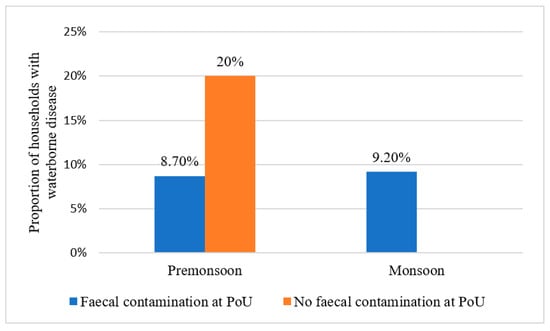
Figure 6.
Proportion of households with waterborne diseases and fecal contamination of water at PoU during pre-monsoon and monsoon seasons.
There was a significant negative correlation between the cleaning interval of storage vessels (r = −0.40, p ≤ 0.01) and the total amount of water consumption in both seasons, which revealed that the cleaning interval increased with a decrease in the amount of water consumption. Similarly, the Mann–Whitney U-test showed that there was a statistically significant difference in cleaning interval among the households with and without fecal contamination of water at point of use in the pre-monsoon season (p = 0.01) and the monsoon season (p = 0.04), stating that the increase in cleaning interval might cause fecal contamination.
4. Discussion
The vulnerabilities in the WASH sector identified were limited access to improved water supply sources, lack of sufficient quantity of water for domestic purposes, poor water quality, hygiene, and safe water storage, which increased the risk of waterborne diseases.
This study revealed that the number of households using unimproved sources was very high. The proportion was higher than the national average, i.e., 7% [29]. The use of improved sources should be increased with the assurance of water quality. Households without access to sufficient water (<50 L/c/d) had a high prevalence of waterborne diseases in both the pre-monsoon and monsoon seasons. The reason for this is that less water consumption hinders hygiene behavior, which increases the risk of waterborne diseases. A similar study conducted in Kathmandu Valley of Nepal also demonstrated a high prevalence of diarrhea among the households consuming less water [31]. Moreover, several other studies have also stated that good hygiene with a sufficient amount of safe water is associated with a decrease in diarrhea [32,33], typhoid [34], and hepatitis A and E [13]. This evidence can be further explained based on whether the microorganisms are spread by direct or indirect contact. Direct contact comprises person-to-person contact, including the fecal–oral route, whereas indirect contact with pathogens occurs because of cross-contamination, especially by the transfer of potentially harmful microorganisms from one surface to another, including the hands or food. In households, microorganisms spread and grow, particularly on kitchen surfaces, in bathrooms, and in laundry areas [35]. Therefore, the home environment plays a significant role in transmitting infectious diseases [36]. In such circumstances, a sufficient amount of water, along with hygiene at the personal and household levels, strongly acts as a barrier to break the fecal–oral route and reduce the risk of disease [37].
In addition to these factors, proper handling and safe storage of water at PoU is equally important [38,39]. Maintaining the cleanliness of storage vessels is one of the key factors required for safe storage [40]. In our study, the cleaning interval of storage vessels depended on water availability since it increases the ease of maintaining the vessels’ cleanliness. The increase in cleaning interval intensified the risk of fecal contamination, and the use of fecally contaminated water at PoU further increased the occurrence of waterborne diseases. The findings of our study were in line with a study conducted in the slums of Kenya, which also uncovered that the lack of properly cleaned storage vessels caused recontamination of water at point of use as a result of the number of pathogens attached to the container walls and the formation of biofilm [40]. Biofilm formation and fecal indicator bacteria increased with long storage time, which significantly contributed to early-childhood diarrhea in South Africa [41]. Similarly, a study conducted in Kathmandu Valley also illustrated that water quantity influenced the cleanliness of storage vessels and the quality of stored water [42]. Our study summarized that the cleanliness of storage vessels for the safe storage of water can be maintained only by sufficient access to water, further aiding in minimizing the prevalence of waterborne diseases. In addition, several studies have also illustrated the importance of household water treatment at PoU to maintain the quality of stored water [43,44]. However, the treatment will be more effective if water is stored in clean vessels [40].
In the pre-disaster phase, mitigation measures and preparedness for improving water availability should include the exploration of alternative water sources, construction of seismic-resistant water supply sources, promotion of rainwater-harvesting practices, construction of seismic-resistant rainwater collection cisterns [7,45], and implementation of efficient measures for water conservation at the community level, as it will reduce the risk associated with water scarcity [45,46].
