

Risk of Secondary Cancer after Adjuvant Tamoxifen Treatment for Ductal Carcinoma In Situ: A Nationwide Cohort Study in South Korea

 , ,
, ,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
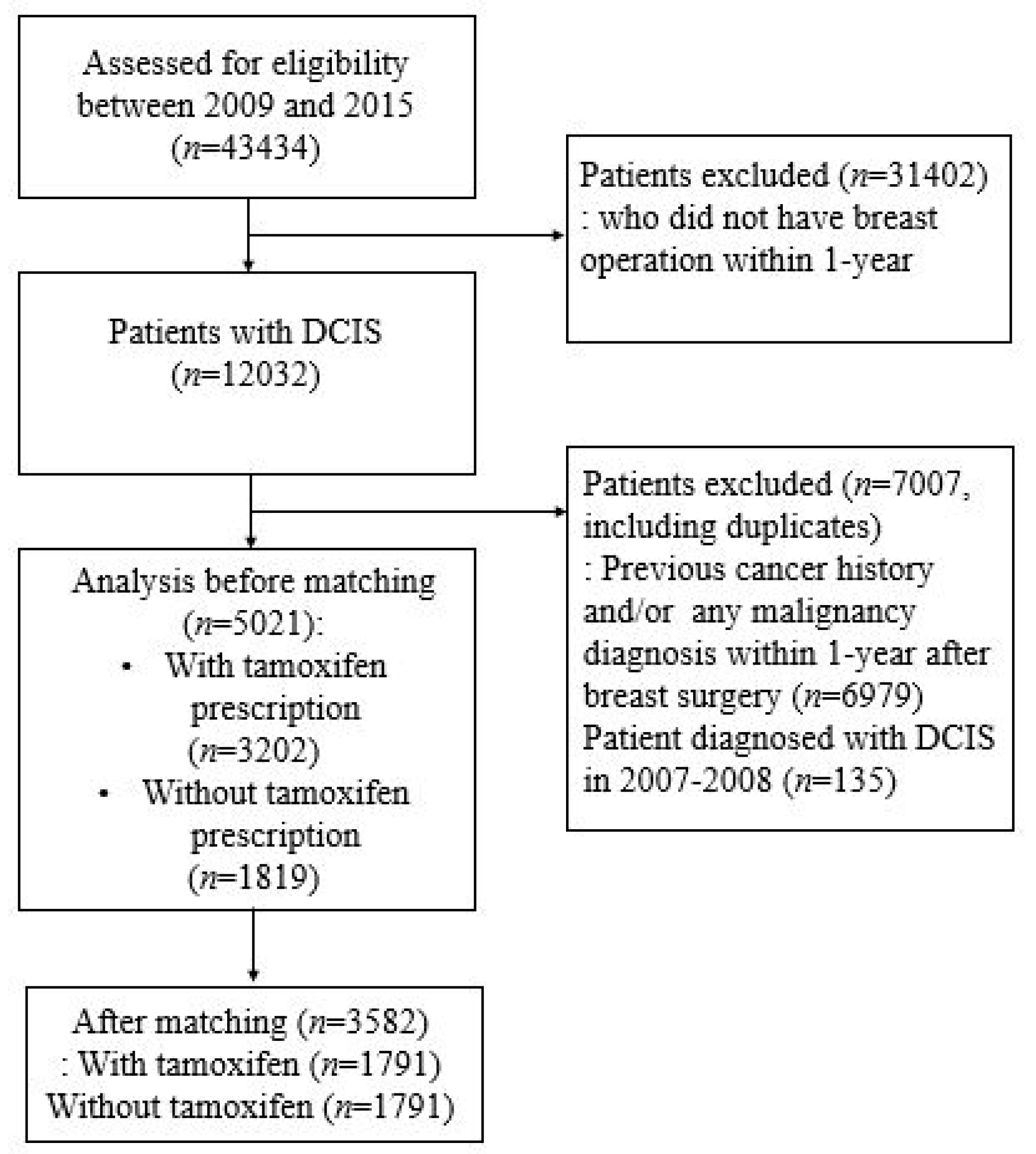
3.1. Patient Cohort
3.2. Demographic Characteristics and Incidence of Second Primary Cancer
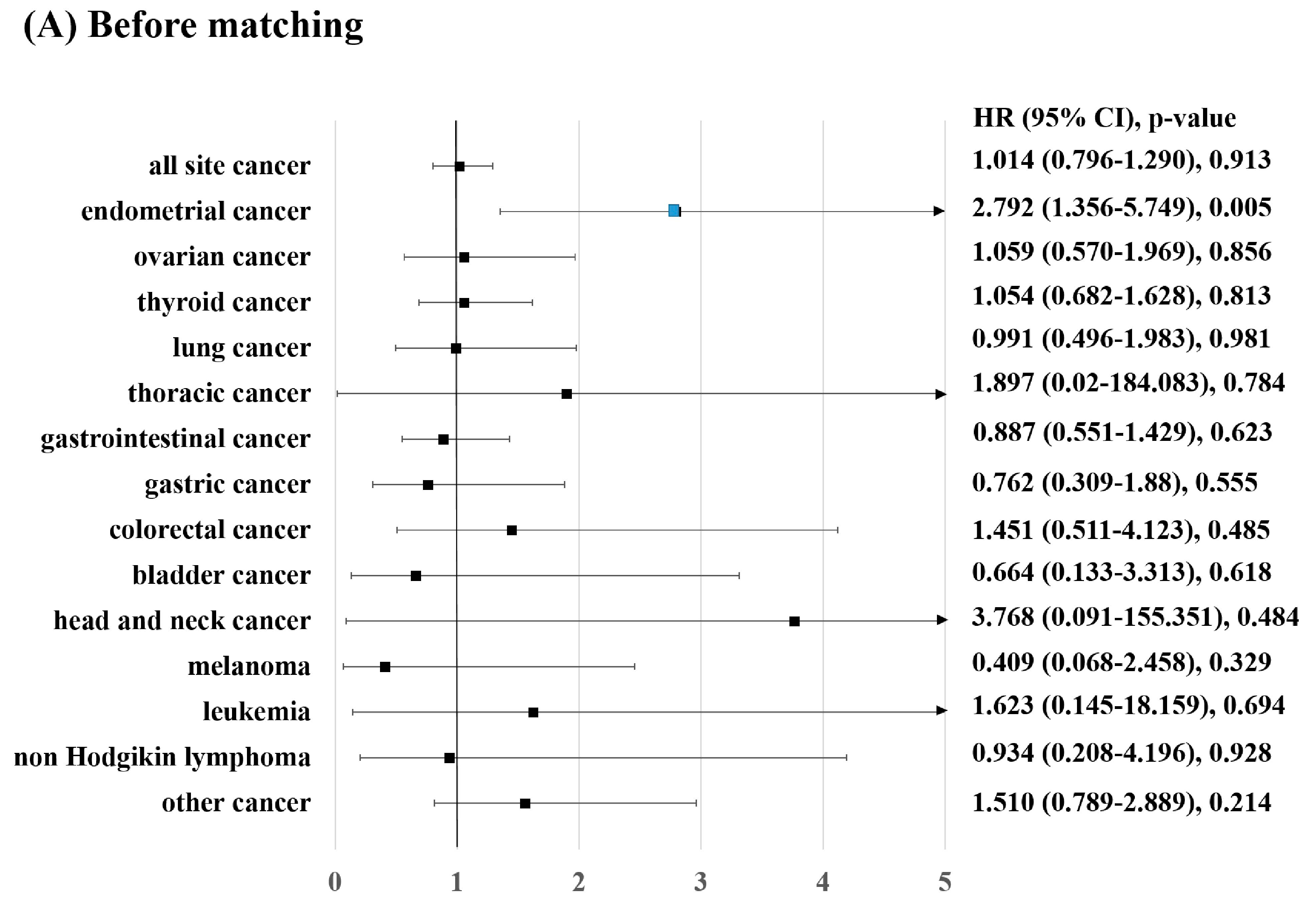
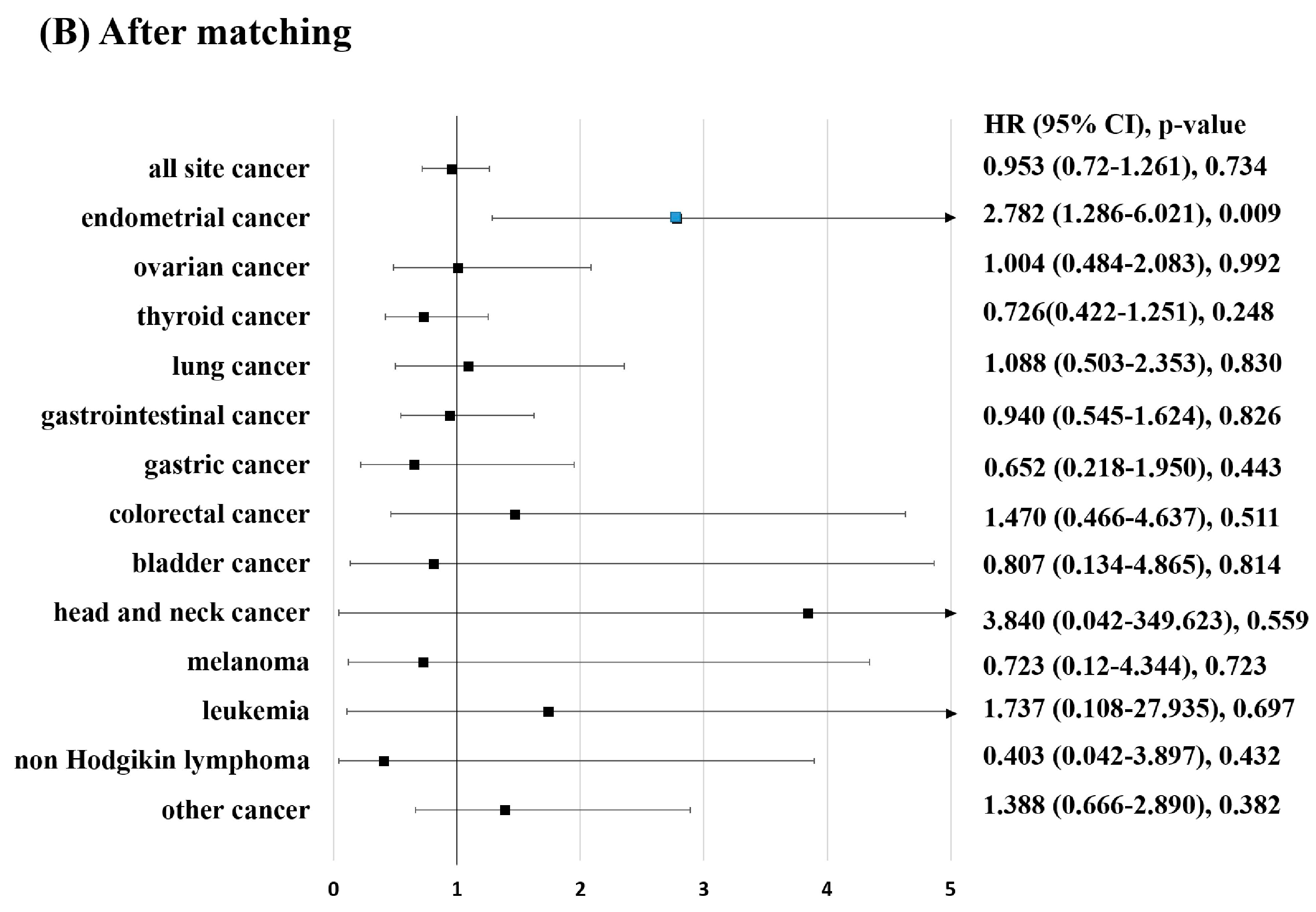
3.3. Risk Factors of Second Primary Cancer
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Davies, C.; Godwin, J.; Gray, R.; Clarke, M.; Cutter, D.; Darby, S.; Early Breast Cancer Trialists’ Collaborative Group. Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: Patient-level meta-analysis of randomised trials. Lancet 2011, 378, 771–784. [Google Scholar] [PubMed]
- Fisher, B.; Costantino, J.P.; Wickerham, D.L.; Cecchini, R.; Cronin, W.M.; Robidoux, A.; Bevers, T.B.; Kavanah, M.T.; Atkins, J.N.; Margolese, R.G.; et al. Tamoxifen for the Prevention of Breast Cancer: Current Status of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. Gynecol. Oncol. 2005, 97, 1652–1662. [Google Scholar] [CrossRef] [PubMed]
- Yu, K.; Huang, Z.-Y.; Xu, X.-L.; Li, J.; Fu, X.-W.; Deng, S.-L. Estrogen Receptor Function: Impact on the Human Endometrium. Front. Endocrinol. 2022, 13, 827724. [Google Scholar] [CrossRef] [PubMed]
- Mourits, M.J.; De Vries, E.G.; Willemse, P.H.; Hoor, K.A.T.; Hollema, H.; Van Der Zee, A.G. Tamoxifen treatment and gynecologic side effects: A review. Obstet. Gynecol. 2001, 97, 855–866. [Google Scholar] [CrossRef]
- Love, R.R.; Wiebe, D.A.; Feyzi, J.M.; Newcomb, P.A.; Chappell, R.J. Effects of tamoxifen on cardiovascular risk factors in postmeno-pausal women after 5 years of treatment. J. Natl. Cancer Inst. 1994, 86, 1534–1539. [Google Scholar] [CrossRef]
- Swerdlow, A.J.; Jones, M. Tamoxifen treatment for the British Tamoxifen Second Cancer Study Group Tamoxifen Treatment for Breast Cancer and Risk of Endometrial Cancer: A Case-Control Study. Gynecol. Oncol. 2005, 97, 375–384. [Google Scholar] [CrossRef]
