
Diagnostic Implications of Irritable Bowel Syndrome Is an Independent Risk Factor for Undergoing Surgical Interventions in Patients with Inflammatory Bowel Disease


Abstract
1. Introduction
2. Material and Methods
2.1. Data Source
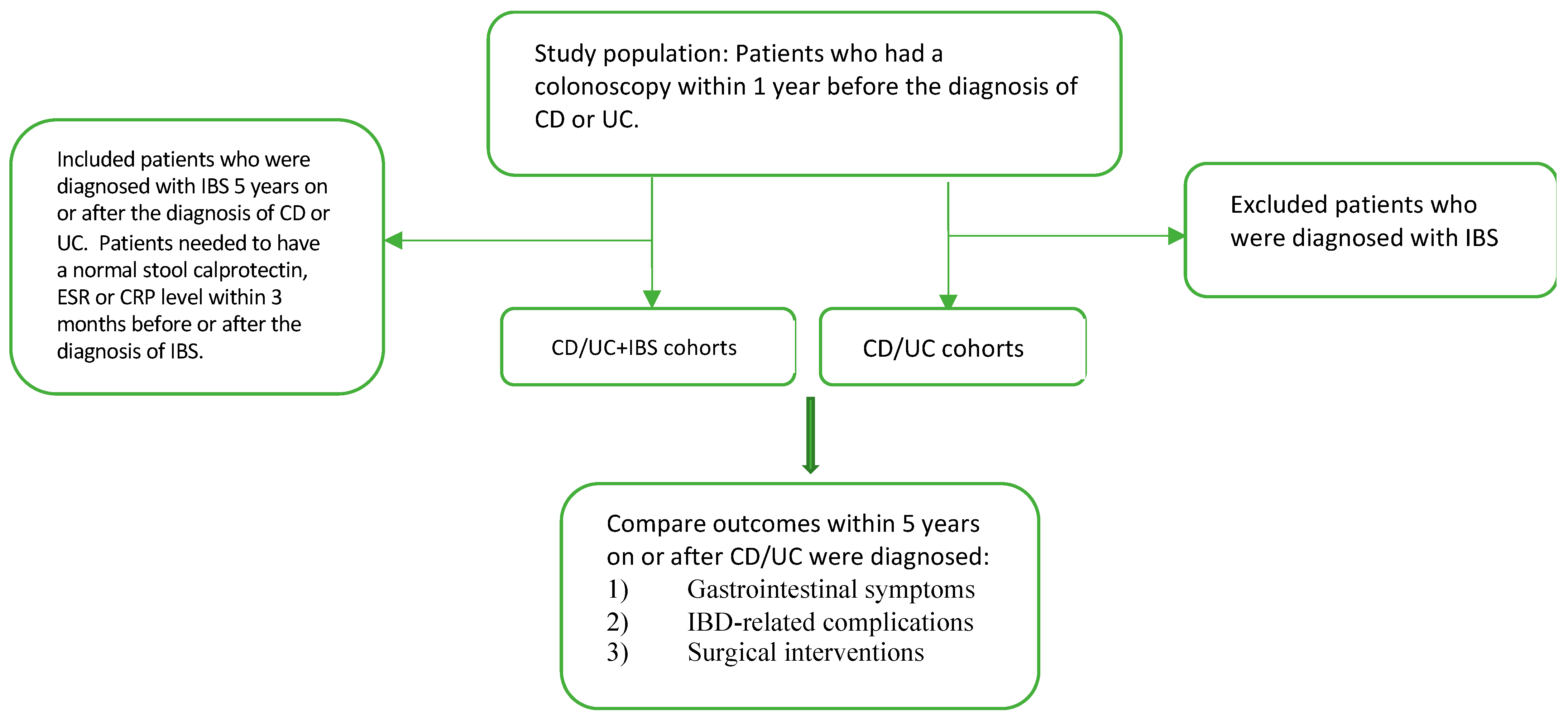
2.2. Cohort Definition
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
3.1. Population
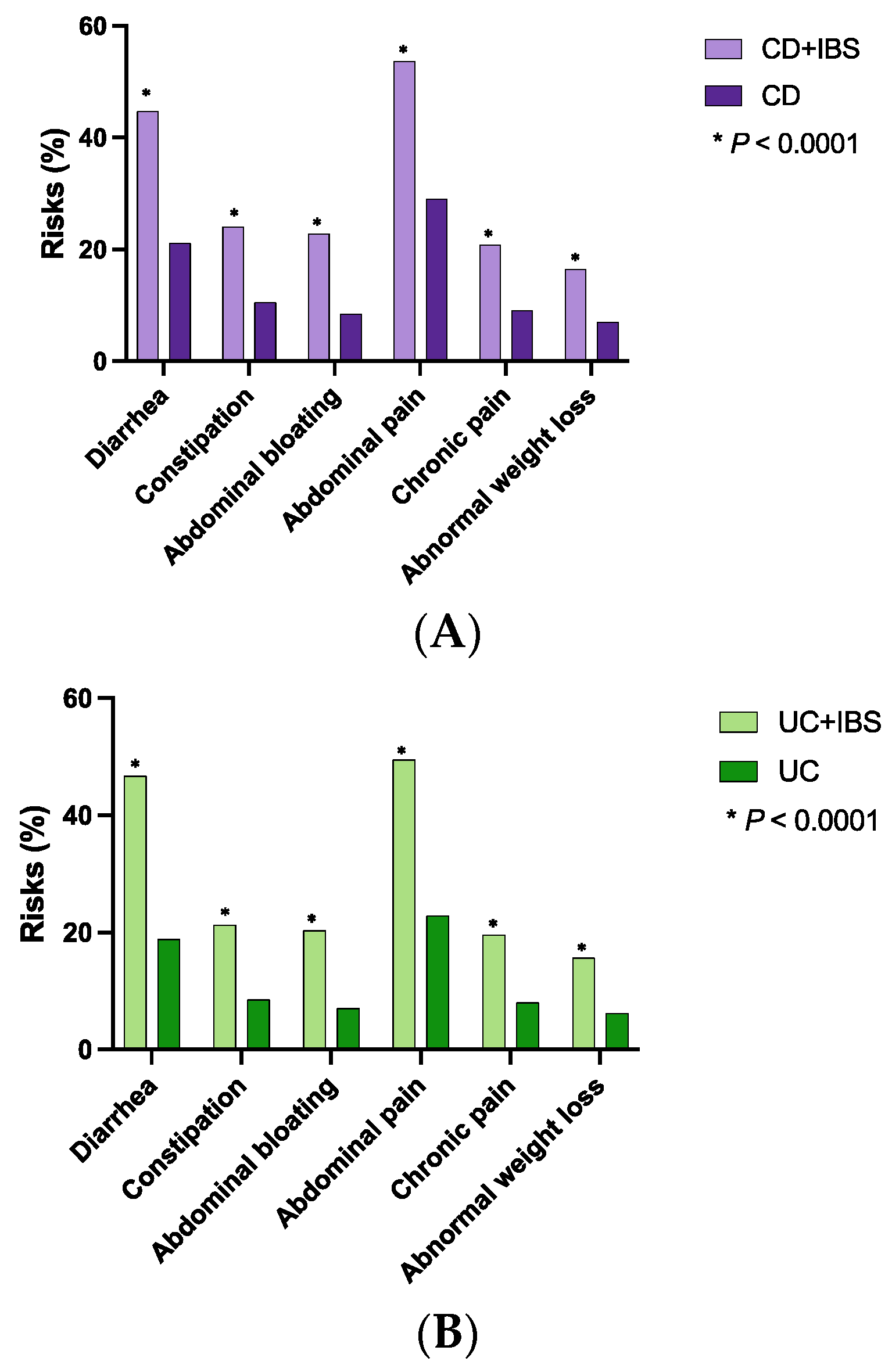
3.2. Gastrointestinal Symptoms
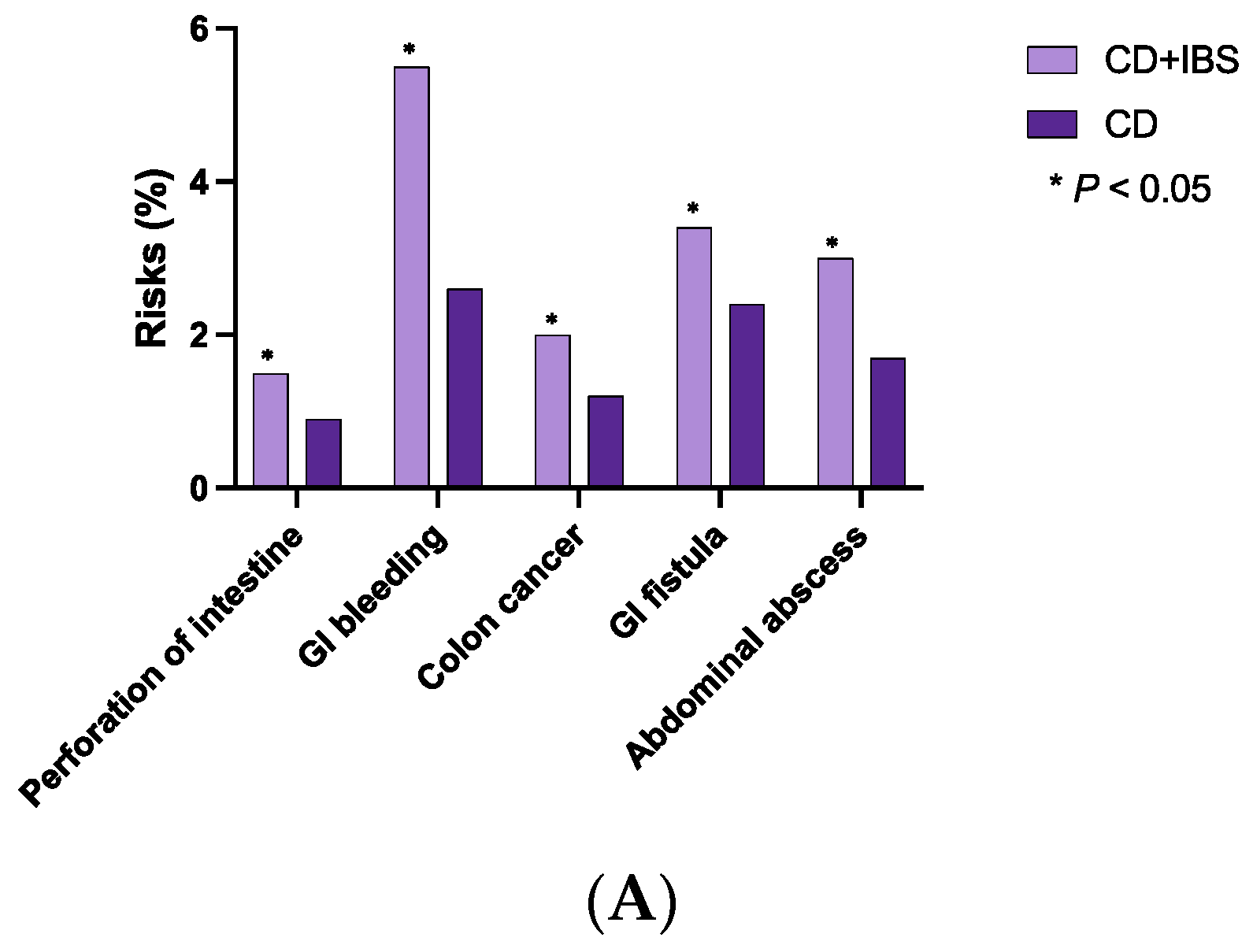
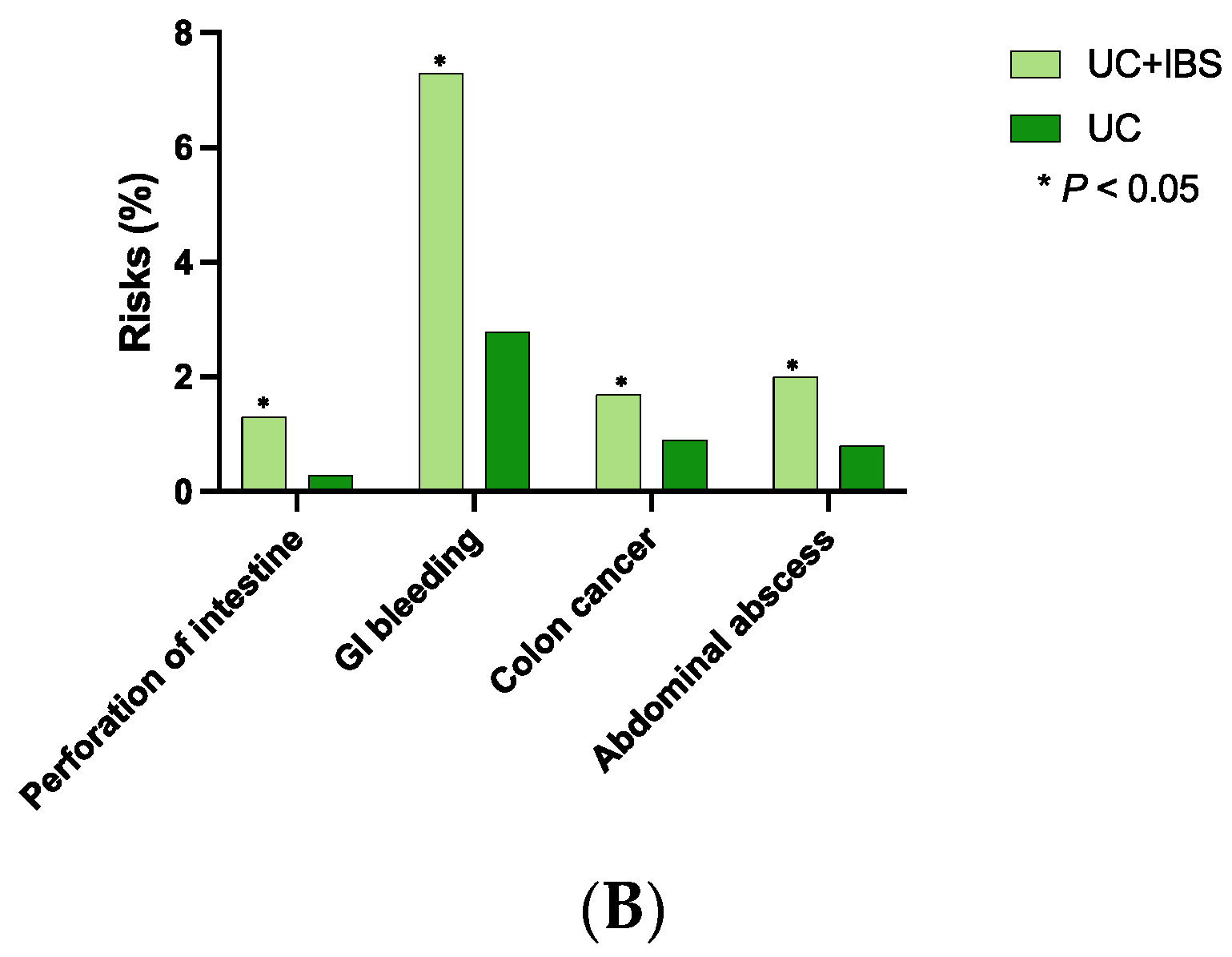
3.3. IBD-Related Complications
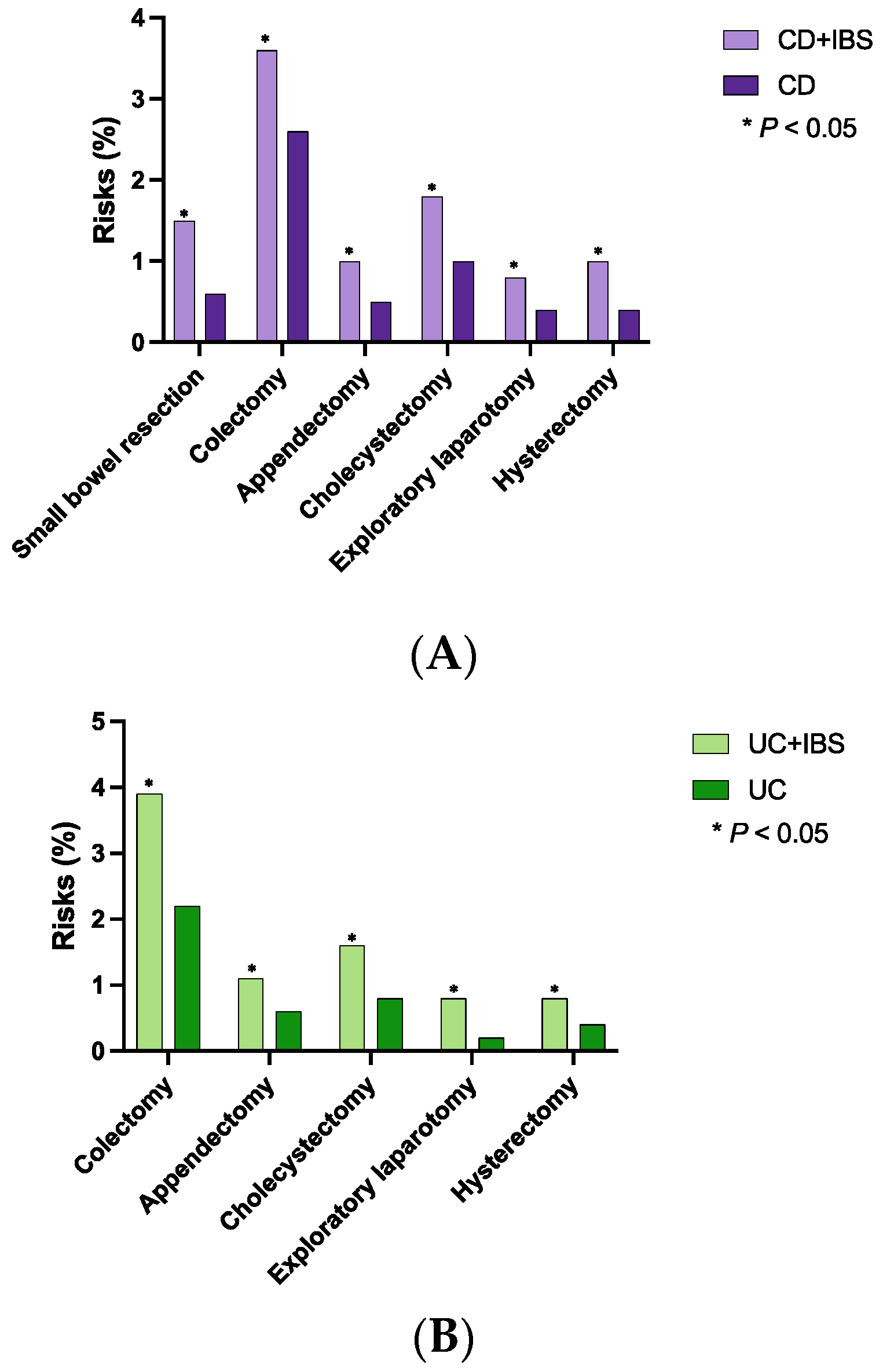
3.4. Surgical Interventions
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Szałwińska, P.; Włodarczyk, J.; Spinelli, A.; Fichna, J.; Włodarczyk, M. IBS-Symptoms in IBD Patients-Manifestation of Concomitant or Different Entities. J. Clin. Med. 2020, 10, 31. [Google Scholar] [CrossRef] [PubMed]
- Spiller, R.; Major, G. IBS and IBD—Separate entities or on a spectrum? Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Grover, M.; Herfarth, H.; Drossman, D.A. The functional-organic dichotomy: Postinfectious irritable bowel syndrome and inflammatory bowel disease-irritable bowel syndrome. Clin. Gastroenterol. Hepatol. 2009, 7, 48–53. [Google Scholar] [CrossRef]
- Fairbrass, K.M.; Costantino, S.J.; Gracie, D.J.; Ford, A.C. Prevalence of irritable bowel syndrome-type symptoms in patients with inflammatory bowel disease in remission: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 1053–1062. [Google Scholar] [CrossRef] [PubMed]
