
The Impact of Total Tumor Diameter on Lymph Node Metastasis and Tumor Recurrence in Papillary Thyroid Carcinomas

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
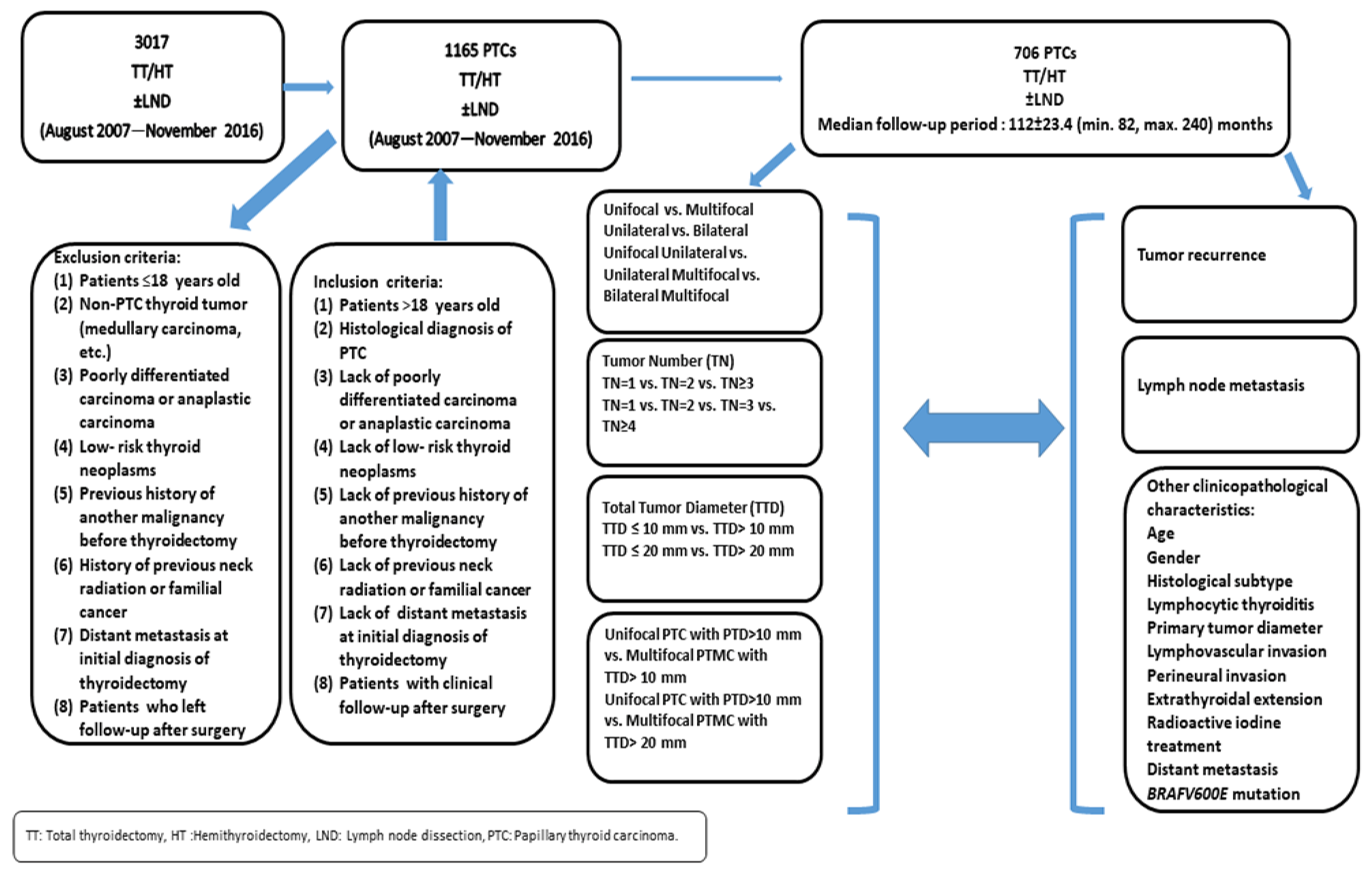
2.1. Study Design
2.2. Histopathological Features
2.2.1. Focality/Laterality and Number of Tumor Foci
2.2.2. Total Tumor Diameter
2.3. Clinical Features and Follow-Up Data
2.4. Molecular Analysis
2.5. Statistical Analysis
3. Results
3.1. Patients’ Clinicopathological Characteristics
3.2. Distribution of Clinicopathological Features According to Focality and Number of Tumor Foci
3.3. Comparisons of Clinicopathological Features among Unilateral Unifocal PTCs, Unilateral Multifocal PTCs, and Bilateral Multifocal PTCs
3.4. Distribution of Clinicopathological Features by Total Tumor Diameter
3.4.1. Comparison of Clinicopathological Features between Patients with a TTD of >10 mm and Patients with a TTD of ≤10 mm
3.4.2. Comparison of Clinicopathological Features between Patients with a TTD of >20 mm and Patients with a TTD of ≤20 mm
3.4.3. Comparison of Clinicopathological Features between Patients with Unifocal Papillary Thyroid Carcinomas Larger Than 10 mm and Patients with Multifocal Papillary Microcarcinomas with a TTD of >10 mm and >20 mm
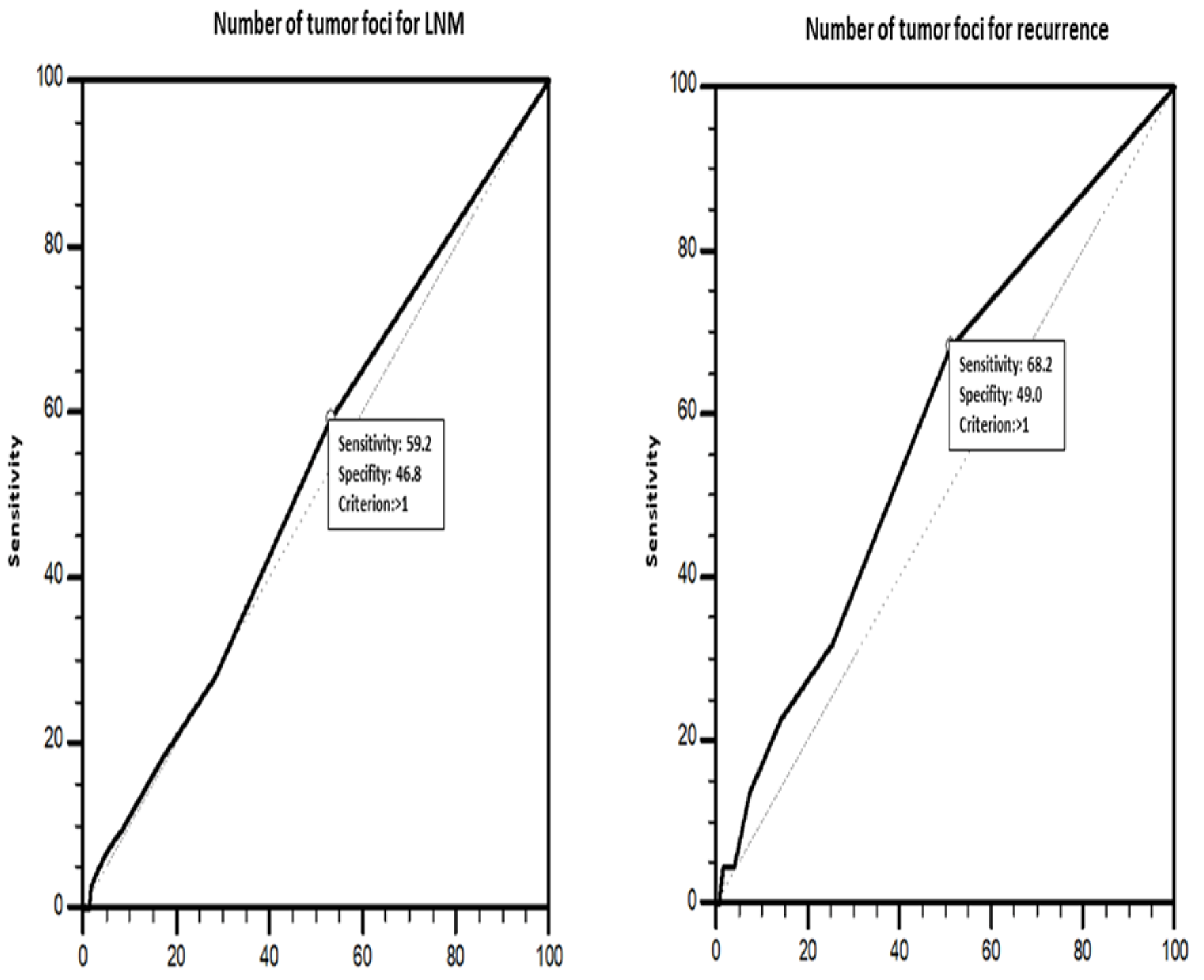
3.5. Clinicopathological Features Predictive of LNM
3.6. Clinicopathological Features Predictive of Recurrence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Miranda-Filho, A.; Lortet-Tieulent, J.; Bray, F.; Cao, B.; Franceschi, S.; Vaccarella, S.; Dal Maso, L. Thyroid cancer incidence trends by histology in 25 countries: A population-based study. Lancet Diabetes Endocrinol. 2021, 9, 225–234. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Davies, L.; Welch, H.G. Current thyroid cancer trends in the United States. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Sawka, A.M.; Alexander, E.K.; Bible, K.C.; Caturegli, P.; Doherty, G.M.; Mandel, S.J.; Morris, J.C.; Nassar, A.; Pacini, F.; et al. American Thyroid Association Guidelines on the Management of Thyroid Nodules and Differentiated Thyroid Cancer Task Force Review and Recommendation on the Proposed Renaming of Encapsulated Follicular Variant Papillary Thyroid Carcinoma Without Invasion to Noninvasive Follicular Thyroid Neoplasm with Papillary-Like Nuclear Features. Thyroid 2017, 27, 481–483. [Google Scholar] [PubMed]
- Lamartina, L.; Grani, G.; Arvat, E.; Nervo, A.; Zatelli, M.C.; Rossi, R.; Puxeddu, E.; Morelli, S.; Torlontano, M.; Massa, M.; et al. 8th edition of the AJCC/TNM staging system of thyroid cancer: What to expect (ITCO#2). Endocr. Relat. Cancer 2018, 25, L7–L11. [Google Scholar] [PubMed]
- Tuttle, R.M.; Haugen, B.; Perrier, N.D. Updated American Joint Committee on Cancer/Tumor-Node-Metastasis Staging System for Differentiated and Anaplastic Thyroid Cancer (Eighth Edition): What Changed and Why? Thyroid 2017, 27, 751–756. [Google Scholar] [CrossRef] [PubMed]
- Gharib, H.; Papini, E.; Garber, J.R.; Duick, D.S.; Harrell, R.M.; Hegedus, L.; Paschke, R.; Valcavi, R.; Vitti, P. American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi Medical Guidelines for Clinical Practice for the Diagnosis and Management of Thyroid Nodules—2016 Update. Endocr. Pract. 2016, 22, 622–639. [Google Scholar] [CrossRef]
- Perros, P.; Boelaert, K.; Colley, S.; Evans, C.; Evans, R.M.; Gerrard Ba, G.; Gilbert, J.; Harrison, B.; Johnson, S.J.; Giles, T.E.; et al. Guidelines for the management of thyroid cancer. Clin. Endocrinol. 2014, 81 (Suppl. S1), 1–122. [Google Scholar] [CrossRef]
- Haddad, R.I.; Bischoff, L.; Ball, D.; Bernet, V.; Blomain, E.; Busaidy, N.L.; Campbell, M.; Dickson, P.; Duh, Q.Y.; Ehya, H.; et al. Thyroid Carcinoma, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2022, 20, 925–951. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.J.; Kim, S.M.; Lee, Y.S.; Chung, W.Y.; Chang, H.S.; Park, C.S. Prognostic significance of tumor multifocality in papillary thyroid carcinoma and its relationship with primary tumor size: A retrospective study of 2,309 consecutive patients. Ann. Surg. Oncol. 2015, 22, 125–131. [Google Scholar] [CrossRef]
- Omi, Y.; Haniu, K.; Kamio, H.; Fujimoto, M.; Yoshida, Y.; Horiuchi, K.; Okamoto, T. Pathological multifocality is not a prognosis factor of papillary thyroid carcinoma: A single-center, retrospective study. World J. Surg. Oncol. 2022, 20, 394. [Google Scholar] [CrossRef]
- Ozdemir, K.; Harmantepe, A.T.; Gonullu, E.; Kocer, B.; Bayhan, Z. Should multifocality be an indication for prophylactic central neck dissection in papillary thyroid cancer? Updates Surg. 2023, 75, 701–706. [Google Scholar] [CrossRef]