- Andersson, M.; Storm, H.H.; Mouridsen, H.T. Incidence of New Primary Cancers After Adjuvant Tamoxifen Therapy and Radiotherapy for Early Breast Cancer. Gynecol. Oncol. 1991, 83, 1013–1017. [Google Scholar] [CrossRef]
- Bergman, L.; Beelen, M.L.; Gallee, M.P.; Hollema, H.; Benraadt, J.; van Leeuwen, F.E. Risk and prognosis of endometrial cancer after tamoxifen for breast cancer. Lancet 2000, 356, 881–887. [Google Scholar] [CrossRef]
- Neven, P.; Vernaeve, H. Guidelines for monitoring patients taking tamoxifen treatment. Drug Saf. 2000, 22, 1–11. [Google Scholar] [CrossRef]
- Rosenstock, A.S.; Niu, J.; Giordano, S.H.; Zhao, H.; Wolff, A.C.; Chavez-MacGregor, M. Acute myeloid leukemia and myelodysplastic syndrome after adjuvant chemotherapy: A population-based study among older breast cancer patients. Cancer 2017, 124, 899–906. [Google Scholar] [CrossRef]
- Freedman, R.A.; Seisler, D.K.; Foster, J.C.; Sloan, J.A.; Lafky, J.M.; Kimmick, G.G.; Hurria, A.; Cohen, H.J.; Winer, E.P.; Hudis, C.A.; et al. Risk of acute myeloid leukemia and myelo-dysplastic syndrome among older women receiving anthracycline-based adjuvant chemotherapy for breast cancer on Modern Cooperative Group Trials (Alliance A151511). Breast Cancer Res. Treat. 2017, 161, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Wils, J.; Bliss, J.; Marty, M.; Coombes, G.; Fontaine, C.; Morvan, F.; Olmos, T.; Pérez-López, F.; Vassilopoulos, P.; Woods, E.; et al. Epirubicin Plus Tamoxifen Versus Tamoxifen Alone in Node-Positive Postmenopausal Patients With Breast Cancer: A Randomized Trial of the International Collaborative Cancer Group. J. Clin. Oncol. 1999, 17, 1988. [Google Scholar] [CrossRef] [PubMed]
- Salminen, S.H.; Sampo, M.M.; Böhling, T.O.; Tuomikoski, L.; Tarkkanen, M.; Blomqvist, C.P. Radiation-associated sarcoma after breast cancer in a nationwide population: Increasing risk of angiosarcoma. Cancer Med. 2018, 7, 4825–4835. [Google Scholar] [CrossRef]
