
A Histological Evaluation of the Efficiency of Using Periprosthetic Autologous Fat to Prevent Capsular Contracture Compared to Other Known Methods—An Experimental Study

 , , , ,
, , , , 
Abstract
1. Introduction
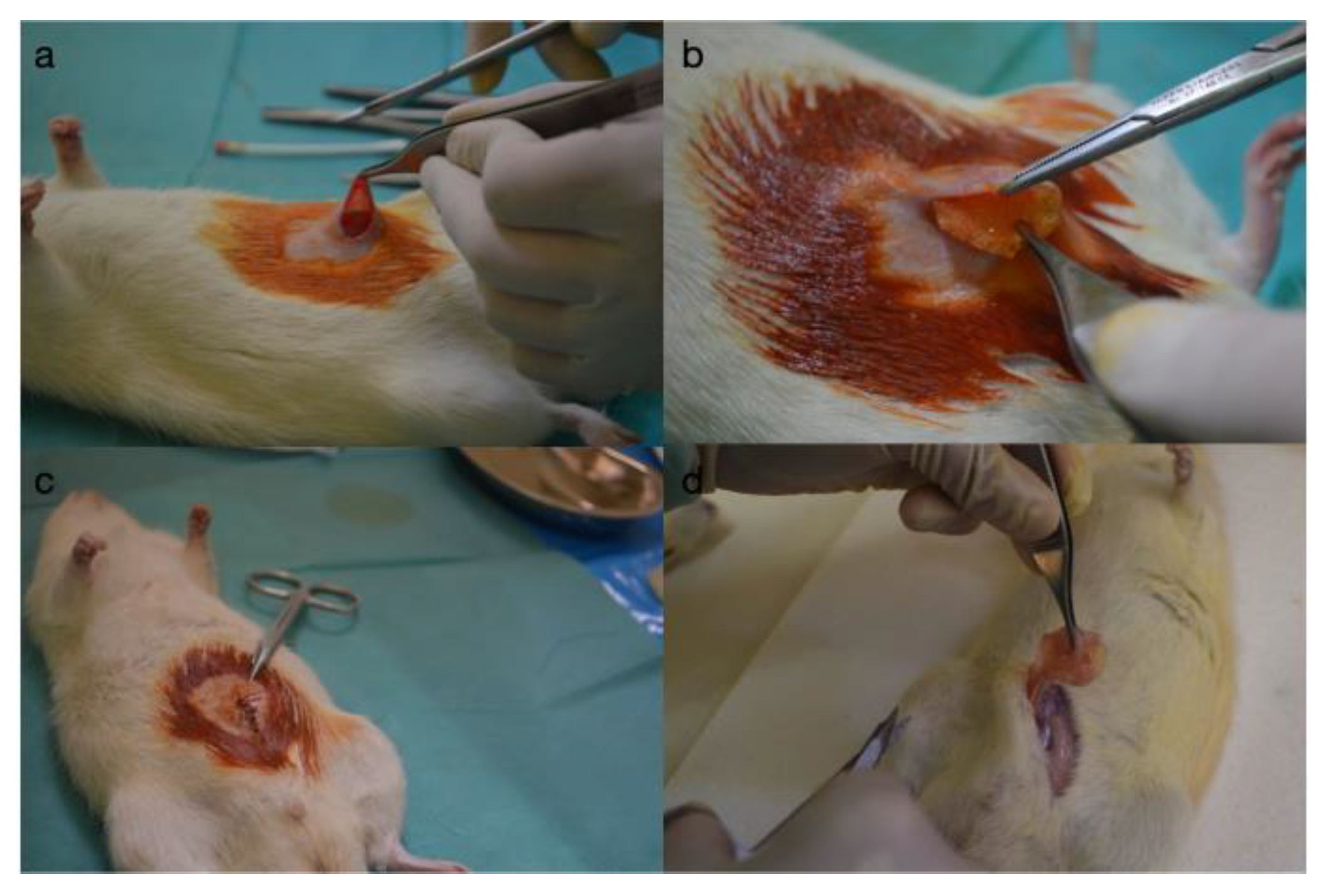
2. Materials and Methods
Statistical Analysis
3. Results
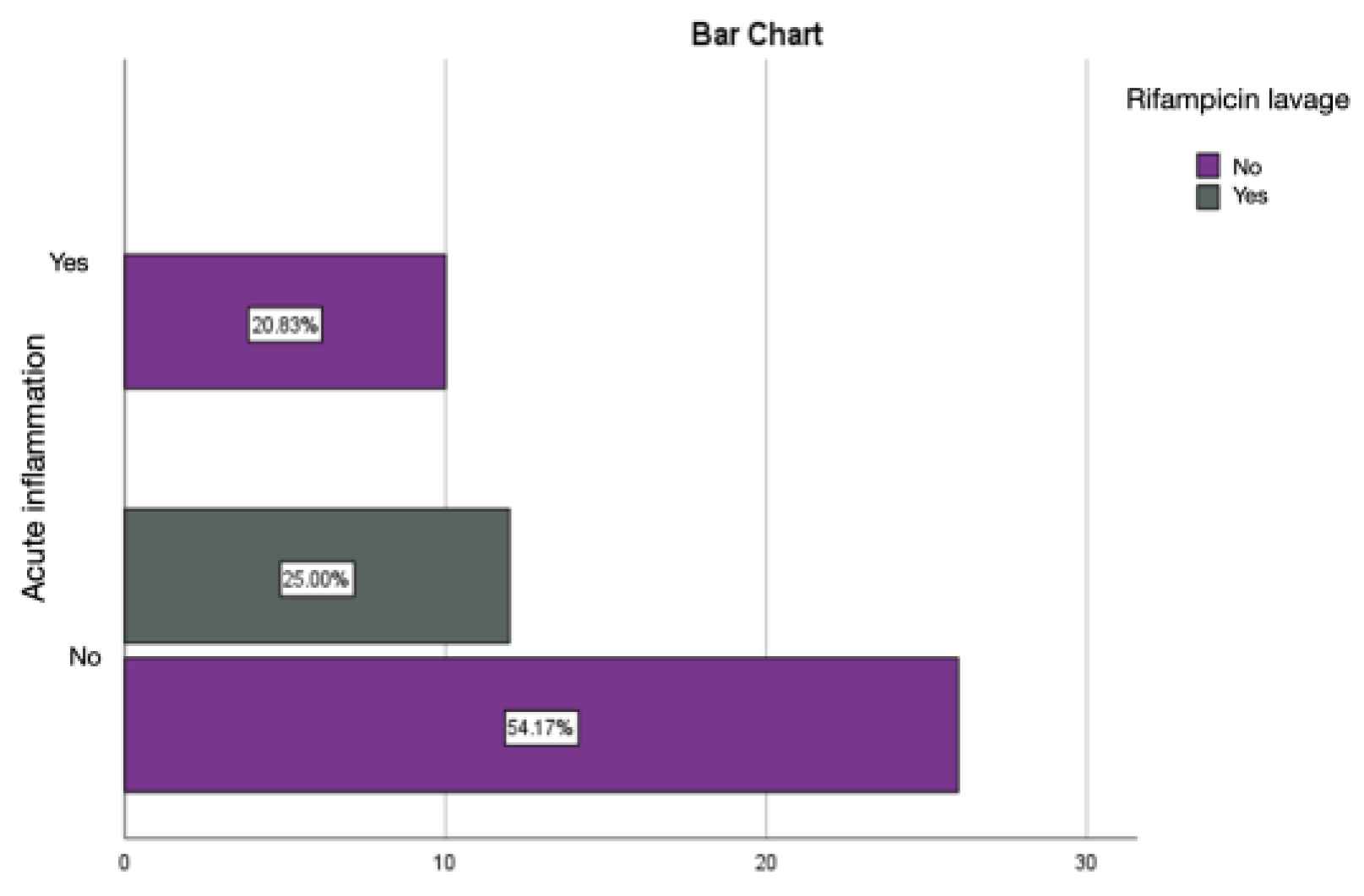
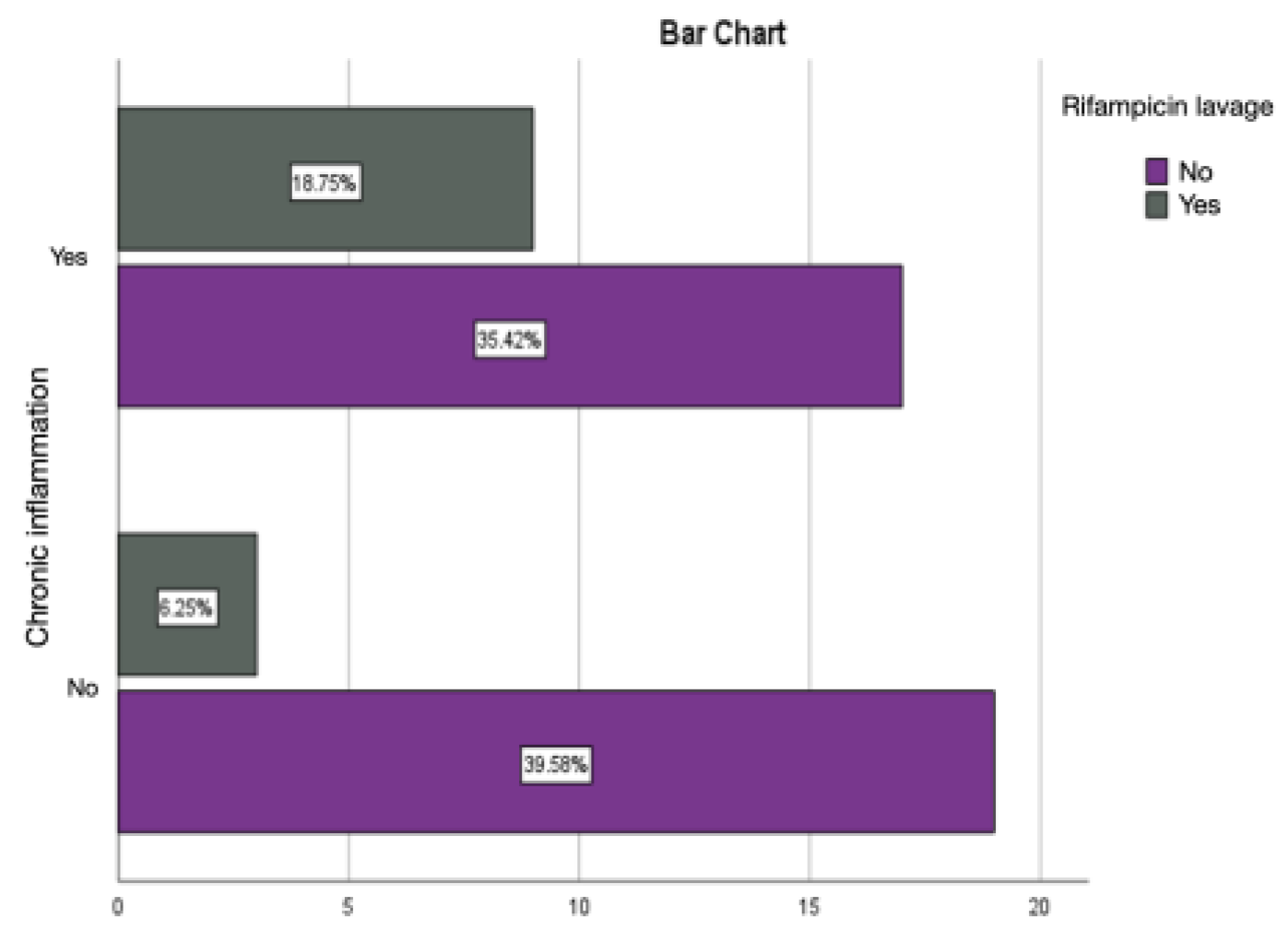
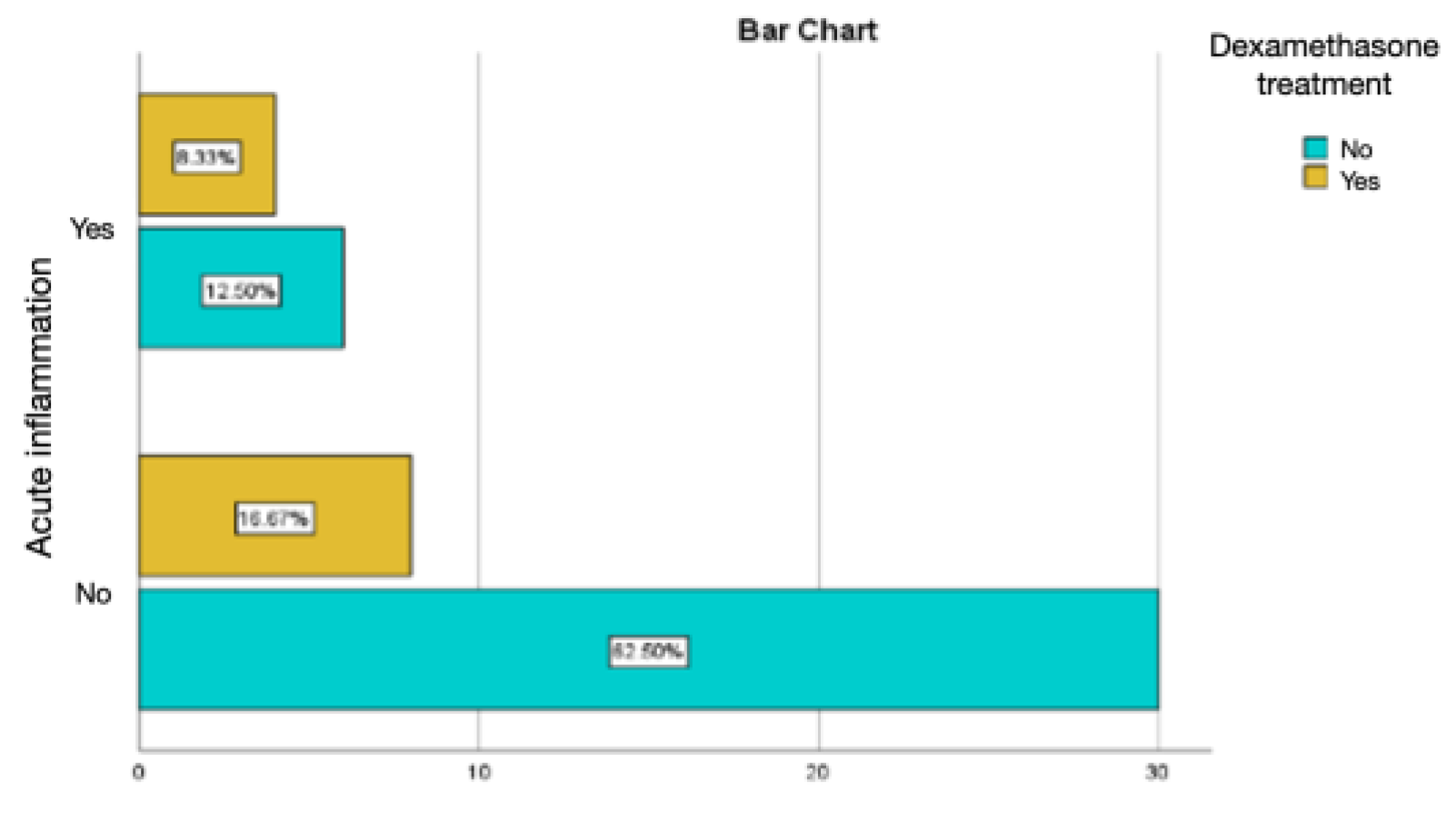
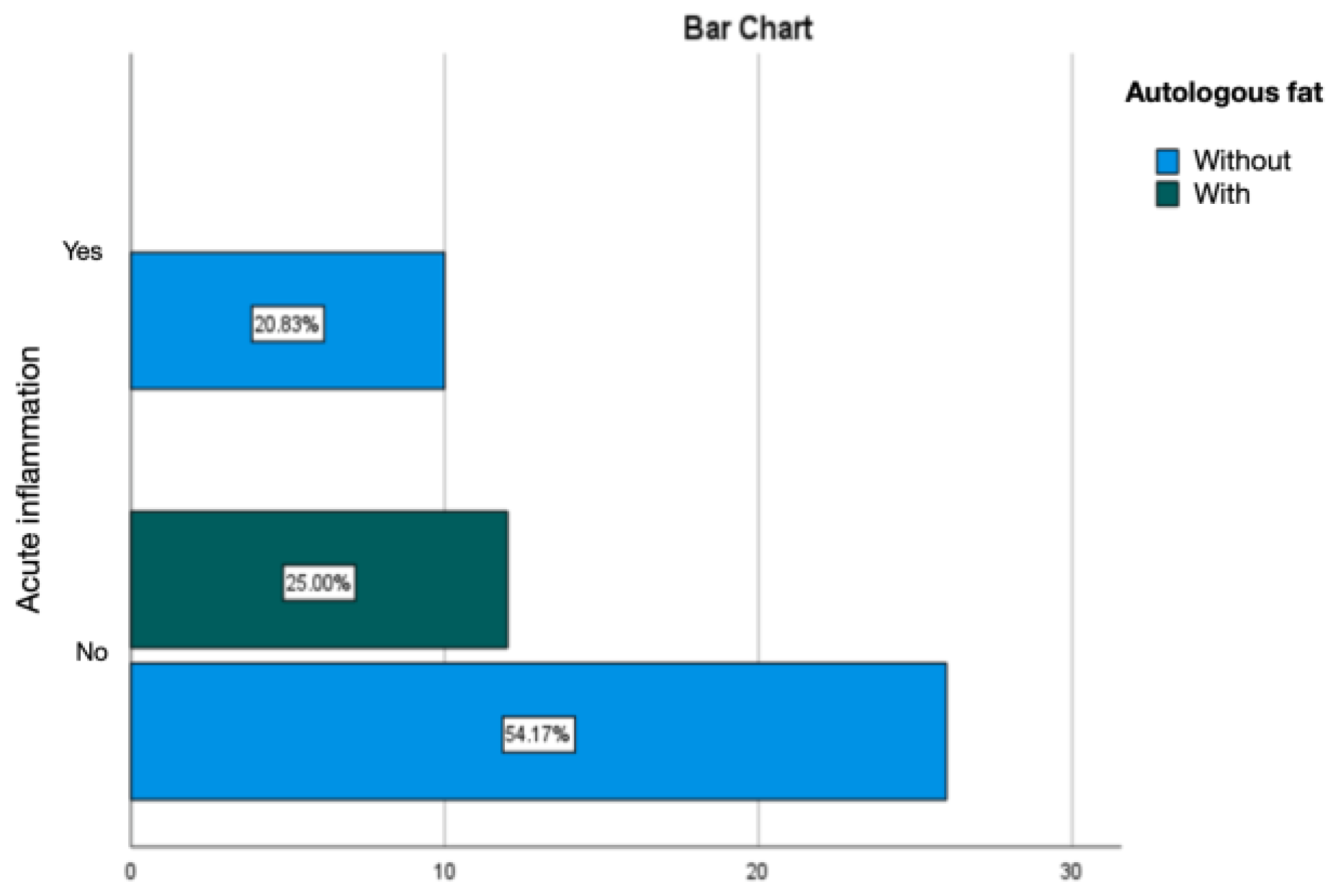
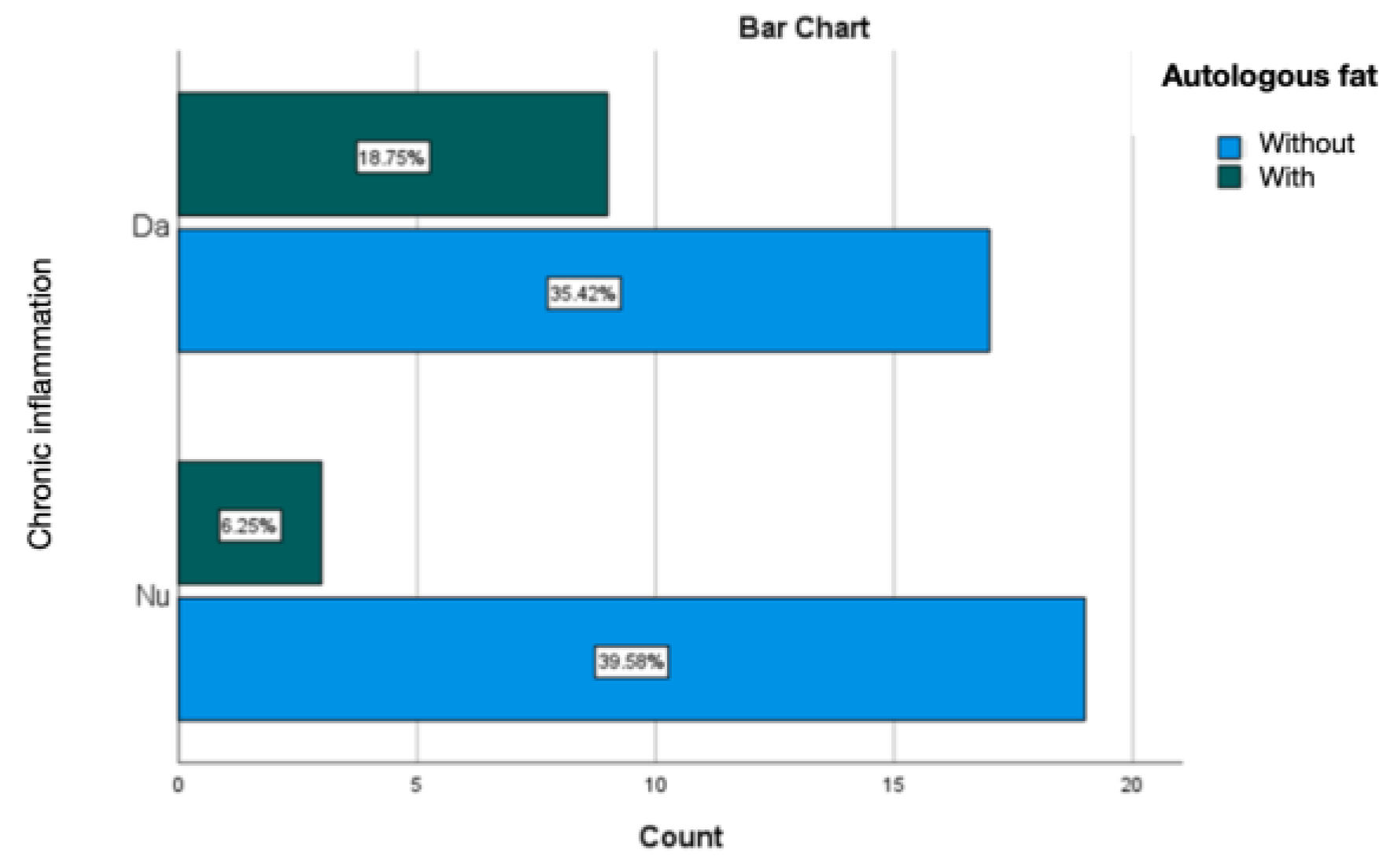
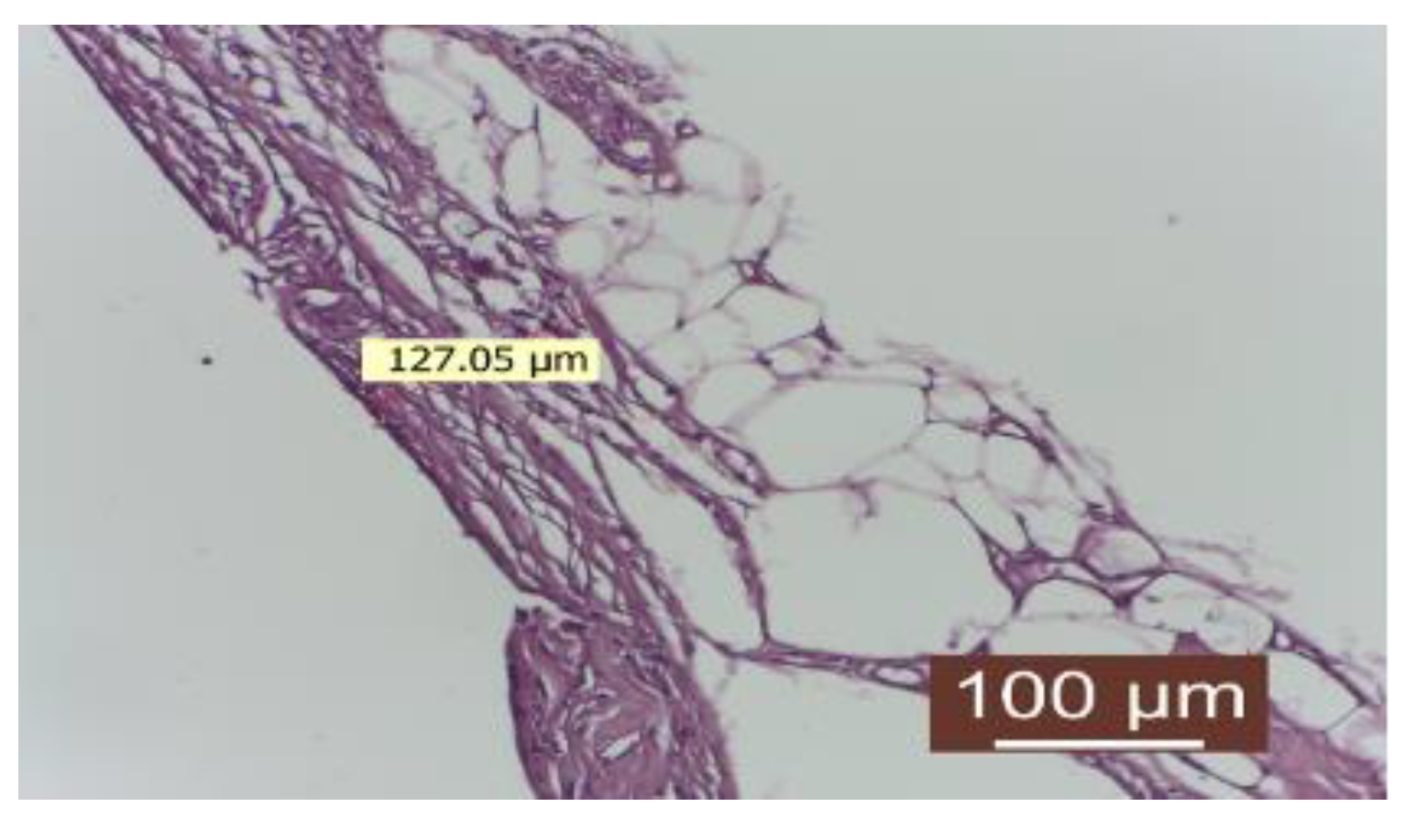
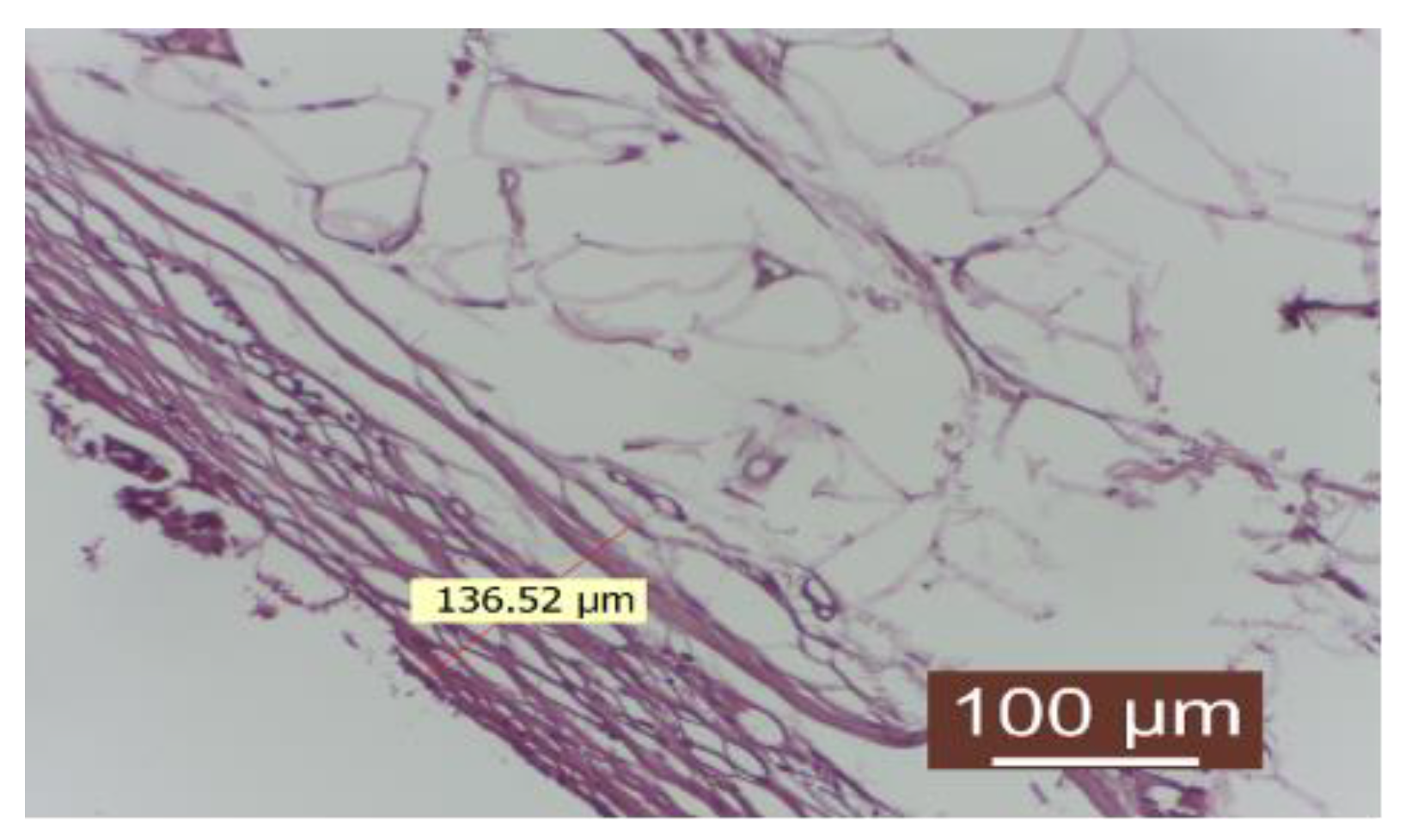
3.1. Analysis of Periprosthetic Inflammation
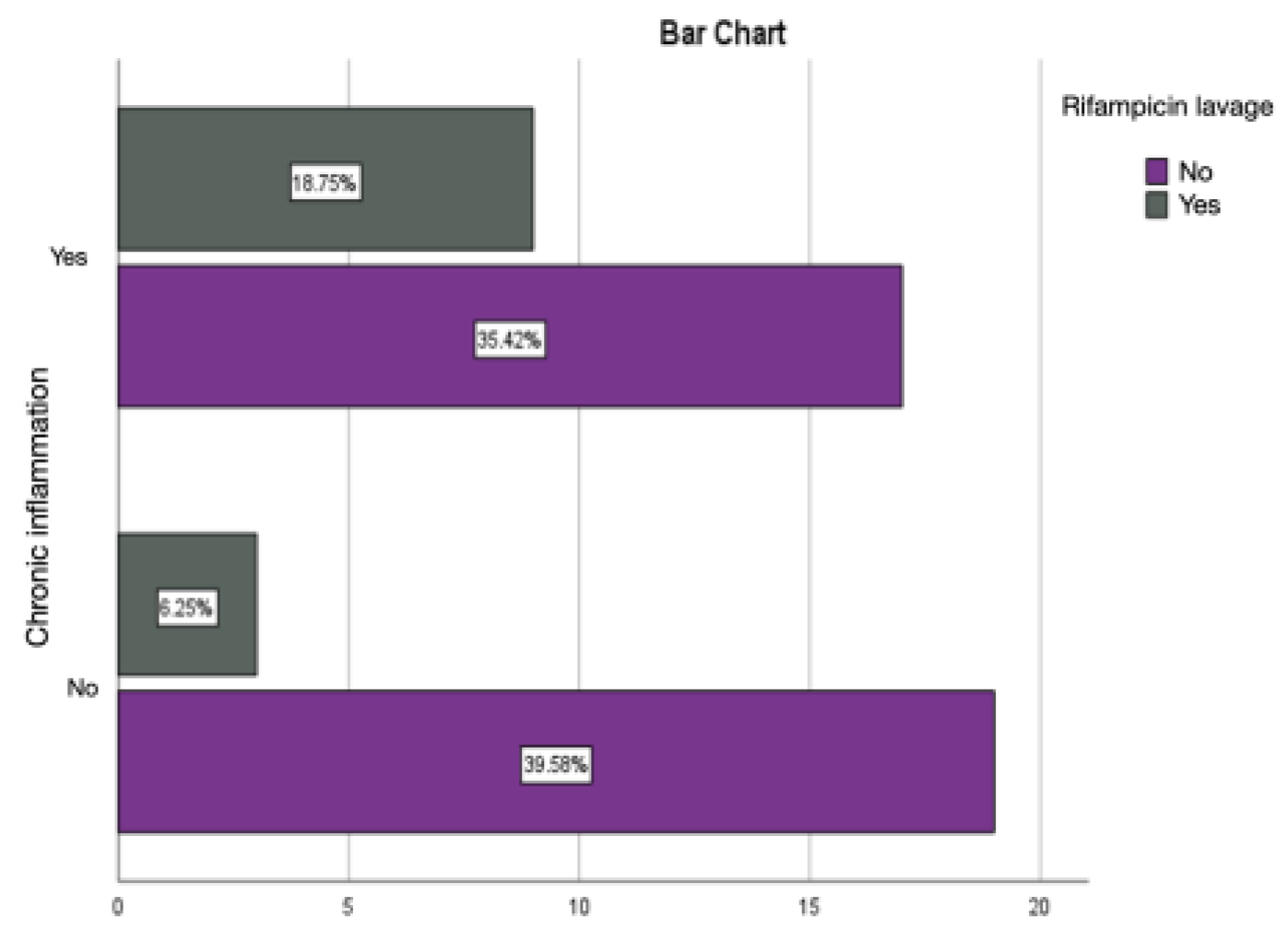
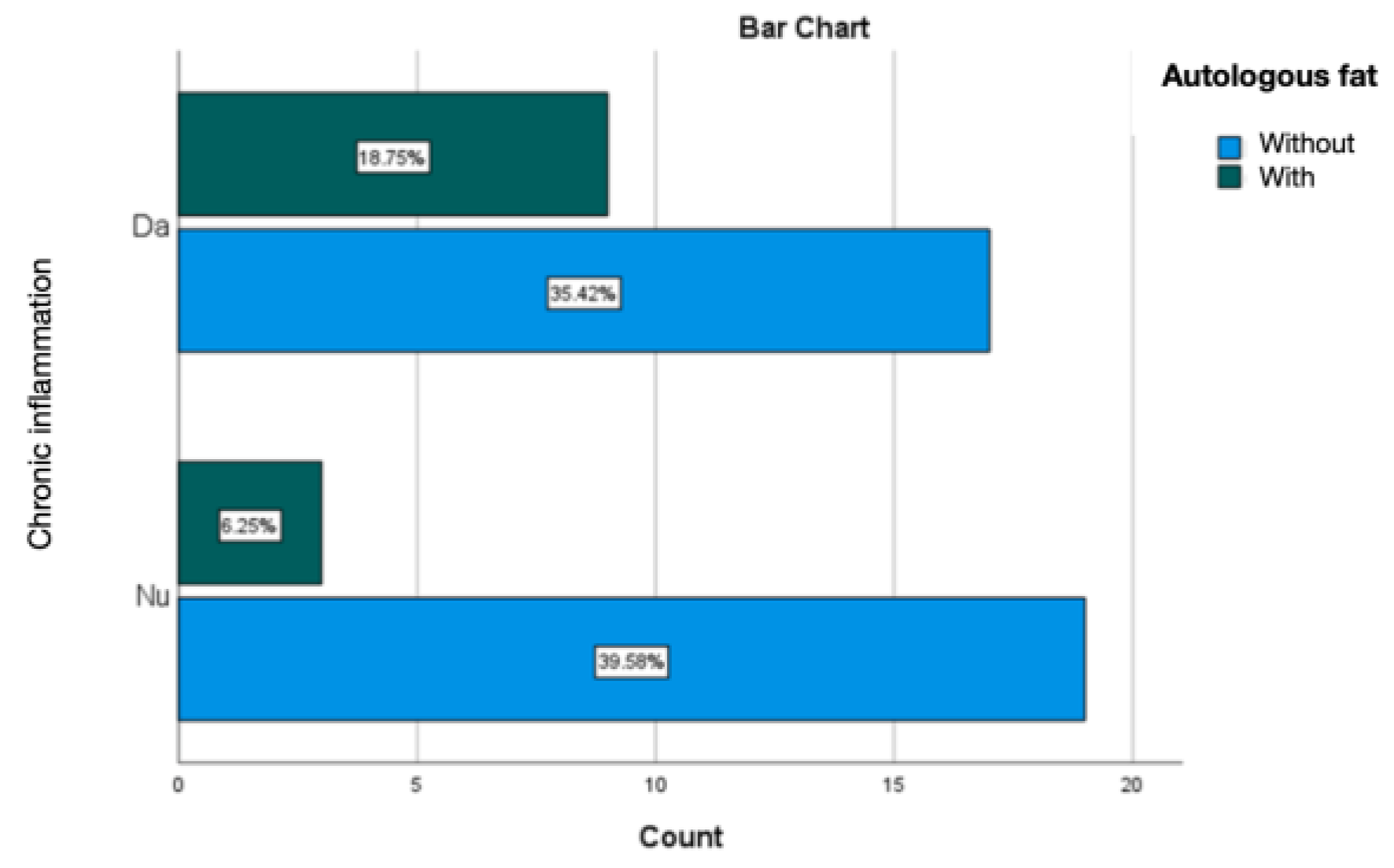
3.2. Statistical Study Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Berry, M.; Davies, D. Breast augmentation: Part I—A review of the silicone prosthesis. J. Plast. Reconstr. Aesthetic Surg. 2010, 63, 1761–1768. [Google Scholar] [CrossRef]
- Hajdu, S.D.; Agmon-Levin, N.; Shoenfeld, Y. Silicone and autoimmunity. Eur. J. Clin. Investig. 2011, 41, 203–211. [Google Scholar] [CrossRef]
- Zuckerman, D.M. Reasonably safe? Breast implants and informed consent. Reprod. Health Matters 2010, 18, 94–102. [Google Scholar] [CrossRef]
- Pittet, B.; Montandon, D.; Pittet, D. Infection in breast implants. Lancet Infect. Dis. 2005, 5, 94–106. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, T.F.; Hölmich, L.R.; Fryzek, J.P.; Friis, S.; McLaughlin, J.K.; Høyer, A.P.; Kjøller, K.; Olsen, J.H. Incidence and severity of short-term complications after breast augmentation results from a nationwide breast implant registry. Ann. Plast. Surg. 2003, 51, 531–539. [Google Scholar] [CrossRef]
- Fagrell, D.; Berggren, A.; Tarpila, E. Capsular contracture around saline-filled fine textured and smooth mammary implants: A prospective 7.5-year follow-up. Plast. Reconstr. Surg. 2001, 108, 2108–2112. [Google Scholar] [CrossRef]
- Wong, C.-H.; Samuel, M.; Tan, B.-K.; Song, C. Capsular Contracture in Subglandular Breast Augmentation with Textured versus Smooth Breast Implants: A Systematic Review. Plast. Reconstr. Surg. 2006, 118, 1224–1236. [Google Scholar] [CrossRef] [PubMed]
- Camirand, A.; Doucet, J. Breast Augmentation: Teaching Our Patients How Compression Can Help Prevent Capsular Contracture. Aesthetic Plast. Surg. 2000, 24, 221–226. [Google Scholar] [CrossRef]