- Pitt, S.C.; Sippel, R.S.; Chen, H. Contralateral papillary thyroid cancer: Does size matter? Am. J. Surg. 2009, 197, 342–347. [Google Scholar] [CrossRef]
- Pasieka, J.L.; Thompson, N.W.; McLeod, M.K.; Burney, R.E.; Macha, M. The incidence of bilateral well-differentiated thyroid cancer found at completion thyroidectomy. World J. Surg. 1992, 16, 711–716, discussion 6–7. [Google Scholar] [CrossRef]
- Dewil, B.; Van Damme, B.; Vander Poorten, V.; Delaere, P.; Debruyne, F. Completion thyroidectomy after the unexpected diagnosis of thyroid cancer. B-ENT 2005, 1, 67–72. [Google Scholar] [PubMed]
- Tam, A.A.; Ozdemir, D.; Cuhaci, N.; Baser, H.; Dirikoc, A.; Aydin, C.; Yazgan, A.K.; Ersoy, R.; Çakır, B. Can ratio of the biggest tumor diameter to total tumor diameter be a new parameter in the differential diagnosis of agressive and favorable multifocal papillary thyroid microcarcinoma? Oral Oncol. 2017, 65, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Su, X.; He, K.; Wang, Y.; Wang, H.; Wang, H.; Zhao, Y.; Zhao, W.; Zarnegar, R.; Fahey, T.J.; et al. Comparison of the clinicopathologic features and prognosis of bilateral versus unilateral multifocal papillary thyroid cancer: An updated study with more than 2000 consecutive patients. Cancer 2016, 122, 198–206. [Google Scholar] [CrossRef]
- Tam, A.A.; Ozdemir, D.; Cuhaci, N.; Baser, H.; Aydin, C.; Yazgan, A.K.; Ersoy, R.; Çakır, B. Association of multifocality, tumor number, and total tumor diameter with clinicopathological features in papillary thyroid cancer. Endocrine 2016, 53, 774–783. [Google Scholar] [CrossRef]
- Pisanu, A.; Saba, A.; Podda, M.; Reccia, I.; Uccheddu, A. Nodal metastasis and recurrence in papillary thyroid microcarcinoma. Endocrine 2015, 48, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Ye, T.; Lai, S.; Cao, B.; Xu, B.; Wang, R. Analysis of risk factors for recurrence of differentiated thyroid carcinoma after surgical resection combined with iodine-131 and TSH suppression therapy. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2023, 37, 370–374. [Google Scholar]
- Kaur, J.; Nadarajan, A.; Janardhan, D.; George, N.A.; Thomas, S.; Varghese, B.T.; Krishna, J. Predictive factors for nodal recurrence in differentiated thyroid cancers. Cancer Treat Res. Commun. 2023, 36, 100728. [Google Scholar] [CrossRef]
- Rodriguez Schaap, P.M.; Lin, J.F.; Metman, M.J.H.; Dreijerink, K.M.A.; Links, T.P.; Bonjer, H.J.; Nieveen van Dijkum, E.J.M.; Dickhoff, C.; Kruijff, S.; Engelsman, A.F. Bilaterality, not multifocality, is an independent risk factor for recurrence in low-risk papillary thyroid cancer. J. Natl. Cancer Inst. 2023, 115, 1071–1076. [Google Scholar] [CrossRef]
- Zhu, F.; Shen, Y.B.; Li, F.Q.; Fang, Y.; Hu, L.; Wu, Y.J. The Effects of Hashimoto Thyroiditis on Lymph Node Metastases in Unifocal and Multifocal Papillary Thyroid Carcinoma: A Retrospective Chinese Cohort Study. Medicine 2016, 95, e2674. [Google Scholar] [CrossRef]
- So, Y.K.; Kim, M.W.; Son, Y.I. Multifocality and bilaterality of papillary thyroid microcarcinoma. Clin. Exp. Otorhinolaryngol. 2015, 8, 174–178. [Google Scholar] [CrossRef]
- Pyo, J.S.; Sohn, J.H.; Kang, G.; Kim, D.H.; Yun, J. Total surface area is useful for differentiating between aggressive and favorable multifocal papillary thyroid carcinomas. Yonsei Med. J. 2015, 56, 355–361. [Google Scholar] [CrossRef]
- Zhao, Q.; Ming, J.; Liu, C.; Shi, L.; Xu, X.; Nie, X.; Huang, T. Multifocality and total tumor diameter predict central neck lymph node metastases in papillary thyroid microcarcinoma. Ann. Surg. Oncol. 2013, 20, 746–752. [Google Scholar] [CrossRef]
- Kuo, S.F.; Lin, S.F.; Chao, T.C.; Hsueh, C.; Lin, K.J.; Lin, J.D. Prognosis of multifocal papillary thyroid carcinoma. Int. J. Endocrinol. 2013, 2013, 809382. [Google Scholar] [CrossRef]
- Kim, H.J.; Sohn, S.Y.; Jang, H.W.; Kim, S.W.; Chung, J.H. Multifocality, but not bilaterality, is a predictor of disease recurrence/persistence of papillary thyroid carcinoma. World J. Surg. 2013, 37, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Mazeh, H.; Samet, Y.; Hochstein, D.; Mizrahi, I.; Ariel, I.; Eid, A.; Freund, H.R. Multifocality in well-differentiated thyroid carcinomas calls for total thyroidectomy. Am. J. Surg. 2011, 201, 770–775. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.W.; Qu, Z.; Qin, A.C.; Pan, H.; Ye, J.; Jiang, Y. Significance of multifocality in papillary thyroid carcinoma. Eur. J. Surg. Oncol. 2020, 46 Pt 10A, 1820–1828. [Google Scholar] [CrossRef] [PubMed]
