
Associated Anomalies and Outcome in Patients with Prenatal Diagnosis of Aortic Arch Anomalies as Aberrant Right Subclavian Artery, Right Aortic Arch and Double Aortic Arch


 , and
, and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Chromosomal Anomalies in AAAs
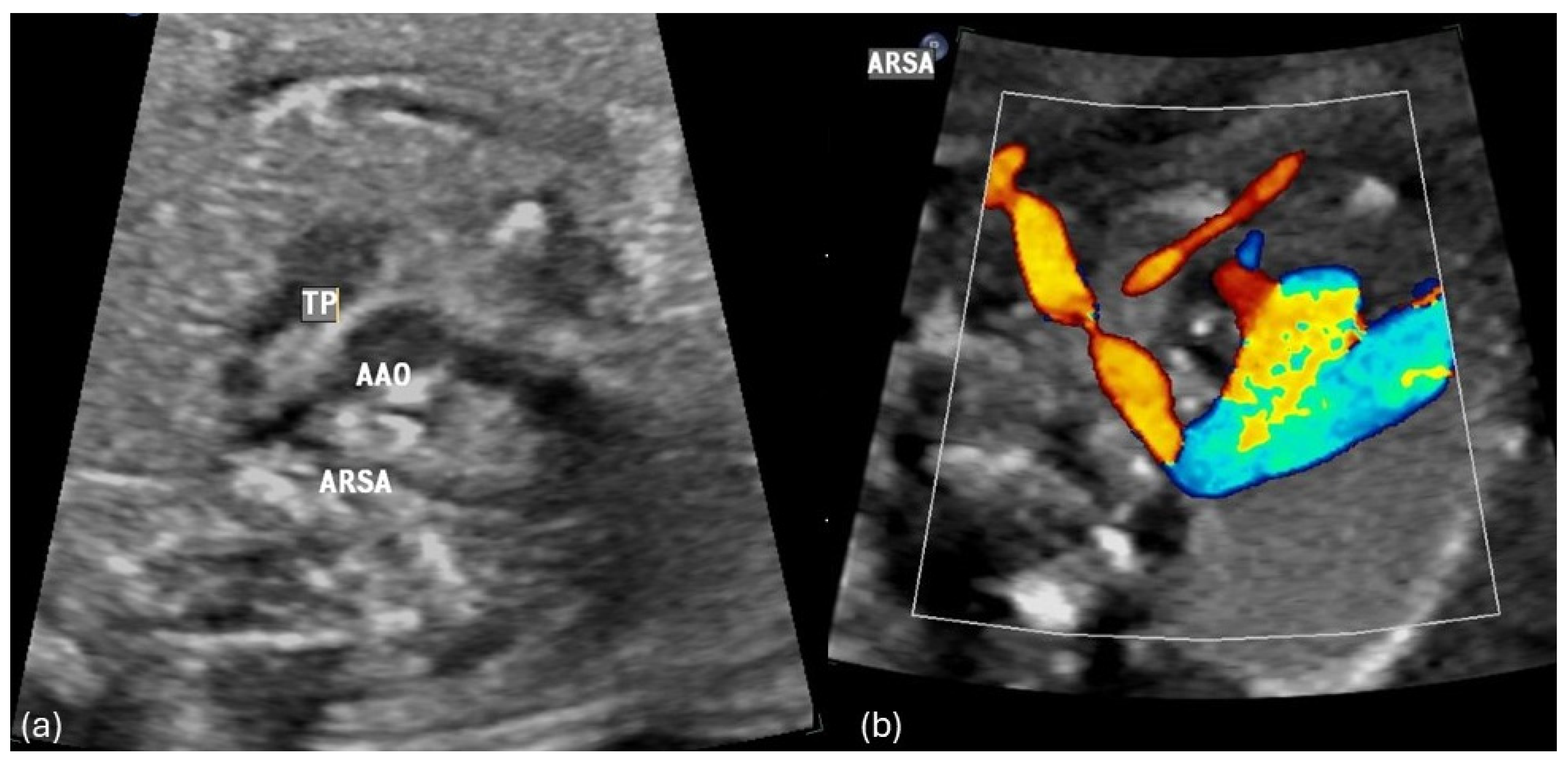
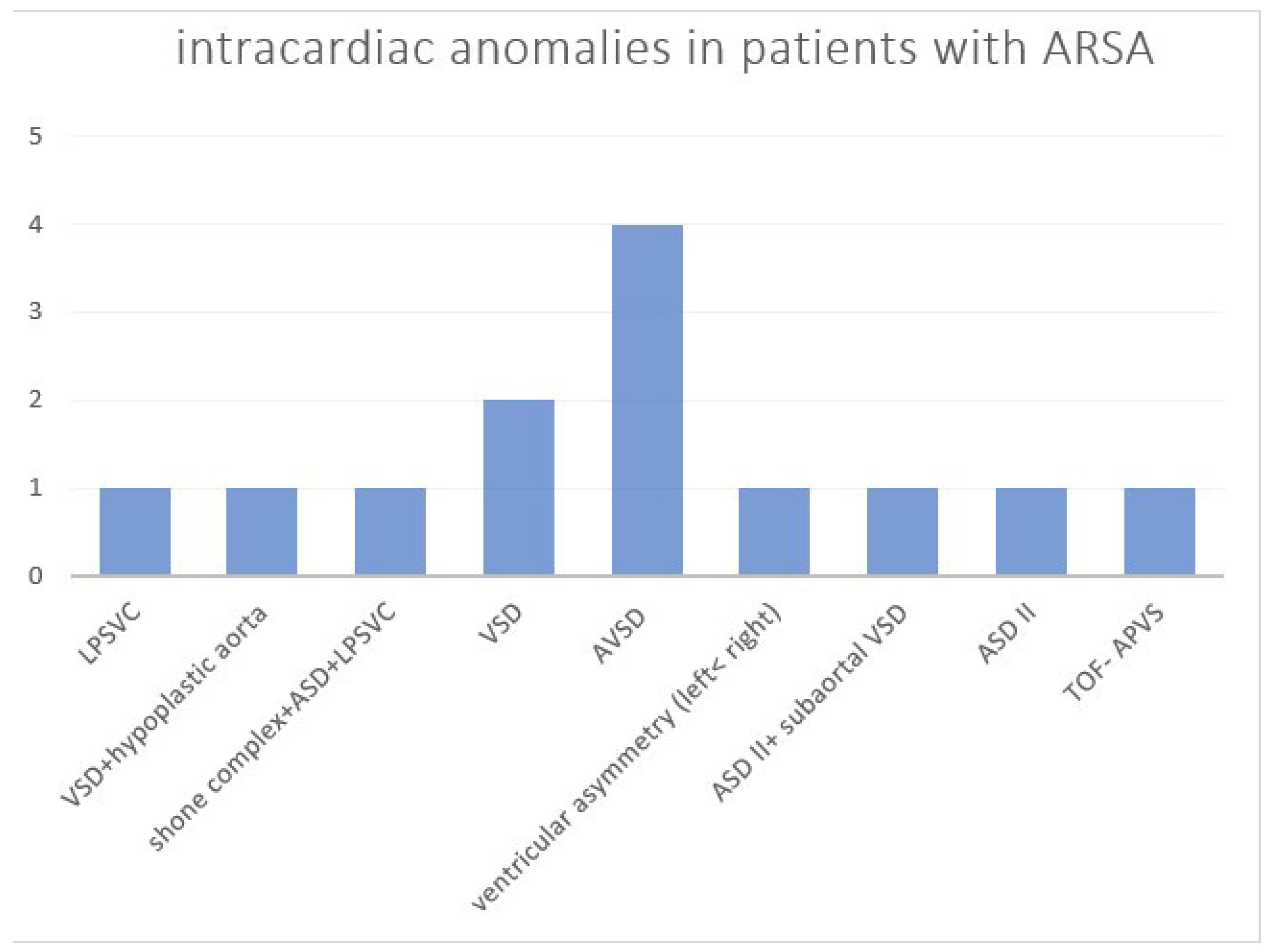
3.2. Associated Intracardiac Anomalies in AAAs
3.3. Associated Extracardiac Anomalies in AAA
3.4. Isolated AAAs
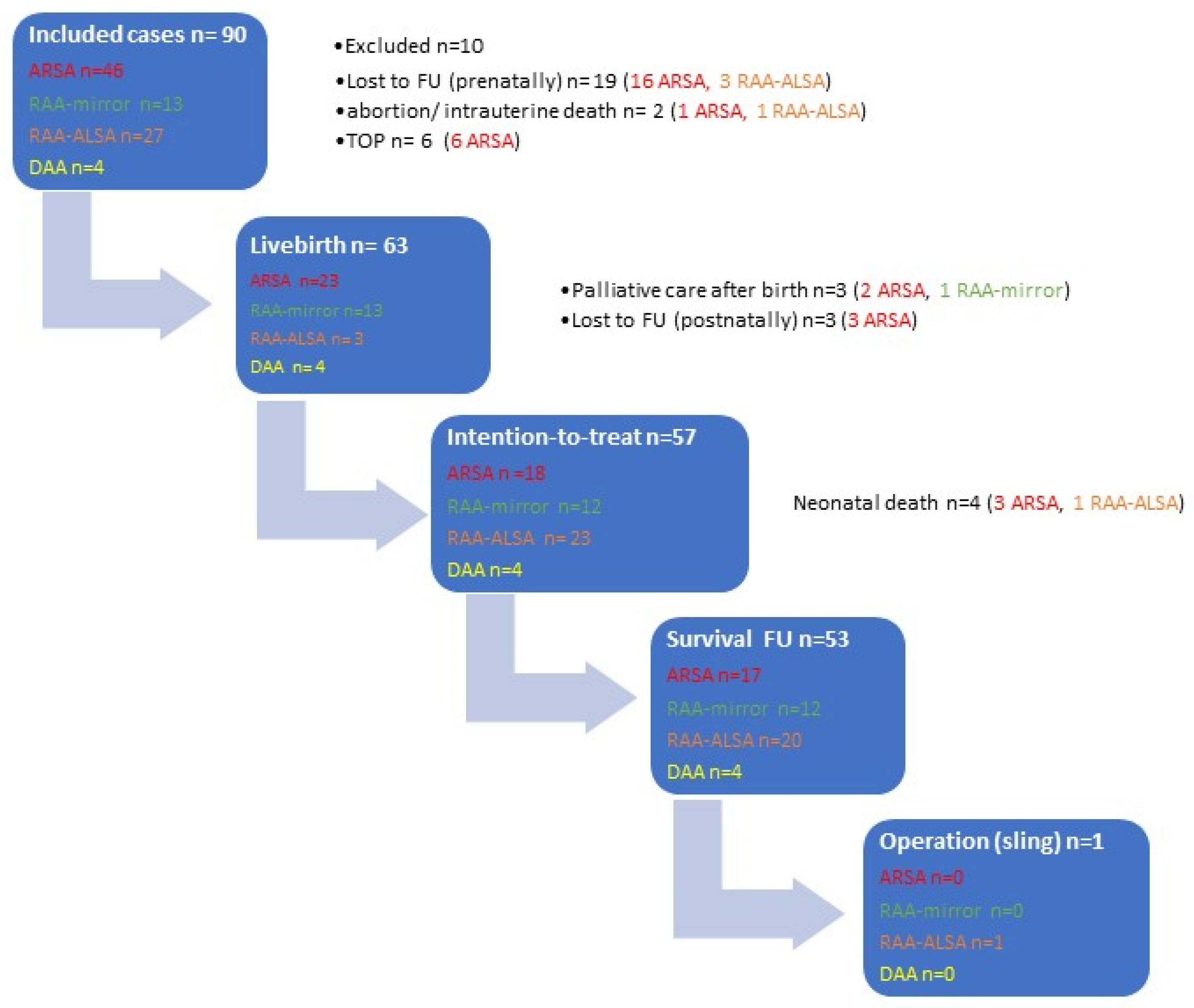
3.5. Prenatal Outcome in AAAs
3.6. Postnatal Outcome in AAAs
4. Discussion
4.1. AAA Diagnostics of AAA and Accuracy Rate
4.2. ARSA-Isolated versus Non-Isolated Forms
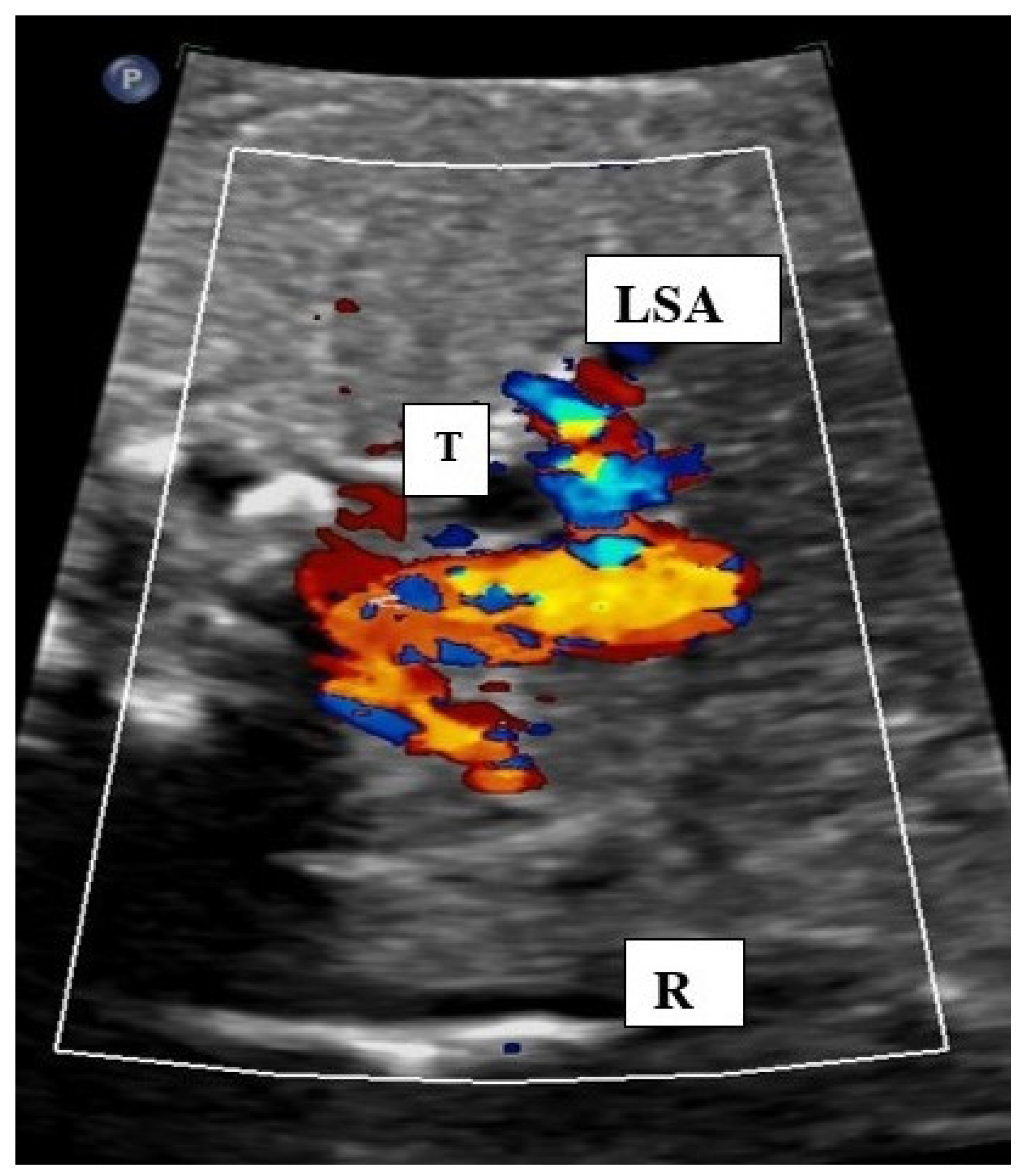
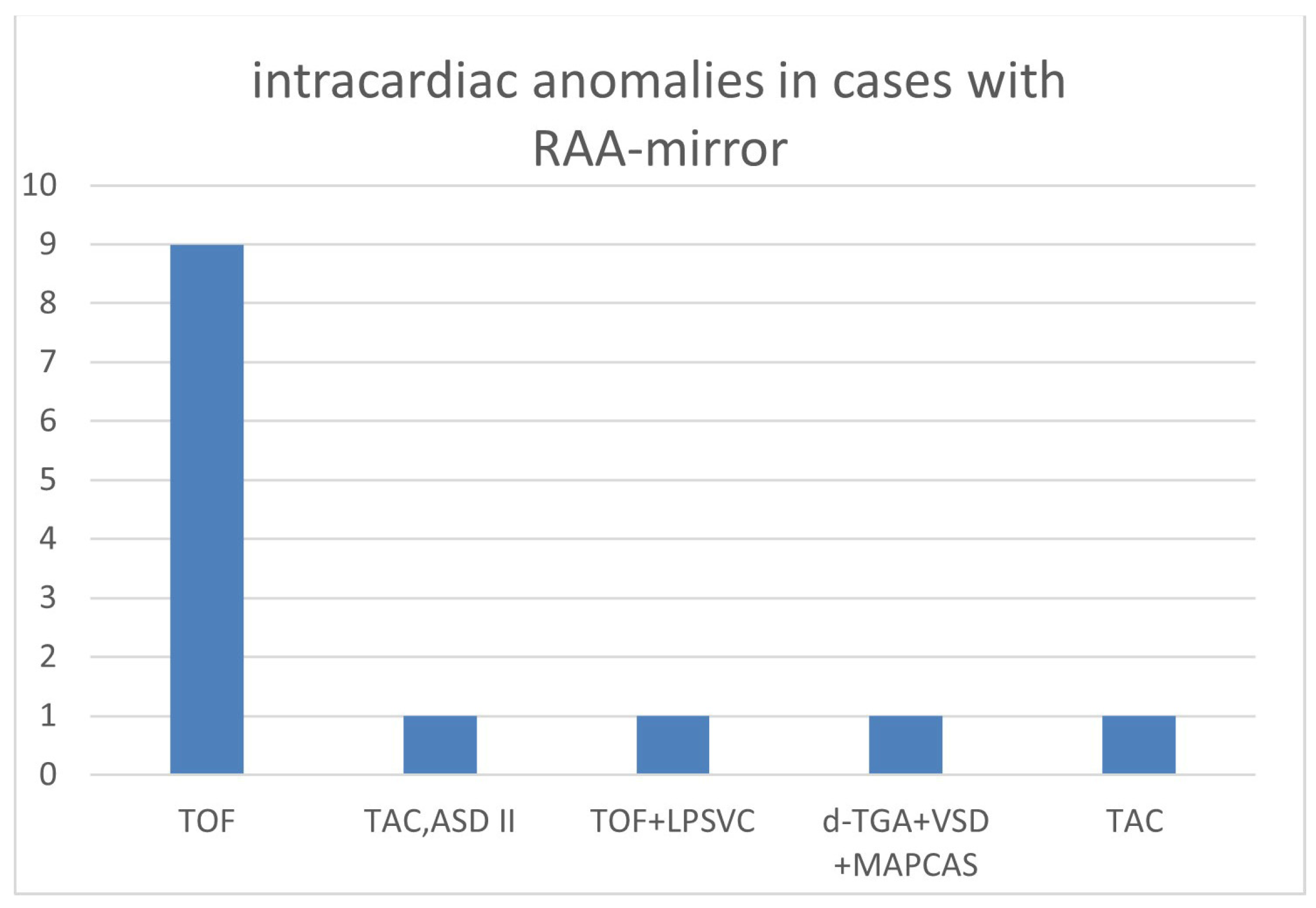
4.3. Associated Anomalies in RAA
4.4. Symptoms of Vascular Ring/Sling in AAA
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Edwards, J.E. Vascular rings related to anomalies of the aortic arches. Mod. Concepts Cardiovasc. Dis. 1948, 17, 1. [Google Scholar] [PubMed]
- Edwards, J. Malformations of the aortic arch system manifested as vascular rings—PubMed. Lab. Investig. 1953, 2, 56–75. [Google Scholar]
- Schleich, J. Images in cardiac embryology: Development of the human heart: Days 15–21. Heart 2002, 87, 487. [Google Scholar] [CrossRef] [PubMed]
- Kau, T.; Sinzig, M.; Gasser, J.; Lesnik, G.; Rabitsch, E.; Celedin, S.; Eicher, W.; Illiasch, H.; Hausegger, K. Aortic development and anomalies. Semin. Interv. Radiol. 2007, 24, 141–152. [Google Scholar] [CrossRef] [PubMed]
- Tuo, G.; Volpe, P.; Bava, G.; Bondanza, S.; De Robertis, V.; Pongiglione, G.; Marasini, M. Prenatal diagnosis and outcome of isolated vascular rings. Am. J. Cardiol. 2009, 10, 416–419. [Google Scholar] [CrossRef]
- Berg, C.; Bender, F.; Soukup, M.; Geipel, A.; Axt-Fliedner, R.; Breuer, J.; Herberg, U.; Gembruch, U. Right aortic arch detected in fetal life. Ultrasound Obs. Gynecol. 2006, 28, 882–889. [Google Scholar] [CrossRef]
