Figure 1.
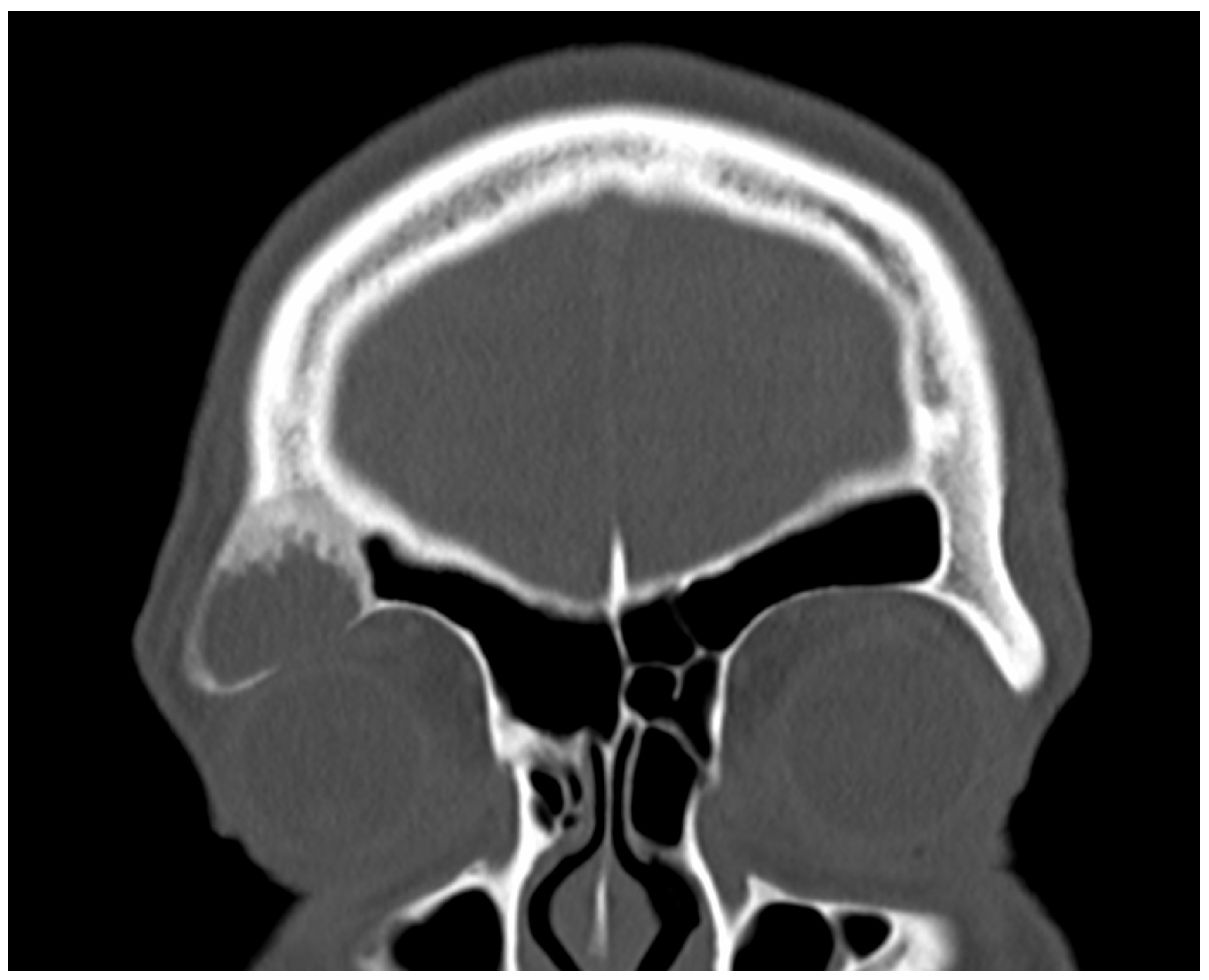
A 38-year-old male presented to the emergency outpatient clinic with sudden-onset headache, nausea, and general discomfort. Neurological and otorhinolaryngological examinations and laboratory analyses revealed no abnormalities. Cranial CT did not indicate any neurovascular events but incidentally detected a cystic, osteodestructive lesion measuring 2.5 cm in diameter in the right frontal sinus. Based on its location, characteristics, and the patient’s history of recurrent frontal headaches and retrobulbar pressure, a mucocele was initially suspected. As the patient’s acute complaints resolved on symptomatic therapy quickly, we decided on elective surgery to drain the plausible mucocele. Due to the lesion’s far lateral position, an endonasal approach was impractical, leading to a supraorbital external approach. A right-sided frontal bone window was created using a piezo device. During the removal of the frontal bone cap, yellowish turbid fluid was discharged from the frontal sinus. The fluid was totally aspirated, and the suspicious mucosa was completely excised and sent for histological analysis. The bony floor of the frontal sinus was found to be thinned and partially eroded, exposing the underlying periorbita, which appeared intact and healthy. The clinical appearance during surgery reinforced the mucocele diagnosis. Subsequently, the bone cap was repositioned, and the external wound was securely closed. The surgery proceeded without any intra- or postoperative complications. Fibrous histiocytoma, or dermatofibroma, is one of the most common cutaneous soft tissue lesions [
1]. However, it hardly ever occurs in the skeleton. Its incidence among surgically treated benign skeletal lesions is approximately 1% [
2]. The occurrence of benign fibrous histiocytoma in the skull is rarely described in the literature. To our knowledge, this present case is the first confirmed benign fibrous histiocytoma in the frontal sinus. Only one was reported earlier in this location; however, this was a malignant tumor [
3]. The first ever reported benign fibrous histiocytoma in the paranasal sinuses was described by Townsend et al. in 1973 [
4]. Considering the extremely rare localization and the potential for malignization, the case was presented to the interdisciplinary TUMOR-Board. Since R0 resection is neither clinically nor histologically confirmed and the risk involved in revision surgery is high, close monitoring was chosen, in view of the approximately 11% recurrence rate reported by Bielamowitz et al. [
5]. The patient has remained symptom-free without evidence of recurrence, as confirmed by clinical and imaging assessments.