- Snow, A.; Ring, A.; Struycken, L.; Mack, W.; Koç, M.; Lang, J.E. Incidence of radiation induced sarcoma attributable to radiotherapy in adults: A retrospective cohort study in the SEER cancer registries across 17 primary tumor sites. Cancer Epidemiol. 2020, 70, 101857. [Google Scholar] [CrossRef]
- World Health Organization. International Statistical Classification of Diseases and Related health Problems: Tenth Revision, 2nd ed.; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Braithwaite, R.S.; Chlebowski, R.T.; Lau, J.; George, S.; Hess, R.; Col, N.F. Meta-analysis of vascular and neoplastic events associated with tamoxifen. J. Gen. Intern. Med. 2003, 18, 937–947. [Google Scholar] [CrossRef]
- Davies, C.; Pan, H.; Godwin, J.; Gray, R.; Arriagada, R.; Raina, V.; Abraham, M.; Medeiros Alencar, V.H.; Badran, A.; Bonfill, X.; et al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet 2013, 381, 805–816. [Google Scholar] [CrossRef] [PubMed]
- Cuzick, J.; Sestak, I.; Cawthorn, S.; Hamed, H.; Holli, K.; Howell, A.; Forbes, J.F.; IBIS-I Investigators. Tamoxifen for prevention of breast cancer: Extended long-term follow-up of the IBIS-I breast cancer prevention trial. Lancet Oncol. 2015, 16, 67–75. [Google Scholar] [CrossRef]
- Smith, R.E.; Bryant, J.; DeCillis, A.; Anderson, S. Acute myeloid leukemia and myelodysplastic syndrome after doxorubi-cin-cyclophosphamide adjuvant therapy for operable breast cancer: The National Surgical Adjuvant Breast and Bowel Project Experience. J. Clin. Oncol. 2003, 21, 1195–1204. [Google Scholar] [CrossRef]
- Rosell, J.; Nordenskjöld, B.; Bengtsson, N.-O.; Fornander, T.; Hatschek, T.; Lindman, H.; Malmström, P.-O.; Wallgren, A.; Stål, O.; Carstensen, J. Long-term effects on the incidence of second primary cancers in a randomized trial of two and five years of adjuvant tamoxifen. Acta Oncol. 2017, 56, 614–617. [Google Scholar] [CrossRef]
- Matsuyama, Y.; Tominaga, T.; Nomura, Y.; Koyama, H.; Kimura, M.; Sano, M.; Miura, S.; Takashima, S.; Ueo, H.; Ohshi, Y.I.; et al. Second cancers after adjuvant tamoxifen therapy for breast cancer in Japan. Ann. Oncol. 2000, 11, 1537–1543. [Google Scholar] [CrossRef]