- Ancona, A.; Petito, C.; Iavarone, I.; Petito, V.; Galasso, L.; Leonetti, A.; Turchini, L.; Belella, D.; Ferrarrese, D.; Addolorato, G.; et al. The gut-brain axis in irritable bowel syndrome and inflammatory bowel disease. Dig. Liver Dis. 2021, 53, 298–305. [Google Scholar] [CrossRef]
- Gracie, D.J.; Hamlin, P.J.; Ford, A.C. The influence of the brain-gut axis in inflammatory bowel disease and possible implications for treatment. Lancet Gastroenterol. Hepatol. 2019, 4, 632–642. [Google Scholar] [CrossRef]
- Michielan, A.; D’Incà, R. Intestinal Permeability in Inflammatory Bowel Disease: Pathogenesis, Clinical Evaluation, and Therapy of Leaky Gut. Mediat. Inflamm. 2015, 2015, 628157. [Google Scholar] [CrossRef]
- Dunlop, S.P.; Hebden, J.; Campbell, E.; Naesdal, J.; Olbe, L.; Perkins, A.C.; Spiller, R.C. Abnormal intestinal permeability in subgroups of diarrhea-predominant irritable bowel syndromes. Am. J. Gastroenterol. 2006, 101, 1288–1294. [Google Scholar] [CrossRef]
- Cremon, C.; Carini, G.; Wang, B.; Vasina, V.; Cogliandro, R.F.; De Giorgio, R.; Stanghellini, V.; Grundy, D.; Tonini, M.; De Ponti, F.; et al. Intestinal serotonin release, sensory neuron activation, and abdominal pain in irritable bowel syndrome. Am. J. Gastroenterol. 2011, 106, 1290–1298. [Google Scholar] [CrossRef]
