
Evaluation of Crohn’s Disease Small-Bowel Mucosal Healing Using Capsule Endoscopy and Usefulness of Leucine-Rich α2-Glycoprotein

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
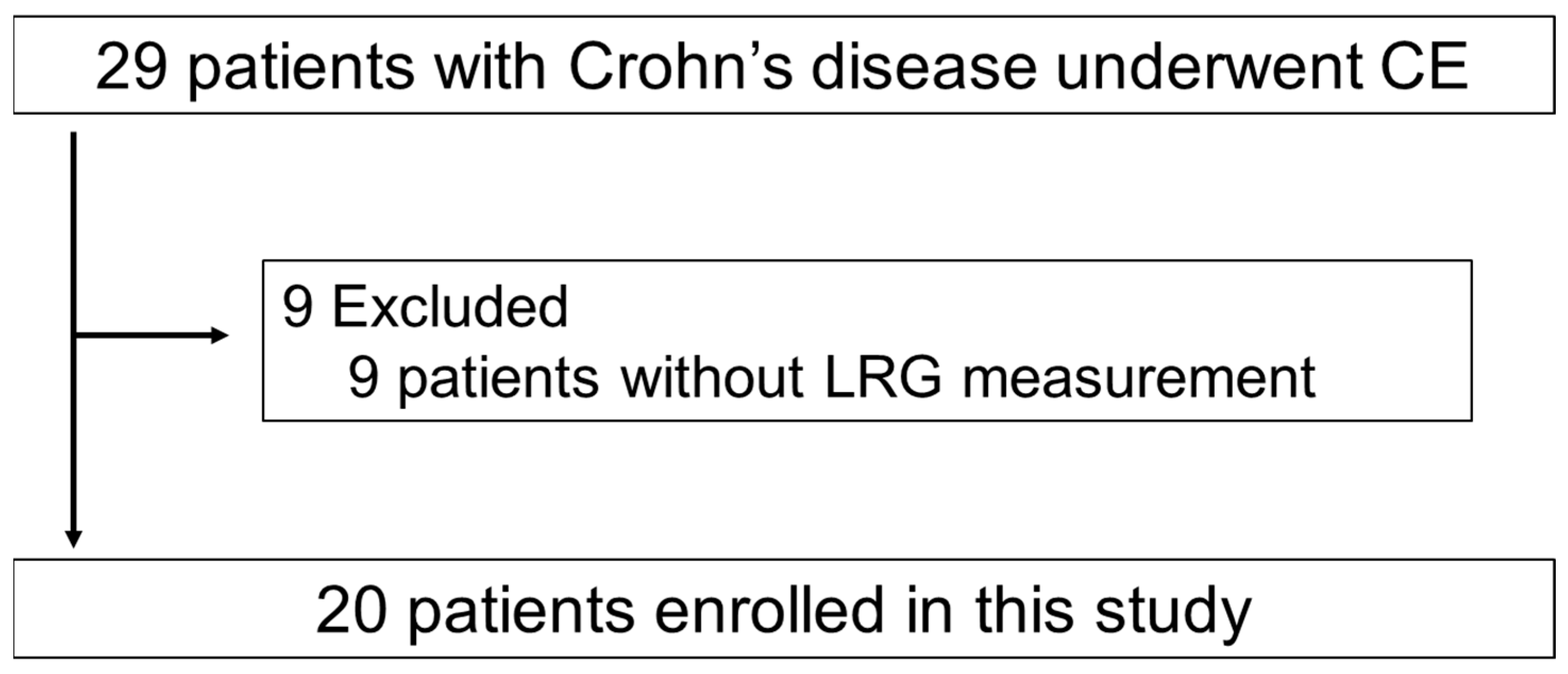
2.1. Study Design and Patients
2.2. Capsule Endoscopy Procedure
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Connection between Crohn’s Disease Activity Markers and the Achieving Mucosal Healing in Ileocolonoscopy
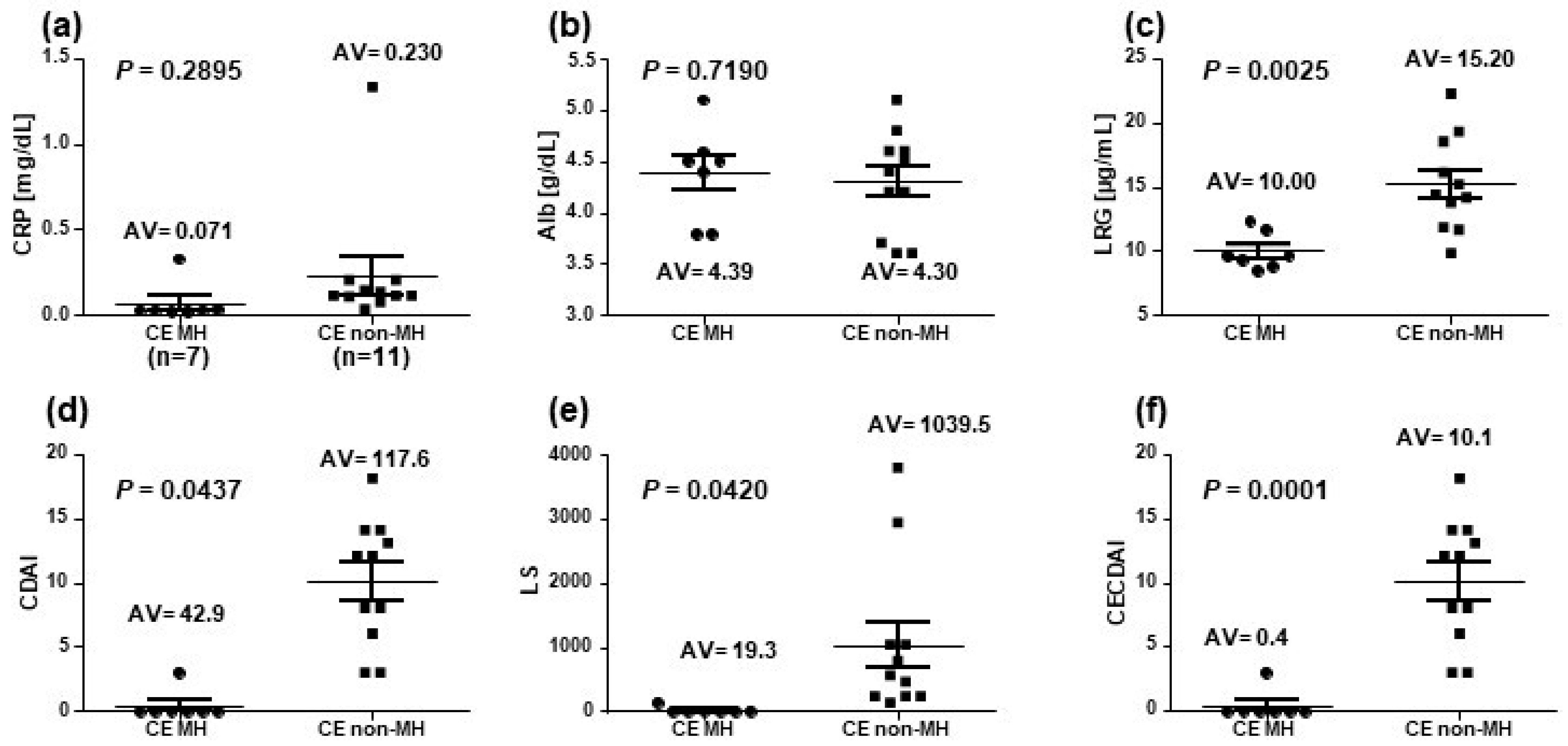
3.3. Connection between Crohn’s Disease Activity Markers and the Achievement of Mucosal Healing in Capsule Endoscopy
3.4. Correlation of Leucine-Rich α2-Glycoprotein with Crohn’s Disease Activity Markers
3.5. The Original Pictures of CE Findings
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- D’Incà, R.; Caccaro, R. Measuring disease activity in Crohn’s disease: What is currently available to the clinician. Clin. Exp. Gastroenterol. 2014, 7, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, G.R.; Hanauer, S.B.; Sandborn, W.J.; Practice Parameters Committee of American College of Gastroenterology. Management of Crohn’s disease in adults. Am. J. Gastroenterol. 2009, 104, 465–483. [Google Scholar] [CrossRef] [PubMed]
- Turner, D.; Ricciuto, A.; Lewis, A.; D’Amico, F.; Dhaliwal, J.; Griffiths, A.M.; Bettenworth, D.; Sandborn, W.J.; Sands, B.E.; Reinisch, W.; et al. STRIDE-II: An Update on the Selecting Therapeutic Targets in inflammatory bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining therapeutic goals for treat-to-target strategies in IBD. Gastroenterology 2021, 160, 1570–1583. [Google Scholar] [CrossRef] [PubMed]
- Hall, B.; Holleran, G.; Chin, J.L.; Smith, S.; Ryan, B.; Mahmud, N.; McNamara, D. A prospective 52 week mucosal healing assessment of small bowel Crohn’s disease as detected by capsule endoscopy. J. Crohns Colitis. 2014, 8, 1601–1609. [Google Scholar] [CrossRef]
- Hall, B.J.; Holleran, G.E.; Smith, S.M.; Mahmud, N.; McNamara, D.A. A prospective 12-week mucosal healing assessment of small bowel Crohn’s disease as detected by capsule endoscopy. Eur. J. Gastroenterol. Hepatol. 2014, 26, 1253–1259. [Google Scholar] [CrossRef]