- Macedo, F.I.; Mittal, V.K. Total thyroidectomy versus lobectomy as initial operation for small unilateral papillary thyroid carcinoma: A meta-analysis. Surg. Oncol. 2015, 24, 117–122. [Google Scholar] [CrossRef]
- Tam, A.A.; Ozdemir, D.; Ogmen, B.E.; Faki, S.; Dumlu, E.G.; Yazgan, A.K.; Ersoy, R.; Cakır, B. Should Multifocal Papillary Thyroid Carcinomas Classified as T1a with a Tumor Diameter Sum of 1 to 2 Centimeters Be Reclassified as T1b? Endocr. Pract. 2017, 23, 526–535. [Google Scholar] [CrossRef]
- Lou, J.; Yang, J.; Luo, Y.; Zhu, Y.; Xu, Z.; Hua, T. Analysis of the influence factors of cervical lymph node metastasis in Papillary thyroid carcinoma: A retrospective observational study. Medicine 2023, 102, e35045. [Google Scholar] [CrossRef]
- Feng, J.W.; Pan, H.; Wang, L.; Ye, J.; Jiang, Y.; Qu, Z. Total tumor diameter: The neglected value in papillary thyroid microcarcinoma. J. Endocrinol. Investig. 2020, 43, 601–613. [Google Scholar] [CrossRef]
- Feng, J.W.; Wu, W.X.; Hu, J.; Hong, L.Z.; Qin, A.C.; Jiang, Y.; Ye, J. Influence of Tumor Number on Clinicopathologic Features and Outcomes of Patients With Papillary Thyroid Carcinoma. Am. J. Clin. Pathol. 2020, 154, 848–858. [Google Scholar] [CrossRef] [PubMed]
- Christofer Juhlin, C.; Mete, O.; Baloch, Z.W. The 2022 WHO classification of thyroid tumors: Novel concepts in nomenclature and grading. Endocr. Relat. Cancer 2023, 30, e220293. [Google Scholar] [CrossRef]
- Cooper, D.S.; Doherty, G.M.; Haugen, B.R.; Kloos, R.T.; Lee, S.L.; Mandel, S.J.; Mazzaferri, E.L.; Mciver, B.; Pacini, F.; Schlumberger, M.; et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 2009, 19, 1167–1214. [Google Scholar] [CrossRef] [PubMed]
- Griffin, M.J.; Baik, F.M.; Brandwein-Weber, M.; Qazi, M.; Yue, L.E.; Osorio, M.; Urken, M.L. Positive Lymph Node Counts in American Thyroid Association Low-Risk Papillary Thyroid Carcinoma Patients. World J. Surg. 2020, 44, 1892–1897. [Google Scholar] [CrossRef] [PubMed]
- Heng, Y.; Yang, Z.; Lin, J.; Liu, Q.; Cai, W.; Tao, L. Risks of central lymph node metastasis in papillary thyroid carcinoma with or without multifocality in at least one lobe: A multi-center analysis. Oral Oncol. 2022, 134, 106185. [Google Scholar] [CrossRef] [PubMed]
- Geron, Y.; Benbassat, C.; Shteinshneider, M.; Or, K.; Markus, E.; Hirsch, D.; Levy, S.; Ziv-Baran, T.; Muallem-Kalmovich, L. Multifocality Is not an Independent Prognostic Factor in Papillary Thyroid Cancer: A Propensity Score-Matching Analysis. Thyroid 2019, 29, 513–522. [Google Scholar] [CrossRef]
- Iacobone, M.; Jansson, S.; Barczynski, M.; Goretzki, P. Multifocal papillary thyroid carcinoma--a consensus report of the European Society of Endocrine Surgeons (ESES). Langenbecks Arch. Surg. 2014, 399, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Wang, Y.; Miao, C.; Yu, X.; Yan, H.; Xie, Q.; Sanjay, J.; Zhao, Q. Defining a New Tumor Dimension in Staging of Papillary Thyroid Carcinoma. Ann. Surg. Oncol. 2017, 24, 1551–1556. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Lan, X.; Zhang, H.; Dong, W.; Wang, Z.; He, L.; Zhang, T.; Liu, S. Risk Factors for Central Lymph Node Metastasis in CN0 Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0139021. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.D.; Chao, T.C.; Hsueh, C.; Kuo, S.F. High recurrent rate of multicentric papillary thyroid carcinoma. Ann. Surg. Oncol. 2009, 16, 2609–2616. [Google Scholar] [CrossRef]
- Papageorgiou, M.S.; Liratzopoulos, N.; Efremidou, E.I.; Karanikas, M.; Minipoulos, G.; Manolas, K.J. Multifocality of thyroid carcinomas: A “privilege” of papillary tumors or not? Il G. Di Chir. 2010, 31, 20–23. [Google Scholar]
- Riss, J.C.; Peyrottes, I.; Chamorey, E.; Haudebourg, J.; Sudaka, A.; Benisvy, D.; Marcy, P.Y.; Nao, E.E.; Demard, F.; Vallicioni, J.; et al. Prognostic impact of tumour multifocality in thyroid papillary microcarcinoma based on a series of 160 cases. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2012, 129, 175–178. [Google Scholar] [CrossRef]
- Yang, Y.; Chen, C.; Chen, Z.; Jiang, J.; Chen, Y.; Jin, L.; Guo, G.; Zhang, X.; Ye, T. Prediction of central compartment lymph node metastasis in papillary thyroid microcarcinoma. Clin. Endocrinol. 2014, 81, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Iida, F.; Yonekura, M.; Miyakawa, M. Study of intraglandular dissemination of thyroid cancer. Cancer 1969, 24, 764–771. [Google Scholar] [CrossRef]
- Al Afif, A.; Williams, B.A.; Rigby, M.H.; Bullock, M.J.; Taylor, S.M.; Trites, J.; Hart, R.D. Multifocal Papillary Thyroid Cancer Increases the Risk of Central Lymph Node Metastasis. Thyroid 2015, 25, 1008–1012. [Google Scholar] [CrossRef]
