
The Comparison of Accuracy of Post Space Digital Impressions Made by Three Different Intraoral Scanners: An In Vitro Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Size Determination
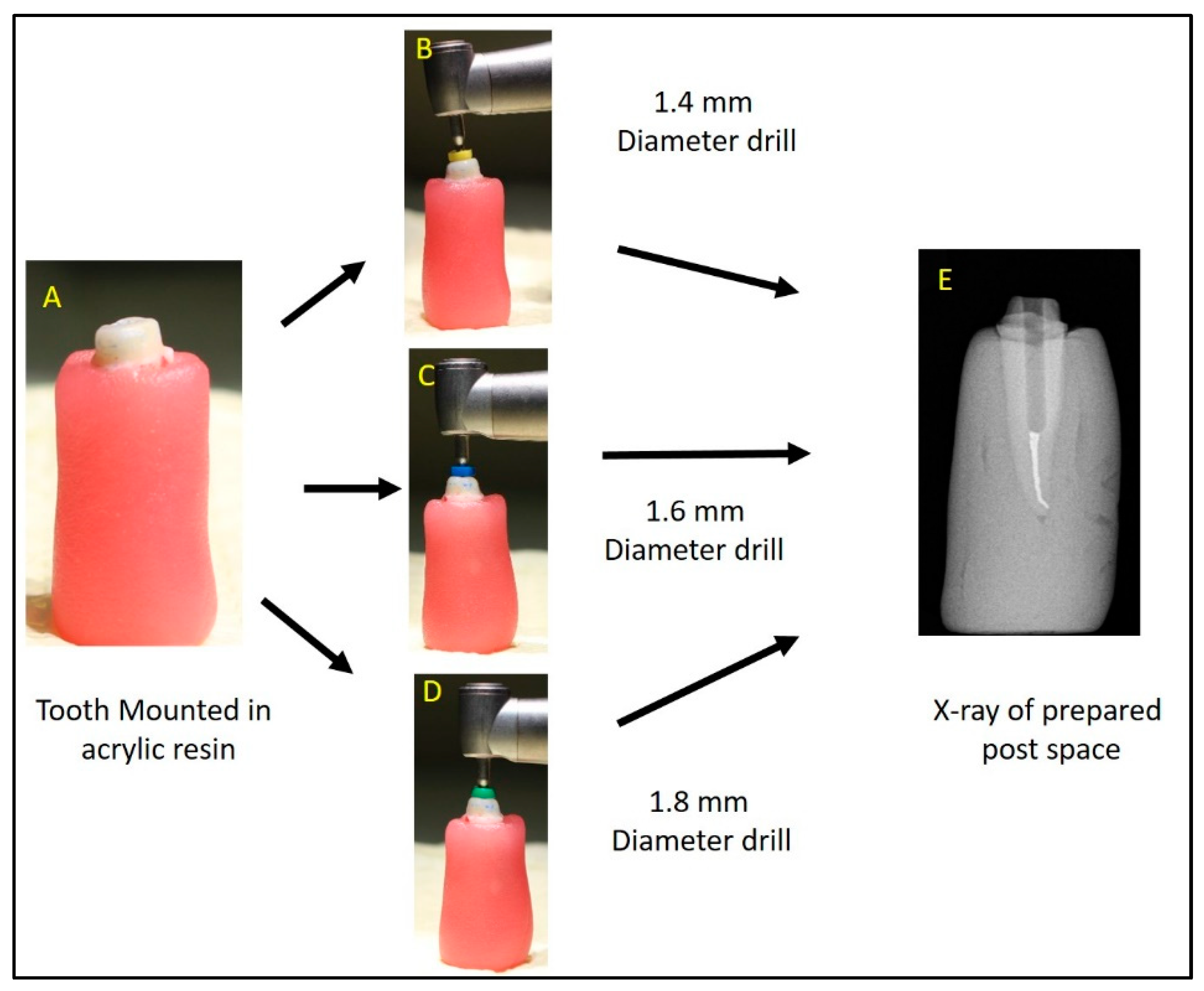