- Araco, A.; Gravante, G.; Araco, F.; Delogu, D.; Cervelli, V.; Walgenbach, K. A Retrospective Analysis of 3,000 Primary Aesthetic Breast Augmentations: Postoperative Complications and Associated Factors. Aesthetic Plast. Surg. 2007, 31, 532–539. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, G.P.; Gabriel, A. Breast Augmentation. In Plastic Surgery, 3rd ed.; Peter, C.N., Ed.; Elsevier: Amsterdam, The Netherlands, 2012; Volume 5, pp. 37–38. [Google Scholar]
- Maxwekk, G.P.; Hartley, R.W., Jr. Breast Augmentation. In Plastic Surgery, 2nd ed.; Mathes, S.J., Ed.; Elsevier: Amsterdam, The Netherlands, 2005; Volume 6, pp. 26–29. [Google Scholar]
- Embrey, M.; Adams, E.E.; Cunningham, B.; Peters, W.; Young, V.L.; Carlo, G.L. A Review of the Literature on the Etiology of Capsular Contracture and a Pilot Study to Determine the Outcome of Capsular Contracture Interventions. Aesthetic Plast. Surg. 1999, 23, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Smalley, D.L.; Shanklin, D.R.; Hall, M.F.; Stevens, M.V.; Hanissian, A. Immunologic stimulation of T lymphocytes by silica after use of silicone mammary implants. FASEB J. 1995, 9, 424–427. [Google Scholar] [CrossRef]
- Smalley, D.L.; Shanklin, D.R.; Hall, M.F. Monocyte-dependent stimulation of human T cells by silicon dioxide. Pathobiology 1998, 66, 302–305. [Google Scholar] [CrossRef]
- Wolfram, D.; Rainer, C.; Niederegger, H.; Piza, H.; Wick, G. Cellular and molecular composition of fibrous capsules formed around silicone breast implants with special focus on local immune reactions. J. Autoimmun. 2004, 23, 81–91. [Google Scholar]
- Safran, T.; Nepon, H.; Chu, K.C.; Winocour, S.; Murphy, M.; Davison, G.P.; Dionisopolos, T.; Vorstenbosch, J. Current Concepts in Capsular Contracture: Pathophysiology, Prevention, and Management. In Seminars in Plastic Surgery; Thieme Medical Publishers, Inc.: Leipzig, Germany, 2021; Volume 35, pp. 189–197. [Google Scholar]
- Susini, P.; Nisi, G.; Pierazzi, D.M.; Giardino, F.R.; Pozzi, M.; Grimaldi, L.; Cuomo, R. Advances on Capsular Contracture—Prevention and Management Strategies: A Narrative Review of the Literature. Plast. Reconstr. Surg. Glob. Open 2023, 11, e5034. [Google Scholar] [CrossRef]
- Headon, H.; Kasem, A.; Mokbel, K. Capsular Contracture after Breast Augmentation: An Update for Clinical Practice. Arch. Plast. Surg. 2015, 42, 532–543. [Google Scholar] [CrossRef]