- Galindo, A.; Nieto, O.; Nieto, M.; Rodríguez-Martín, O.; Herraiz, I.; Escribano, D.; Granados, M. Prenatal diagnosis of right aortic arch: Associated findings, pregnancy outcome, and clinical significance of vascular rings. Prenat. Diagn. 2009, 29, 975–981. [Google Scholar] [CrossRef]
- Yaron, R.; Berant, M.; Fogelman, R.; Gabriel, A.; Birk, E. Prenatal diagnosis and outcome of right aortic arch without significant intracardiac anomaly. J. Am. Soc. Echocardiogr. 2014, 27, 1352–1358. [Google Scholar]
- De León-Luis, J.; Gámez, F.; Bravo, C.; Tenías, J.; Arias, Á.; Pérez, R.; Maroto, E.; Aguarón, Á.; Ortiz-Quintana, L. Second-trimester fetal aberrant right subclavian artery: Original study, systematic review and meta-analysis of performance in detection of Down syndrome. Ultrasound Obs. Gynecol. 2014, 44, 147–153. [Google Scholar] [CrossRef]
- Hastreiter, A.; ID’Cruz, I.; Cantez, T.; Namin, E.; Licata, R. Right-sided aorta. I. Occurrence of right aortic arch in various types of congenital heart disease. II. Right aortic arch, right descending aorta, and associated anomalies. Br. Heart J. 1966, 28, 722–739. [Google Scholar] [CrossRef]
- Achiron, R.; Rotstein, Z.; Heggesh, J.; Bronshtein, M.; Zimand, S.; Lipitz, S.; Yagel, S. Anomalies of the fetal aortic arch: A novel sonographic approach to in-utero diagnosis. Ultrasound Obs. Gynecol. 2002, 20, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Bravo, C.; Gámez, F.; Pérez, R.; Álvarez, T.; De León-Luis, J. Fetal Aortic Arch Anomalies: Key Sonographic Views for Their Differential Diagnosis and Clinical Implications Using the Cardiovascular System Sonographic Evaluation Protocol. J. Ultrasound Med. 2016, 35, 237–251. [Google Scholar] [CrossRef] [PubMed]
- Zapata, H.; Edwards, J.E.; Titus, J.L. Aberrant right subclavian artery with left aortic arch: Associated cardiac anomalies. Pediatr. Cardiol. 1993, 14, 159–161. [Google Scholar] [CrossRef]