- Kopylov, U.; Yablecovitch, D.; Lahat, A.; Neuman, S.; Levhar, N.; Greener, T.; Klang, E.; Rozendorn, N.; Amitai, M.M.; Ben-Horin, S.; et al. Detection of small bowel mucosal healing and deep remission in patients with known small bowel Crohn’s disease using biomarkers, capsule endoscopy, and imaging. Am. J. Gastroenterol. 2015, 110, 1316–1323. [Google Scholar] [CrossRef]
- Dionisio, P.M.; Gurudu, S.R.; Leighton, J.A.; Leontiadis, G.I.; Fleischer, D.E.; Hara, A.K.; Heigh, R.I.; Shiff, A.D.; Sharma, V.K. Capsule endoscopy has a significantly higher diagnostic yield in patients with suspected and established small-bowel Crohn’s disease: A meta-analysis. Am. J. Gastroenterol. 2010, 105, 1240–1248. [Google Scholar] [CrossRef]
- Casciani, E.; Masselli, G.; Di Nardo, G.; Polettini, E.; Bertini, L.; Oliva, S.; Floriani, I.; Cucchiara, S.; Gualdi, G. MR enterography versus capsule endoscopy in paediatric patients with suspected Crohn’s disease. Eur. Radiol. 2011, 21, 823–831. [Google Scholar] [CrossRef]
- Jensen, M.D.; Nathan, T.; Rafaelsen, S.R.; Kjeldsen, J. Diagnostic accuracy of capsule endoscopy for small bowel Crohn’s disease is superior to that of MR enterography or CT enterography. Clin. Gastroenterol. Hepatol. 2011, 9, 124–129. [Google Scholar] [CrossRef]
- Voderholzer, W.A.; Beinhoelzl, J.; Rogalla, P.; Murrer, S.; Schachschal, G.; Lochs, H.; Ortner, M.A. Small bowel involvement in Crohn’s disease: A prospective comparison of wireless capsule endoscopy and computed tomography enteroclysis. Gut 2005, 54, 369–373. [Google Scholar] [CrossRef]
- Enns, R.A.; Hookey, L.; Armstrong, D.; Bernstein, C.N.; Heitman, S.J.; Teshima, C.; Leontiadis, G.I.; Tse, F.; Sadowski, D. Clinical practice guidelines for the use of video capsule endoscopy. Gastroenterology 2017, 152, 497–514. [Google Scholar] [CrossRef] [PubMed]
- Gralnek, I.M.; Cohen, S.A.; Ephrath, H.; Napier, A.; Gobin, T.; Sherrod, O.; Lewis, J. Small bowel capsule endoscopy impacts diagnosis and management of pediatric inflammatory bowel disease: A prospective study. Dig. Dis. Sci. 2012, 57, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo-Zúñiga, V.; de Vega, V.M.; Domènech, E.; Cabré, E.; Mañosa, M.; Boix, J. Impact of capsule endoscopy findings in the management of Crohn’s disease. Dig. Dis. Sci. 2010, 55, 411–414. [Google Scholar] [CrossRef] [PubMed]