Our study also showed that most of the water samples from the source were found to be fecally contaminated in both seasons. The contamination may be attributed to the lack of source protection and cleanliness. Though many households used toilets in the study area, understanding land-use practice and wastewater management is important to trace the source of water contamination. On the other hand, unsafe and haphazard solid waste disposal observed in the study area might also increase the risk of groundwater pollution [47]. It further contaminates the surrounding environment by increasing the breeding of vectors that carry the pathogens of fecal–oral disease [48]. Moreover, the hydrogeological and hydrochemical changes after an earthquake also affect microbial communities, which increase fecal contamination [49]. Fecal contamination in water sources is always considered as one of the major issues in the post-disaster scenario [50]. For instance, an increase in the microbial contamination of water sources was found in Kathmandu, Nepal, after the 2015 Gorkha Earthquake [3], and in Pakistan after the 2005 earthquake [51]. Similarly, after the Haiti earthquake in 2010, 24.6% of improved sources and 80.9% of unimproved sources of water were found to have fecal contamination in the post-earthquake scenario [52].
In such situations, several measures of water source protection should be implemented. The construction of seismic-resistant sewage facilities can prevent nearby water source pollution from wastewater. Moreover, the disposal of solid waste in an appropriate manner in a sanitary landfill site and the isolation of waste to prevent leachate movement through the installation of barrier liners [53], along with the reduce, reuse, recycle (3R) principles [54], can help to make the surrounding environment and groundwater less polluted.
Although there are some programs that have been implemented concerning WASH after the earthquake in the Sindhupalchowk district [55], regular monitoring and evaluation of these programs are very important to understand their effectiveness, along with planning for introducing new programs. Therefore, capacity-building programs for relevant and responsible stakeholders working for disaster risk management should be emphasized. Such programs should include education on disaster risk, hazards, vulnerabilities, preparedness and response, transmission routes and prevention of disease, effective integration of WASH into the disaster management plan, and managing the financing of WASH interventions and sustainability of programs and facilities [56].
Some examples, such as the integration of WASH for Disaster Risk Reduction (DRR) in the Public Health Project of Kenya (2007/08) by Oxfam Great Britain, the community water security program in Myanmar (2008/2009) by the International Rescue Committee, and the Livelihood and Shelter Project in India (2010/2011) by Care India, were successful in increasing the resilience of the community’s people [45].
5. Conclusions
This study is important to understand the vulnerabilities in the WASH sector in earthquake-affected areas. Most households did not have access to improved water sources and enough water (50 L/c/d) required for domestic purposes. The proportion of households without access to enough water was higher during the pre-monsoon season. A higher prevalence of waterborne diseases was observed among households without sufficient access to water (<50 L/c/d) in both seasons due to the lack of sufficient quantities of water, which adversely impacted hygiene practices, resulting in poor health. Fecal contaminations at the source and point of use were also observed in many households as a result of the lack of source protection and cleanliness of the storage vessel hindering safe water storage. The risk of water source contamination can be reduced by emphasizing the sanitation situation, such as (i) controlling the haphazard disposal of solid waste in the study area by proper solid waste management and (ii) having a detailed understanding of liquid waste generation and land-use practice, along with the implementation of their proper management. Conclusively, water, sanitation, and hygiene facilities reduce the transmission of disease-causing pathogens and lessen the risk of waterborne disease outbreaks. Moreover, access to sufficient quantities of water acts as a key factor in maintaining hygiene, as well as water quality, at the household level. For this reason, priority should be given to the capacity building of the community’s people and concerned organizations working in this sector, which will help in integrating and fulfilling safely managed WASH [29] in the disaster management plan. This plan should aim to increase the availability of water quantity, improve water quality, promote hygiene, safe water handling and storage, proper solid waste management, etc., to increase community resilience. The research findings will also help to guide the formulation of a disaster management plan and the integration of WASH in developing countries with limited facilities.
Limitations of the study: We used kits for microbial water quality analysis in our study. Due to the lack of resources and remoteness of the study area, we were not able to conduct a detailed lab analysis to detect specific microbiological organisms and quantify the microbial contamination. Moreover, we did not measure chlorine residual in the water samples. Many places in the study areas were damaged by the earthquake, further creating difficulties in data collection and access to facilities.