- Mittal, R.; Debs, L.H.; Patel, A.P.; Nguyen, D.; Patel, K.; O’Connor, G.; Grati, M.; Mittal, J.; Yan, D.; Eshraghi, A.A.; et al. Neurotransmitters: The Critical Modulators Regulating Gut-Brain Axis. J. Cell. Physiol. 2017, 232, 2359–2372. [Google Scholar] [CrossRef]
- Moloney, R.D.; Johnson, A.C.; O’Mahony, S.M.; Dinan, T.G.; Greenwood-Van Meerveld, B.; Cryan, J.F. Stress and the Microbiota-Gut-Brain Axis in Visceral Pain: Relevance to Irritable Bowel Syndrome. CNS Neurosci. Ther. 2016, 22, 102–117. [Google Scholar] [CrossRef] [PubMed]
- Bisgaard, T.H.; Allin, K.H.; Keefer, L.; Ananthakrishnan, A.N.; Jess, T. Depression and anxiety in inflammatory bowel disease: Epidemiology, mechanisms and treatment. Nat. Rev. Gastroenterol. Hepatol. 2022, 19, 717–726. [Google Scholar] [CrossRef] [PubMed]
- Piacentino, D.; Cesarini, M.; Badiali, D.; Pallotta, N.; Biondi, M.; Corazziari, E.S. The central role of psychopathology and its association with disease severity in inflammatory bowel disease and irritable bowel syndrome. Riv. Psichiatr. 2019, 54, 75–83. [Google Scholar] [CrossRef]
- Annaházi, A.; Schemann, M. Contribution of the Enteric Nervous System to Autoimmune Diseases and Irritable Bowel Syndrome. Adv. Exp. Med. Biol. 2022, 1383, 1–8. [Google Scholar] [CrossRef]
- Ni, J.; Wu, G.D.; Albenberg, L.; Tomov, V.T. Gut microbiota and IBD: Causation or correlation? Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 573–584. [Google Scholar] [CrossRef] [PubMed]
