
Molecular Imaging Diagnosis of Renal Cancer Using 99mTc-Sestamibi SPECT/CT and Girentuximab PET-CT-Current Evidence and Future Development of Novel Techniques

 ,
,  , ,
, ,  ,
,  ,
,  ,
,  , ,
, ,  ,
,
Abstract
1. Introduction
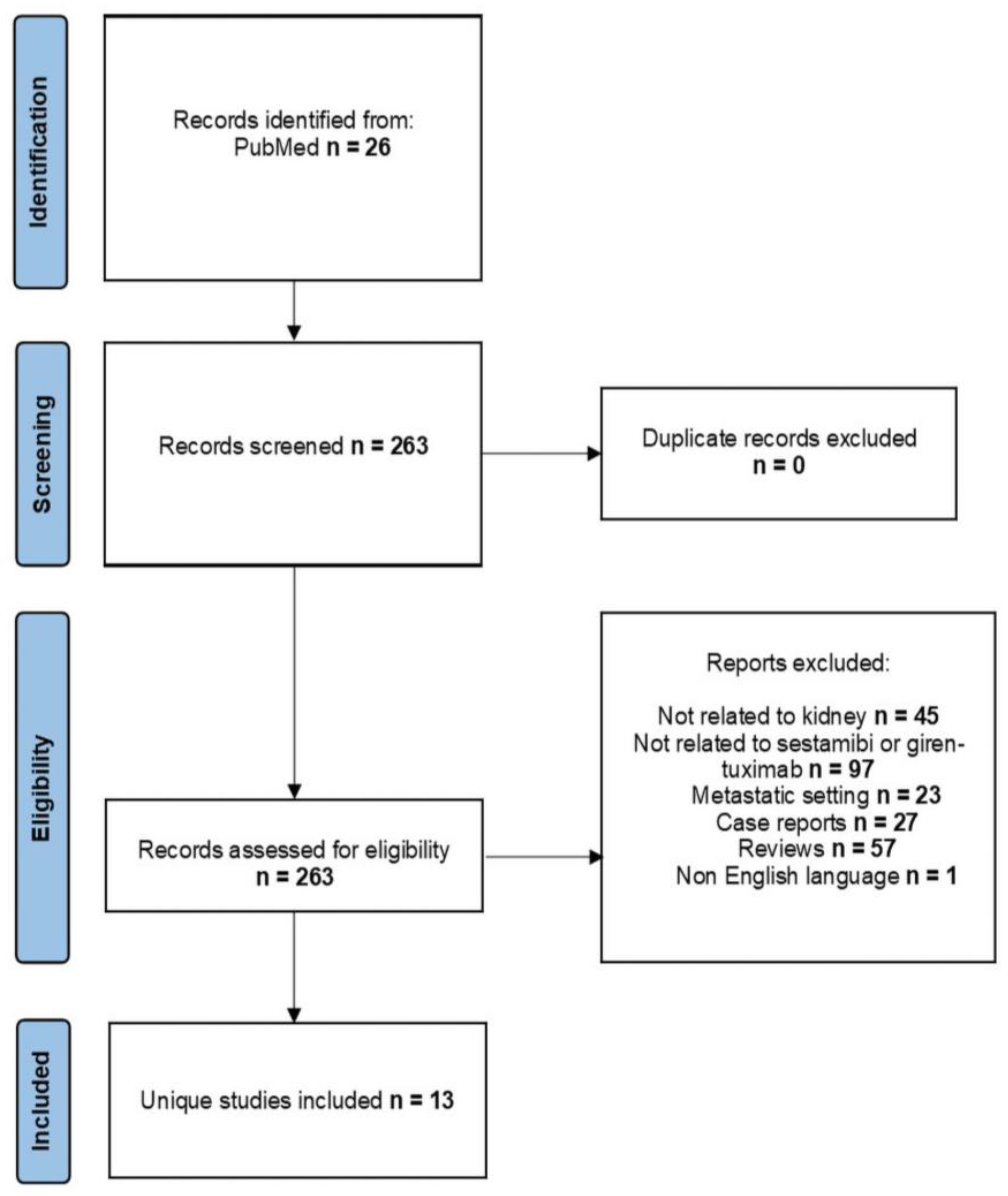
2. Materials and Methods
3. Results
3.1. Molecular Imaging
3.2. 99mTc-Sestamibi SPECT/CT
3.3. Girentuximab PET/CT
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef]
- Turner, R.M.; Morgan, T.M.; Jacobs, B.L. Epidemiology of the Small Renal Mass and the Treatment Disconnect Phenomenon. Urol. Clin. N. Am. 2017, 44, 147–154. [Google Scholar] [CrossRef]
- Meyer, A.R.; Allaf, M.E.; Rowe, S.P.; Gorin, M.A. The role of molecular imaging in the characterization of renal masses. Curr. Opin. Urol. 2018, 28, 159–165. [Google Scholar] [CrossRef]
- Williamson, S.R. Clear cell papillary renal cell carcinoma: An update after 15 years. Pathology 2021, 53, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Frank, I.; Blute, M.L.; Cheville, J.C.; Lohse, C.M.; Weaver, A.L.; Zincke, H. An outcome prediction model for patients with clear cell renal cell carcinoma treated with radical nephrectomy based on tumor stage, size, grade and necrosis: The SSIGN score. J. Urol. 2002, 168, 2395–2400. [Google Scholar] [CrossRef] [PubMed]
- Frank, I.; Blute, M.L.; Cheville, J.C.; Lohse, C.M.; Weaver, A.L.; Zincke, H. Solid renal tumors: An analysis of pathological features related to tumor size. J. Urol. 2003, 170, 2217–2220. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.P.; Vertosick, E.A.; Corradi, R.B.; Vilaseca, A.; Benfante, N.E.; Touijer, K.A.; Sjoberg, D.D.; Russo, P. Histological subtype of renal cell carcinoma significantly affects survival in the era of partial nephrectomy. Urol. Oncol. 2016, 34, 259.e1–259.e8. [Google Scholar] [CrossRef] [PubMed]
- Warren, A.Y.; Harrison, D. WHO/ISUP classification, grading and pathological staging of renal cell carcinoma: Standards and controversies. World J. Urol. 2018, 36, 1913–1926. [Google Scholar] [CrossRef]
- Kutikov, A.; Fossett, L.K.; Ramchandani, P.; Tomaszewski, J.E.; Siegelman, E.S.; Banner, M.P.; Van Arsdalen, K.N.; Wein, A.J.; Malkowicz, S.B. Incidence of benign pathologic findings at partial nephrectomy for solitary renal mass presumed to be renal cell carcinoma on preoperative imaging. Urology 2006, 68, 737–740. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.C.; Vukina, J.; Smith, A.B.; Meyer, A.-M.; Wheeler, S.B.; Kuo, T.-M.; Tan, H.-J.; Woods, M.E.; Raynor, M.C.; Wallen, E.M.; et al. Preoperatively misclassified, surgically removed benign renal masses: A systematic review of surgical series and United States population level burden estimate. J. Urol. 2015, 193, 30–35. [Google Scholar] [CrossRef]
- Yoo, S.; You, D.; Song, C.; Hong, B.; Hong, J.H.; Kim, C.-S.; Ahn, H.; Jeong, I.G. Declining incidence of benign lesions among small renal masses treated with surgery: Effect of diagnostic tests for characterization. Urol. Oncol. 2018, 36, 362.e9–362.e15. [Google Scholar] [CrossRef]
- Nandanan, N.; Veccia, A.; Antonelli, A.; Derweesh, I.; Mottrie, A.; Minervini, A.; Aron, M.; Simone, G.; Capitanio, U.; Simeone, C.; et al. Outcomes and predictors of benign histology in patients undergoing robotic partial or radical nephrectomy for renal masses: A multicenter study. Cent. Eur. J. Urol. 2020, 73, 33–38. [Google Scholar] [CrossRef]