- Shattuck, T.M.; Westra, W.H.; Ladenson, P.W.; Arnold, A. Independent clonal origins of distinct tumor foci in multifocal papillary thyroid carcinoma. N. Engl. J. Med. 2005, 352, 2406–2412. [Google Scholar] [CrossRef]
- Russell, W.O.; Ibanez, M.L.; Clark, R.L.; White, E.C. Thyroid Carcinoma. Classification, Intraglandular Dissemination, and Clinicopathological Study Based Upon Whole Organ Sections of 80 Glands. Cancer 1963, 16, 1425–1460. [Google Scholar] [CrossRef]
- Zhu, J.; Wang, X.; Zhang, X.; Li, P.; Hou, H. Clinicopathological features of recurrent papillary thyroid cancer. Diagn. Pathol. 2015, 10, 96. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Beom Heo, D.; Piao, Y.; Hee Lee, J.; Ju, S.H.; Yi, H.S.; Su Kim, M.; Won, H.R.; Won Chang, J.; Seok Koo, B.; Eun Kang, Y. Completion thyroidectomy may not be required for papillary thyroid carcinoma with multifocality, lymphovascular invasion, extrathyroidal extension to the strap muscles, or five or more central lymph node micrometastasis. Oral Oncol. 2022, 134, 106115. [Google Scholar] [CrossRef]
- Wang, F.; Yu, X.; Shen, X.; Zhu, G.; Huang, Y.; Liu, R.; Viola, D.; Elisei, R.; Puxeddu, E.; Fugazzola, L.; et al. The Prognostic Value of Tumor Multifocality in Clinical Outcomes of Papillary Thyroid Cancer. J. Clin. Endocrinol. Metab. 2017, 102, 3241–3250. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Park, H.K.; Byun, D.W.; Suh, K.; Yoo, M.H.; Min, Y.K.; Kim, S.W.; Chung, J.H. Number of tumor foci as predictor of lateral lymph node metastasis in papillary thyroid carcinoma. Head Neck 2015, 37, 650–654. [Google Scholar] [CrossRef] [PubMed]
- Qu, N.; Zhang, L.; Ji, Q.H.; Zhu, Y.X.; Wang, Z.Y.; Shen, Q.; Wang, Y.; Li, D.S. Number of tumor foci predicts prognosis in papillary thyroid cancer. BMC Cancer 2014, 14, 914. [Google Scholar] [CrossRef]
- Siddiqui, S.; White, M.G.; Antic, T.; Grogan, R.H.; Angelos, P.; Kaplan, E.L.; Cipriani, N.A. Clinical and Pathologic Predictors of Lymph Node Metastasis and Recurrence in Papillary Thyroid Microcarcinoma. Thyroid 2016, 26, 807–815. [Google Scholar] [CrossRef]
- Liu, L.S.; Liang, J.; Li, J.H.; Liu, X.; Jiang, L.; Long, J.X.; Jiang, Y.M.; Wei, Z.X. The incidence and risk factors for central lymph node metastasis in cN0 papillary thyroid microcarcinoma: A meta-analysis. Eur. Arch. Otorhinolaryngol. 2017, 274, 1327–1338. [Google Scholar] [CrossRef]
- Ma, B.; Wang, Y.; Yang, S.; Ji, Q. Predictive factors for central lymph node metastasis in patients with cN0 papillary thyroid carcinoma: A systematic review and meta-analysis. Int. J. Surg. 2016, 28, 153–161. [Google Scholar] [CrossRef]
- Xiang, Y.; Lin, K.; Dong, S.; Qiao, L.I.; He, Q.; Zhang, X. Prediction of central lymph node metastasis in 392 patients with cervical lymph node-negative papillary thyroid carcinoma in Eastern China. Oncol Lett. 2015, 10, 2559–2564. [Google Scholar] [CrossRef]
- Liang, K.; He, L.; Dong, W.; Zhang, H. Risk factors of central lymph node metastasis in cN0 papillary thyroid carcinoma: A study of 529 patients. Med. Sci. Monit. 2014, 20, 807–811. [Google Scholar]
- Wu, Z.J.; Xia, B.Y.; Chen, Z.W.; Gong, H.; Abuduwaili, M.; Xing, Z.C.; Su, A.P. The value of total tumor diameter in unilateral multifocal papillary thyroid carcinoma: A propensity score matching analysis. Front. Endocrinol. 2023, 14, 1217613. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.M.; Park, J.B.; Bae, K.S.; Kang, S.J. Analysis of prognostic factors in patients with multiple recurrences of papillary thyroid carcinoma. Surg. Oncol. 2012, 21, 185–190. [Google Scholar] [CrossRef]
- Koo, B.S.; Lim, H.S.; Lim, Y.C.; Yoon, Y.H.; Kim, Y.M.; Park, Y.H.; Rha, K.S. Occult contralateral carcinoma in patients with unilateral papillary thyroid microcarcinoma. Ann. Surg. Oncol. 2010, 17, 1101–1105. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Liu, Z.; Yu, P.; Liu, C.; Ming, J.; Zhang, N.; Yusufu, M.; Chen, C.; Huang, T. Using foci number to predict central lymph node metastases of papillary thyroid microcarcinomas with multifocality. Int. J. Clin. Exp. Med. 2015, 8, 9925–9930. [Google Scholar] [PubMed]
- Qu, H.; Sun, G.R.; Liu, Y.; He, Q.S. Clinical risk factors for central lymph node metastasis in papillary thyroid carcinoma: A systematic review and meta-analysis. Clin. Endocrinol. 2015, 83, 124–132. [Google Scholar] [CrossRef]
- Bansal, M.; Gandhi, M.; Ferris, R.L.; Nikiforova, M.N.; Yip, L.; Carty, S.E.; Nikiforov, Y.E. Molecular and histopathologic characteristics of multifocal papillary thyroid carcinoma. Am. J. Surg. Pathol. 2013, 37, 1586–1591. [Google Scholar] [CrossRef]