2.2. Digital Acquisition of the Post Space Using IOS
2.3. Acquisition of Post Space Impression Using Extra Oral Scanner as the Reference Group
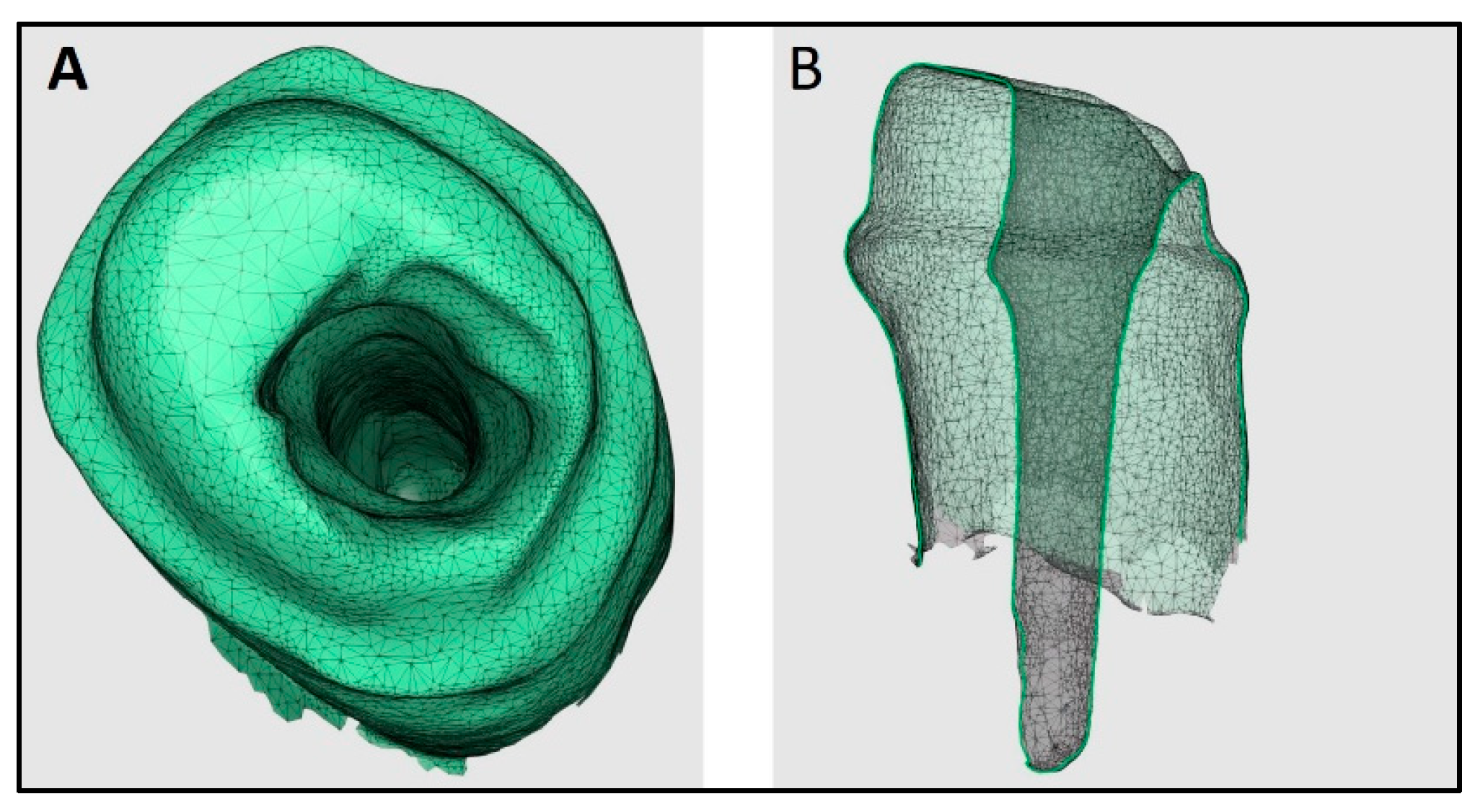
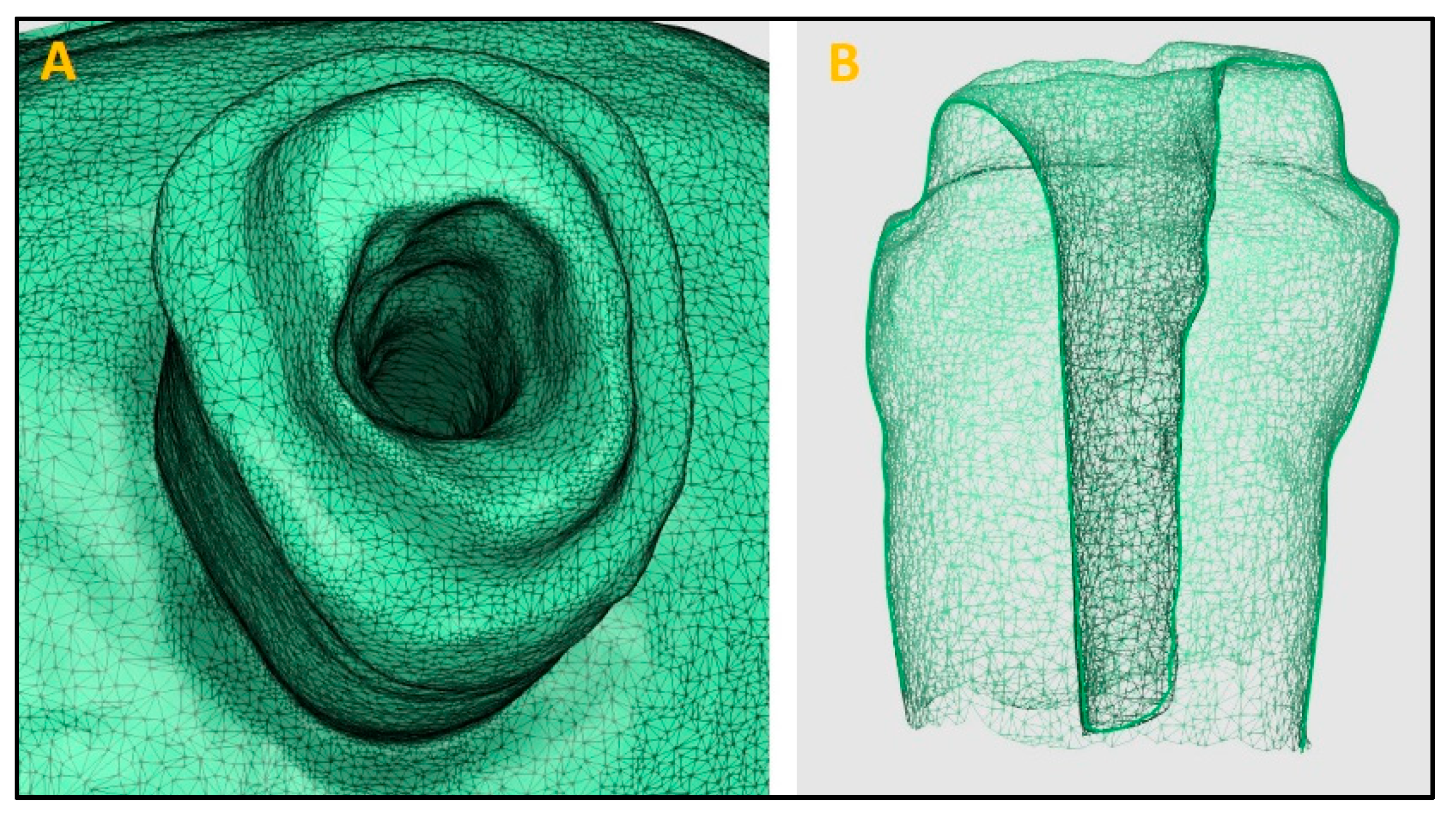