Figure 1.
A 38-year-old male presented to the emergency outpatient clinic with sudden-onset headache, nausea, and general discomfort. Neurological and otorhinolaryngological examinations and laboratory analyses revealed no abnormalities. Cranial CT did not indicate any neurovascular events but incidentally detected a cystic, osteodestructive lesion measuring 2.5 cm in diameter in the right frontal sinus. Based on its location, characteristics, and the patient’s history of recurrent frontal headaches and retrobulbar pressure, a mucocele was initially suspected. As the patient’s acute complaints resolved on symptomatic therapy quickly, we decided on elective surgery to drain the plausible mucocele. Due to the lesion’s far lateral position, an endonasal approach was impractical, leading to a supraorbital external approach. A right-sided frontal bone window was created using a piezo device. During the removal of the frontal bone cap, yellowish turbid fluid was discharged from the frontal sinus. The fluid was totally aspirated, and the suspicious mucosa was completely excised and sent for histological analysis. The bony floor of the frontal sinus was found to be thinned and partially eroded, exposing the underlying periorbita, which appeared intact and healthy. The clinical appearance during surgery reinforced the mucocele diagnosis. Subsequently, the bone cap was repositioned, and the external wound was securely closed. The surgery proceeded without any intra- or postoperative complications. Fibrous histiocytoma, or dermatofibroma, is one of the most common cutaneous soft tissue lesions [
1]. However, it hardly ever occurs in the skeleton. Its incidence among surgically treated benign skeletal lesions is approximately 1% [
2]. The occurrence of benign fibrous histiocytoma in the skull is rarely described in the literature. To our knowledge, this present case is the first confirmed benign fibrous histiocytoma in the frontal sinus. Only one was reported earlier in this location; however, this was a malignant tumor [
3]. The first ever reported benign fibrous histiocytoma in the paranasal sinuses was described by Townsend et al. in 1973 [
4]. Considering the extremely rare localization and the potential for malignization, the case was presented to the interdisciplinary TUMOR-Board. Since R0 resection is neither clinically nor histologically confirmed and the risk involved in revision surgery is high, close monitoring was chosen, in view of the approximately 11% recurrence rate reported by Bielamowitz et al. [
5]. The patient has remained symptom-free without evidence of recurrence, as confirmed by clinical and imaging assessments.
![Diagnostics 15 00056 g001]()
Figure 2.