- Lin, X.; Finkelstein, S.D.; Zhu, B.; Silverman, J.F. Molecular analysis of multifocal papillary thyroid carcinoma. J. Mol. Endocrinol. 2008, 41, 195–203. [Google Scholar] [CrossRef]
- Wang, W.; Wang, H.; Teng, X.; Wang, H.; Mao, C.; Teng, R.; Zhao, W.; Cao, J.; Fahey, T.J.; Teng, L. Clonal analysis of bilateral, recurrent, and metastatic papillary thyroid carcinomas. Hum. Pathol. 2010, 41, 1299–1309. [Google Scholar] [CrossRef]
- Can, N.; Tastekin, E.; Ozyilmaz, F.; Sezer, Y.A.; Guldiken, S.; Sut, N.; Sarikas, N.; Oz Puyan, F.; Guler, B.; Ayturk, S.; et al. Histopathological Evidence of Lymph Node Metastasis in Papillary Thyroid Carcinoma. Endocr. Pathol. 2015, 26, 218–228. [Google Scholar] [CrossRef]
- Liu, C.; Wang, S.; Zeng, W.; Guo, Y.; Liu, Z.; Huang, T. Total tumour diameter is superior to unifocal diameter as a predictor of papillary thyroid microcarcinoma prognosis. Sci. Rep. 2017, 7, 1846. [Google Scholar] [CrossRef] [PubMed]
- Xue, S.; Wang, P.; Liu, J.; Chen, G. Total thyroidectomy may be more reasonable as initial surgery in unilateral multifocal papillary thyroid microcarcinoma: A single-center experience. World J. Surg. Oncol. 2017, 15, 62. [Google Scholar] [CrossRef] [PubMed]
- Buffet, C.; Golmard, J.L.; Hoang, C.; Tresallet, C.; Du Pasquier Fediaevsky, L.; Fierrard, H.; Fierrard, H.; Aurengo, A.; Menegaux, F.; Leenhardt, L. Scoring system for predicting recurrences in patients with papillary thyroid microcarcinoma. Eur. J. Endocrinol. 2012, 167, 267–275. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chereau, N.; Tresallet, C.; Noullet, S.; Godiris-Petit, G.; Tissier, F.; Leenhardt, L.; Menegaux, F. Does the T1 subdivision correlate with the risk of recurrence of papillary thyroid cancer? Langenbecks Arch. Surg. 2016, 401, 223–230. [Google Scholar] [CrossRef]
- Manso, J.; Censi, S.; Roberti, A.; Iacobone, M.; Barollo, S.; Bertazza, L.; Galuppini, F.; Vianello, F.; Albinger, N.; Scaroni, C.; et al. Prognostic significance of the sum of the diameters of single foci in multifocal papillary thyroid cancer: The concept of new-old tumor burden. Ther. Adv. Endocrinol. Metab. 2020, 11, 2042018820964326. [Google Scholar] [CrossRef]
- Hitu, L.; Stefan, P.A.; Piciu, D. Total Tumor Diameter and Unilateral Multifocality as Independent Predictor Factors for Metastatic Papillary Thyroid Microcarcinoma. J. Clin. Med. 2021, 10, 3707. [Google Scholar] [CrossRef]
- Jiang, K.C.; Lin, B.; Zhang, Y.; Zhao, L.Q.; Luo, D.C. Total tumor diameter is a better indicator of multifocal papillary thyroid microcarcinoma: A propensity score matching analysis. Front. Endocrinol. 2022, 13, 974755. [Google Scholar] [CrossRef]
- Kwon, H.; Lim, W.; Moon, B.I. Number of Tumor Foci as a Risk Factor for Recurrence in Papillary Thyroid Carcinoma: Does It Improve Predictability? Cancers 2022, 14, 4141. [Google Scholar] [CrossRef]
- Rowe, C.W.; Dill, T.; Griffin, N.; Jobling, P.; Faulkner, S.; Paul, J.W.; King, S.; Smith, R.; Hondermarck, H. Innervation of papillary thyroid cancer and its association with extra-thyroidal invasion. Sci. Rep. 2020, 10, 1539. [Google Scholar] [CrossRef]
- Limberg, J.; Lee-Saxton, Y.J.; Egan, C.E.; AlAnazi, A.; Easthausen, I.; Stefanova, D.; Stamatiou, A.; Beninato, T.; Zarnegar, R.; Scognamiglio, T.; et al. Perineural Invasion in Papillary Thyroid Cancer: A Rare Indicator of Aggressive Disease. Ann. Surg. Oncol. 2023, 30, 3570–3577. [Google Scholar] [CrossRef]
- Sezer, A.; Celik, M.; Yilmaz Bulbul, B.; Can, N.; Tastekin, E.; Ayturk, S.; Ustun, F.; Guldiken, S.; Sut, N. Relationship between lymphovascular invasion and clinicopathological features of papillary thyroid carcinoma. Bosn. J. Basic Med. Sci. 2017, 17, 144–151. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| In Papillary Carcinomas n (%) | Total | In Papillary Microcarcinomas n (%) | Total | ||
|---|---|---|---|---|---|
| Age | ≤45 years | 235 (33.3) | 706 | 123 (30.3) | 406 |
| >45 years | 471 (66.7) | 283 (69.7) | |||
| Gender | Female | 589 (83.4) | 706 | 351 (86.5) | 406 |
| Male | 117 (16.6) | 55 (13.5) | |||
| Surgery Procedure | Total thyroidectomy | 668 (94.6) | 706 | 372 (91.6) | 406 |
| Lobectomy | 38 (5.4) | 34 (8.4) | |||
| + LN dissection | 434 (61.5) | 236 (58.1) | |||
| Lymphocytic thyroiditis | Absent | 411 (58.3) | 706 | 228 (56.2) | 406 |
| Present | 295 (41.7) | 178 (43.8) | |||
| Primary tumor diameter | ≤10 mm | 406 (57.5) | 706 | 406 (100.0) | 406 |
| >10 mm | 300 (42.5) | ||||
| Total tumor diameter: 10 mm | ≤10 mm | 323 (45.2) | 706 | 316 (77.8) | 406 |