- Perera, L.P.; Radigan, M.; Guilday, C.; Banerjee, I.; Eastwood, D.; Babygirija, R.; Massey, B.T. Presence of Irritable Bowel Syndrome Symptoms in Quiescent Inflammatory Bowel Disease Is Associated with High Rate of Anxiety and Depression. Dig. Dis. Sci. 2019, 64, 1923–1928. [Google Scholar] [CrossRef]
- Pedersen, N.; Ankersen, D.V.; Felding, M.; Wachmann, H.; Végh, Z.; Molzen, L.; Burisch, J.; Andersen, J.R.; Munkholm, P. Low-FODMAP diet reduces irritable bowel symptoms in patients with inflammatory bowel disease. World J. Gastroenterol. 2017, 23, 3356–3366. [Google Scholar] [CrossRef]
- Hoekman, D.R.; Vlieger, A.M.; Stokkers, P.C.; Mahhmod, N.; Rietdijk, S.; de Boer, N.K.; de Meij, T.G.; Frankenhuis, C.; D’Haens, G.R.; Benninga, M.A. Hypnotherapy for Irritable Bowel Syndrome-Type Symptoms in Patients with Quiescent Inflammatory Bowel Disease: A Randomized, Controlled Trial. J. Crohns Colitis 2021, 15, 1106–1113. [Google Scholar] [CrossRef]
- Oka, P.; Parr, H.; Barberio, B.; Black, C.J.; Savarino, E.V.; Ford, A.C. Global prevalence of irritable bowel syndrome according to Rome III or IV criteria: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 908–917. [Google Scholar] [CrossRef]
- Camilleri, M. Diagnosis and Treatment of Irritable Bowel Syndrome: A Review. Jama 2021, 325, 865–877. [Google Scholar] [CrossRef]
