
Diagnostic Potential of CTRP5 and Chemerin for Coronary Artery Disease: A Study by Coronary Computed Tomography Angiography



Abstract
1. Introduction
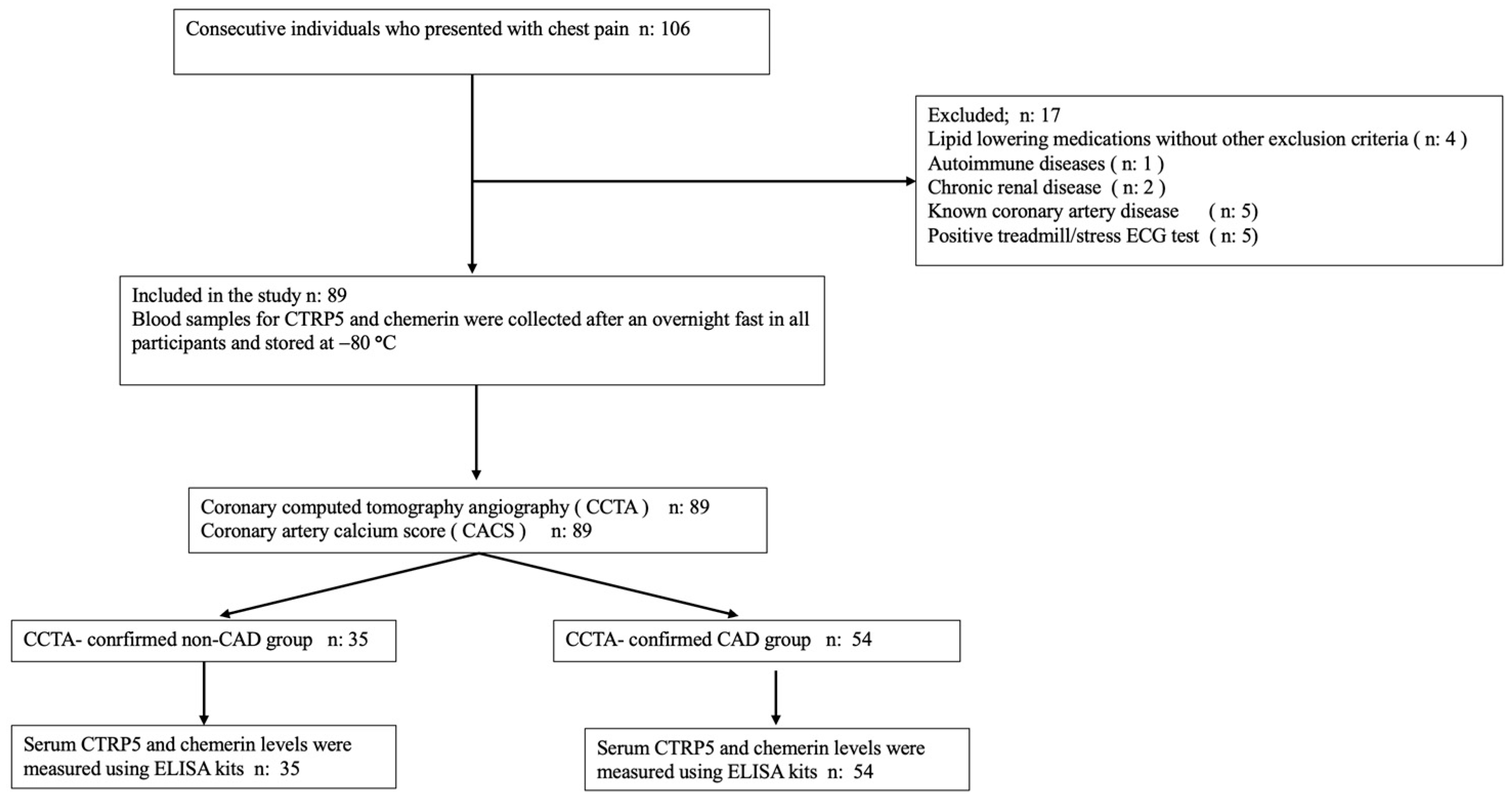
2. Materials and Methods
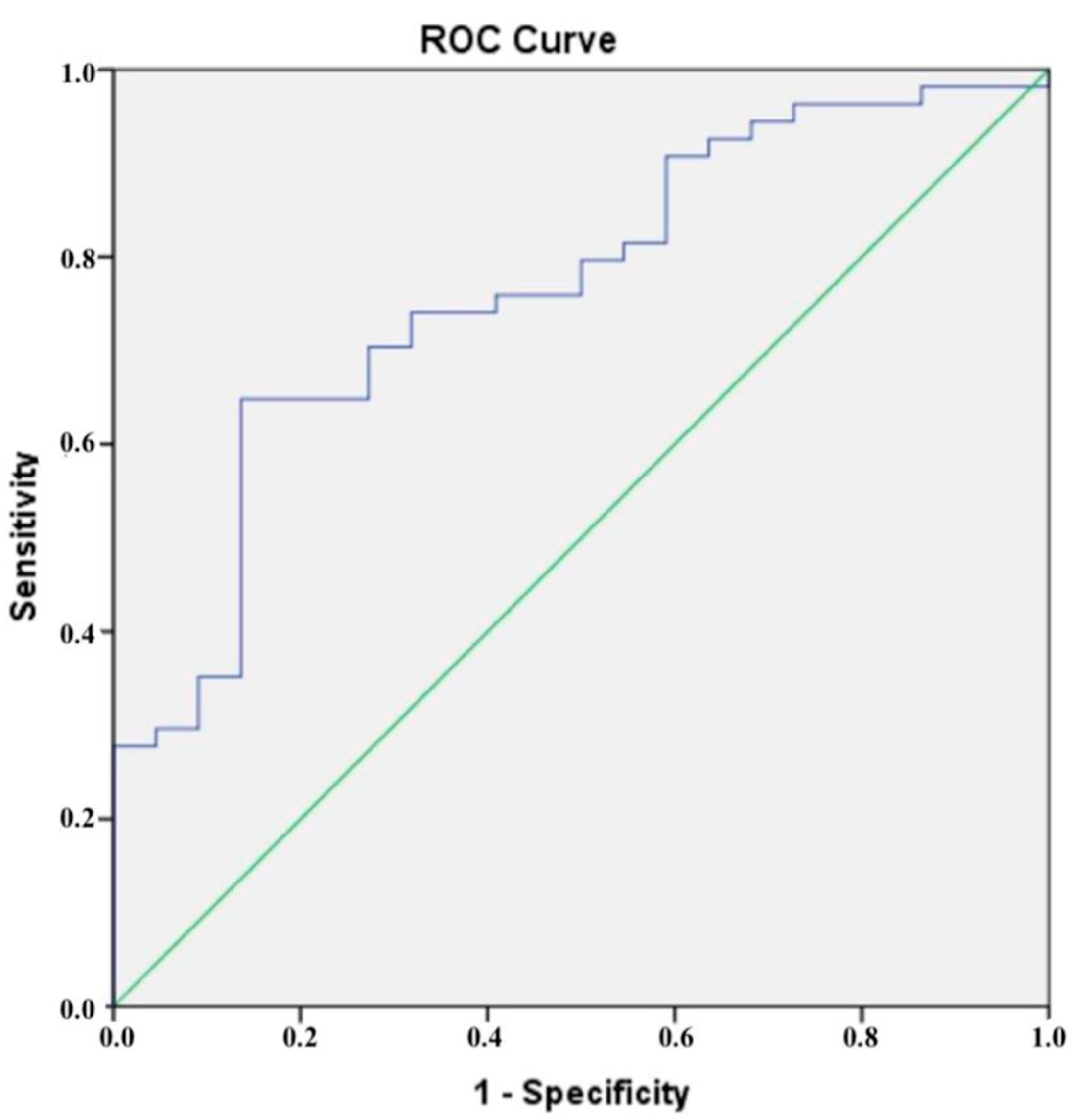
Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef] [PubMed]
- Hartley, A.; Marshall, D.C.; Salciccioli, J.D.; Sikkel, M.B.; Maruthappu, M.; Shalhoub, J. Trends in Mortality From Ischemic Heart Disease and Cerebrovascular Disease in Europe: 1980 to 2009. Circulation 2016, 133, 1916–1926. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2021 Update: A Report from the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [PubMed]
- Dimitriadis, K.; Pyrpyris, N.; Theofilis, P.; Mantzouranis, E.; Beneki, E.; Kostakis, P.; Koutsopoulos, G.; Aznaouridis, K.; Aggeli, K.; Tsioufis, K. Computed Tomography Angiography Identified High-Risk Coronary Plaques: From Diagnosis to Prognosis and Future Management. Diagnostics 2024, 14, 1671. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef]
- Attiq, A.; Afzal, S.; Ahmad, W.; Kandeel, M. Hegemony of inflammation in atherosclerosis and coronary artery disease. Eur. J. Pharmacol. 2024, 966, 176338. [Google Scholar] [CrossRef]
- Okan, T.; Topaloglu, C. Association of ratios of monocyte/high-density lipoprotein cholesterol and neutrophil/high-density lipoprotein cholesterol with atherosclerotic plaque type on coronary computed tomography. Cardiovasc. J. Afr. 2024, 34, 1–6. [Google Scholar]
- Okan, T.; Doruk, M.; Ozturk, A.; Topaloglu, C.; Dogdus, M.; Yilmaz, M.B. Evaluation of Plasma Atherogenic Index, Triglyceride-Glucose Index and Other Lipid Ratios as Predictive Biomarkers of Coronary Artery Disease in Different Age Groups. Diagnostics 2024, 14, 1495. [Google Scholar] [CrossRef]
- Striukova, E.V.; Shramko, V.S.; Kashtanova, E.V.; Polonskaya, Y.V.; Stakhneva, E.M.; Kurguzov, A.V.; Chernyavsky, A.M.; Ragino, Y.I. Adipokine Levels in Men with Coronary Atherosclerosis on the Background of Abdominal Obesity. J. Pers. Med. 2022, 12, 1248. [Google Scholar] [CrossRef]