| >10 mm | 383 (54.2) | 90 (22.2) | |||
| Total tumor diameter: 20 mm | ≤20 mm | 528 (74.8) | 706 | 398 (98.0) | 406 |
| >20 mm | 178 (25.2) | 8 (2.0) | |||
| Histological subtype | CPTC | 346 (49.0) | 706 | 210 (51.7) | 406 |
| IFPTC | 336 (47.6) | 188 (46.3) | |||
| ASPTC | 24 (3.4) | 8 (2.0) | |||
| Tumor laterality | Unilateral | 440 (65.9) | 668 | 269 (72.3) | 372 |
| Bilateral | 228 (34.1) | 103 (27.7) | |||
| Tumor focality | Unifocal | 340 (48.2) | 706 | 219 (53.9) | 406 |
| Multifocal | 366 (51.8) | 187 (46.1) | |||
| Tumor laterality and focality | Unilateral/unifocal | 308 (46.1) | 668 | 190 (51.1) | 372 |
| Unilateral/multifocal | 134 (20.1) | 80 (21.5) | |||
| Bilateral/multifocal | 226 (33.8) | 102 (27.4) | |||
| Tumor foci (4-tiered system) | 1 | 342 (48.4) | 706 | 219 (54.0) | 406 |
| 2 | 183 (25.9) | 104 (25.6) | |||
| 3 | 79 (11.2) | 42 (10.3) | |||
| 4+ | 102 (14.5) | 41 (10.1) | |||
| Tumor foci (3-tiered system) | 1 | 342 (48.4) | 219 (54.0)) | ||
| 2 | 183 (25.9) | 104 (25.6) | |||
| 3+ | 181 (25.7) | 83 (20.4) | |||
| Lymphovascular invasion | Absent | 639 (90.5) | 706 | 393 (96.8) | 406 |
| Present | 67 (9.5) | 13 (3.2) | |||
| Perineural invasion | Absent | 693 (98.2) | 706 | 403 (99.3) | 406 |
| Present | 13 (1.8) | 3 (0.7) | |||
| Lymph node metastasis | Absent | 362 (83.4) | 434 | 210 (89.0) | 236 |
| Present | 72 (16.6) | 26 (11.0) | |||
| Extrathyroidal extension | Absent | 566 (80.2) | 706 | 357 (87.9) | 406 |
| Present | 140 (19.8) | 49 (12.1) | |||
| Radioactive iodine therapy | Absent | 326 (46.2) | 706 | 319 (78.6) | 406 |
| Present | 380 (53.8) | 87 (21.4) | |||
| Recurrence | Absent | 684 (96.9) | 706 | 399 (98.3) | 406 |
| Present | 22 (3.1) | 7 (1.7) | |||
| Distant metastasis | Absent | 705 (99.9) | 706 | 406 (100.0) | 406 |
| Present | 1 (0.1) | - | |||
| BRAFV600E | Wild-type | 362 (79.6) | 455 | 218 (84.2) | 259 |
| Mutated | 93 (20.4) | 41 (15.8) | |||
| Variables | TTD ≤10 mm n: 323 | TTD >10 mm n: 383 | p | TTD ≤20 mm n: 528 | TTD >20 mm n: 178 | p | |
|---|---|---|---|---|---|---|---|
| Age | ≤45 years | 102 (43.4) | 133 (56.6) | 0.377 | 172 (73.2) | 63 (26.8) | 0.490 |
| >45 years | 221 (46.9) | 250 (53.1) | 356 (75.6) | 115 (24.4) | |||
| Gender | Female | 280 (47.5) | 309 (52.5) | 0.032 | 451 (76.6) | 138 (23.4) | 0.014 |
| Male | 43 (36.8) | 74 (63.2) | 77 (65.8) | 40 (34.2) | |||
| Lymphocytic thyroiditis | Absent | 191 (46.5) | 220 (53.5) | 0.675 | 307 (74.7) | 104 (25.3) | 0.932 |
| Present | 132 (44.7) | 163 (55.3) | 221 (74.9) | 74 (25.1) | |||
| Primary tumor diameter | ≤10 mm | 316 (77.8) | 90 (22.2) | <0.001 | 398 (98.0) | 8 (2.0) | <0.001 |
| >10 mm | 7 (2.3) | 293 (97.7) | 130 (43.3) | 170 (56.7) | |||
| Histological subtype | CPTC | 164 (47.4) | 182 (52.6) | 0.091 | 263 (76.0) | 83 (24.0) | 0.002 |
| IFPTC | 153 (45.5) | 183 (54.5) | 255 (75.9) | 81 (24.1) | |||
| ASPTC | 6 (25.0) | 18 (75.0) | 10 (41.7) | 14 (58.3) | |||
| LVI | Absent | 317 (49.6) | 322 (50.4) | <0.001 | 493 (77.1) | 146 (22.9) | <0.001 |
| Present | 6 (9.0) | 61 (91.0) | 35 (52.2) | 32 (47.8) | |||
| PNI | Absent | 320 (46.2) | 373 (53.8) | 0.008 | 523 (75.5) | 170 (24.5) | 0.017 |
| Present | 3 (23.1) | 10 (76.9) | 5 (38.5) | 8 (61.5) | |||
| LNM | Absent | 161 (44.5) | 201 (55.5) | <0.001 | 268 (74.0) | 94 (26.0) | 0.044 |
| Present | 16 (22.2) | 56 (77.8) | 47 (65.3) | 25 (34.7) | |||
| ETE | Absent | 293 (51.8) | 273 (48.2) | <0.001 | 441 (77.9) | 125 (22.1) | <0.001 |
| Present | 30 (21.4) | 110 (78.5) | 87 (62.1) | 53 (37.9) | |||
| RAI therapy | Absent | 266 (81.6) | 60 (18.4) | <0.001 | 320 (98.2) | 6 (1.8) | <0.001 |
| Present | 57 (15.0) | 323 (85.0) | 208 (54.7) | 172 (45.3) | |||
| Recurrence | Absent | 318 (46.5) | 371 (53.5) | 0.078 | 522 (75.5) | 169 (24.5) | 0.005 |
| Present | 5 (22.7) | 17 (77.3) | 10 (40.0) | 12 (60.0) | |||
| Distant metastasis | Absent | 323 (45.8) | 382 (54.2) | 0.542 | 528 (74.9) | 177 (25.1) | 0.252 |
| Present | 0 (0.0) | 1 (100.0) | 0 (0.0) | 1 (100.0) | |||
| BRAFV600E | Wild-type | 173 (47.8) | 189 (52.2) | 0.012 | 271 (74.9) | 91 (25.1) | 0.238 |
| Mutated | 31 (33.3) | 62 (66.7) | 64 (68.8) | 29 (31.2) | |||
| Variables | PTD >10 mm Unifocal n (%) | PTD ≤10 mm TTD >10 mm Multifocal n (%) | p | PTD >10 mm Unifocal n (%) | PTD ≤10 mm TTD >20 mm Multifocal n (%) | p | |
|---|---|---|---|---|---|---|---|
| Age | ≤45 years | 53 (69.7) | 23 (30.3) | 0.011 | 53 (96.4) | 2 (3.6) | 0.284 |
| >45 years | 68 (50.7) | 66 (49.3) | 68 (91.9) | 6 (8.1) | |||
| Gender | Female | 94 (55.0) | 77 (45.0) | 0.148 | 94 (93.1) | 7 (6.9) | 1.000 |