- Sands, B.E. Biomarkers of Inflammation in Inflammatory Bowel Disease. Gastroenterology 2015, 149, 1275–1285.e1272. [Google Scholar] [CrossRef] [PubMed]
- Colombel, J.F.; Shin, A.; Gibson, P.R. AGA Clinical Practice Update on Functional Gastrointestinal Symptoms in Patients With Inflammatory Bowel Disease: Expert Review. Clin. Gastroenterol. Hepatol. 2019, 17, 380–390.e381. [Google Scholar] [CrossRef] [PubMed]
- Gallo, G.; Kotze, P.G.; Spinelli, A. Surgery in ulcerative colitis: When? How? Best. Pract. Res. Clin. Gastroenterol. 2018, 32–33, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Meima-van Praag, E.M.; Buskens, C.J.; Hompes, R.; Bemelman, W.A. Surgical management of Crohn’s disease: A state of the art review. Int. J. Colorectal Dis. 2021, 36, 1133–1145. [Google Scholar] [CrossRef]
- Hasler, W.L.; Schoenfeld, P. Systematic review: Abdominal and pelvic surgery in patients with irritable bowel syndrome. Aliment. Pharmacol. Ther. 2003, 17, 997–1005. [Google Scholar] [CrossRef]
- Longstreth, G.F.; Yao, J.F. Irritable bowel syndrome and surgery: A multivariable analysis. Gastroenterology 2004, 126, 1665–1673. [Google Scholar] [CrossRef]
- Larabi, A.; Barnich, N.; Nguyen, H.T.T. New insights into the interplay between autophagy, gut microbiota and inflammatory responses in IBD. Autophagy 2020, 16, 38–51. [Google Scholar] [CrossRef]