- Kraaijenhof, J.M.; Mol, B.M.; Nurmohamed, N.S.; Dzobo, K.E.; Kroon, J.; Hovingh, G.K.; Mokry, M.; de Borst, G.J.; Stroes, E.S.G.; de Kleijn, D.P.V. Plasma C-reactive protein is associated with a pro-inflammatory and adverse plaque phenotype. Atherosclerosis 2024, 396, 118532. [Google Scholar] [CrossRef]
- Lu, Z.; Jiang, Z.; Tang, J.; Lin, C.P.; Zhang, H. Functions and origins of cardiac fat. FEBS J. 2023, 290, 1705–1718. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zhang, S.; Li, Z. Adipokines in glucose and lipid metabolism. Adipocyte 2023, 12, 2202976. [Google Scholar] [CrossRef] [PubMed]
- Fan, W.; Si, Y.; Xing, E.; Feng, Z.; Ding, Z.; Liu, Y.; Wei, C.; Tian, Y.; Zhang, Y.; Liu, J.; et al. Human epicardial adipose tissue inflammation correlates with coronary artery disease. Cytokine 2023, 162, 156119. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G. Epicardial adipose tissue in contemporary cardiology. Nat. Rev. Cardiol. 2022, 19, 593–606. [Google Scholar] [CrossRef] [PubMed]
- Ntaios, G.; Gatselis, N.K.; Makaritsis, K.; Dalekos, G.N. Adipokines as mediators of endothelial function and atherosclerosis. Atherosclerosis 2013, 227, 216–221. [Google Scholar] [CrossRef]
- Si, Y.; Fan, W.; Sun, L. A Review of the Relationship Between CTRP Family and Coronary Artery Disease. Curr. Atheroscler. Rep. 2020, 22, 22. [Google Scholar] [CrossRef]
- Li, C.; Chen, J.W.; Liu, Z.H.; Shen, Y.; Ding, F.H.; Gu, G.; Liu, J.; Qiu, J.P.; Gao, J.; Zhang, R.Y.; et al. CTRP5 promotes transcytosis and oxidative modification of low-density lipoprotein and the development of atherosclerosis. Atherosclerosis 2018, 278, 197–209. [Google Scholar] [CrossRef]
- Moradi, N.; Fadaei, R.; Rashidbeygi, E.; Bagheri Kargasheh, F.; Malek, M.; Shokoohi Nahrkhalaji, A.; Fallah, S. Evaluation of changing the pattern of CTRP5 and inflammatory markers levels in patients with coronary artery disease and type 2 diabetes mellitus. Arch. Physiol. Biochem. 2022, 128, 964–969. [Google Scholar] [CrossRef]