Author Contributions
Conceptualization, S.S., R.M. and F.K.; methodology, S.S. and R.M.; formal analysis, S.S. and R.M.; investigation, S.S.; resources, R.M.; writing—original draft preparation, S.S.; writing—review and editing, R.M. and F.K.; supervision, project administration, S.S. and R.M.; funding acquisition, R.M. and F.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research is funded by the Kurita Water and Environment Foundation (KWEF), Japan under its Special Earthquake Fund for Nepal.
Institutional Review Board Statement
The study was undertaken after the approval from the District Development Committee Sindhupalchowk of the Government of Nepal.
Informed Consent Statement
Informed consent was obtained from all the participants involved in the study.
Data Availability Statement
Data will be available on request.
Conflicts of Interest
The authors of this study declare no conflict of interest.
Appendix A
WASH and Health in Sindhupalchowk district of Nepal after the Gorkha Earthquake.
Table A1.
Survey Questionnaire.
Table A1.
Survey Questionnaire.
| Q.N.1 Do you or any of your family member have any of following diseases last month? Please choose the appropriate answers. (√) | ||||||
| (i) Diarrhoea | (ii) Hepatitis A and E | (iii) Typhoid | ||||
| Q.N.2 How many family members do you have in your family? | ||||||
| Q.N.3 Please choose the water source used for household purpose (√) and also mention the amount of water used. | ||||||
| S.N. | Types of water source | Total amount of water used by household (liters/day) | ||||
| 1. | Water supply system | |||||
| 2. | Spring | |||||
| 3. | River | |||||
| 4. | Others | |||||
| Q.N.4 When did you clean storage vessel last time? | ||||||
| …………days ago | ||||||
| Q.N.5 Do you use toilet? | ||||||
| (i) Yes | (ii) No | |||||
| Q.N.6 How do you dispose solid waste? | ||||||
| (i) Burn | (ii) Bury | (iii) Throw outside | ||||
| (iv) Others | ||||||
| Q.N.7 Please choose the answer appropriate for you regarding hygiene behaviour (√) | ||||||
| S.N. | Items | Most of the time | Sometimes | Rarely | Never | |
| (1) | Do you wash your hand after going to toilet? | |||||
| (2) | Do you wash your hand before eating? | |||||
| (3) | Do you wash your hand before preparing food? | |||||
| (4) | Do you wash your hand after getting home? | |||||
| (5) | Do you use soap to wash your hand? | |||||
| (6) | Do you take a bath regularly? | |||||
| (7) | Do you wash your clothes regularly? | |||||
| (8) | Do you clean toilet regularly? | |||||
| (9) | Do you clean the kitchen regularly? | |||||
| (10) | Do you wash fruits and vegetables with sufficient water? | |||||
References
- Ersel, M. Water and Sanitation Standards in Humanitarian Action. Turk. J. Emerg. 2015, 15, 27–33. [Google Scholar] [CrossRef]
- PAHO. The Challenges in Disaster Reduction for the Water and Sanitation Sector. 2006. Available online: https://www3.paho.org/disasters/index.php?option=com_content&view=category&view=article&id=657&Itemid=1&lang=en (accessed on 4 May 2022).
- Nepal, S. How Big Earthquakes Rattle Spring Dynamics. ICIMOD. 2015. Available online: https://www.icimod.org/article/how-big-earthquakes-rattle-spring-dynamics/ (accessed on 4 May 2022).
- Pant, B.; Thapa, K.; Koju, R. Post-earthquake drinking water quality in the Kathmandu valley: A pilot study. Al. Ameen. J. Med. Sci. 2016, 9, 130–133. [Google Scholar]
- UNHCR. Water, Sanitation and Hygiene in Post Emergency Contexts. 2018. Available online: https://oxfamilibrary.openrepository.com/bitstream/handle/10546/620598/rr-wash-post-emergency-delivery-041218-en.pdf;jsessionid=2018079FED033226194CCE98EB69723E?sequence=1 (accessed on 4 May 2022).