- Ryu, K.-J.; Kim, M.S.; Lee, J.Y.; Nam, S.; Jeong, H.G.; Kim, T.; Park, H. Risk of Endometrial Polyps, Hyperplasia, Carcinoma, and Uterine Cancer After Tamoxifen Treatment in Premenopausal Women With Breast Cancer. JAMA Netw. Open 2022, 5, e2243951. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Lee, Y.J.; Jeong, J.H.; Jung, J.; Lee, J.W.; Kim, H.J.; Ko, B.S.; Son, B.H.; Ahn, S.H.; Lee, Y.; et al. Risk of Endometrial Cancer and Frequencies of Invasive Endometrial Procedures in Young Breast Cancer Survivors Treated With Tamoxifen: A Nationwide Study. Front. Oncol. 2021, 11, 636378. [Google Scholar] [CrossRef] [PubMed]
- Chu, T.-Y.; Chu, S.-C.; Hsieh, C.-J.; Wang, T.-F.; Hong, M.-K. Younger tamoxifen-treated breast cancer patients also had higher risk of endometrial cancer and the risk could be reduced by sequenced aromatase inhibitor use: A population-based study in Taiwan. Tzu-Chi Med. J. 2020, 32, 175–180. [Google Scholar] [CrossRef]
- Ignatov, A.; Ortmann, O. Endocrine Risk Factors of Endometrial Cancer: Polycystic Ovary Syndrome, Oral Contraceptives, Infertility, Tamoxifen. Cancers 2020, 12, 1766. [Google Scholar] [CrossRef] [PubMed]
- Tokutake, N.; Ushiyama, R.; Matsubayashi, K.; Aoki, Y. Age-specific incidence rates of breast cancer among Japanese women increasing in a conspicuous bimodal distribution pattern. Proc. Singap. Heal. 2020, 30, 166–169. [Google Scholar] [CrossRef]
- Seo, H.J.; Oh, I.-H.; Yoon, S.-J. A Comparison of the Cancer Incidence Rates between the National Cancer Registry and Insurance Claims Data in Korea. Asian Pac. J. Cancer Prev. 2012, 13, 6163–6168. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before Matching | After Matching | |||||||
|---|---|---|---|---|---|---|---|---|
| Total | Tamoxifen | p-Value | Total | Tamoxifen | p-Value | |||
| n(%) | No(n = 1819) | Yes(n = 3205) | n(%) | No(n = 1802) | Yes(n = 1802) | |||
| All-site cancer | ||||||||
| No | 4739(94.38) | 1712(94.12) | 3027(94.53) | 0.537 | 3385(94.50) | 1686(94.14) | 1699(94.86) | 0.34 |