- Macvanin, M.T.; Rizzo, M.; Radovanovic, J.; Sonmez, A.; Paneni, F.; Isenovic, E.R. Role of Chemerin in Cardiovascular Diseases. Biomedicines 2022, 10, 2970. [Google Scholar] [CrossRef]
- Yan, Q.; Zhang, Y.; Hong, J.; Gu, W.; Dai, M.; Shi, J.; Zhai, Y.; Wang, W.; Li, X.; Ning, G. The association of serum chemerin level with risk of coronary artery disease in Chinese adults. Endocrine 2012, 41, 281–288. [Google Scholar] [CrossRef]
- Dong, B.; Ji, W.; Zhang, Y. Elevated serum chemerin levels are associated with the presence of coronary artery disease in patients with metabolic syndrome. Intern. Med. 2011, 50, 1093–1097. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Kou, W.; Ji, S.; Shen, R.; Ji, H.; Zhuang, J.; Zhao, Y.; Li, B.; Peng, W.; Yu, X.; et al. Prognostic value of plasma adipokine chemerin in patients with coronary artery disease. Front. Cardiovasc. Med. 2022, 9, 968349. [Google Scholar] [CrossRef] [PubMed]
- Spiroglou, S.G.; Kostopoulos, C.G.; Varakis, J.N.; Papadaki, H.H. Adipokines in periaortic and epicardial adipose tissue: Differential expression and relation to atherosclerosis. J. Atheroscler. Thromb. 2010, 17, 115–130. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H.J.; Choi, H.Y.; Yang, S.J.; Kim, H.Y.; Seo, J.A.; Kim, S.G.; Kim, N.H.; Choi, K.M.; Choi, D.S.; Baik, S.H. Circulating chemerin level is independently correlated with arterial stiffness. J. Atheroscler. Thromb. 2012, 19, 59–66. [Google Scholar] [CrossRef]
- Rampidis, G.; Rafailidis, V.; Kouskouras, K.; Davidhi, A.; Papachristodoulou, A.; Samaras, A.; Giannakoulas, G.; Ziakas, A.; Prassopoulos, P.; Karvounis, H. Relationship between Coronary Arterial Geometry and the Presence and Extend of Atherosclerotic Plaque Burden: A Review Discussing Methodology and Findings in the Era of Cardiac Computed Tomography Angiography. Diagnostics 2022, 12, 2178. [Google Scholar] [CrossRef]