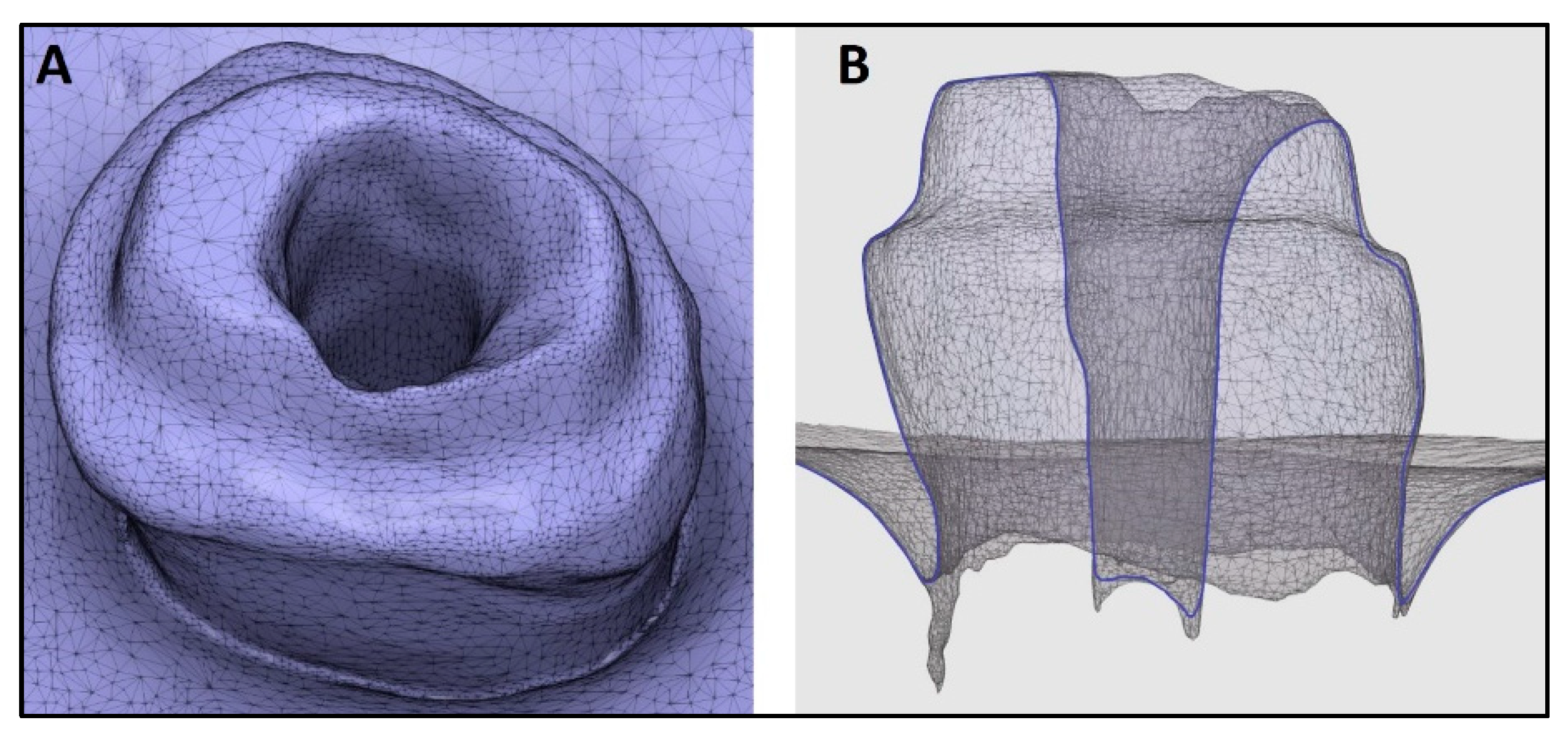
2.4. Superimposition of STL Files
2.5. Statistical Analysis
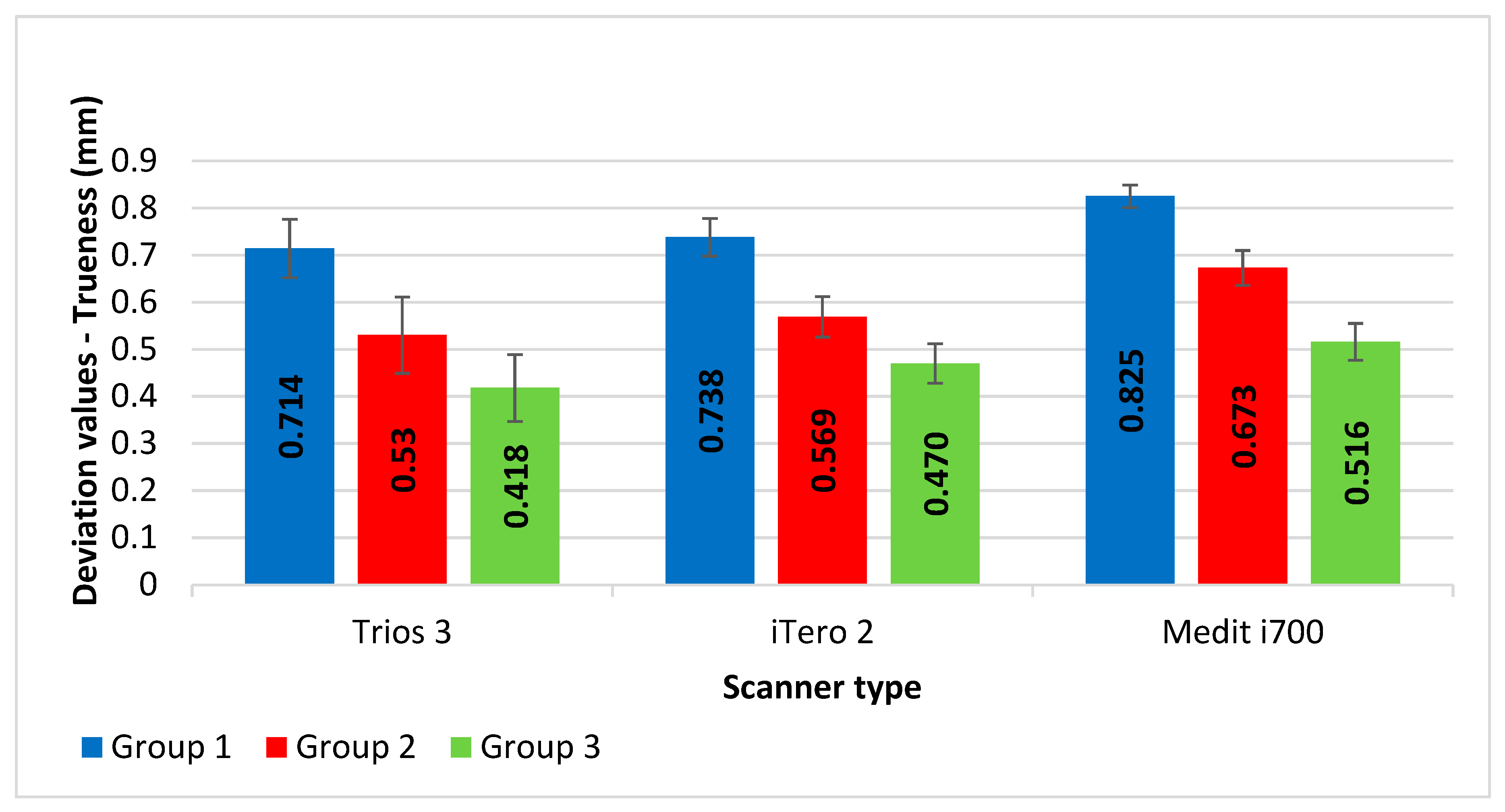
3. Results
4. Discussion
5. Conclusions
- Trios3 IOS has higher accuracy (as it exhibited minimal deviation for trueness) in recording post space, followed by iTero2 and Mediti700 IOS.
- As the diameter of the post space is increased, the accuracy of recording by IOS increases.