- Amaral, B.S.; Macek, P.; Arora, A.; Pazeto, C.L.; Zugail, A.S.; Mombet, A.; Fregeville, A.; Lefevre, M.; Sanchez-Salas, R.; Cathelineau, X. Renal Tumor Biopsy: Rationale to Avoid Surgery in Small Renal Masses. Curr. Urol. Rep. 2021, 22, 46. [Google Scholar] [CrossRef]
- Richard, P.O.; Jewett, M.A.S.; Tanguay, S.; Saarela, O.; Liu, Z.A.; Pouliot, F.; Kapoor, A.; Rendon, R.; Finelli, A. Safety, reliability and accuracy of small renal tumour biopsies: Results from a multi-institution registry. BJU Int. 2017, 119, 543–549. [Google Scholar] [CrossRef]
- Renshaw, A.A.; Powell, A.; Caso, J.; Gould, E.W. Needle track seeding in renal mass biopsies. Cancer Cytopathol. 2019, 127, 358–361. [Google Scholar] [CrossRef] [PubMed]
- Garstka, N.; Shariat, S.F.; Remzi, M. The evolving role of percutaneous biopsy in renal masses. Curr. Opin. Urol. 2018, 28, 364–368. [Google Scholar] [CrossRef]
- Velez-Torres, J.; Guido, L.P.; Jorda, M. Adult Renal Neoplasms: Cytology, Immunohistochemistry, and Cytogenetic Characteristics. Surg. Pathol. Clin. 2018, 11, 611–631. [Google Scholar] [CrossRef]
- Cazzato, R.L.; De Marini, P.; Auloge, P.; Leclerc, L.; Tricard, T.; Linder, V.; Jost, M.; Ramamurthy, N.; Lang, H.; Garnon, J.; et al. Diagnostic accuracy and safety of percutaneous MRI-guided biopsy of solid renal masses: Single-center results after 4.5 years. Eur. Radiol. 2021, 31, 580–590. [Google Scholar] [CrossRef]
- Ferrari, M.; Cartolari, R.; Barizzi, J.; Pereira Mestre, R.; D’Antonio, E.; Renard, J. Percutaneous biopsy of small renal mass: Can diagnostic accuracy be affected by hospital volume? Cent. Eur. J. Urol. 2021, 74, 334–340. [Google Scholar] [CrossRef]
- Klotz, L. Overdiagnosis in urologic cancer: For World Journal of Urology Symposium on active surveillance in prostate and renal cancer. World J. Urol. 2022, 40, 1–8. [Google Scholar] [CrossRef]
- Crișan, G.; Moldovean-Cioroianu, N.S.; Timaru, D.-G.; Andrieș, G.; Căinap, C.; Chiș, V. Radiopharmaceuticals for PET and SPECT Imaging: A Literature Review over the Last Decade. Int. J. Mol. Sci. 2022, 23, 5023. [Google Scholar] [CrossRef]
- Cuocolo, A.; Petretta, M. PET and SPECT Specialty Grand Challenge. When Knowledge Travels at the Speed of Light, Photons Take to the Field. Front. Nucl. Med. 2021, 1, 671914. [Google Scholar] [CrossRef]
- van der Meulen, N.P.; Strobel, K.; Lima, T.V.M. New Radionuclides and Technological Advances in SPECT and PET Scanners. Cancers 2021, 13, 6183. [Google Scholar] [CrossRef]
- Wadsak, W.; Mitterhauser, M. Basics and principles of radiopharmaceuticals for PET/CT. Eur. J. Radiol. 2010, 73, 461–469. [Google Scholar] [CrossRef]
- Lau, J.; Rousseau, E.; Kwon, D.; Lin, K.-S.; Bénard, F.; Chen, X. Insight into the Development of PET Radiopharmaceuticals for Oncology. Cancers 2020, 12, 1312. [Google Scholar] [CrossRef]
- Lee, Y.-S. Radiopharmaceuticals for molecular imaging. Open Nucl. Med. J. 2010, 2, 178–185. [Google Scholar] [CrossRef]
- Duatti, A. Review on 99mTc radiopharmaceuticals with emphasis on new advancements. Nucl. Med. Biol. 2021, 92, 202–216. [Google Scholar] [CrossRef]
- Israel, O.; Pellet, O.; Biassoni, L.; De Palma, D.; Estrada-Lobato, E.; Gnanasegaran, G.; Kuwert, T.; la Fougère, C.; Mariani, G.; Massalha, S.; et al. Two decades of SPECT/CT—The coming of age of a technology: An updated review of literature evidence. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1990–2012. [Google Scholar] [CrossRef]