- Schreml, S.; Heine, N.; Eisenmann-Klein, M.; Prantl, L. Bacterial colonization is of major relevance for high-grade capsular con-tracture after augmentation mammaplasty. Ann. Plast. Surg. 2007, 59, 126–130. [Google Scholar] [CrossRef] [PubMed]
- Guimier, E.; Carson, L.; David, B.; Lambert, J.M.; Heery, E.; Malcolm, R.K. Pharmacological Approaches for the Prevention of Breast Implant Capsular Contracture. J. Surg. Res. 2022, 280, 129–150. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, J.R.; Salinas, H.M.; Broelsch, G.F.; McCormack, M.C.; Meppelink, A.M.; Randolph, M.A.; Redmond, R.W.; Austen, W.G., Jr. Prevention of capsular contracture with photochemical tissue passivation. Plast. Reconstr. Surg. 2014, 133, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Adams, W.P., Jr.; Rios, J.L.; Smith, S.J. Enhancing patient outcomes in aesthetic and reconstructive breast surgery using triple anti-biotic breast irrigation: Six-year prospective clinical study. Plast. Reconstr. Surg. 2006, 117, 30–36. [Google Scholar] [PubMed]
- Darouiche, R.O.; Meade, R.; Mansouri, M.D.; Netscher, D.T. In vivo efficacy of antimicrobe-impregnated saline-filled silicone im-plants. Plast. Reconstr. Surg. 2002, 109, 1352–1357. [Google Scholar] [CrossRef] [PubMed]
- Richters, C.D.; Paauw, N.J.; Mayen, I.; Van Bloois, L.; Metselaer, J.M.; Storm, G.; du Pont, J.S.; Hoekstra, M.J.; Kreis, R.W.; Kamperdijk, E.W. Administration of prednisolone phosphate–liposomes reduces wound contraction in a rat partial-thickness wound model. Wound Repair Regen. 2006, 14, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Moreira, M.; Fagundes, D.J.; Simões, M.d.J.; Taha, M.O.; Perez, L.M.N.; Bazotte, R.B. The effect of liposome-delivered prednisolone on collagen density, myofibroblasts, and fibrous capsule thickness around silicone breast implants in rats. Wound Repair Regen. 2010, 18, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Roça, G.B.; Graf, R.; Freitas, R.D.S.; Salles, G.; Francisco, J.C.; Noronha, L.; Maluf, I. Autologous Fat Grafting for Treatment of Breast Implant Capsular Contracture: A Study in Pigs. Aesthetic Surg. J. 2014, 34, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Correia-Pinto, J.M.; Poleri, F.; Barbosa, J.P.; Casimiro, R.; Azevedo, M.S.; Andresen, C.; Coelho, G.; Cunha, C.S.; Costa, H. Comparing Polyurethane and Acellular Dermal Matrix Implant Cover in Prepectoral Breast Reconstruction: Short-term Complications. Plast. Reconstr. Surg. Glob. Open 2023, 11, e4798. [Google Scholar] [CrossRef] [PubMed]