- For all the tested IOSs (except for the use of Trios3 IOS and iTero IOS, in post space with 1.8 mm canal diameter), the deviations in trueness were higher than the clinically acceptable limits. Thus, IOSs should be used cautiously when recording impressions of post spaces.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tang, W.; Wu, Y.; Smales, R.J. Identifying and reducing risks for potential fractures in endodontically treated teeth. J. Endod. 2010, 36, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Al-Omiri, M.K.; Mahmoud, A.A.; Rayyan, M.R.; Abu-Hammad, O. Fracture resistance of teeth restored with post-retained restorations: An overview. J. Endod. 2010, 36, 1439–1449. [Google Scholar] [CrossRef] [PubMed]
- Hendi, A.R.; Moharrami, M.; Siadat, H.; Hajmiragha, H.; Alikhasi, M. The effect of conventional, half-digital, and full-digital fabrication techniques on the retention and apical gap of post and core restorations. J. Prosthet. Dent. 2019, 121, 364.e1–364.e6. [Google Scholar] [CrossRef] [PubMed]
- Plotino, G.; Grande, N.M.; Bedini, R.; Pameijer, C.H.; Somma, F. Flexural properties of endodontic posts and human root dentin. Dent. Mater. 2007, 23, 1129–1135. [Google Scholar] [CrossRef] [PubMed]
- Vichi, A.; Ferrari, M.; Davidson, C.L. Influence of ceramic and cement thickness on the masking of various types of opaque posts. J. Prosthet. Dent. 2000, 83, 412–417. [Google Scholar] [CrossRef]
- Lamichhane, A.; Xu, C.; Zhang, F.Q. Dental fiber-post resin base material: A review. J. Adv. Prosthodont. 2014, 6, 60–65. [Google Scholar] [CrossRef]
- Teixeira, K.N.; Duque, T.M.; Maia, H.P.; Gonçalves, T. Fracture Resistance and Failure Mode of Custom-made Post-and-cores of Polyetheretherketone and Nano-ceramic Composite. Oper. Dent. 2020, 45, 506–515. [Google Scholar] [CrossRef]
- Gomes, G.M.; Monte-Alto, R.V.; Santos, G.O.; Fai, C.K.; Loguercio, A.D.; Gomes, O.M.; Gomes, J.C.; Reis, A. Use of a Direct Anatomic Post in a Flared Root Canal: A Three-year Follow-up. Oper. Dent. 2016, 41, E23–E28. [Google Scholar] [CrossRef]
- Grandini, S.; Sapio, S.; Simonetti, M. Use of anatomic post and core for reconstructing an endodontically treated tooth: A case report. J. Adhes. Dent. 2003, 5, 243–247. [Google Scholar]
- Choudhary, S.; Choudhary, P.; Tripathi, S.; Begum, Z. Comparative evaluation of retention of prefabricated and conventional cast post: An in vitro study. J. Int. Soc. Prev. Community Dent. 2014, 4, 87–91. [Google Scholar] [CrossRef]
- Morgano, S.M.; Milot, P. Clinical success of cast metal posts and cores. J. Prosthet. Dent. 1993, 70, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Cheung, W. A review of the management of endodontically treated teeth. Post, core and the final restoration. J. Am. Dent. Assoc. 2005, 136, 611–619. [Google Scholar] [CrossRef]
- Bergman, B.; Lundquist, P.; Sjögren, U.; Sundquist, G. Restorative and endodontic results after treatment with cast posts and cores. J. Prosthet. Dent. 1989, 61, 10–15. [Google Scholar] [CrossRef]
- Ni, C.W.; Chang, C.H.; Chen, T.Y.F.; Chuang, S.F. A multiparametric evaluation of post-restored teeth with simulated bone loss. J. Mech. Behav. Biomed. Mater. 2011, 4, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Milot, P.; Stein, R.S. Root fracture in endodontically treated teeth related to post selection and crown design. J. Prosthet. Dent. 1992, 68, 428–435. [Google Scholar] [CrossRef]
- Rayyan, M.R.; Roa’a, A.A.; Alsadun, S.F.; Hijazy, F.R. Accuracy of cast posts fabricated by the direct and the indirect techniques. J. Prosthet. Dent. 2016, 116, 411–415. [Google Scholar] [CrossRef]
- Sabbak, S.A. Indirect fabrication of multiple post-and-core patterns with a vinyl polysiloxane matrix. J. Prosthet. Dent. 2002, 88, 555–557. [Google Scholar] [CrossRef]
- De Vico, G.; Ferraris, F.; Arcuri, L.; Guzzo, F.; Spinelli, D. A novel workflow for computer guided implant surgery matching digital dental casts and CBCT scan. ORAL Implantol. 2016, 9, 33–48. [Google Scholar]
- Ender, A.; Mehl, A. Full arch scans: Conventional versus digital impressions-an in-vitro study. Int. J. Comput. Dent. 2011, 14, 11–21. [Google Scholar]