- Fahey, F.; Stabin, M. Dose optimization in nuclear medicine. Semin. Nucl. Med. 2014, 44, 193–201. [Google Scholar] [CrossRef]
- Mettler, F.A.; Huda, W.; Yoshizumi, T.T.; Mahesh, M. Effective doses in radiology and diagnostic nuclear medicine: A catalog. Radiology 2008, 248, 254–263. [Google Scholar] [CrossRef]
- Weissleder, R.; Mahmood, U. Molecular imaging. Radiology 2001, 219, 316–333. [Google Scholar] [CrossRef] [PubMed]
- Roussel, E.; Capitanio, U.; Kutikov, A.; Oosterwijk, E.; Pedrosa, I.; Rowe, S.P.; Gorin, M.A. Novel Imaging Methods for Renal Mass Characterization: A Collaborative Review. Eur. Urol. 2022, 81, 476–488. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Yang, B.; Dong, A.; Ye, H.; Cheng, C.; Pan, G.; Zuo, C. Dual-Phase 99mTc-MIBI SPECT/CT in the Characterization of Enhancing Solid Renal Tumors: A Single-Institution Study of 147 Cases. Clin. Nucl. Med. 2020, 45, 765–770. [Google Scholar] [CrossRef]
- van Oostenbrugge, T.; Mulders, P. Targeted PET/CT imaging for clear cell renal cell carcinoma with radiolabeled antibodies: Recent developments using girentuximab. Curr. Opin. Urol. 2021, 31, 249–254. [Google Scholar] [CrossRef]
- Schillaci, O.; Danieli, R.; Filippi, L.; Romano, P.; Cossu, E.; Manni, C.; Simonetti, G. Scintimammography with a hybrid SPECT/CT imaging system. Anticancer Res. 2007, 27, 557–562. [Google Scholar]
- Tiling, R.; Tatsch, K.; Sommer, H.; Meyer, G.; Pechmann, M.; Gebauer, K.; Münzing, W.; Linke, R.; Khalkhali, I.; Hahn, K. Technetium-99m-sestamibi scintimammography for the detection of breast carcinoma: Comparison between planar and SPECT imaging. J. Nucl. Med. 1998, 39, 849–856. [Google Scholar] [PubMed]
- Urbano, N.; Scimeca, M.; Bonanno, E.; Schillaci, O. 99mTc sestamibi SPECT: A possible tool for early detection of breast cancer lesions with high bone metastatic potential. Future Oncol. 2019, 15, 455–457. [Google Scholar] [CrossRef]
- Chiti, A.; Maffioli, L.S.; Infante, M.; Grasselli, G.; Incarbone, M.; Gasparini, M.D.; Savelli, G.; Bombardieri, E. Assessment of mediastinal involvement in lung cancer with technetium-99m-sestamibi SPECT. J. Nucl. Med. 1996, 37, 938–942. [Google Scholar]
- Mosci, C.; Pericole, F.V.; Oliveira, G.B.; Delamain, M.T.; Takahashi, M.E.S.; Carvalheira, J.B.C.; Etchebehere, E.C.S.C.; Santos, A.O.; Miranda, E.C.M.; Lima, M.C.L.; et al. 99mTc-sestamibi SPECT/CT and 18F-FDG-PET/CT have similar performance but different imaging patterns in newly diagnosed multiple myeloma. Nucl. Med. Commun. 2020, 41, 1081–1088. [Google Scholar] [CrossRef]
- Prigent-Le Jeune, F.; Dubois, F.; Perez, S.; Blond, S.; Steinling, M. Technetium-99m sestamibi brain SPECT in the follow-up of glioma for evaluation of response to chemotherapy: First results. Eur. J. Nucl. Med. Mol. Imaging 2004, 31, 714–719. [Google Scholar] [CrossRef]
- Lavely, W.C.; Goetze, S.; Friedman, K.P.; Leal, J.P.; Zhang, Z.; Garret-Mayer, E.; Dackiw, A.P.; Tufano, R.P.; Zeiger, M.A.; Ziessman, H.A. Comparison of SPECT/CT, SPECT, and planar imaging with single- and dual-phase (99m)Tc-sestamibi parathyroid scintigraphy. J. Nucl. Med. 2007, 48, 1084–1089. [Google Scholar] [CrossRef] [PubMed]