- Lo, N.; Leung, P.; Lau, K.; Yeung, C. Congenital cardiovascular malformations in Chinese children with Down’s syndrome. Chin. Med. J. 1989, 102, 382–386. [Google Scholar]
- Goldstein, W.B. Aberrant right subclavian artery in mongolism. Am. J. Roentgenol. Radium Ther. Nucl. Med. 1965, 95, 131–134. [Google Scholar] [CrossRef] [PubMed]
- Chaoui, R.; Heling, K.S.; Sarioglu, N.; Schwabe, M.; Dankof, A.; Bollmann, R. Aberrant right subclavian artery as a new cardiac sign in second- and third-trimester fetuses with Down syndrome. Am. J. Obs. Gynecol. 2005, 192, 257–263. [Google Scholar] [CrossRef]
- Zalel, Y.; Achiron, R.; Yagel, S.; Kivilevitch, Z. Fetal aberrant right subclavian artery in normal and Down syndrome fetuses. Ultrasound Obs. Gynecol. 2008, 31, 25–29. [Google Scholar] [CrossRef]
- Trobo, D.; Bravo, .C.; Alvarez, T.; Pérez, R.; Gámez, F.; De León-Luis, J. Prenatal Sonographic Features of a Double Aortic Arch: Literature Review and Perinatal Management. J. Ultrasound Med. 2015, 34, 1921–1927. [Google Scholar] [CrossRef]
- Guo, Q.; Kong, Y.; Zeng, S.; Zhou, J.; Wang, X.; Shang, Q.; Zhou, J.; Yuan, H.; Wang, L.; Tong, L.; et al. Fetal double aortic arch: Prenatal sonographic and postnatal computed tomography angiography features, associated abnormalities and clinical outcomes. BMC Pregnancy Childbirth 2020, 20, 614. [Google Scholar] [CrossRef]
- Kent, P.; Poterucha, T. Images in clinical medicine. Aberrant Right Subclavian Artery Dysphagia Lusoria. N. Engl. J. Med. 2002, 346, 1637. [Google Scholar] [CrossRef]
- Rosa, P.; Gillespie, D.L.; Goff, J.M.; O’Donnell, S.D.; Starnes, B. Aberrant right subclavian artery syndrome: A case of chronic cough. J. Vasc. Surg. 2003, 37, 1318–1321. [Google Scholar] [CrossRef] [PubMed]
- Turner, A.; Gavel, G.; Coutts, J. Vascular rings—Presentation, investigation and outcome. Eur. J. Pediatr. 2005, 164, 266–270. [Google Scholar] [CrossRef] [PubMed]