- Awad, M.A.; Marghalani, T.Y. Fabrication of a custom made ceramic post and core using CAD-CAM technology. J. Prosthet. Dent. 2007, 98, 161–162. [Google Scholar] [CrossRef]
- Liu, P.; Deng, X.-L.; Wang, X.-Z. Use of a CAD/CAM-fabricated glass fiber post and core to restore fractured anterior teeth: A clinical report. J. Prosthet. Dent. 2010, 103, 330–333. [Google Scholar] [CrossRef] [PubMed]
- Pinto, A.; Arcuri, L.; Carosi, P.; Nardi, R.; Libonati, A.; Ottria, L.; Campanella, V. In vitro evaluation of the post-space depth reading with an intraoral scanner (IOS) compared to a traditional silicon impression. ORAL Implantol. 2017, 10, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Al-Qarni, F.D. Customized post and cores fabricated with CAD/CAM technology: A literature review. Int. J. Gen. Med. 2022, 6, 4771–4779. [Google Scholar] [CrossRef] [PubMed]
- Moustapha, G.; AlShwaimi, E.; Silwadi, M.; Ounsi, H.; Ferrari, M.; Salameh, Z. Marginal and internal fit of CAD/CAM fiber post and cores. Int. J. Comput. Dent. 2019, 22, 45–53. [Google Scholar] [PubMed]
- Abduo, J.; Elseyoufi, M. Accuracy of intraoral scanners: A systematic review of influencing factors. Eur. J. Prosthodont. Restor. Dent. 2018, 26, 101–121. [Google Scholar]
- Almalki, A.; Conejo, J.; Wünsche, A.; Anadioti, E.; Blatz, M.B. Digital smile design and fabrication of CAD/CAM restorations in a complex esthetic case. Compend. Contin. Educ. Dent. 2022, 43, 664–688. [Google Scholar]
- Al-Hassiny, A.; Végh, D.; Bányai, D.; Végh, Á.; Géczi, Z.; Borbély, J.; Hermann, P.; Hegedüs, T. User experience of intraoral scanners in dentistry: Transnational questionnaire study. Int. Dent. J. 2023, 73, 754–759. [Google Scholar] [CrossRef]
- Bandiaky, O.N.; Le Bars, P.; Gaudin, A.; Hardouin, J.B.; Cheraud-Carpentier, M.; Mbodj, E.B.; Soueidan, A. Comparative assessment of complete-coverage, fixed tooth-supported prostheses fabricated from digital scans or conventional impressions: A systematic review and meta-analysis. J. Prosthet. Dent. 2022, 127, 71–79. [Google Scholar] [CrossRef]
- Eggmann, F.; Blatz, M.B. Recent Advances in Intraoral Scanners. J. Dent. Res. 2024, 103, 1349–1357. [Google Scholar] [CrossRef]
- Logozzo, S.; Zanetti, E.M.; Franceschini, G.; Kilpelä, A.; Mäkynen, A. Recent advances in dental optics–Part I: 3D intraoral scanners for restorative dentistry. Opt. Lasers Eng. 2014, 54, 203–221. [Google Scholar] [CrossRef]
- Mizumoto, R.M.; Yilmaz, B. Intraoral scan bodies in implant dentistry: A systematic review. J. Prosthet. Dent. 2018, 120, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Ting-shu, S.; Jian, S. Intraoral digital impression technique: A review. J. Prosthodont. 2015, 24, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.G.; Veronesi, G.; Hauschild, U.; Mijiritsk, E.; Mangano, C. Trueness and precision of four intraoral scanners in oral implantology: A comparative in vitro study. PLoS ONE 2016, 11, e0163107. [Google Scholar] [CrossRef] [PubMed]
- Imburgia, M.; Logozzo, S.; Hauschild, U.; Veronesi, G.; Mangano, C.; Mangano, F.G. Accuracy of four intraoral scanners in oral implantology: A comparative in vitro study. BMC Oral Health 2017, 17, 92. [Google Scholar] [CrossRef] [PubMed]
- Bilgin, M.S.; Erdem, A.; Dilber, E.; Ersoy, I. Comparison of fracture resistance between cast, CAD/CAM milling, and direct metal laser sintering metal post systems. J. Prosthodont. Res. 2016, 60, 23–28. [Google Scholar] [CrossRef]
- Van Noort, R. The future of dental devices is digital. Dent. Mater. 2012, 28, 3–12. [Google Scholar] [CrossRef]
- Joda, T.; Gintaute, A.; Brägger, U.; Ferrari, M.; Weber, K.; Zitzmann, N.U. Time-efficiency and cost-analysis comparing three digital workflows for treatment with monolithic zirconia implant fixed dental prostheses: A double-blinded RCT. J. Dent. 2021, 113, 103779. [Google Scholar] [CrossRef]
- Safrany-Fark, A.; Laczi, B.; Nagy, A.; Lengyel, L.; Piffko, J.; Segatto, E. A novel approach for determining instantaneous centers of rotation of the mandible with an intraoral scanner: A preliminary study. PLoS ONE 2023, 18, e0285162. [Google Scholar] [CrossRef]