| Yes | 282(5.62) | 107(5.88) | 175(5.47) | 197(5.50) | 105(5.86) | 92(5.14) | ||
| Endometrial cancer | ||||||||
| No | 4971(99.00) | 1810(99.51) | 3161(98.72) | 0.007 | 3550(99.11) | 1782(99.50) | 1768(98.72) | 0.013 |
| Yes | 50(1.00) | 9(0.49) | 41(1.28) | 32(0.89) | 9(0.50) | 23(1.28) | ||
| Ovarian cancer | ||||||||
| No | 4978(99.14) | 1803(99.12) | 3175(99.16) | 0.893 | 3553(99.19) | 1776(99.16) | 1777(99.22) | 0.852 |
| Yes | 43(0.86) | 16(0.88) | 27(0.84) | 29(0.81) | 15(0.84) | 14(0.78) | ||
| Thyroid cancer | ||||||||
| No | 4933(98.25) | 1787(98.24) | 3146(98.25) | 0.978 | 3528(98.49) | 1759(98.21) | 1769(98.77) | 0.17 |
| Yes | 88(1.75) | 32(1.76) | 56(1.75) | 54(1.51) | 32(1.79) | 22(1.23) | ||
| Lung cancer | ||||||||
| No | 4987(99.32) | 1806(99.29) | 3181(99.34) | 0.807 | 3556(99.27) | 1778(99.27) | 1778(99.27) | >0.999 |
| Yes | 34(0.68) | 13(0.71) | 21(0.66) | 26(0.73) | 13(0.73) | 13(0.73) | ||
| Thoracic cancer | ||||||||
| No | 5020(99.98) | 1819(100.00) | 3201(99.97) | >0.999 | 3582(100.00) | 1791(100.00) | 1791(100.00) | >0.999 |
| Yes | 1(0.02) | 0(0.00) | 1(0.03) | 0(0.00) | 0(0.00) | 0(0.00) | ||
| Gastrointestinal cancer | ||||||||
| No | 4951(98.61) | 1790(98.41) | 3161(98.72) | 0.362 | 3530(98.55) | 1763(98.44) | 1767(98.66) | 0.576 |
| Yes | 70(1.39) | 29(1.59) | 41(1.28) | 52(1.45) | 28(1.56) | 24(1.34) | ||
| Gastric cancer | ||||||||
| No | 5002(99.62) | 1810(99.51) | 3192(99.69) | 0.311 | 3568(99.61) | 1782(99.50) | 1786(99.72) | 0.284 |
| Yes | 19(0.38) | 9(0.49) | 10(0.31) | 14(0.39) | 9(0.50) | 5(0.28) | ||
| Colorectal cancer | ||||||||
| No | 5004(99.66) | 1814(99.73) | 3190(99.63) | 0.558 | 3570(99.66) | 1786(99.72) | 1784(99.61) | 0.563 |
| Yes | 17(0.34) | 5(0.27) | 12(0.37) | 12(0.34) | 5(0.28) | 7(0.39) | ||
| Bladder cancer | ||||||||
| No | 5015(99.88) | 1816(99.84) | 3199(99.91) | 0.674 | 3577(99.86) | 1788(99.83) | 1789(99.89) | >0.999 |
| Yes | 6(0.12) | 3(0.16) | 3(0.09) | 5(0.14) | 3(0.17) | 2(0.11) | ||