| Male | 27 (69.2) | 12 (30.8) | 27 (96.4) | 1 (3.6) | |||
| Histological subtype | CPTC | 47 (50.0) | 47 (50.0) | 0.130 | 47 (87.0) | 7 (13.0) | 0.020 |
| IFVPTC | 71 (64.0) | 40 (36.0) | 71 (98.6) | 1 (1.4) | |||
| ASPTC | 3 (60.0) | 2 (40.0) | 3 (100.0) | 0 (0.0) | |||
| LVI | Absent | 95 (54.0) | 81 (46.0) | 0.025 | 95 (93.1) | 7 (6.9) | 0.522 |
| Present | 26 (76.5) | 8 (23.5) | 26 (96.3) | 1 (3.7) | |||
| PNI | Absent | 115 (56.7) | 88 (43.3) | 0.243 | 115 (93.5) | 8 (6.5) | 1.000 |
| Present | 6 (85.5) | 1 (14.3) | 6 (100.0) | 0 (0.0) | |||
| LNM | Absent | 59 (52.7) | 53 (47.3) | 0.136 | 59 (90.8) | 6 (9.2) | 1.000 |
| Present | 20 (66.7) | 10 (33.3) | 20 (95.2) | 1 (4.8) | |||
| ETE | Absent | 76 (52.8) | 68 (47.2) | 0.052 | 76 (93.8) | 5 (6.2) | 1.000 |
| Present | 45 (68.2) | 21 (31.8) | 45 (93.8) | 3 (6.3) | |||
| Radioactive iodine therapy | Absent | 4 (7.1) | 52 (92.9) | <0.001 | 4 (57.1) | 3 (42.9) | 0.005 |
| Present | 117 (76.0) | 37 (24.0) | 117 (95.9) | 5 (4.1) | |||
| Recurrence | Absent | 117 (57.4) | 87 (42.6) | 0.264 | 117 (93.6) | 8 (6.4) | 1.000 |
| Present | 4 (66.7) | 2 (33.3) | 4 (100.0) | 0 (0.0) | |||
| BRAFV600E | Wild-type | 48 (51.6) | 45 (48.4) | 0.128 | 48 (92.3) | 4 (7.7) | 1.000 |
| Mutated | 24 (68.6) | 11 (31.4) | 24 (92.3) | 2 (7.7) | |||
| Univariate Analyses | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Lymph Node Metastasis | Univariate | Variables | Recurrence | Univariate | ||||||
| Absent | Present | p | OR (95% CI) | Absent | Present | p | OR (95% CI) | ||||
| Age | ≤45 years | 120 (77.9) | 34 (22.1) | 0.018 | 0.537 (0.321–0.899) | Age | ≤45 years | 225 (95.7) | 10 (4.3) | 0.223 | 0.588 (0.250–1.382) |
| >45 years | 243 (86.8) | 37 (13.2) | >45 years | 459 (97.5) | 12 (2.5) | ||||||
| Gender | Female | 321 (87.2) | 47 (12.8) | <0.001 | 3.903 (2.169–7.023) | Gender | Female | 572 (97.1) | 17 (2.9) | 0.433 | 1.502 (0.543–4.155) |
| Male | 42 (63.6) | 24 (36.4) | Male | 112 (95.7) | 5 (4.3) | ||||||
| Lymphocytic thyroiditis | Absent | 184 (81.8) | 41 (18.2) | 0.277 | 0.752 (0.450–1.257) | Lymphocytic thyroiditis | Absent | 396 (96.4) | 15 (3.6) | 0.339 | 0.642 (0.258–1.594) |
| Present | 179 (85.6) | 30 (14.4) | Present | 288 (97.6) | 7 (2.4) | ||||||
| Tumor focality and laterality * | Unilateral Unifocal | 159 (84.6) | 29 (15.4) | Tumor focality and laterality ** | Unilateral Unifocal | 302 (97.7) | 7 (2.3) | ||||
| Unilateral Multifocal | 66 (82.5) | 14 (17.5) | 0.672 | 1.163 (0.578–2.341) | Unilateral Multifocal | 133 (97.8) | 3 (2.2) | 0.969 | 0.973 (0.248–3.821) | ||
| Bilateral Multifocal | 126 (81.8) | 28 (18.2) | 0.497 | 1.218 (0.689–2.153) | Bilateral Multifocal | 214 (94.7) | 12 (5.3) | 0.068 | 2.419 (0.937–6.246) | ||
| Tumor focality | Unifocal | 169 (85.4) | 29 (14.6) | 0.378 | 1.262 (0.753–2.114) | Tumor focality | Unifocal | 333 (97.9) | 7 (2.1) | 0.126 | 2.033 (0.819–5.048) |
| Multifocal | 194 (82.2) | 42 (17.8) | Multifocal | 351 (95.9) | 15 (4.1) | ||||||
| Primary tumor diameter | ≤1 cm | 211 (89.4) | 25 (10.6) | 0.001 | 2.554 (1.504–4.338) | Primary tumor diameter | ≤1 cm | 399 (98.3) | 7 (1.7) | 0.018 | 3.000 (1.208–7.452) |
| >1 cm | 152 (76.8) | 46 (23.2) | >1 cm | 285 (95.0) | 15 (5.0) | ||||||
| Tumor laterality | Unilateral | 223 (83.8) | 43 (16.2) | 0.637 | 1.134 (0.672–1.914) | Tumor laterality * | Unilateral | 433 (97.7) | 10 (2.3) | 0.044 | 2.406 (1.023–5.656) |
| Bilateral | 128 (82.1) | 28 (17.9) | Bilateral | 216 (94.7) | 12 (5.3) | ||||||
| Total tumor diameter: 10 mm | ≤10 mm | 162 (91.5) | 15 (8.5) | <0.001 | 3.009 (1.641–5.517) | Total tumor diameter: 10 mm | ≤10 mm | 318 (98.5) | 5 (1.5) | 0.035 | 2.954 (1.078–8.098) |
| >10 mm | 201 (78.2) | 56 (21.8) | >10 mm | 366 (95.6) | 17 (4.4) | ||||||
| Total tumor diameter: 20 mm | ≤20 mm | 269 (85.4) | 46 (14.6) | 0.109 | 1.555 (0.906–2.671) | Total tumor Diameter: 20 mm | ≤20 mm | 518 (98.1) | 10 (1.9) | 0.003 | 3.745 (1.589–8.824) |
| >20 mm | 94 (79.0) | 25 (21.0) | >20 mm | 166 (93.3) | 12 (6.7) | ||||||
| Total tumor diameter: 11.5 mm | ≤11.5 mm | 176 (91.7) | 17 (8.3) | <0.001 | 3.235 (1.787–5.857) | Total tumor diameter: 19.5 mm | ≤19.5 mm | 345 (98.6) | 5 (1.4) | 0.016 | 3.460 (1.262–9.484) |
| >11.5 mm | 187 (77.3) | 55 (22.7) | >19.5 mm | 339 (95.2) | 17 (4.8) | ||||||
| Histological subtype | CPTC | 183 (76.9) | 55 (23.1) | <0.001 | 0.261 (0.137–0.494) | Histological subtype | CPTC | 333 (96.2) | 13 (3.8) | 0.126 | 0.466 (0.175–1.240) |
| IFPTC | 166 (92.7) | 13 (7.3) | IFVPTC | 330 (98.2) | 6 (1.8) | ||||||
| ASPTC | 14 (82.4) | 3 (17.6) | ASPTC | 21 (87.5) | 3 (12.5) | ||||||