- Mallick, R.; Malik, J.; Yip, L.; Muthukrishnan, A.; Carty, S.E.; McCoy, K.L. Novel Findings on SPECT-CT Tc-99 Sestamibi Imaging for Primary Hyperparathyroidism. J. Surg. Res. 2020, 252, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Rowe, S.P.; Gorin, M.A.; Gordetsky, J.; Ball, M.W.; Pierorazio, P.M.; Higuchi, T.; Epstein, J.I.; Allaf, M.E.; Javadi, M.S. Initial experience using 99mTc-MIBI SPECT/CT for the differentiation of oncocytoma from renal cell carcinoma. Clin. Nucl. Med. 2015, 40, 309–313. [Google Scholar] [CrossRef]
- Gorin, M.A.; Rowe, S.P.; Baras, A.S.; Solnes, L.B.; Ball, M.W.; Pierorazio, P.M.; Pavlovich, C.P.; Epstein, J.I.; Javadi, M.S.; Allaf, M.E. Prospective Evaluation of (99m)Tc-sestamibi SPECT/CT for the Diagnosis of Renal Oncocytomas and Hybrid Oncocytic/Chromophobe Tumors. Eur. Urol. 2016, 69, 413–416. [Google Scholar] [CrossRef] [PubMed]
- Tzortzakakis, A.; Gustafsson, O.; Karlsson, M.; Ekström-Ehn, L.; Ghaffarpour, R.; Axelsson, R. Visual evaluation and differentiation of renal oncocytomas from renal cell carcinomas by means of 99mTc-sestamibi SPECT/CT. EJNMMI Res. 2017, 7, 29. [Google Scholar] [CrossRef]
- Sheikhbahaei, S.; Jones, C.S.; Porter, K.K.; Rowe, S.P.; Gorin, M.A.; Baras, A.S.; Pierorazio, P.M.; Ball, M.W.; Higuchi, T.; Johnson, P.T.; et al. Defining the Added Value of 99mTc-MIBI SPECT/CT to Conventional Cross-Sectional Imaging in the Characterization of Enhancing Solid Renal Masses. Clin. Nucl. Med. 2017, 42, e188–e193. [Google Scholar] [CrossRef]
- Jones, K.M.; Solnes, L.B.; Rowe, S.P.; Gorin, M.A.; Sheikhbahaei, S.; Fung, G.; Frey, E.C.; Allaf, M.E.; Du, Y.; Javadi, M.S. Use of quantitative SPECT/CT reconstruction in 99mTc-sestamibi imaging of patients with renal masses. Ann. Nucl. Med. 2018, 32, 87–93. [Google Scholar] [CrossRef]
- Tzortzakakis, A.; Holstensson, M.; Hagel, E.; Karlsson, M.; Axelsson, R. Intra- and Interobserver Agreement of SUV SPECT Quantitative SPECT/CT Processing Software, Applied in Clinical Settings for Patients with Solid Renal Tumors. J. Nucl. Med. Technol. 2019, 47, 258–262. [Google Scholar] [CrossRef]
- Su, Z.T.; Patel, H.D.; Huang, M.M.; Meyer, A.R.; Pavlovich, C.P.; Pierorazio, P.M.; Javadi, M.S.; Allaf, M.E.; Rowe, S.P.; Gorin, M.A. Cost-effectiveness Analysis of 99mTc-sestamibi SPECT/CT to Guide Management of Small Renal Masses. Eur. Urol. Focus 2021, 7, 827–834. [Google Scholar] [CrossRef]
- Warren, H.; Boydell, A.-R.; Reza, A.; Pencharz, D.; Holman, B.F.; El-Sheikh, S.; Wildgoose, W.H.; Barod, R.; Patki, P.; Mumtaz, F.; et al. Use of 99m Tc-sestamibi SPECT/CT for indeterminate renal tumours: A pilot diagnostic accuracy study. BJU Int. 2022, 130, 748–750. [Google Scholar] [CrossRef]
- Parihar, A.S.; Mhlanga, J.; Ronstrom, C.; Schmidt, L.R.; Figenshau, R.S.; Dehdashti, F.; Wahl, R.L. Diagnostic accuracy of 99mTc-Sestamibi SPECT/CT for characterization of solid renal masses. J. Nucl. Med. 2022, 64, 90–95. [Google Scholar] [CrossRef]
- Sistani, G.; Bjazevic, J.; Kassam, Z.; Romsa, J.; Pautler, S. The value of 99mTc-sestamibi single-photon emission computed tomography-computed tomography in the evaluation and risk stratification of renal masses. Can. Urol. Assoc. J. 2021, 15, 197–201. [Google Scholar] [CrossRef]
- Viswambaram, P.; Picardo, A.; Hohnen, A.; Pham, K.; Macdonald, W.; Hayne, D.; Hamid, A. Technetium-99 m-sestamibi single-photon emission computerised tomography (CT)/CT in the prediction of malignant versus benign small renal masses. BJU Int. 2022, 130, 23–31. [Google Scholar] [CrossRef]