- Nakazato, R.; Shalev, A.; Doh, J.H.; Koo, B.K.; Gransar, H.; Gomez, M.J.; Leipsic, J.; Park, H.B.; Berman, D.S.; Min, J.K. Aggregate plaque volume by coronary computed tomography angiography is superior and incremental to luminal narrowing for diagnosis of ischemic lesions of intermediate stenosis severity. J. Am. Coll. Cardiol. 2013, 62, 460–467. [Google Scholar] [CrossRef]
- Mitsis, A.; Khattab, E.; Christodoulou, E.; Myrianthopoulos, K.; Myrianthefs, M.; Tzikas, S.; Ziakas, A.; Fragakis, N.; Kassimis, G. From Cells to Plaques: The Molecular Pathways of Coronary Artery Calcification and Disease. J. Clin. Med. 2024, 13, 6352. [Google Scholar] [CrossRef]
- Sangiorgi, G.; Rumberger, J.A.; Severson, A.; Edwards, W.D.; Gregoire, J.; Fitzpatrick, L.A.; Schwartz, R.S. Arterial calcification and not lumen stenosis is highly correlated with atherosclerotic plaque burden in humans: A histologic study of 723 coronary artery segments using nondecalcifying methodology. J. Am. Coll. Cardiol. 1998, 31, 126–133. [Google Scholar] [CrossRef]
- Alexopoulos, N.; Raggi, P. Calcification in atherosclerosis. Nat. Rev. Cardiol. 2009, 6, 681–688. [Google Scholar] [CrossRef]
- Ross, R. Atherosclerosis—An inflammatory disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef]
- Shen, Y.; Li, C.; Zhang, R.Y.; Zhang, Q.; Shen, W.F.; Ding, F.H.; Lu, L. Association of increased serum CTRP5 levels with in-stent restenosis after coronary drug-eluting stent implantation: CTRP5 promoting inflammation, migration and proliferation in vascular smooth muscle cells. Int. J. Cardiol. 2017, 228, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Zhou, Y.; Nabavi, S.M.; Sahebkar, A.; Little, P.J.; Xu, S.; Weng, J.; Ge, J. Mechanisms of Oxidized LDL-Mediated Endothelial Dysfunction and Its Consequences for the Development of Atherosclerosis. Front. Cardiovasc. Med. 2022, 9, 925923. [Google Scholar] [CrossRef] [PubMed]
- Blagov, A.V.; Markin, A.M.; Bogatyreva, A.I.; Tolstik, T.V.; Sukhorukov, V.N.; Orekhov, A.N. The Role of Macrophages in the Pathogenesis of Atherosclerosis. Cells 2023, 12, 522. [Google Scholar] [CrossRef] [PubMed]