- McLaren, C.; Elliott, M.; Derek, J. Vascular compression of the airway in children. Paediatr. Respir. Rev. 2008, 9, 85–94. [Google Scholar] [CrossRef]
- McElhinney, D.B.; Clark, B.J.; Weinberg, P.M.; Kenton, M.L.; McDonald-McGinn, D.; Driscoll, D.A.; Zackai, E.H.; Goldmuntz, E. Association of chromosome 22q11 deletion with isolated anomalies of aortic arch laterality and branching. J. Am. Coll. Cardiol. 2001, 37, 2114–2119. [Google Scholar] [CrossRef] [PubMed]
- Zidere, V.; Tsapakis, E.; Huggon, I.; Allan, L. Right aorticarch in the fetus. Ultrasound Obs. Gynecol. 2006, 28, 876–881. [Google Scholar] [CrossRef] [PubMed]
- Babu, R.; Pierro, A.; Spitz, D.; Drake, P.; Kiely, E.M. The management of oesophageal atresia in neonates with right-sided aortic arch. J. Pediatr. Surg. 2000, 35, 56–58. [Google Scholar] [CrossRef] [PubMed]
- Pico, H.; Mancini, J.; Lafouge, A.; Bault, J.P.; Gorincour, G.; Quarello, E. Prenatal Associated Features in Fetuses Diagnosed with an Aberrant Right Subclavian Artery. Fetal Diagn. Ther. 2016, 40, 187–194. [Google Scholar] [CrossRef]
- Ranzini, A.; Hyman, F.; Jamaer, E.; van Mieghem, T. Aberrant Right Subclavian Artery: Correlation Between Fetal and Neonatal Abnormalities and Abnormal Genetic Screening or Testing. J. Ultrasound Med. 2017, 36, 785–790. [Google Scholar] [CrossRef]
- Chaoui, R.; Thiel, G.; Heling, K. Prevalence of an aberrant right subclavian artery (ARSA) in normal fetuses: A new soft marker for trisomy 21 risk assessment. Ultrasound Obs. Gynecol. 2005, 26, 356. [Google Scholar] [CrossRef]
- Willruth, A.M.; Dwinger, N.; Ritgen, J.; Stressig, R.; Geipel, A.; Gembruch, U.; Berg, C. Fetal aberrant right subclavian artery (ARSA)—A potential new soft marker in the genetic scan? Ultraschall Med. 2012, 33, 114–118. [Google Scholar] [CrossRef]