- Hester, T.R., Jr.; Bahair, H.G.; Hunter, R.M. Use of Dermal Matrix to Prevent Capsular Contracture in Aesthetic Breast Surgery. Plast. Reconstr. Surg. 2012, 130, 126S–136S. [Google Scholar] [CrossRef]
- Spear, S.L.; Sinkin, J.C.; Al-attar, A. Porcine Acellular Dermal Matrix (Steattice) in Primary and Revision Cosmetic Breast Surgery. Plast. Reconstr. Surg. 2013, 131, 1140–1148. [Google Scholar] [CrossRef]
- Gorgy, A.; Barone, N.; Nepon, H.; Dalfen, J.; Efanov, J.I.; Davison, P.; Vorstenbosch, J. Implant-based breast surgery and capsular formation: When, how and why?—A narrative review. Ann. Transl. Med. 2023, 11, 385. [Google Scholar] [CrossRef]
- Gonzalez, A.C.D.O.; Costa, T.F.; de Araújo Andrade, Z.; Medrado, A.R.A.P. Wound Healing—A Literature Review. An. Bras. Dermatol. 2016, 91, 614–620. [Google Scholar] [CrossRef]
- Colaris, M.J.L.; Ruhl, T.; Beier, J.P. Effects of Silicone Breast Implants on Human Cell Types In Vitro: A Closer Look on Host and Implant. Aesthetic Plast. Surg. 2022, 46, 2208–2217. [Google Scholar] [CrossRef]
- Park, J.U.; Ham, J.; Kim, S.; Seo, J.H.; Kim, S.H.; Lee, S.; Min, H.J.; Choi, S.; Choi, R.M.; Kim, H.; et al. Alleviation of capsular formations on silicone implants in rats using biomem-brane-mimicking coatings. Acta Biomater. 2014, 10, 4217–4225. [Google Scholar] [CrossRef]
- El-Sheikh, Y.; Tutino, R.; Knight, C.; Farrokhyar, F.; Hynes, N. Incidence of capsular contracture in silicone versus saline cosmetic augmentation mammoplasty: A meta-analysis. Can. J. Plast. Surg. 2008, 16, 211–215. [Google Scholar] [CrossRef]
- Hammond, J.B.; Kosiorek, H.E.; Cronin, P.A.; Rebecca, A.M.; Casey, W.J., 3rd; Wong, W.W.; Vargas, C.E.; Vern-Gross, T.Z.; McGee, L.A.; Pockaj, B.A. Capsular contracture in the modern era: A multidisciplinary look at the incidence and risk factors after mastectomy and implant-based breast reconstruction. Am. J. Surg. 2021, 221, 1005–1010. [Google Scholar] [CrossRef]
- Mendes, F.H.; Viterbo, F.; DeLucca, L. The Influence of External Ultrasound on the Histologic Architecture of the Organic Capsule Around Smooth Silicone Implants: Experimental Study in Rats. Aesthetic Plast. Surg. 2008, 32, 442–450. [Google Scholar] [CrossRef]