- Samuel, S.; Bruining, D.H.; Loftus, E.V., Jr.; Becker, B.; Fletcher, J.G.; Mandrekar, J.N.; Zinsmeister, A.R.; Sandborn, W.J. Endoscopic skipping of the distal terminal ileum in Crohn’s disease can lead to negative results from ileocolonoscopy. Clin. Gastroenterol. Hepatol. 2012, 10, 1253–1259. [Google Scholar] [CrossRef] [PubMed]
- Takenaka, K.; Ohtsuka, K.; Kitazume, Y.; Matsuoka, K.; Nagahori, M.; Fujii, T.; Saito, E.; Kimura, M.; Fujioka, T.; Watanabe, M. Utility of magnetic resonance enterography for small bowel endoscopic healing in patients with Crohn’s disease. Am. J. Gastroenterol. 2018, 113, 283–294. [Google Scholar] [CrossRef]
- Takenaka, K.; Ohtsuka, K.; Kitazume, Y.; Nagahori, M.; Fujii, T.; Saito, E.; Fujioka, T.; Matsuoka, K.; Naganuma, M.; Watanabe, M. Correlation of the endoscopic and magnetic resonance scoring systems in the deep small intestine in Crohn’s disease. Inflamm Bowel. Dis. 2015, 21, 1832–1838. [Google Scholar] [CrossRef]
- D’Haens, G.; Ferrante, M.; Vermeire, S.; Baert, F.; Noman, M.; Moortgat, L.; Geens, P.; Iwens, D.; Aerden, I.; Van Assche, G.; et al. Fecal calprotectin is a surrogate marker for endoscopic lesions in inflammatory bowel disease. Inflamm. Bowel. Dis. 2012, 18, 2218–2224. [Google Scholar] [CrossRef]
- Schoepfer, A.M.; Beglinger, C.; Straumann, A.; Safroneeva, E.; Romero, Y.; Armstrong, D.; Schmidt, C.; Trummler, M.; Pittet, V.; Vavricka, S.R. Fecal calprotectin more accurately reflects endoscopic activity of ulcerative colitis than the Lichtiger Index, C-reactive protein, platelets, hemoglobin, and blood leukocytes. Inflamm. Bowel. Dis. 2013, 19, 332–341. [Google Scholar] [CrossRef]
- Waugh, N.; Cummins, E.; Royle, P.; Kandala, N.B.; Shyangdan, D.; Arasaradnam, R.; Clar, C.; Johnston, R. Faecal calprotectin testing for differentiating amongst inflammatory and non-inflammatory bowel diseases: Systematic review and economic evaluation. Health. Technol. Assess. 2013, 17, 1–211. [Google Scholar] [CrossRef]
- Krzystek-Korpacka, M.; Kempiński, R.; Bromke, M.; Neubauer, K. Biochemical biomarkers of mucosal healing for inflammatory bowel disease in adults. Diagnostics 2020, 10, 367. [Google Scholar] [CrossRef]
- Maréchal, C.; Aimone-Gastin, I.; Baumann, C.; Dirrenberger, B.; Guéant, J.L.; Peyrin-Biroulet, L. Compliance with the faecal calprotectin test in patients with inflammatory bowel disease. United Eur. Gastroenterol. J. 2017, 5, 702–707. [Google Scholar] [CrossRef] [PubMed]