- Gul, A.; Corbacioglu, A.; Bakirci, I.T.; Ceylan, Y. Associated anomalies and outcome of fetal aberrant right subclavian artery. Arch. Gynecol. Obstet. 2012, 285, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Paladini, D.; Sglavo, G.; Pastore, G.; Masucci, A.; D’Armiento, M.; Nappi, C. Aberrant right subclavian artery: Incidence and correlation with other markers of Down syndrome in second-trimester fetuses. Ultrasound Obs. Gynecol. 2012, 39, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Scala, C.; Leone Roberti Maggiore, U.; Candiani, M.; Venturini, P.; Ferrero, S.; Greco, T.; Cavoretto, P. Aberrant right subclavian artery in fetuses with Down syndrome: A systematic review and meta-analysis. Ultrasound Obs. Gynecol. 2015, 46, 266–276. [Google Scholar] [CrossRef] [PubMed]
- Vigneswaran Jabak, S.; Syngelaki, A.; Charakida, M.; Simpson, J.; Nicolaides, K.; Zidere, V. Prenatal incidence of isolated right aortic arch and double aortic arch. J. Matern. Fetal Neonatal Med. 2021, 34, 2985–2990. [Google Scholar] [CrossRef] [PubMed]
- Rauch, R.; Rauch, A.; Koch, A.; Zink, S.; Kaulitz, R.; Girisch, M.; Singer, H.; Hofbeck, M. Laterality of the aortic arch and anomalies of the subclavian artery—Reliable indicators for 22q11.2 deletion syndromes? Eur. J. Pediatr. 2004, 163, 642–645. [Google Scholar] [CrossRef]
- Carles, D.; Pelluard, F.; André, G.; Nocart, N.; Sauvestre, F. Aberrant right subclavian artery (arteria lusoria) and the risk for trisomy 21. Retrospective study of 11,479 fetopathological examinations. J. Gynecol. Obs. Biol. Reprod. 2014, 43, 698–703. [Google Scholar] [CrossRef]
- Yoo, S.; Min, J.; Lee, Y.; Roman, K.; Jaeggi, E.; Smallhorn, J. Fetal sonographic diagnosis of aortic arch anomalies. Ultrasound Obs. Gynecol. 2003, 22, 535–546. [Google Scholar] [CrossRef]
- D’Antonio, F.; Khalil, A.; Zidere, V.; Carvalho, J. Fetuses with right aortic arch: A multicenter cohort study and meta-analysis. Ultrasound Obs. Gynecol. 2016, 47, 423–432. [Google Scholar] [CrossRef]