- Kihara, H.; Hatakeyama, W.; Komine, F.; Takafuji, K.; Takahashi, T.; Yokota, J.; Oriso, K.; Kondo, H. Accuracy and practicality of intraoral scanner in dentistry: A literature review. J. Prosthodont. Res. 2020, 64, 109–113. [Google Scholar] [CrossRef]
- Anadioti, E.; Aquilino, S.A.; Gratton, D.G.; Holloway, J.A.; Denry, I.L.; Thomas, G.W.; Qian, F. Internal fit of pressed and computer-aided design/computer-aided manufacturing ceramic crowns made from digital and conventional impressions. J. Prosthet. Dent. 2015, 113, 304–309. [Google Scholar] [CrossRef]
- Tamam, E.; Bankoğlu Güngör, M.; Karakoca Nemli, S.; Bilecenoğlu, B.; Ocak, M. Effect of different preparation finishing procedures on the marginal and internal fit of CAD-CAM-produced restorations: A microcomputed tomography evaluation. J. Prosthet. Dent. 2023, 130, 605–610. [Google Scholar] [CrossRef] [PubMed]
- Kanduti, D.; Korat, L.; Kosec, T.; Legat, A.; Ovsenik, M.; Kopač, I. Comparison Between Accuracy of Posts Fabricated Using a Digital CAD/CAM Technique and a Conventional Direct Technique. Int. J. Prosthodont. 2021, 34, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Elter, B.; Diker, B.; Tak, Ö. The trueness of an intraoral scanner in scanning different post space depths. J. Dent. 2022, 127, 104352. [Google Scholar] [CrossRef] [PubMed]
- Almalki, A.; Conejo, J.; Kutkut, N.; Blatz, M.; Hai, Q.; Anadioti, E. Evaluation of the accuracy of direct intraoral scanner impressions for digital post and core in various post lengths: An in-vitro study. J. Esthet. Restor. Dent. 2024, 36, 673–679. [Google Scholar] [CrossRef] [PubMed]
- Emam, M.; Ghanem, L.; Abdel Sadek, H.M. Effect of different intraoral scanners and post-space depths on the trueness of digital impressions. Dent. Med. Probl. 2024, 61, 577–584. [Google Scholar] [CrossRef]
- Taha, N.M.; Zohdy, M.M.; Fattah, G.A. Effect of different intraoral scanners on the trueness of custom post space scans with two different cervical diameters. Int. J. Appl. Dent. Sci. 2024, 10, 38–43. [Google Scholar] [CrossRef]
- Lee, K.M. Comparison of two intraoral scanners based on three-dimensional surface analysis. Prog. Orthod. 2018, 19, 6. [Google Scholar] [CrossRef]
- Dupagne, L.; Mawussi, B.; Tapie, L.; Lebon, N. Comparison of the measurement error of optical impressions obtained with four intraoral and one extra-oral dental scanners of post and core preparations. Heliyon 2023, 9, e13235. [Google Scholar] [CrossRef]
- Yilmaz, B.; Marques, V.R.; Donmez, M.B.; Cuellar, A.R.; Lu, W.E.; Abou-Ayash, S.; Çakmak, G. Influence of 3D analysis software on measured deviations of CAD-CAM resin crowns from virtual design file: An in-vitro study. J. Dent. 2022, 118, 103933. [Google Scholar] [CrossRef]
- Gurpinar, B.; Tak, O. Effect of pulp chamber depth on the accuracy of endocrown scans made with different intraoral scanners versus an industrial scanner: An in vitro study. J. Prosthet. Dent. 2022, 127, 430–437. [Google Scholar] [CrossRef]
- Yang, X.; Lv, P.; Liu, Y.; Si, W.; Feng, H. Accuracy of Digital Impressions and Fitness of Single Crowns Based on Digital Impressions. Materials 2015, 8, 3945–3957. [Google Scholar] [CrossRef]
- Diker, B.; Tak, Ö. Comparing the accuracy of six intraoral scanners on prepared teeth and effect of scanning sequence. J. Adv. Prosthodont. 2020, 12, 299–306. [Google Scholar] [CrossRef]
- Medina-Sotomayor, P.; Pascual-Moscardo, A.; Camps, A.I. Accuracy of 4 digital scanning systems on prepared teeth digitally isolated from a complete dental arch. J. Prosthet. Dent. 2019, 121, 811–820. [Google Scholar] [CrossRef]
- McLean, J.W.; von Fraunhofer, J.A. The estimation of cement film thickness by an in vivo technique. Br. Dent. J. 1971, 131, 107–111. [Google Scholar] [CrossRef]
- Perdigão, J.; Gomes, G.; Augusto, V. The effect of dowel space on the bond strengths of fiber posts. J. Prosthodont. 2007, 16, 154–164. [Google Scholar] [CrossRef]
- Moshonov, J.; Slutzky-Goldberg, I.; Gottlieb, A.; Peretz, B. The effect of the distance between post and residual gutta-percha on the clinical outcome of endodontic treatment. J. Endod. 2005, 31, 177–179. [Google Scholar] [CrossRef]