- Zittan, E.; Gralnek, I.M.; Berns, M.S. The new proactive approach and precision medicine in Crohn’s disease. Biomedicines 2020, 8, 193. [Google Scholar] [CrossRef]
- Haupt, H.; Baudner, S. [Isolation and characterization of an unknown, leucine-rich 3.1-S-alpha2-glycoprotein from human serum (author’s transl)]. Hoppe. Seylers. Z. Physiol. Chem. 1977, 358, 639–646. [Google Scholar] [CrossRef]
- Takahashi, N.; Takahashi, Y.; Putnam, F.W. Periodicity of leucine and tandem repetition of a 24-amino acid segment in the primary structure of leucine-rich alpha 2-glycoprotein of human serum. Proc. Natl. Acad. Sci. USA 1985, 82, 1906–1910. [Google Scholar] [CrossRef] [PubMed]
- Serada, S.; Fujimoto, M.; Ogata, A.; Terabe, F.; Hirano, T.; Iijima, H.; Shinzaki, S.; Nishikawa, T.; Ohkawara, T.; Iwahori, K.; et al. iTRAQ-based proteomic identification of leucine-rich alpha-2 glycoprotein as a novel inflammatory biomarker in autoimmune diseases. Ann. Rheum. Dis. 2010, 69, 770–774. [Google Scholar] [CrossRef] [PubMed]
- Serada, S.; Fujimoto, M.; Terabe, F.; Iijima, H.; Shinzaki, S.; Matsuzaki, S.; Ohkawara, T.; Nezu, R.; Nakajima, S.; Kobayashi, T.; et al. Serum leucine-rich alpha-2 glycoprotein is a disease activity biomarker in ulcerative colitis. Inflamm. Bowel. Dis. 2012, 18, 2169–2179. [Google Scholar] [CrossRef]
- Shinzaki, S.; Matsuoka, K.; Iijima, H.; Mizuno, S.; Serada, S.; Fujimoto, M.; Arai, N.; Koyama, N.; Morii, E.; Watanabe, M.; et al. Leucine-rich Alpha-2 glycoprotein is a serum biomarker of mucosal healing in ulcerative colitis. J. Crohns. Colitis 2017, 11, 84–91. [Google Scholar] [CrossRef]
- Kawamoto, A.; Takenaka, K.; Hibiya, S.; Ohtsuka, K.; Okamoto, R.; Watanabe, M. Serum leucine-rich alpha2 glycoprotein: A novel biomarker for small bowel mucosal activity in Crohn’s disease. Clin. Gastroenterol. Hepatol. 2022, 20, e1196–e1200. [Google Scholar] [CrossRef]
- Omori, T.; Sasaki, Y.; Koroku, M.; Murasugi, S.; Yonezawa, M.; Nakamura, S.; Tokushige, K. Serum leucine-rich alpha-2 glycoprotein in quiescent Crohn’s disease as a potential surrogate marker for small-bowel ulceration detected by capsule endoscopy. J. Clin. Med. 2022, 11, 2494. [Google Scholar] [CrossRef]
- Best, W.R.; Becktel, J.M.; Singleton, J.W.; Kern, F., Jr. Development of a Crohn’s disease activity index. National Cooperative Crohn’s disease Study. Gastroenterology 1976, 70, 439–444. [Google Scholar] [CrossRef]