- Dimitriadis, G.K.; Kaur, J.; Adya, R.; Miras, A.D.; Mattu, H.S.; Hattersley, J.G.; Kaltsas, G.; Tan, B.K.; Randeva, H.S. Chemerin induces endothelial cell inflammation: Activation of nuclear factor-kappa beta and monocyte-endothelial adhesion. Oncotarget 2018, 9, 16678–16690. [Google Scholar] [CrossRef]
- Liu, Y.; Wei, C.; Ding, Z.; Xing, E.; Zhao, Z.; Shi, F.; Tian, Y.; Zhang, Y.; Fan, W.; Sun, L. Role of serum C1q/TNF-related protein family levels in patients with acute coronary syndrome. Front. Cardiovasc. Med. 2022, 9, 967918. [Google Scholar] [CrossRef]
- Mitsis, A.; Khattab, E.; Myrianthefs, M.; Tzikas, S.; Kadoglou, N.P.E.; Fragakis, N.; Ziakas, A.; Kassimis, G. Chemerin in the Spotlight: Revealing Its Multifaceted Role in Acute Myocardial Infarction. Biomedicines 2024, 12, 2133. [Google Scholar] [CrossRef]
- Kostopoulos, C.G.; Spiroglou, S.G.; Varakis, J.N.; Apostolakis, E.; Papadaki, H.H. Chemerin and CMKLR1 expression in human arteries and periadventitial fat: A possible role for local chemerin in atherosclerosis? BMC Cardiovasc. Disord. 2014, 14, 56. [Google Scholar] [CrossRef]
- Watts, S.W.; Dorrance, A.M.; Penfold, M.E.; Rourke, J.L.; Sinal, C.J.; Seitz, B.; Sullivan, T.J.; Charvat, T.T.; Thompson, J.M.; Burnett, R.; et al. Chemerin connects fat to arterial contraction. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 1320–1328. [Google Scholar] [CrossRef]
- Neves, K.B.; Lobato, N.S.; Lopes, R.A.; Filgueira, F.P.; Zanotto, C.Z.; Oliveira, A.M.; Tostes, R.C. Chemerin reduces vascular nitric oxide/cGMP signalling in rat aorta: A link to vascular dysfunction in obesity? Clin. Sci. 2014, 127, 111–122. [Google Scholar] [CrossRef]
- Bozaoglu, K.; Curran, J.E.; Stocker, C.J.; Zaibi, M.S.; Segal, D.; Konstantopoulos, N.; Morrison, S.; Carless, M.; Dyer, T.D.; Cole, S.A.; et al. Chemerin, a novel adipokine in the regulation of angiogenesis. J. Clin. Endocrinol. Metab. 2010, 95, 2476–2485. [Google Scholar] [CrossRef]