- Tamboto, H.; Vickery, K.; Deva, A.K. Subclinical (Biofilm) Infection Causes Capsular Contracture in a Porcine Model following Augmentation Mammaplasty. Plast. Reconstr. Surg. 2010, 126, 835–842. [Google Scholar] [CrossRef]
- Lee, J.S.; Kim, J.S.; Lee, J.W.; Choi, K.Y.; Yang, J.D.; Cho, B.C.; Oh, E.J.; Kim, T.J.; Ko, U.H.; Shin, J.H.; et al. Effect of Keratinocytes on Myofibroblasts in Hypertrophic Scars. Aesthetic Plast. Surg. 2019, 43, 1371–1380. [Google Scholar] [CrossRef]
- Sarrazy, V.; Billet, F.; Micallef, L.; Coulomb, B.; Desmoulière, A. Mechanisms of pathological scarring: Role of myofibroblasts and current developments. Wound Repair Regen. 2011, 19, s10–s15. [Google Scholar] [CrossRef]
- Mony, M.P.; Harmon, K.A.; Hess, R.; Dorafshar, A.H.; Shafikhani, S.H. An Updated Review of Hypertrophic Scarring. Cells 2023, 12, 678. [Google Scholar] [CrossRef] [PubMed]
- Unlu, R.E.; Yilmaz, A.D.; Orbay, H.; Can, B.; Tekdemir, I.; Sensoz, O. Influence of rifampin on capsule formation around silicone im-plants in a rat model. Aesthetic Plast. Surg. 2007, 31, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Monstrey, S.J.; Govaers, K.; Lejuste, P.; Lepelletier, D.; Ribeiro de Oliveira, P. Evaluation of the role of povidone-iodine in the pre-vention of surgical site infections. Surg. Open Sci. 2023, 13, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Gofstein-Hayuth, D.; Fliss, E.; Barnea, Y.; Legarda, C.; Bracha, G.; Lerner, A.; Lellouche, J.; Carmeli, Y.; Shani, N.; Arad, E. Comparing the efficacy of antimicrobial pocket-irrigation protocols in an in vivo breast implant infection model. J. Plast. Reconstr. Aesthetic Surg. 2023, 85, 165–173. [Google Scholar] [CrossRef]
- Frois, A.O.B.; Harbour, P.O.B.; Azimi, F.M.; Young, J.M.; Chan, B.M.; Mak, C.M.; Warrier, S.M. The Role of Antibiotics in Breast Pocket Irrigation and Implant Immersion: A Systematic Review. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1868. [Google Scholar] [CrossRef]
- Aladari, N.; Palaghia, M.M.; Trofin, A.-M.; Cojocaru, E.; Ungureanu, C.; Ianole, V.; Morosan, E.; Budacu, C.C.; Motruc, T.C.; Pertea, M.; et al. Reducing Capsular Contracture Formation in Breast Augmentation with Silicone Implants: Experimental Study on Rats. Appl. Sci. 2022, 12, 4056. [Google Scholar] [CrossRef]