- Gralnek, I.M.; Defranchis, R.; Seidman, E.; Leighton, J.A.; Legnani, P.; Lewis, B.S. Development of a capsule endoscopy scoring index for small bowel mucosal inflammatory change. Aliment. Pharmacol. Ther. 2008, 27, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Niv, Y.; Ilani, S.; Levi, Z.; Hershkowitz, M.; Niv, E.; Fireman, Z.; O’Donnel, S.; O’Morain, C.; Eliakim, R.; Scapa, E.; et al. Validation of the Capsule Endoscopy Crohn’s disease Activity Index (CECDAI or Niv score): A multicenter prospective study. Endoscopy 2012, 44, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Rosa, B.; Moreira, M.J.; Rebelo, A.; Cotter, J. Lewis Score: A useful clinical tool for patients with suspected Crohn’s disease submitted to capsule endoscopy. J. Crohns. Colitis 2012, 6, 692–697. [Google Scholar] [CrossRef] [PubMed]
- Toniatti, C.; Arcone, R.; Majello, B.; Ganter, U.; Arpaia, G.; Ciliberto, G. Regulation of the human C-reactive protein gene, a major marker of inflammation and cancer. Mol. Biol. Med. 1990, 7, 199–212. [Google Scholar] [PubMed]
- Vermeire, S.; Van Assche, G.; Rutgeerts, P. Laboratory markers in IBD: Useful, magic, or unnecessary toys? Gut 2006, 55, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Levy, I.; Gralnek, I.M. Complications of diagnostic colonoscopy, upper endoscopy, and enteroscopy. Best. Pract. Res. Clin. Gastroenterol. 2016, 30, 705–718. [Google Scholar] [CrossRef]
- Levesque, B.G.; Sandborn, W.J.; Ruel, J.; Feagan, B.G.; Sands, B.E.; Colombel, J.F. Converging goals of treatment of inflammatory bowel disease from clinical trials and practice. Gastroenterology 2015, 148, 37–51. [Google Scholar] [CrossRef]
- Sturm, A.; Maaser, C.; Calabrese, E.; Annese, V.; Fiorino, G.; Kucharzik, T.; Vavricka, S.R.; Verstockt, B.; van Rheenen, P.; Tolan, D.; et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 2: IBD scores and general principles and technical aspects. J. Crohns. Colitis 2019, 13, 273–284. [Google Scholar] [CrossRef]
- Ben-Horin, S.; Lahat, A.; Amitai, M.M.; Klang, E.; Yablecovitch, D.; Neuman, S.; Levhar, N.; Selinger, L.; Rozendorn, N.; Turner, D.; et al. Assessment of small bowel mucosal healing by video capsule endoscopy for the prediction of short-term and long-term risk of Crohn’s disease flare: A prospective cohort study. Lancet. Gastroenterol. Hepatol. 2019, 4, 519–528. [Google Scholar] [CrossRef]