- Uprety, S.; Hong, P.Y.; Sadik, N.; Dangol, B.; Adhikari, R.; Jutla, A.; Shisler, J.L.; Degnan, P.; Nguyen, T.H. The Effect of the 2015 Earthquake on the Bacterial Community Compositions in Water in Nepal. Front. Microbiol. 2017, 8, 2380. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.T.; Han, M.Y. Water environmental and sanitation status in disaster relief of Pakistan’s 2005 earthquake. Desalination 2009, 248, 436–445. [Google Scholar] [CrossRef]
- AGUASAN. Briefing Note: Disaster Risk Reduction in WASH. 31st AGUASAN Workshop. 2015. Available online: http://www.aguasan.ch/ws2015/AGUASAN_Workshop_2015_Briefing_Note.pdf (accessed on 20 February 2022).
- Simkhada, P.; Teijlingen, E.V.; Pant, P.R.; Sathian, B.; Tuladhar, G. Public Health, Prevention and Health Promotion in Post-Earthquake Nepal. Nepal. J. Epidemiol. 2015, 5, 462–464. [Google Scholar] [CrossRef]
- Matrajt, G.; Lillis, L.; Meschke, J.S. Review of Methods Suitable for Environmental Surveillance of Salmonella Typhi and Paratyphi. Clin. Infect. Dis. 2020, 71, S79–S83. [Google Scholar] [CrossRef] [PubMed]
- Hunter, P.R. Drinking water and diarrhoeal disease due to Escherichia coli. J. Water Health 2003, 1, 65–72. [Google Scholar] [CrossRef]
- Dan-Nwafor, C.C.; Ogbonna, U.; Onyiah, P.; Gidado, S.; Adebobola, B.; Nguku, P.; Nsubuga, P. A cholera outbreak in a rural north central Nigerian community: An unmatched case-control study. BMC Public Health 2019, 19, 112. [Google Scholar] [CrossRef]
- Kadri, S.M.; Rehman, S.U.; Rehana, K.; Benetou, D.R.; Ahmad, D.F.; Abdullah, A.; Chattu, V.K. Hepatitis A and E Outbreak Surveillance during 2015–2017 in Kashmir, India: Is the Water to Blame? J. Epidemiol. Glob. Health 2018, 8, 203–207. [Google Scholar] [CrossRef]
- Gelting, R.; Bliss, K.; Patrick, M.; Lochart, G.; Handzel, T. Water, Sanitation and Hygiene in Haiti: Past, Present and Future. Am. J. Trop Med. Hyg. 2013, 89, 665–670. [Google Scholar] [CrossRef]
- NPL. Post Disaster Need Assessment; National Planning Commission; Government of Nepal: Kathmandu, Nepal, 2015.
- Adhikari, S.; Harada, K.; Dahal, N.K.; Kandel, S. Earthquake Impacts on the Livelihoods of Community Forest Users in Sindhupalchok District, Nepal, and Their Perceptions towards Forest Conservation. Conservation 2021, 1, 327–341. [Google Scholar] [CrossRef]
- Bagcchi, S. Risk of Infection after the Nepal earthquake. Lancet 2015, 15, 770–771. [Google Scholar] [CrossRef]
- Dube, S. Earthquake in Nepal: A Miserable Environmental Hazard Visited by Nature. Acad. Voices A Multidiscip. J. 2016, 5, 56–66. [Google Scholar] [CrossRef][Green Version]
- UN General Assembly, Transforming Our World: The 2030 Agenda for Sustainable Development, 21 October 2015, A/RES/70/1. Available online: https://www.refworld.org/docid/57b6e3e44.html (accessed on 20 February 2022).
- MoHA. National Policy for Disaster Risk Reduction 2018; Ministry of Home Affairs; Government of Nepal: Kathmandu, Nepal, 2018.