- Asi, T.; Tuncali, M.Ç.; Tuncel, M.; Alkanat, N.E.İ.; Hazir, B.; Kösemehmetoğlu, K.; Baydar, D.E.; Akdoğan, B. The role of Tc-99m MIBI scintigraphy in clinical T1 renal mass assessment: Does it have a real benefit? In Proceedings of the Urologic Oncology: Seminars and Original Investigations; Elsevier: Amsterdam, The Netherlands, 2020; Volume 38, pp. 937.e11–937.e17. [Google Scholar]
- Ljungberg, B.; Albiges, L.; Abu-Ghanem, Y.; Bedke, J.; Capitanio, U.; Dabestani, S.; Fernández-Pello, S.; Giles, R.H.; Hofmann, F.; Hora, M.; et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2022 Update. Eur. Urol. 2022, 82, 399–410. [Google Scholar] [CrossRef]
- Wilson, M.P.; Katlariwala, P.; Murad, M.H.; Abele, J.; McInnes, M.D.F.; Low, G. Diagnostic accuracy of 99mTc-sestamibi SPECT/CT for detecting renal oncocytomas and other benign renal lesions: A systematic review and meta-analysis. Abdom. Radiol. 2020, 45, 2532–2541. [Google Scholar] [CrossRef]
- Rowe, S.P.; Gorin, M.A.; Solnes, L.B.; Ball, M.W.; Choudhary, A.; Pierorazio, P.M.; Epstein, J.I.; Javadi, M.S.; Allaf, M.E.; Baras, A.S. Correlation of 99mTc-sestamibi uptake in renal masses with mitochondrial content and multi-drug resistance pump expression. EJNMMI Res. 2017, 7, 80. [Google Scholar] [CrossRef]
- Oosterwijk, E.; Ruiter, D.J.; Hoedemaeker, P.J.; Pauwels, E.K.; Jonas, U.; Zwartendijk, J.; Warnaar, S.O. Monoclonal antibody G 250 recognizes a determinant present in renal-cell carcinoma and absent from normal kidney. Int. J. Cancer 1986, 38, 489–494. [Google Scholar] [CrossRef]
- Stillebroer, A.B.; Mulders, P.F.A.; Boerman, O.C.; Oyen, W.J.G.; Oosterwijk, E. Carbonic anhydrase IX in renal cell carcinoma: Implications for prognosis, diagnosis, and therapy. Eur. Urol. 2010, 58, 75–83. [Google Scholar] [CrossRef]
- Steffens, M.G.; Boerman, O.C.; Oosterwijk-Wakka, J.C.; Oosterhof, G.O.; Witjes, J.A.; Koenders, E.B.; Oyen, W.J.; Buijs, W.C.; Debruyne, F.M.; Corstens, F.H.; et al. Targeting of renal cell carcinoma with iodine-131-labeled chimeric monoclonal antibody G250. J. Clin. Oncol. 1997, 15, 1529–1537. [Google Scholar] [CrossRef]
- Lau, J.; Lin, K.-S.; Bénard, F. Past, Present, and Future: Development of Theranostic Agents Targeting Carbonic Anhydrase IX. Theranostics 2017, 7, 4322–4339. [Google Scholar] [CrossRef]
- Divgi, C.R.; Pandit-Taskar, N.; Jungbluth, A.A.; Reuter, V.E.; Gönen, M.; Ruan, S.; Pierre, C.; Nagel, A.; Pryma, D.A.; Humm, J.; et al. Preoperative characterisation of clear-cell renal carcinoma using iodine-124-labelled antibody chimeric G250 (124I-cG250) and PET in patients with renal masses: A phase I trial. Lancet Oncol. 2007, 8, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Divgi, C.R.; Uzzo, R.G.; Gatsonis, C.; Bartz, R.; Treutner, S.; Yu, J.Q.; Chen, D.; Carrasquillo, J.A.; Larson, S.; Bevan, P.; et al. Positron emission tomography/computed tomography identification of clear cell renal cell carcinoma: Results from the REDECT trial. J. Clin. Oncol. 2013, 31, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Telix International Pty Ltd. A Confirmatory, Prospective, Open-label, Multi-centre Phase 3 Study to Evaluate Diagnostic Performance of Zirconium-labelled Girentuximab to Non-invasively Detect ccRCC by PET/CT Imaging in Patients with Indeterminate Renal Masses. Available online: clinicaltrials.gov (accessed on 7 December 2022).