- Nam, S.-Y.; Ji, H.B.; Shin, B.H.; Chien, P.N.; Donmez, N.; Zhang, X.R.; Huh, B.K.; Kim, M.J.; Bin Choy, Y.; Heo, C.Y. Silicone Breast Implant Coated with Triamcinolone Inhibited Breast-Implant-Induced Fibrosis in a Porcine Model. Materials 2021, 14, 3917. [Google Scholar] [CrossRef]
- Malahias, M.; Jordan, D.J.; Hughes, L.C.; Hindocha, S.; Juma, A. A literature review and summary of capsular contracture: An on-going challenge to breast surgeons and their patients. Int. J. Surg. Open 2016, 3, 1–7. [Google Scholar] [CrossRef]
- Lemperle, G.; Exner, K. Effect of cortisone on capsular contracture in double-lumen breast implants: Ten years’ experience. Aesthetic Plast. Surg. 1993, 17, 317–323. [Google Scholar] [CrossRef]
- Mladick, R.A. “No-touch” submuscular breast augmentation technique. Aesthetic Plast. Surg. 1993, 17, 183–192. [Google Scholar] [CrossRef]
- Katzel, E.B.B.; Koltz, P.F.M.; Tierney, R.B.; Williams, J.P.; Awad, H.A.; O’keefe, R.J.; Langstein, H.N.M. A Novel Animal Model for Studying Silicone Gel–Related Capsular Contracture. Plast. Reconstr. Surg. 2010, 126, 1483–1491. [Google Scholar] [CrossRef] [PubMed]
- Mojallal, A.; Lequeux, C.; Shipkov, C.; Breton, P.; Foyatier, J.-L.; Braye, F.; Damour, O. Improvement of Skin Quality after Fat Grafting: Clinical Observation and an Animal Study. Plast. Reconstr. Surg. 2009, 124, 765–774. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulos, S.; Vidovic, G.; Neid, M.; Abdallah, A. Using Fat Grafting to Treat Breast Implant Capsular Contracture. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1969. [Google Scholar] [CrossRef] [PubMed]
- Vieira, V.J.; D’Acampora, A.; Neves, F.S.; Mendes, P.R.; DE Vasconcellos, Z.A.; Neves, R.D.; Figueiredo, C.P. Capsular Contracture in Silicone Breast Implants: Insights from Rat Models. An. Acad. Bras. Ciências 2016, 88, 1459–1470. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Evaluation Criteria for the Capsule | Control | Rifampicin | Dexamethasone | Autologous Fat |
|---|---|---|---|---|
| Fibrillar neogenesis (collagen fibers) | +++ | +++ | +++ | ++ |
| Neogenesis of newly formed blood vessels | +++ | +++ | +++ | +++ |
| Leukocytic infiltrate | + | + | +++ | - |
| Thickness of the connective capsule | +++ uniform | ++ uniform | ++ non-uniform | + uniform |