- MoHA. MDisaster Risk Reduction National Strategic Action Plan 2018–2030. Ministry of Home Affairs; Government of Nepal: Kathmandu, Nepal, 2018. [Google Scholar]
- UN. Sendai Framework for Disaster Risk Reduction 2015–2030. In Proceedings of the Third UN World Conference. Sendai, Japan, 18 March 2015. [Google Scholar]
- Shrestha, S.; Nakamura, T.; Malla, R.; Nishida, K. Seasonal variation in the microbial quality of shallow groundwater in the Kathmandu Valley, Nepal. Water Sci. Technol. Water Supply. 2014, 14, 390–397. [Google Scholar] [CrossRef]
- Pokhrel, G.; Rijal, M.L. Seasonal Variation of Springwater In-Situ Parameters in the Bhusundi Catchment, Gorkha, Nepal. J. Inst. Sci. Technol. 2020, 25, 45–51. [Google Scholar] [CrossRef]
- WHO. Training for Mid-Level Managers (MLM). Module 7: The EPI Coverage Survey; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Bilukha, O.O. Old and new cluster designs in emergency field surveys: In search of a one-fits-all solution. Emerg. Themes Epidemiol. 2008, 5, 7. [Google Scholar] [CrossRef]
- Woodard, S.H. Description and Comparison of the Methods of Cluster Sampling and Lot Quality Assurance Sampling to Assess Immunization Coverage; World Health Organization: Geneva, Switzerland, 2001; Available online: https://apps.who.int/iris/handle/10665/66867 (accessed on 3 May 2022).
- Henderson, R.H.; Sundaresan, T. Cluster sampling to assess immunization coverage: A review of experience with a simplified sampling method. Bull. World Health Organ. 1982, 60, 253–260. Available online: https://apps.who.int/iris/handle/10665/264739 (accessed on 3 May 2022).
- WHO/UNICEF. Progress on Drinking Water, Sanitation and Hygiene: 2017 Update and SDG Baselines; World Health Organization (WHO); the United Nations Children’s Fund (UNICEF): Geneva, Switzerland, 2017. [Google Scholar]
- WHO. Guidelines for Drinking Water Quality; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Shrestha, S.; Aihara, Y.; Yoden, K.; Yamagata, Z.; Nishida, K.; Kondo, N. Access to improved water and its relationship with diarrhoea in Kathmandu Valley, Nepal: A cross-sectional study. BMJ Open 2013, 3, e002264. [Google Scholar] [CrossRef] [PubMed]
- Pinfold, J.V.; Horan, N. Measuring the effect of a hygiene behaviour intervention by indicators of behaviour and diarrhoeal disease. Trans. R. Soc. Trop. Med. Hyg. 1996, 90, 366–371. [Google Scholar] [CrossRef]
- Shahid, N.S.; Greenough, W.B.; Samadi, A.R.; Huq, M.I.; Rahaman, N. Hand washing with soap reduces diarrhoea and spread of bacterial pathogens in a Bangladesh village. J. Diarrhoeal. Dis. Res. 1996, 14, 85–89. Available online: https://www.jstor.org/stable/23498442 (accessed on 15 February 2022).
- Gasem, M.H.; Dolmans, W.M.V.; Keuter, M.; Dokomoeljanto, R. Poor food hygiene and housing as risk factors for typhoid fever in Semarang, Indonesia. Trop. Med. Int. Health 2001, 6, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Zhao, P.; Zhao, T.; Doyle, M.P.; Rubino, J.R.; Meng, J. Development of a Model for Evaluation of Microbial Cross Contamination in the Kitchen. J. Food Prot. 1998, 61, 960–963. [Google Scholar] [CrossRef]
- Kagan, L.J.; Aiello, A.E.; Larson, E. The Role of the Home Environment in the Transmission of Infectious Diseases. J. Community Health 2002, 27, 247–267. [Google Scholar] [CrossRef] [PubMed]
- Curtis, V.; Cairncross, S.; Yonli, R. Domestic hygiene and diarrhoea–pinpointing the problem. Trop. Med. Int. Health 2000, 5, 22–23. [Google Scholar] [CrossRef]
- Mintz, E.; Reiff, F.; Tauxe, R. Safe Water Treatment and Storage at home: A practical new strategy to prevent waterborne disease. JAMA 1995, 273, 948–953. [Google Scholar] [CrossRef] [PubMed]
- Luby, S.P.; Agboatwalla, M.; Painter, J.; Altaf, A.; Billhimer, W.; Keswick, B.; Hoekstra, R.M. Combining Drinking Water Treatment and Hand Washing for Diarrhoea Prevention, A Cluster Randomised Controlled Trial. Trop. Med. Int. Health 2006, 11, 479–489. [Google Scholar] [CrossRef]