- Kaur, J.; Mattu, H.S.; Chatha, K.; Randeva, H.S. Chemerin in human cardiovascular disease. Vascul Pharmacol. 2018, 110, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Ismaiel, A.; Ashfaq, M.Z.; Leucuta, D.C.; Ismaiel, M.; Ensar Ismaiel, D.; Popa, S.L.; Dumitrascu, D.L. Chemerin Levels in Acute Coronary Syndrome: Systematic Review and Meta-Analysis. Lab Med. 2022, 53, 552–560. [Google Scholar] [CrossRef] [PubMed]
- Xiaotao, L.; Xiaoxia, Z.; Yue, X.; Liye, W. Serum chemerin levels are associated with the presence and extent of coronary artery disease. Coron. Artery Dis. 2012, 23, 412–416. [Google Scholar] [CrossRef] [PubMed]
- Aksan, G.; İnci, S.; Nar, G.; Soylu, K.; Gedikli, Ö.; Yüksel, S.; Özdemir, M.; Nar, R.; Meriç, M.; Şahin, M. Association of serum chemerin levels with the severity of coronary artery disease in patients with metabolic syndrome. Int. J. Clin. Exp. Med. 2014, 7, 5461–5468. [Google Scholar] [PubMed]
- Mortensen, M.B.; Dzaye, O.; Steffensen, F.H.; Bøtker, H.E.; Jensen, J.M.; Rønnow Sand, N.P.; Kragholm, K.H.; Sørensen, H.T.; Leipsic, J.; Mæng, M.; et al. Impact of Plaque Burden Versus Stenosis on Ischemic Events in Patients With Coronary Atherosclerosis. J. Am. Coll. Cardiol. 2020, 76, 2803–2813. [Google Scholar] [CrossRef]
- Szpakowicz, A.; Kaminski, K.A.; Szpakowicz, M.; Lapinska, M.; Paniczko, M.; Lawicki, S.; Glazewska, K.; Raczkowski, A.; Kondraciuk, M.; Sawicka, E.; et al. Chemerin in coronary artery disease patients. Eur. Heart J. 2020, 41, ehaa946–ehaa1263. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | CCTA-Confirmed Non-CAD Group n = 35 | CCTA-Confirmed CAD Group n = 54 | p |
|---|---|---|---|
| Age (years) | 58.9 ± 7.7 | 56.7 ± 7.2 | 0.231 |
| Gender (female %) | 40 | 38.9 | 0.861 |
| Smoking % | 34 | 37 | 0.756 |
| DM % | 20 | 22.2 | 0.843 |
| HT % | 28.6 | 31.4 | 0.703 |
| BMI (kg/m2) | 28.1 ± 3.4 | 27.6 ± 3.1 | 0.535 |
| Metabolic Syndrome % | 25.7 | 27.7 | 0.756 |
| Agatston score | 0 | 224.0 ± 342.3 | <0.001 |