- Ludwig, A.K.; Ludwig, M. Schwangerschaften nach assistierter Reproduktion. In Reproduktionsmedizin; Diedrich, K., Ludwig, M., Griesinger, G., Eds.; Springer: Berlin/Heidelberg, Germany, 2018; pp. 1–18. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | Twin Pregnancy | ART (IVF/ ICSI) | Genetic Anomalies | NT >95 Percentile | Intracardiac Anomalies | Extracardiac Anomalies | Isolated (No Other Malformation) | Genetic Anomalies within Isolated Cases | |
|---|---|---|---|---|---|---|---|---|---|
| ARSA | 46 | 5 (10.9%) | 3 (6.5%) | 17 (37.0%) | 9 (19.6%) | 13 (28.3%) | 13 (28.3%) | 26 (56.5%) | 3/26 (11.5%) |
| RAA-mirror | 13 | 1 (7.7%) | 3 (23.1%) | 1 (7.7%) | 0 (0%) | 13 (100%) | 4 (30.7%) | 0 (0%) | 0 (0%) |
| RAA-ALSA | 27 | 2 (7.4%) | 2 (7.4%) | 1 (3,7%) | 0 (0%) | 10 (37.0%) | 6 (22.2%) | 13 (48.1%) | 0 (0%) |
| DAA | 4 | 0 (0%) | 1 (25%) | 0 (0%) | 0 (0%) | 0 (0%) | 1 (25%) | 3 (75%) | 0 (0%) |
| all | 90 | 8 (8.9%) | 9 (10.0%) | 19 (21.1%) | 9 (10%) | 36 (40.0%) | 24 (26.7%) | 42 (46.7) | 3/42 (7.1%) |
| ARSA 13 Patients | RAA-Mirror 4 Patients | RAA-ALSA 6 Patients | DAA 1 Patient |
|---|---|---|---|
| pes eqinovarus (T21) plexus cyst n = 2 hemivertebra megacisterna magna, hypoplastic cerebellar vermis, cleft palate (T18) omphalocele, esophageal atresia, hand deformity, pes equinovarus (T18) single umbilical artery, hydrops fetalis (T18) single umbilical artery double kidney, edema (turner) microcephaly (T21) hypospadia, preauricular appendage duodenal atresia (mosaic T21) appendage right hand, muscular gap proximal to umbilicus (microdeletion 22q11.2) | equinovarus, hydrocephalus, macrocephaly, cerebellar hypoplasia microtia, glaucoma, nevus flammeus (face), angioma (supratentorial) (GNAQ chromosome 9 mutation) hydronephrosis, megaureter, dysplastic ear left esophageal atresia, renal agenesis, Madelung’s deformity left hand, anal atresia with rectovaginal fistula (VACTERL) | syndactyly left hand (III/IV), feet deformity cleft lip radial polydactyly, preauricular fistula, preauricular appendage microcephaly n = 2 (one case with microdeletion 22q11.2) meningomyelocele + renal agenesis | hypospadia |