- Cheal, S.M.; Punzalan, B.; Doran, M.G.; Evans, M.J.; Osborne, J.R.; Lewis, J.S.; Zanzonico, P.; Larson, S.M. Pairwise comparison of 89Zr- and 124I-labeled cG250 based on positron emission tomography imaging and nonlinear immunokinetic modeling: In vivo carbonic anhydrase IX receptor binding and internalization in mouse xenografts of clear-cell renal cell carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 985–994. [Google Scholar] [CrossRef] [PubMed]
- Merkx, R.I.J.; Lobeek, D.; Konijnenberg, M.; Jiménez-Franco, L.D.; Kluge, A.; Oosterwijk, E.; Mulders, P.F.A.; Rijpkema, M. Phase I study to assess safety, biodistribution and radiation dosimetry for 89Zr-girentuximab in patients with renal cell carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 3277–3285. [Google Scholar] [CrossRef] [PubMed]
- Bertolo, R.; Autorino, R.; Simone, G.; Derweesh, I.; Garisto, J.D.; Minervini, A.; Eun, D.; Perdona, S.; Porter, J.; Rha, K.H.; et al. Outcomes of Robot-assisted Partial Nephrectomy for Clinical T2 Renal Tumors: A Multicenter Analysis (ROSULA Collaborative Group). Eur. Urol. 2018, 74, 226–232. [Google Scholar] [CrossRef]
- de Campos, N.S.P.; Souza, B.S.; da Silva, G.C.P.; Porto, V.A.; Chalbatani, G.M.; Lagreca, G.; Janji, B.; Suarez, E.R. Carbonic Anhydrase IX: A Renewed Target for Cancer Immunotherapy. Cancers 2022, 14, 1392. [Google Scholar] [CrossRef]
- Crane, P.; Laliberté, R.; Heminway, S.; Thoolen, M.; Orlandi, C. Effect of mitochondrial viability and metabolism on technetium-99m-sestamibi myocardial retention. Eur. J. Nucl. Med. 1993, 20, 20–25. [Google Scholar] [CrossRef]
- Tobe, S.W.; Noble-Topham, S.E.; Andrulis, I.L.; Hartwick, R.W.; Skorecki, K.L.; Warner, E. Expression of the multiple drug resistance gene in human renal cell carcinoma depends on tumor histology, grade, and stage. Clin. Cancer Res. 1995, 1, 1611–1615. [Google Scholar]
- Garousi, J.; Huizing, F.J.; Vorobyeva, A.; Mitran, B.; Andersson, K.G.; Leitao, C.D.; Frejd, F.Y.; Löfblom, J.; Bussink, J.; Orlova, A.; et al. Comparative evaluation of affibody- and antibody fragments-based CAIX imaging probes in mice bearing renal cell carcinoma xenografts. Sci. Rep. 2019, 9, 14907. [Google Scholar] [CrossRef]
- Rahmim, A.; Zaidi, H. PET versus SPECT: Strengths, limitations and challenges. Nucl. Med. Commun. 2008, 29, 193–207. [Google Scholar] [CrossRef]
- Minn, I.; Koo, S.M.; Lee, H.S.; Brummet, M.; Rowe, S.P.; Gorin, M.A.; Sysa-Shah, P.; Lewis, W.D.; Ahn, H.-H.; Wang, Y.; et al. [64Cu]XYIMSR-06: A dual-motif CAIX ligand for PET imaging of clear cell renal cell carcinoma. Oncotarget 2016, 7, 56471–56479. [Google Scholar] [CrossRef] [PubMed]
- Urbano, N.; Scimeca, M.; Di Russo, C.; Mauriello, A.; Bonanno, E.; Schillaci, O. [99mTc]Sestamibi SPECT Can Predict Proliferation Index, Angiogenesis, and Vascular Invasion in Parathyroid Patients: A Retrospective Study. J. Clin. Med. 2020, 9, 2213. [Google Scholar] [CrossRef] [PubMed]
- Leung, K. 1-(9H-Carbazol-4-yloxy)-3-(2-(2-[11C]methoxyphenoxy)ethylamino)-propan-2-ol. In Molecular Imaging and Contrast Agent Database (MICAD); National Center for Biotechnology Information (US): Bethesda, MD, USA, 2004. [Google Scholar]
- Leung, K. 6,7-Dimethoxy-2-{3-[4-[11C]methoxy-3,4-dihydro-2H-naphthalen-(1E)-ylidene]-propyl}-1,2,3,4-tetrahydro-isoquinoline. In Molecular Imaging and Contrast Agent Database (MICAD); National Center for Biotechnology Information (US): Bethesda, MD, USA, 2004. [Google Scholar]