- Hillestad, E.M.R.; van der Meeren, A.; Nagaraja, B.H.; Bjørsvik, B.R.; Haleem, N.; Benitez-Paez, A.; Sanz, Y.; Hausken, T.; Lied, G.A.; Lundervold, A.; et al. Gut bless you: The microbiota-gut-brain axis in irritable bowel syndrome. World J. Gastroenterol. 2022, 28, 412–431. [Google Scholar] [CrossRef]
- Vich Vila, A.; Imhann, F.; Collij, V.; Jankipersadsing, S.A.; Gurry, T.; Mujagic, Z.; Kurilshikov, A.; Bonder, M.J.; Jiang, X.; Tigchelaar, E.F.; et al. Gut microbiota composition and functional changes in inflammatory bowel disease and irritable bowel syndrome. Sci. Transl. Med. 2018, 10, eaap8914. [Google Scholar] [CrossRef]
- Camilleri, M.; Madsen, K.; Spiller, R.; Greenwood-Van Meerveld, B.; Verne, G.N. Intestinal barrier function in health and gastrointestinal disease. Neurogastroenterol. Motil. 2012, 24, 503–512. [Google Scholar] [CrossRef]
- Ng, Q.X.; Soh, A.Y.S.; Loke, W.; Lim, D.Y.; Yeo, W.S. The role of inflammation in irritable bowel syndrome (IBS). J. Inflamm. Res. 2018, 11, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Aguilera-Lizarraga, J.; Hussein, H.; Boeckxstaens, G.E. Immune activation in irritable bowel syndrome: What is the evidence? Nat. Rev. Immunol. 2022, 22, 674–686. [Google Scholar] [CrossRef] [PubMed]
- Longstreth, G.F. Avoiding unnecessary surgery in irritable bowel syndrome. Gut 2007, 56, 608–610. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, T.M.; Jones, R.H. Epidemiology of cholecystectomy and irritable bowel syndrome in a UK population. Br. J. Surg. 2000, 87, 1658–1663. [Google Scholar] [CrossRef] [PubMed]