| Head and neck cancer | ||||||||
| No | 5019(99.96) | 1819(100.00) | 3200(99.94) | 0.537 | 3581(99.97) | 1791(100.00) | 1790(99.94) | >0.999 |
| Yes | 2(0.04) | 0(0.00) | 2(0.06) | 1(0.03) | 0(0.00) | 1(0.06) | ||
| Melanoma | ||||||||
| No | 5016(99.90) | 1816(99.84) | 3200(99.94) | 0.359 | 3577(99.86) | 1788(99.83) | 1789(99.89) | >0.999 |
| Yes | 5(0.10) | 3(0.16) | 2(0.06) | 5(0.14) | 3(0.17) | 2(0.11) | ||
| Leukemia | ||||||||
| No | 5018(99.94) | 1818(99.95) | 3200(99.94) | >0.999 | 3580(99.94) | 1790(99.94) | 1790(99.94) | >0.999 |
| Yes | 3(0.06) | 1(0.05) | 2(0.06) | 2(0.06) | 1(0.06) | 1(0.06) | ||
| Non-Hodgkin lymphoma | ||||||||
| No | 5014(99.86) | 1816(99.84) | 3198(99.88) | 0.709 | 3578(99.89) | 1788(99.83) | 1790(99.94) | 0.625 |
| Yes | 7(0.14) | 3(0.16) | 4(0.12) | 4(0.11) | 3(0.17) | 1(0.06) | ||
| Other cancer | ||||||||
| No | 4977(99.12) | 1806(99.29) | 3171(99.03) | 0.354 | 3553(99.19) | 1778(99.27) | 1775(99.11) | 0.576 |
| Yes | 44(0.88) | 13(0.71) | 31(0.97) | 29(0.81) | 13(0.73) | 16(0.89) | ||
| Type of surgery | ||||||||
| BCS | 4482(89.27) | 1584(87.08) | 2898(90.51) | <0.001 | 3132(87.44) | 1564(87.33) | 1568(87.55) | 0.84 |
| mastectomy | 539(10.73) | 235(12.92) | 304(9.49) | 450(12.56) | 227(12.67) | 223(12.45) | ||
| DM | ||||||||
| No | 4415(87.93) | 1630(89.61) | 2785(86.98) | 0.006 | 3222(89.95) | 1608(89.78) | 1614(90.12) | 0.739 |
| Yes | 606(12.07) | 189(10.39) | 417(13.02) | 360(10.05) | 183(10.22) | 177(9.88) | ||
| HTN | ||||||||
| No | 3929(78.25) | 1437(79.00) | 2492(77.83) | 0.333 | 2834(79.12) | 1421(79.34) | 1413(78.89) | 0.742 |
| Yes | 1092(21.75) | 382(21.00) | 710(22.17) | 748(20.88) | 370(20.66) | 378(21.11) | ||
| Hyperlipidemia | ||||||||
| No | 3564(70.98) | 1335(73.39) | 2229(69.61) | 0.005 | 2626(73.31) | 1312(73.26) | 1314(73.37) | 0.94 |
| Yes | 1457(29.02) | 484(26.61) | 973(30.39) | 956(26.69) | 479(26.74) | 477(26.63) | ||
| COPD | ||||||||
| No | 4894(97.47) | 1771(97.36) | 3123(97.53) | 0.709 | 3486(97.32) | 1746(97.49) | 1740(97.15) | 0.535 |