| n | Invasive Testing | NIPT (Without Further Invasive Testing) | Abnormal Result | Outcome in Abnormal Results | Outcome in Patients with Normal Karyotype/Normal NIPT | Outcome Patients without Prenatal Testing/Invasive Testing | |
|---|---|---|---|---|---|---|---|
| ARSA | 26 | 6/26 (23.1%) 3 of them with high-risk NIPT for T21 and subsequent amniocentesis | 7 | 3/26 (11.5%) | 1 lost to FU prenatally, 2 TOP | 5 lost to FU prenatally 3 lost to FU postpartum 2 livebirths with FU | 5 lost to FU prenatally; 8 livebirths with FU |
| RAA-mirror | 0 | - | - | - | - | - | - |
| RAA-ALSA | 13 | 2/13 (15.4%) | 2 (Both without testing for microdeletion) | 0 | - | 4 livebirths with FU | 6 livebirths 1 IUD 29 + 4 wks in a monochorionic twin with sFGR 2 lost to FU prenatally |
| DAA | 3 | 0/3 (0%) | 0 | 0 | - | - | 3 livebirths, no operation during FU |
| Reference | Cohort | ARSA (Total) | ARSA (Total) with Chromosomal Anomalies | Isolated ARSA | Isolated ARSA with Chromosomal Anomalies |
|---|---|---|---|---|---|
| Chaoui et al., 2005 [16] | 14 fetuses with trisomy 21 (HR) | 5 | 5 | 1 | 1 |
| Gul et al., 2011 [31] | 4125 fetuses (LR) | 17 | 1 | 9 | 1 |
| Paladini et al., 2012 [32] | 106 fetuses with trisomy 21 (HR) | 27 | 27 | 8 | 8 |
| Pico et al., 2016 [27] | 120 fetuses with ARSA (108 with outcome) (M) | 108 | 22 (9 with T 21) | 54 | 0 |
| Ranzini et al., 2017 [28] | 79 fetuses with ARSA (M) | 79 | 11 (7 with T 21) | 43 | 0 |
| Willruth et al., 2012 [30] | 1337 fetuses (M) | 14 | 3 (1 × T21) | 9 | 0 |
| Zalel et al., 2008 [17] | 924 fetuses (M) | 16 | 3 (3 × T21) | 6 | 0 |
| our results | 46 fetuses with ARSA (M) | 46 | 17 (7 × T21) | 26 | 3 |
| Reference | Cohort | FU Time (Months) | Operation (Vascular Ring/Sling) |
|---|---|---|---|
| Achiron et al., 2002 [11] | 19 fetuses with vascular ring/sling | 60 (median) | 1/19 (5.3%) (DAA case) |