- Leven, R.; Schmidt, A.; Binder, R.; Kampschulte, M.; Vogler, J.; Wöstmann, B.; Schlenz, M.A. Accuracy of Digital Impression Taking with Intraoral Scanners and Fabrication of CAD/CAM Posts and Cores in a Fully Digital Workflow. Materials 2022, 15, 4199. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Materials/Instrument | Company Details | Lot Number |
|---|---|---|
| Rotary Files | Protaper Gold, Dentsply Maillefer, Ballaigues, Switzerland | 1461889 |
| Gutta-percha | DiaDent group International, Chungcheongbuk-do, Republic of Korea | 010321 |
| Post Drills | Relyx Fiber Post drills, 3M, ESPE, Neuss, Germany | 372580 |
| Pattern Resin | GC America INC, Alsip, IL, USA. | 907231 |
| 3Shape E2 lab scanner | 3Shape, Copenhagen, Denmark | (21)-1UB2048014B |
| Trios 3 Intra Oral Scanner | 3Shape, Copenhagen, Denmark | 1C1843S01861B |
| iTero Element™ 2 Intra Oral Scanner | Align Technology, Inc., Tempe, Arizona | BLX2019W45A645 |
| MEDIT i700 wireless Intra Oral Scanner | MEDIT 2024 Intraoral Scanners and Dental SoftwareSeoul, Republic of Korea | BF2301100612 |
| Software | Medit Link 3.3.2 and Medit design 2.1.4, Medit Corp., Seoul, Republic of Korea | - |
| Groups | Trios3 Mean (±SD) | iTero2 Mean (±SD) | Medit i700 Mean (±SD) | Mean Square | F | p Value a |
|---|---|---|---|---|---|---|
| Group 1 | 0.714 (±0.062) | 0.738 (±0.081) | 0.825 (±0.071) | 0.034 | 8.651 | 0.0023 |
| Group 2 | 0.530 (±0.040) | 0.569 (±0.043) | 0.673 (±0.042) | 0.055 | 39.778 | <0.0001 |
| Group 3 | 0.418 (±0.024) | 0.470 (±0.037) | 0.516 (±0.039) | 0.024 | 22.888 | <0.0001 |
| Mean square | 0.223 | 0.183 | 0.240 | |||
| F | 111.503 | 55.831 | 86.359 | |||
| p value b | <0.0001 | <0.0001 | <0.0001 |
| Groups | Mean Difference | Std. Error | p-Value | |
|---|---|---|---|---|
| Group 1 | Trios3 vs. iTero2 | 0.024 | 0.03317 | 0.4930 |
| Trios3 vs. Medit i700 | 0.111 | 0.02669 | 0.0024 | |
| iTero2 vs. Medit i700 | 0.088 | 0.02381 | 0.0051 | |
| Group 2 | Trios3 vs. iTero2 | 0.039 | 0.01673 | 0.0430 |
| Trios3 vs. Medit i700 | 0.143 | 0.01520 | <0.0001 | |
| iTero vs. Medit i700 | 0.104 | 0.01783 | 0.0002 | |
| Group 3 | Trios3 vs. iTero2 | 0.052 | 0.01538 | 0.0082 |
| Trios3 vs. Medit i700 | 0.097 | 0.01256 | <0.0001 | |
| iTero2 vs. Medit i700 | 0.045 | 0.01506 | 0.0146 |
| Scanner Type | Mean Difference | Std. Error | p-Value | |
|---|---|---|---|---|
| Trios3 | Group 1 vs. Group 2 | 0.184 | 0.019997 | <0.0001 |
| Group 1 vs. Group 3 | 0.296 | 0.019997 | <0.0001 | |
| Group 2 vs. Group 3 | 0.111 | 0.019997 | <0.0001 | |
| iTero2 | Group 1 vs. Group 2 | 0.168 | 0.025594 | <0.0001 |
| Group 1 vs. Group 3 | 0.268 | 0.025594 | <0.0001 | |
| Group 2 vs. Group 3 | 0.099 | 0.025594 | 0.0025 | |
| Medit i700 | Group 1 vs. Group 2 | 0.152 | 0.023559 | <0.0001 |
| Group 1 vs. Group 3 | 0.310 | 0.023559 | <0.0001 | |
| Group 2 vs. Group 3 | 0.158 | 0.023559 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meshni, A.A.; Jain, S.; Osaysi, H.N.M.; Hezam, K.N.; Adlan, S.S.G. The Comparison of Accuracy of Post Space Digital Impressions Made by Three Different Intraoral Scanners: An In Vitro Study. Diagnostics 2024, 14, 2893. https://doi.org/10.3390/diagnostics14242893
Meshni AA, Jain S, Osaysi HNM, Hezam KN, Adlan SSG. The Comparison of Accuracy of Post Space Digital Impressions Made by Three Different Intraoral Scanners: An In Vitro Study. Diagnostics. 2024; 14(24):2893. https://doi.org/10.3390/diagnostics14242893
Chicago/Turabian StyleMeshni, Abdullah A., Saurabh Jain, Hanan Nasser Marie Osaysi, Khadijah Nasser Hezam, and Samar Samir Gomaan Adlan. 2024. "The Comparison of Accuracy of Post Space Digital Impressions Made by Three Different Intraoral Scanners: An In Vitro Study" Diagnostics 14, no. 24: 2893. https://doi.org/10.3390/diagnostics14242893
APA StyleMeshni, A. A., Jain, S., Osaysi, H. N. M., Hezam, K. N., & Adlan, S. S. G. (2024). The Comparison of Accuracy of Post Space Digital Impressions Made by Three Different Intraoral Scanners: An In Vitro Study. Diagnostics, 14(24), 2893. https://doi.org/10.3390/diagnostics14242893