| Yes | 127(2.53) | 48(2.64) | 79(2.47) | 96(2.68) | 45(2.51) | 51(2.85) | ||
| CKD | ||||||||
| No | 4974(99.06) | 1798(98.85) | 3176(99.19) | 0.226 | 3551(99.13) | 1776(99.16) | 1775(99.11) | 0.857 |
| Yes | 47(0.94) | 21(1.15) | 26(0.81) | 31(0.87) | 15(0.84) | 16(0.89) | ||
| Liver cirrhosis | ||||||||
| No | 5005(99.68) | 1810(99.51) | 3195(99.78) | 0.095 | 3572(99.72) | 1785(99.66) | 1787(99.78) | 0.526 |
| Yes | 16(0.32) | 9(0.49) | 7(0.22) | 10(0.28) | 6(0.34) | 4(0.22) | ||
| Heart failure | ||||||||
| No | 4975(99.08) | 1798(98.85) | 3177(99.22) | 0.182 | 3550(99.11) | 1775(99.11) | 1775(99.11) | >0.999 |
| Yes | 46(0.92) | 21(1.15) | 25(0.78) | 32(0.89) | 16(0.89) | 16(0.89) | ||
| Age (mean ± SD) | 49.746 ± 10.224 | 49.396 ± 10.787 | 49.944 ± 9.886 | 0.075 | 49.385 ± 10.501 | 49.413 ± 10.681 | 49.357 ± 10.321 | 0.8736 |
| Before Matching | After Matching | |||||||
|---|---|---|---|---|---|---|---|---|
| Univariable Model | Multivariable Model | Univariable Model | Multivariable Model | |||||
| HR(95% CI) | p-Value | HR(95% CI) | p-Value | HR(95% CI) | p-Value | HR(95% CI) | p-Value | |
| Tamoxifen | ||||||||
| No | ref | Ref | ref | ref | ||||
| Yes | 2.792(1.356–5.749) | 0.005 | 2.664(1.309–5.421) | 0.007 | 2.782(1.286–6.021) | 0.0094 | 2.672(1.244–5.739) | 0.0118 |
| Type of surgery | ||||||||
| BCS | ref | Ref | ref | ref | ||||
| mastectomy | 1.165(0.496–2.734) | 0.725 | 1.281(0.558–2.940) | 0.559 | 1.340(0.516–3.480) | 0.547 | 1.446(0.573–3.649) | 0.434 |
| DM | ||||||||
| No | ref | Ref | ref | ref | ||||
| Yes | 1.454(0.682–3.098) | 0.332 | 1.094(0.490–2.443) | 0.827 | 1.342(0.470–3.826) | 0.583 | 1.414(0.481–4.152) | 0.529 |
| HTN | ||||||||
| No | ref | Ref | ref | ref | ||||
| Yes | 1.548(0.846–2.835) | 0.157 | 1.213(0.594–2.476) | 0.596 | 1.273(0.572–2.833) | 0.555 | 1.318(0.529–3.284) | 0.554 |
| Hyperlipidemia | ||||||||
| No | ref | Ref | ref | ref | ||||
| Yes | 1.629(0.919–2.888) | 0.095 | 1.387(0.727–2.644) | 0.321 | 0.997(0.447–2.222) | 0.994 | 0.925(0.392–2.180) | 0.858 |