- Howard, B.A. Molecular Imaging in the Head and Neck: Diagnosis and Therapy. Radiol. Clin. N. Am. 2020, 58, 1135–1146. [Google Scholar] [CrossRef] [PubMed]
- Smaldone, M.C.; Chen, D.Y.; Yu, J.Q.; Plimack, E.R. Potential role of (124)I-girentuximab in the presurgical diagnosis of clear-cell renal cell cancer. Biologics 2012, 6, 395–407. [Google Scholar] [CrossRef]
- Brouwers, A.H.; van Sluis, J.; van Snick, J.H.; Schröder, C.P.; Baas, I.O.; Boellaard, R.; Glaudemans, A.W.J.M.; Borra, R.J.H.; Lammertsma, A.A.; Dierckx, R.A.J.O.; et al. First-time imaging of [89Zr]trastuzumab in breast cancer using a long axial field-of-view PET/CT scanner. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 3593–3595. [Google Scholar] [CrossRef]
- Filippi, L.; Dimitrakopoulou-Strauss, A.; Evangelista, L.; Schillaci, O. Long axial field-of-view PET/CT devices: Are we ready for the technological revolution? Expert Rev. Med. Devices 2022, 19, 739–743. [Google Scholar] [CrossRef]
- Slart, R.H.J.A.; Tsoumpas, C.; Glaudemans, A.W.J.M.; Noordzij, W.; Willemsen, A.T.M.; Borra, R.J.H.; Dierckx, R.A.J.O.; Lammertsma, A.A. Long axial field of view PET scanners: A road map to implementation and new possibilities. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4236–4245. [Google Scholar] [CrossRef]


{kind=link}
| Authors | Study Type/No. Patients or Histological Diagnosis | Pathologic Diagnosis/Biopsy | Positive/Negative on 99mTc-Sestamibi SPECT/CT, n (%) | Results |
|---|---|---|---|---|
| Rowe et al. [43] | Evaluation prospective study/6 | Oncocytoma RCC | Yes, 3 (100%) No, 3 (100%) | Maximum radiotracer uptake similar/above adjacent renal parenchyma (average tumor uptake, 1.19; range, 0.85–1.78) Markedly photopenic relative to renal parenchyma average tumor uptake of 0.26 (range, 0.21–0.31) |
| Gorin et al. [44] | Prospective/50 | Oncocytoma HOCTs chRCC RCC | Yes, 5 (83.3%) Yes, 2 (100%) Yes, falsely 2 (50%) No, 40 (100%) | 99mTc-sestamibi SPECT/CT correctly identified 5 of 6 (83.3%) oncocytomas and 2 of 2 (100%) HOCTs Good sensitivity of 87.5% (95% CI, 47.4–99.7%) and specificity of 95.2% (95% CI, 83.8–99.4%). |
| Tzortzakakis et al. [45] | Prospective/27 | Oncocytoma HOCTs AML ccRCC papRCC chRCC ch/papRCC | Yes, 12 (91.6%) Yes, 3 (100%) Yes, 1 (100%) No, 0 No, 1 slightly positive (33.3%) No, 0 No, 0 | 91.6% of oncocytomas displayed positive uptake of 99mTc-sestamibi |
| Sheikhbahaei et al. [46] | Prospective/48 | Oncocytoma HOCTs AML RCC papRCC ccRCC Unclassified RCC chRCC | Yes, 6; (12.5%) False-positive 1 Yes, 2 (4.2%) Yes 2, (4.2%) False-positive results 1 No, 25 (52%) No, 4 (8.3%) No, 2 (4.2%) No, 1 (2.1) No, 4; (8.3%) Yes 2 falsely high uptake | AUC 0.60 to distinguish between benign and cancerous tissue for conventional imaging alone AUC 0.85 after reviewing 99mTc-sestamibi (p for difference = 0.03) |
| Zhu et al. [33] | Prospective/147 patients and 148 histopathology results | Oncocytoma AML Malignant tumors | Yes, 4 (2.7%) Yes, 8 (5.4%) No, 124 (83.8%) Partial early uptake, 7 (5.1% from malignant tumors) Partial delayed uptake, 5 (3.7% from malignant tumors) | Higher ERUV and DRUV than malignant renal tumors (n = 136; both p < 0.0001). ERUV cutoff value of 0.53 helped to differentiate benign from malignant renal tumors (DRUV of 0.50), with sensitivity of 100%, specificity of 94.8%, and accuracy of 95.3% (DRUV sensitivity 100%, specificity 96.3%, accuracy of 96.6%) for the diagnosis of benign renal tumors. |