| Uniformity of the capsule thickness | smooth | deformed (spicules) | deformed (spicules) | smooth |
| Acute Inflammation | Chronic Inflammation | Active Chronic Inflammation | Without Prosthesis Treatment | ||
|---|---|---|---|---|---|
| Acute inflammation | Pearson Correlation | 1 | −0.455 ** | −0.103 | 0.415 ** |
| Sig. (2-tailed) | 0.001 | 0.484 | 0.003 | ||
| N | 48 | 48 | 48 | 48 | |
| Chronic inflammation | Pearson Correlation | −0.455 ** | 1 | −0.422 ** | −0.338 * |
| Sig. (2-tailed) | 0.001 | 0.003 | 0.019 | ||
| N | 48 | 48 | 48 | 48 | |
| Active chronic inflammation | Pearson Correlation | −0.103 | −0.422 ** | 1 | 0.159 |
| Sig. (2-tailed) | 0.484 | 0.003 | 0.281 | ||
| N | 48 | 48 | 48 | 48 | |
| Without prosthesis treatment | Pearson Correlation | 0.415 ** | −0.338 * | 0.159 | 1 |
| Sig. (2-tailed) | 0.003 | 0.019 | 0.281 | ||
| N | 48 | 48 | 48 | 48 | |
| Acute Inflammation | Chronic Inflammation | Active Chronic Inflammation | Rifampicin Lavage | ||
|---|---|---|---|---|---|
| Acute inflammation | Pearson Correlation | 1 | −0.455 ** | −0.103 | −0.296 * |
| Sig. (2-tailed) | 0.001 | 0.484 | 0.041 | ||
| N | 48 | 48 | 48 | 48 | |
| Chronic inflammation | Pearson Correlation | −0.455 ** | 1 | −0.422 ** | 0.241 |
| Sig. (2-tailed) | 0.001 | 0.003 | 0.098 | ||
| N | 48 | 48 | 48 | 48 | |
| Active chronic inflammation | Pearson Correlation | −0.103 | −0.422 ** | 1 | −0.053 |
| Sig. (2-tailed) | 0.484 | 0.003 | 0.721 | ||
| N | 48 | 48 | 48 | 48 | |
| Rifampicin lavage | Pearson Correlation | −0.296 * | 0.241 | −0.053 | 1 |
| Sig. (2-tailed) | 0.041 | 0.098 | 0.721 | ||
| N | 48 | 48 | 48 | 48 | |
| Acute Inflammation | Chronic Inflammation | Active Chronic Inflammation | Dexamethasone Treatment | ||
|---|---|---|---|---|---|
| Acute inflammation | Pearson Correlation | 1 | −0.455 ** | −0.103 | 0.178 |
| Sig. (2-tailed) | 0.001 | 0.484 | 0.227 | ||
| N | 48 | 48 | 48 | 48 | |
| Chronic inflammation | Pearson Correlation | −0.455 ** | 1 | −0.422 ** | −0.145 |
| Sig. (2-tailed) | 0.001 | 0.003 | 0.326 | ||
| N | 48 | 48 | 48 | 48 | |
| Active chronic inflammation | Pearson Correlation | −0.103 | −0.422 ** | 1 | −0.053 |
| Sig. (2-tailed) | 0.484 | 0.003 | 0.721 | ||
| N | 48 | 48 | 48 | 48 | |
| Dexamethasone treatment | Pearson Correlation | 0.178 | −0.145 | −0.053 | 1 |
| Sig. (2-tailed) | 0.227 | 0.326 | 0.721 | ||