- Yasutomi, E.; Inokuchi, T.; Hiraoka, S.; Takei, K.; Igawa, S.; Yamamoto, S.; Ohmori, M.; Oka, S.; Yamasaki, Y.; Kinugasa, H.; et al. Leucine-rich alpha-2 glycoprotein as a marker of mucosal healing in inflammatory bowel disease. Sci. Rep. 2021, 11, 11086. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | |
|---|---|
| Sex (male: female) | 12: 8 |
| Age (years) | 33 (14–49) |
| Disease location Ileal type Ileocolonic type Colonic type | 3 (15) 15 (75) 2 (10) |
| CDAI Remission Mild Moderate Severe | 97.2 (20–327) 16 (80) 2 (10) 1 (5) 1 (5) |
| Alb (g/dL) | 4.31 (3.6–5.1) |
| CRP (mg/dL) | 0.155 (0.02–1.33) |
| LRG (μg/mL) | 13.32 (8.5–22.2) |
| CE activity scores LS CECDAI | 571.8 (0–3789) 5.7 (0–18) |
| Achievement of MH CS-MH CE-MH | 5/12 (41.7) 9/20 (45) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hiraga, H.; Chinda, D.; Hasui, K.; Murai, Y.; Maeda, T.; Higuchi, N.; Ogasawara, K.; Kudo, S.; Sawada, Y.; Tatsuta, T.; et al. Evaluation of Crohn’s Disease Small-Bowel Mucosal Healing Using Capsule Endoscopy and Usefulness of Leucine-Rich α2-Glycoprotein. Diagnostics 2023, 13, 626. https://doi.org/10.3390/diagnostics13040626
Hiraga H, Chinda D, Hasui K, Murai Y, Maeda T, Higuchi N, Ogasawara K, Kudo S, Sawada Y, Tatsuta T, et al. Evaluation of Crohn’s Disease Small-Bowel Mucosal Healing Using Capsule Endoscopy and Usefulness of Leucine-Rich α2-Glycoprotein. Diagnostics. 2023; 13(4):626. https://doi.org/10.3390/diagnostics13040626
Chicago/Turabian StyleHiraga, Hiroto, Daisuke Chinda, Keisuke Hasui, Yasuhisa Murai, Takato Maeda, Naoki Higuchi, Kohei Ogasawara, Sae Kudo, Yohei Sawada, Tetsuya Tatsuta, and et al. 2023. "Evaluation of Crohn’s Disease Small-Bowel Mucosal Healing Using Capsule Endoscopy and Usefulness of Leucine-Rich α2-Glycoprotein" Diagnostics 13, no. 4: 626. https://doi.org/10.3390/diagnostics13040626
APA StyleHiraga, H., Chinda, D., Hasui, K., Murai, Y., Maeda, T., Higuchi, N., Ogasawara, K., Kudo, S., Sawada, Y., Tatsuta, T., Kikuchi, H., Ebina, M., Hiraga, N., Mikami, T., Sakuraba, H., & Fukuda, S. (2023). Evaluation of Crohn’s Disease Small-Bowel Mucosal Healing Using Capsule Endoscopy and Usefulness of Leucine-Rich α2-Glycoprotein. Diagnostics, 13(4), 626. https://doi.org/10.3390/diagnostics13040626