| Parihar et al. [51] | Retrospective/36 lesions | non-concerning lesions (oncocytic or benign tumors) ccRCC | Yes, 15 (41.7%) No, 13 (36.%) | The sensitivity and specificity of SPECT/CT for discriminating oncocytic or benign tumors = 66.7%, and 89.5%, respectively, compared to 10%, and 75% for CECT, respectively. |
| Asi et al. [54] | Prospective/90 lesions | Oncocytoma AML Chronic sclerosis Fibroma Hydatic cyst chRCC ch/papRCC All RCC | Yes, 10 (11.1%) No, 4 (4.5%) No, 2 (2.2%) No, 1 (1.1%) No, 1 (1.1%) Yes, 5 (5.6%) Yes, 3 (3.3%) No, 64 (71.1%) | PPV and NPV of 60% and 91.3%, respectively for identifying benign lesions. |
| Warren et al. [50] | Prospective, pilot diagnostic accuracy/19 lesions | Oncocytoma Oncocytic RCC chRCC ccRCC papRCC histology unknown | Yes, 6 (31.657%) Yes, 1 (5.3%) Yes, 1 (5.3%) No, 9 (47.4%) No, 2 (10.5%) No, 1 (5.2%) | Qualitative assessment for sestamibi-renal images categorized as avid or photopenic has been identified as 100%. Sensitivity and specificity of sestamibi-renal to detect ch lesions from other RCCs was 100% (95% CI 74 100%) and 100% (95% CI 63–100%), respectively. Sensitivity and specificity for discriminating benign versus cancerous lesions was 100% (95% CI 54–100%) and 85.7% (95% CI 57–98%), respectively. |
| Sistani et al. [52] | Prospective, comparative study/29 patients | Oncocytoma HOCT chRCC ccRCC papRCC cc/papRCC chRCC | Yes, 7 (24.1%) Yes, 1 (3.5%) Yes, 1 low uptake (3.5%) No, 15 (51.7%) No, 4 (13.8%) No, 2 (6.9%) No, 1 (3.4%) | The benign or oncocytic tumors compared to RCCs had higher mean and maximum relative lesion uptake (p = 0.016 and 0.012, respectively). |
| Viswambaram et al. [53] | Prospective/74 patients | Accuracy to detect malignant or benign lesions | 49 (66.2%) 11 (14.8%) | Sensitivity of 89% (95% CI 77–95%) and a specificity of 73% (95% CI 45–91%) for detecting malignant or benign tumors. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tataru, O.S.; Marchioni, M.; Crocetto, F.; Barone, B.; Lucarelli, G.; Del Giudice, F.; Busetto, G.M.; Veccia, A.; Lo Giudice, A.; Russo, G.I.; et al. Molecular Imaging Diagnosis of Renal Cancer Using 99mTc-Sestamibi SPECT/CT and Girentuximab PET-CT-Current Evidence and Future Development of Novel Techniques. Diagnostics 2023, 13, 593. https://doi.org/10.3390/diagnostics13040593
Tataru OS, Marchioni M, Crocetto F, Barone B, Lucarelli G, Del Giudice F, Busetto GM, Veccia A, Lo Giudice A, Russo GI, et al. Molecular Imaging Diagnosis of Renal Cancer Using 99mTc-Sestamibi SPECT/CT and Girentuximab PET-CT-Current Evidence and Future Development of Novel Techniques. Diagnostics. 2023; 13(4):593. https://doi.org/10.3390/diagnostics13040593
Chicago/Turabian StyleTataru, Octavian Sabin, Michele Marchioni, Felice Crocetto, Biagio Barone, Giuseppe Lucarelli, Francesco Del Giudice, Gian Maria Busetto, Alessandro Veccia, Arturo Lo Giudice, Giorgio Ivan Russo, and et al. 2023. "Molecular Imaging Diagnosis of Renal Cancer Using 99mTc-Sestamibi SPECT/CT and Girentuximab PET-CT-Current Evidence and Future Development of Novel Techniques" Diagnostics 13, no. 4: 593. https://doi.org/10.3390/diagnostics13040593
APA StyleTataru, O. S., Marchioni, M., Crocetto, F., Barone, B., Lucarelli, G., Del Giudice, F., Busetto, G. M., Veccia, A., Lo Giudice, A., Russo, G. I., Luzzago, S., Piccinelli, M. L., Vartolomei, M. D., Musi, G., & Ferro, M. (2023). Molecular Imaging Diagnosis of Renal Cancer Using 99mTc-Sestamibi SPECT/CT and Girentuximab PET-CT-Current Evidence and Future Development of Novel Techniques. Diagnostics, 13(4), 593. https://doi.org/10.3390/diagnostics13040593