| LVI | Absent | 347 (92.0) | 30 (8.0) | <0.001 | 29.640 (14.901–58.956) | LVI | Absent | 626 (98.0) | 13 (2.0) | <0.001 | 7.472 (3.064–18.222) |
| Present | 16 (28.1) | 41 (71.9) | Present | 58 (86.6) | 9 (13.4) | ||||||
| PNI | Absent | 359 (84.7) | 65 (15.3) | <0.001 | 8.285 (2.275–30.170) | PNI | Absent | 673 (97.1) | 20 (2.9) | 0.024 | 6.118 (1.272–29.434) |
| Present | 4 (40.0) | 6 (60.0) | Present | 11 (84.6) | 2 (15.4) | ||||||
| ETE | Absent | 302 (91.2) | 29 (8.8) | <0.001 | 7.170 (4.148–12.395) | ETE | Absent | 555 (98.1) | 11 (1.9) | 0.001 | 4.302 (1.825–10.141) |
| Present | 61 (59.2) | 42 (40.8) | Present | 129 (92.1) | 11 (7.9) | ||||||
| BRAFV600E | Wild-type | 190 (87.2) | 28 (12.8) | 0.001 | 2.850 (1.494–5.437) | BRAFV600E | Wild-type | 354 (97.8) | 8 (2.2) | 0.016 | 3.602 (1.271–10.204) |
| Mutated | 50 (70.4) | 21 (29.6) | Mutated | 86 (92.5) | 7 (7.5) | ||||||
| Multivariate Analyses | |||||
|---|---|---|---|---|---|
| Lymph Node Metastasis | Recurrence | ||||
| Variables | p | OR (95% CI) | Variables | p | OR (95% CI) |
| Lymphovascular invasion | 0.001 | 10.305 (2.591–40.987) | Total tumor diameter: 10 mm | <0.001 | 17.912 (6.791–47.239) |
| Extrathyroidal extension | 0.013 | 4.608 (1.388–15.302) | Lymphovascular invasion | 0.004 | 12.146 (2.269–65.019) |
| Study | Year | Country | Study Group | Number of Patients Included in the Study | Suggested Cutoff Value for TTD | Follow-Up Period | Lymph Node Metastasis | Recurrence |
|---|---|---|---|---|---|---|---|---|
| Buffet et al. [73] | 2012 | France | PTMC | 1669 | >20 mm | 4.7 years (1 month–37.9 years). | NE | Significantly associated |
| Zhao et al. [26] | 2013 | China | PTMC | 212 | >10 mm | Lacking | Significantly associated | NE |
| Pyo et al. [25] | 2015 | Korea | PTMC | 384 | >10 mm | Lacking | Not associated | NE |
| Chereau et al. [74] | 2016 | Germany | PTC/PTMC | 2273 | Not suggested | 6.5 years (1–36.4 years) | NE | Significantly associated |
| Tam et al. [18] | 2016 | Turkey | PTC/PTMC | 912 | >10 mm | 37 months (6–99 months) | Significantly associated | NE |
| Wang et al. [42] | 2017 | China | PTC | 1084 | Not suggested | Lacking | Significantly associated | NE |
| Xue et al. [72] | 2017 | China | PTMC | 97 | >10 mm | >10 years for 89 patients | NE | Significantly associated |
| Feng et al. [34] | 2020 | China | PTC | 442 | >10 mm | 43 months (11–99 months) | Significantly associated | Significantly associated |
| Manso et al. [75] | 2020 | Italy | PTC | 370 | ≥40 mm | 69 months (42–92 months) | Not reported | Significantly associated |
| Hitu et al. [76] | 2021 | Romania | PTMC | 82 | >10 mm | Lacking | Significantly associated | NE |
| Jiang et al. [77] | 2022 | China | PTMC | 560 | >10 mm | Lacking | Significantly associated | NE |
| Kwon et al. [78] | 2022 | Korea | PTC | 1288 | Not suggested | 6.4 years (4.4–8.7 years) | Not reported | Significantly associated |
| Wu et al. [62] | 2023 | China | PTC | 1936 | Not suggested | Not reported | Significantly associated | Not reported |
| The present study; Can et al. | 2023 | Turkey | PTC/PTMC | 706 | >10 mm | 112 months (82–240 months) | Significantly associated | Significantly associated |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Can, N.; Bulbul, B.Y.; Ozyilmaz, F.; Sut, N.; Mercan, M.A.; Andaç, B.; Celik, M.; Tastekin, E.; Guldiken, S.; Sezer, Y.A.; et al. The Impact of Total Tumor Diameter on Lymph Node Metastasis and Tumor Recurrence in Papillary Thyroid Carcinomas. Diagnostics 2024, 14, 272. https://doi.org/10.3390/diagnostics14030272
Can N, Bulbul BY, Ozyilmaz F, Sut N, Mercan MA, Andaç B, Celik M, Tastekin E, Guldiken S, Sezer YA, et al. The Impact of Total Tumor Diameter on Lymph Node Metastasis and Tumor Recurrence in Papillary Thyroid Carcinomas. Diagnostics. 2024; 14(3):272. https://doi.org/10.3390/diagnostics14030272
Chicago/Turabian StyleCan, Nuray, Buket Yilmaz Bulbul, Filiz Ozyilmaz, Necdet Sut, Meltem Ayyıldız Mercan, Burak Andaç, Mehmet Celik, Ebru Tastekin, Sibel Guldiken, Yavuz Atakan Sezer, and et al. 2024. "The Impact of Total Tumor Diameter on Lymph Node Metastasis and Tumor Recurrence in Papillary Thyroid Carcinomas" Diagnostics 14, no. 3: 272. https://doi.org/10.3390/diagnostics14030272
APA StyleCan, N., Bulbul, B. Y., Ozyilmaz, F., Sut, N., Mercan, M. A., Andaç, B., Celik, M., Tastekin, E., Guldiken, S., Sezer, Y. A., Salt, S. A., Erdoğan, E. G., Ustun, F., & Gurkan, H. (2024). The Impact of Total Tumor Diameter on Lymph Node Metastasis and Tumor Recurrence in Papillary Thyroid Carcinomas. Diagnostics, 14(3), 272. https://doi.org/10.3390/diagnostics14030272