- Meierhofer, R.; Wietlisbach, B.; Matiko, C. Influence of container cleanliness, container disinfection with chlorine, and container handling on recontamination of water collected from a water kiosk in a Kenyan slum. J. Water Health 2019, 17, 308–317. [Google Scholar] [CrossRef]
- Mellor, J.E.; Smith, J.A.; Learmonth, G.P.; Netshandama, V.O.; Dillingham, R.A. Modeling the complexities of water, hygiene, and health in Limpopo Province, South Africa. Environ. Sci. Technol. 2012, 46, 13512–13520. [Google Scholar] [CrossRef]
- Shrestha, S.; Shrestha, S.; Aihara, Y.; Kondo, N.; Kei, N. Water Quality at Supply Source and Point of Use in the Kathmandu Valley. J. Water Environ. Technol. 2013, 11, 377–389. [Google Scholar] [CrossRef]
- Ngasala, T.M.; Masten, S.J.; Cohen, C.; Ravitz, D.; Mwita, E.J. Implementation of point-of-use water treatment methods in a rural Tanzanian community: A case study. J. Water Sanit. Hyg. Dev. 2020, 10, 1012–1018. [Google Scholar] [CrossRef]
- Clasen, T. Household Water Treatment and Safe Storage to Prevent Diarrheal Disease in Developing Countries. Curr. Envir. Health Rpt. 2015, 2, 69–74. [Google Scholar] [CrossRef] [PubMed]
- GWC. Disaster Risk Reduction and Water Sanitation and Hygiene Comprehensive Guidance; Global WASH Cluster: Geneva, Switzerland, 2011. [Google Scholar]
- Tsai, Y.; Cohen, S.; Vogel, R.M. The Impacts of Water Conservation Strategies on Water Use: Four Case Studies. J. Am. Water Resour. Assoc. 2011, 47, 687–701. [Google Scholar] [CrossRef]
- Usman, M.; Yasin, H.; Nasir, A.; Mehmood, W. 2017. A case study of groundwater contamination due to open dumping of municipal solid waste in Faisalabad Pakistan. Earth Sci. Pak. 2017, 1, 15–16. [Google Scholar] [CrossRef]
- Chavasse, D.C.; Shier, R.P.; Murphy, O.A.; Huttly, S.R.; Cousens, S.N.; Akhtar, T. Impact of fly control on childhood diarrhoea in Pakistan: Community-randomised trial. Lancet 1999, 353, 22–25. [Google Scholar] [CrossRef]
- Morimura, S.; Zeng, X.; Naoki, N.; Hosono, T. Changes to the microbial communities within groundwater in response to a large crustal earthquake in Kumamoto, Southern Japan. J. Hydrol. 2019, 581, 124341. [Google Scholar] [CrossRef]
- Oxfam. Water Quality Analysis in Emergency Situations. 2006. Available online: http://policy-practice.oxfam.org.uk/publications/water-quality-analysis-in-emergency-situations-126714 (accessed on 15 February 2022).
- Rasheed, F.; Kazmi, S.U.; Khan, A. Bacteriological analysis, antimicrobial susceptibility and detection of 16S rRNA gene of Helicobacter pylori by PCR in drinking water samples of earthquake affected areas and other parts of Pakistan. Malays. J. Microbiol. 2009, 5, 123–127. [Google Scholar] [CrossRef]
- Widmer, J.M.; Weppelmann, T.A.; Alam, M.T.; Morrissey, B.D.; Redden, E.; Rashid, M.H.; Diamond, U.; Ali, A.; De Rochars, M.B.; Blackburn, J.K.; et al. Water-related infrastructure in a region of post-earthquake Haiti: High levels of fecal contamination and need for ongoing monitoring. Am. J. Trop. Med. Hyg. 2014, 91, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Panthee, S. Possible methods of preventing groundwater contamination at landfill sites; case studies from Nepal. Bull. Dep. Geol. 2008, 11, 51–60. [Google Scholar] [CrossRef]
- Bouanini, S. The Importance of the 3R Principle of Municipal Solid Waste Management for Achieving Sustainable Development. Mediterranean. Mediterr. J. Soc. Sci. 2013, 4, 129–135. [Google Scholar] [CrossRef]
- MoFALD. Sindhupalchowk District BBB Rehabilitation and Recovery Plan; Ministry of Federal Affairs and Local Development: Kathmandu, Nepal, 2018.
- Blackwell, A. Mainstreaming Disaster Risk Reduction in WASH. In Experience in DRR mainstreaming in Nicaragua; SDC: Managua, Nicaragua, 2015. [Google Scholar]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).