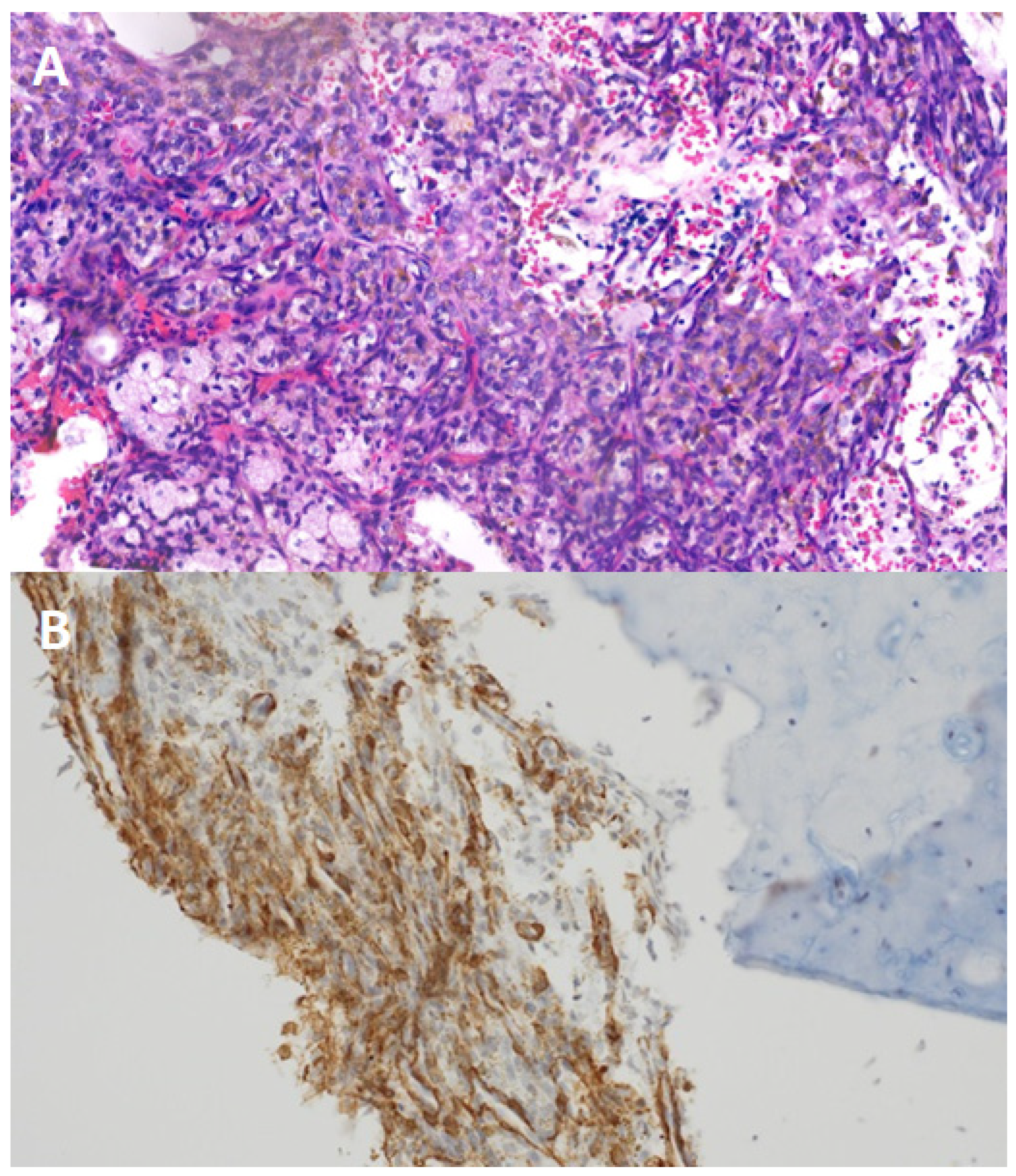
Panel (A): histological analysis of the excised lesion revealed histiocytes, siderophages, cholesterol crystals, and spindle cell proliferation without malignancy markers. Panel (B): immunohistochemical tests showed EMA, S100, and creatinine negativity but SMA positivity, confirming a benign fibrous histiocytoma.
Figure 2.
Panel (A): histological analysis of the excised lesion revealed histiocytes, siderophages, cholesterol crystals, and spindle cell proliferation without malignancy markers. Panel (B): immunohistochemical tests showed EMA, S100, and creatinine negativity but SMA positivity, confirming a benign fibrous histiocytoma.


 ,
, 
{kind=link}
{kind=link}