| Systolic Blood Pressure (mmHg) | 135 ± 13 | 132 ± 25 | 0.623 |
| Diastolic Blood Pressure (mmHg) | 80 ± 10 | 79 ± 12 | 0.938 |
| Fasting Blood Glucose (mg/dL) | 100.9 ± 42.7 | 107.1 ± 35.0 | 0.514 |
| Total Cholesterol (mg/dL) | 225.7 ± 53.4 | 223.3 ± 52.3 | 0.858 |
| Triglyceride (mg/dL) | 153.4 ± 72.5 | 192.0 ± 116.0 | 0.083 |
| LDL Cholesterol (mg/dL) | 149.3 ± 38.1 | 140.0 ± 48.5 | 0.417 |
| HDL Cholesterol (mg/dL) | 50.0 ± 10.6 | 48.5 ± 11.9 | 0.592 |
| Creatinine (mg/dL) | 0.91 ± 0.04 | 0.93 ± 0.03 | 0.875 |
| CTRP5 (ng/mL) | 149.4 ± 51.0 | 221.8 ± 103.8 | 0.003 |
| Chemerin (ng/mL) | 86.1 ± 19.5 | 105.0 ± 35.6 | 0.005 |
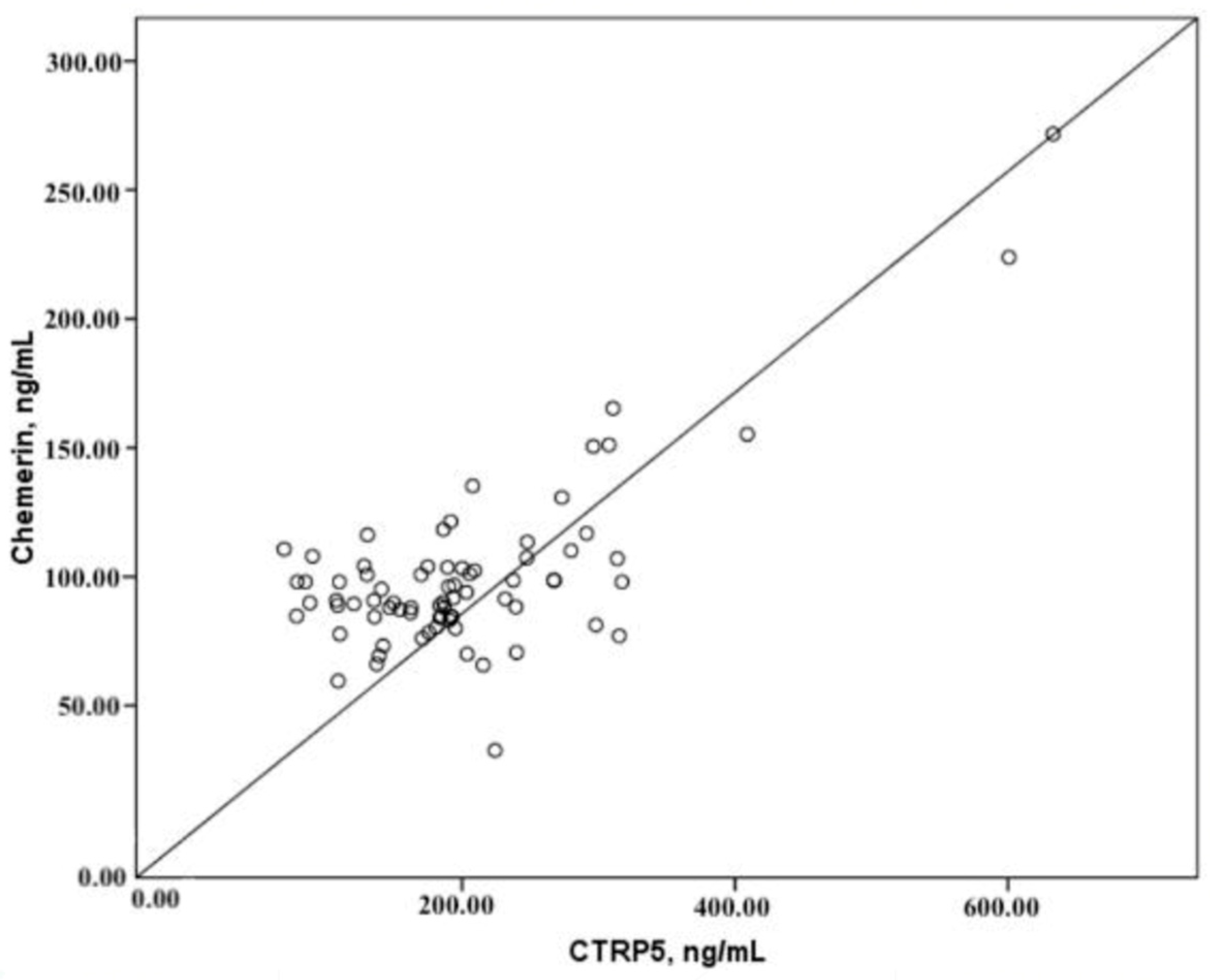
| Chemerin | CTRP5 | Agatson | ||
|---|---|---|---|---|
| Chemerin | r | 0.725 * | 0.059 | |
| p | 0.000 | 0.613 | ||
| CTRP5 | r | 0.725 * | 0.061 | |
| p | 0.000 | 0.601 | ||
| Agatson | r | 0.059 | 0.061 | |
| p | 0.613 | 0.601 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okan, T.; Altın, C.; Topaloglu, C.; Doruk, M.; Yılmaz, M.B. Diagnostic Potential of CTRP5 and Chemerin for Coronary Artery Disease: A Study by Coronary Computed Tomography Angiography. Diagnostics 2025, 15, 206. https://doi.org/10.3390/diagnostics15020206
Okan T, Altın C, Topaloglu C, Doruk M, Yılmaz MB. Diagnostic Potential of CTRP5 and Chemerin for Coronary Artery Disease: A Study by Coronary Computed Tomography Angiography. Diagnostics. 2025; 15(2):206. https://doi.org/10.3390/diagnostics15020206
Chicago/Turabian StyleOkan, Taha, Cihan Altın, Caner Topaloglu, Mehmet Doruk, and Mehmet Birhan Yılmaz. 2025. "Diagnostic Potential of CTRP5 and Chemerin for Coronary Artery Disease: A Study by Coronary Computed Tomography Angiography" Diagnostics 15, no. 2: 206. https://doi.org/10.3390/diagnostics15020206
APA StyleOkan, T., Altın, C., Topaloglu, C., Doruk, M., & Yılmaz, M. B. (2025). Diagnostic Potential of CTRP5 and Chemerin for Coronary Artery Disease: A Study by Coronary Computed Tomography Angiography. Diagnostics, 15(2), 206. https://doi.org/10.3390/diagnostics15020206