| Guo et al., 2020 [19] | 40 fetuses with DAA, 27 live births with DAA | 38 ± 17 (mean) | 11/27 (41%) |
| Tuo et al., 2009 [5] | 19 fetuses with vascular ring/sling | 23.4 (mean) | 4/19 (21.1%) (3 × DAA, 1 × RAA-ALSA) |
| Berg et al., 2006 [6] | 71 fetuses, 28 with vascular ring/sling | minimum 12 for each case | 1/25 (3.6%) (DAA case) |
| Our results | 41 livebirths with vascular ring | 10.5 (median) | 1/41 (2.4%) (RAA-ALSA case) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Axt-Fliedner, R.; Nazar, A.; Bedei, I.; Schenk, J.; Reitz, M.; Rupp, S.; Jux, C.; Wolter, A. Associated Anomalies and Outcome in Patients with Prenatal Diagnosis of Aortic Arch Anomalies as Aberrant Right Subclavian Artery, Right Aortic Arch and Double Aortic Arch. Diagnostics 2024, 14, 238. https://doi.org/10.3390/diagnostics14030238
Axt-Fliedner R, Nazar A, Bedei I, Schenk J, Reitz M, Rupp S, Jux C, Wolter A. Associated Anomalies and Outcome in Patients with Prenatal Diagnosis of Aortic Arch Anomalies as Aberrant Right Subclavian Artery, Right Aortic Arch and Double Aortic Arch. Diagnostics. 2024; 14(3):238. https://doi.org/10.3390/diagnostics14030238
Chicago/Turabian StyleAxt-Fliedner, Roland, Asia Nazar, Ivonne Bedei, Johanna Schenk, Maleen Reitz, Stefan Rupp, Christian Jux, and Aline Wolter. 2024. "Associated Anomalies and Outcome in Patients with Prenatal Diagnosis of Aortic Arch Anomalies as Aberrant Right Subclavian Artery, Right Aortic Arch and Double Aortic Arch" Diagnostics 14, no. 3: 238. https://doi.org/10.3390/diagnostics14030238
APA StyleAxt-Fliedner, R., Nazar, A., Bedei, I., Schenk, J., Reitz, M., Rupp, S., Jux, C., & Wolter, A. (2024). Associated Anomalies and Outcome in Patients with Prenatal Diagnosis of Aortic Arch Anomalies as Aberrant Right Subclavian Artery, Right Aortic Arch and Double Aortic Arch. Diagnostics, 14(3), 238. https://doi.org/10.3390/diagnostics14030238