| COPD | ||||||||
| No | ref | Ref | ref | ref | ||||
| Yes | 0.837(0.116–6.065) | 0.86 | 0.994(0.193–5.105) | 0.994 | 0.592(0.035–10.079) | 0.717 | 0.515(0.035–7.482) | 0.627 |
| CKD | ||||||||
| No | ref | Ref | ref | ref | ||||
| Yes | 2.323(0.321–16.827) | 0.404 | 2.947(0.576–15.085) | 0.195 | 1.882(0.110–32.149) | 0.662 | 1.475(0.082–26.403) | 0.792 |
| Liver cirrhosis | ||||||||
| No | ref | Ref | ref | ref | ||||
| Yes | 3.211(0.193–53.523) | 0.416 | 2.244(0.145–34.822) | 0.563 | 5.868(0.344–100.088) | 0.222 | 6.691(0.440–101.865) | 0.171 |
| Heart failure | ||||||||
| No | ref | Ref | ref | ref | ||||
| Yes | 2.258(0.312–16.354) | 0.42 | 3.005(0.608–14.865) | 0.177 | 1.726(0.101–29.487) | 0.706 | 1.547(0.112–21.295) | 0.744 |
| Age | 1.017(0.991–1.044) | 0.209 | 1.007(0.976–1.039) | 0.666 | 1.008(0.975–1.041) | 0.644 | 1.006(0.968–1.045) | 0.768 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.; Oh, J.; Seok, J.-H.; Lee, H.S.; Jeon, S.; Yoon, C.I. Risk of Secondary Cancer after Adjuvant Tamoxifen Treatment for Ductal Carcinoma In Situ: A Nationwide Cohort Study in South Korea. Diagnostics 2023, 13, 792. https://doi.org/10.3390/diagnostics13040792
Kim D, Oh J, Seok J-H, Lee HS, Jeon S, Yoon CI. Risk of Secondary Cancer after Adjuvant Tamoxifen Treatment for Ductal Carcinoma In Situ: A Nationwide Cohort Study in South Korea. Diagnostics. 2023; 13(4):792. https://doi.org/10.3390/diagnostics13040792
Chicago/Turabian StyleKim, Dooreh, Jooyoung Oh, Jeong-Ho Seok, Hye Sun Lee, Soyoung Jeon, and Chang Ik Yoon. 2023. "Risk of Secondary Cancer after Adjuvant Tamoxifen Treatment for Ductal Carcinoma In Situ: A Nationwide Cohort Study in South Korea" Diagnostics 13, no. 4: 792. https://doi.org/10.3390/diagnostics13040792
APA StyleKim, D., Oh, J., Seok, J.-H., Lee, H. S., Jeon, S., & Yoon, C. I. (2023). Risk of Secondary Cancer after Adjuvant Tamoxifen Treatment for Ductal Carcinoma In Situ: A Nationwide Cohort Study in South Korea. Diagnostics, 13(4), 792. https://doi.org/10.3390/diagnostics13040792