- Corazziari, E.; Attili, A.F.; Angeletti, C.; De Santis, A. Gallstones, cholecystectomy and irritable bowel syndrome (IBS) MICOL population-based study. Dig. Liver Dis. 2008, 40, 944–950. [Google Scholar] [CrossRef]
- Kennedy, T.M.; Jones, R.H. The epidemiology of hysterectomy and irritable bowel syndrome in a UK population. Int. J. Clin. Pract. 2000, 54, 647–650. [Google Scholar] [CrossRef]
- Chaudhary, N.A.; Truelove, S.C. The irritable colon syndrome. A study of the clinical features, predisposing causes, and prognosis in 130 cases. QJM Int. J. Med. 1962, 31, 307–322. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A | |||||||||
| Unadjusted Data | After Propensity-Score Matching | ||||||||
| CD + IBS | CD without IBS | p-Value | SD | CD + IBS | CD without IBS | p-Value | SD | ||
| N of patients | 5510 | 60,180 | 5389 | 5389 | |||||
| Average age | 38.0 ± 18.2 | 40.3 ± 19.4 | <0.001 | 0.122 | 38.0 ± 18.2 | 38.0 ± 18.1 | 0.962 | 0.001 | |
| Gender | Female | 3396 (63.0%) | 28,870 (49.3%) | <0.001 | 0.28 | 3396 (63.0%) | 3392 (62.9%) | 0.936 | 0.002 |
| Male | 1838 (34.1%) | 27,651 (47.2%) | <0.001 | 0.269 | 1838 (34.1%) | 1838 (34.1%) | 1.000 | <0.001 | |
| Race | White | 4405 (81.7%) | 44,580 (76.1%) | <0.001 | 0.139 | 4405 (81.7%) | 4413 (81.9%) | 0.842 | 0.004 |
| Unknown | 420 (7.8%) | 6788 (11.6%) | <0.001 | 0.128 | 420 (7.8%) | 422 (7.8%) | 0.943 | 0.001 | |