| N | 48 | 48 | 48 | 48 | |
| Acute Inflammation | Chronic Inflammation | Active Chronic Inflammation | Autologous Fat | ||
|---|---|---|---|---|---|
| Acute inflammation | Pearson Correlation | 1 | −0.455 ** | −0.103 | −0.296 * |
| Sig. (2-tailed) | 0.001 | 0.484 | 0.041 | ||
| N | 48 | 48 | 48 | 48 | |
| Chronic inflammation | Pearson Correlation | −0.455 ** | 1 | −0.422 ** | 0.241 |
| Sig. (2-tailed) | 0.001 | 0.003 | 0.098 | ||
| N | 48 | 48 | 48 | 48 | |
| Active chronic inflammation | Pearson Correlation | −0.103 | −0.422 ** | 1 | −0.053 |
| Sig. (2-tailed) | 0.484 | 0.003 | 0.721 | ||
| N | 48 | 48 | 48 | 48 | |
| Autologous fat | Pearson Correlation | −0.296 * | 0.241 | −0.053 | 1 |
| Sig. (2-tailed) | 0.041 | 0.098 | 0.721 | ||
| N | 48 | 48 | 48 | 48 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pertea, M.; Aladari, N.; Grosu, O.M.; Luca, S.; Tatar, R.; Avadanei, A.-N.; Palaghia, M.; Trofin, A.M.; Lunca, S.; Filip, N. A Histological Evaluation of the Efficiency of Using Periprosthetic Autologous Fat to Prevent Capsular Contracture Compared to Other Known Methods—An Experimental Study. Diagnostics 2024, 14, 661. https://doi.org/10.3390/diagnostics14060661
Pertea M, Aladari N, Grosu OM, Luca S, Tatar R, Avadanei A-N, Palaghia M, Trofin AM, Lunca S, Filip N. A Histological Evaluation of the Efficiency of Using Periprosthetic Autologous Fat to Prevent Capsular Contracture Compared to Other Known Methods—An Experimental Study. Diagnostics. 2024; 14(6):661. https://doi.org/10.3390/diagnostics14060661
Chicago/Turabian StylePertea, Mihaela, Nadia Aladari, Oxana Madalina Grosu, Stefana Luca, Raluca Tatar, Andrei-Nicolae Avadanei, Madalina Palaghia, Ana Maria Trofin, Sorinel Lunca, and Nina Filip. 2024. "A Histological Evaluation of the Efficiency of Using Periprosthetic Autologous Fat to Prevent Capsular Contracture Compared to Other Known Methods—An Experimental Study" Diagnostics 14, no. 6: 661. https://doi.org/10.3390/diagnostics14060661
APA StylePertea, M., Aladari, N., Grosu, O. M., Luca, S., Tatar, R., Avadanei, A.-N., Palaghia, M., Trofin, A. M., Lunca, S., & Filip, N. (2024). A Histological Evaluation of the Efficiency of Using Periprosthetic Autologous Fat to Prevent Capsular Contracture Compared to Other Known Methods—An Experimental Study. Diagnostics, 14(6), 661. https://doi.org/10.3390/diagnostics14060661