| Black or African American | 486 (9.0%) | 6144 (10.5%) | 0.001 | 0.049 | 486 (9.0%) | 485 (9.0%) | 0.973 | 0.001 | |
| Asian | 54 (1.0%) | 915 (1.6%) | 0.001 | 0.05 | 54 (1.0%) | 55 (1.0%) | 0.923 | 0.002 | |
| Ethnicity | Hispanic or Latino | 231 (4.3%) | 2451 (4.2%) | 0.716 | 0.005 | 231 (4.3%) | 231 (4.3%) | 1.000 | <0.001 |
| Not Hispanic or Latino | 4619 (85.7%) | 46,235 (78.9%) | <0.001 | 0.179 | 4619 (85.7%) | 4622 (85.8%) | 0.934 | 0.002 | |
| Unknown | 539 (10.0%) | 9914 (16.9%) | <0.001 | 0.204 | 539 (10.0%) | 536 (9.9%) | 0.923 | 0.002 | |
| B | |||||||||
| Unadjusted Data | After Propensity-Score Matching | ||||||||
| UC + IBS | UC without IBS | p-Value | SD | UC + IBS | UC without IBS | p-Value | SD | ||
| N of patients | 4200 | 67,639 | 4115 | 4115 | |||||
| Average age | 41.1 ± 19.5 | 47.5 ± 19.3 | <0.001 | 0.332 | 41.1 ± 19.5 | 41.2 ± 19.5 | 0.816 | 0.005 | |
| Gender | Female | 2484 (60.4%) | 31,284 (47.3%) | <0.001 | 0.264 | 2484 (60.4%) | 2482 (60.3%) | 0.964 | 0.001 |
| Male | 1484 (36.1%) | 31,784 (48.1%) | <0.001 | 0.245 | 1484 (36.1%) | 1485 (36.1%) | 0.982 | 0.001 | |
| Race | White | 3314 (80.5%) | 49,608 (75.0%) | <0.001 | 0.133 | 3314 (80.5%) | 3324 (80.8%) | 0.780 | 0.006 |
| Unknown | 360 (8.7%) | 7903 (12.0%) | <0.001 | 0.105 | 360 (8.7%) | 367 (8.9%) | 0.786 | 0.006 | |
| Black or African American | 363 (8.8%) | 7010 (10.6%) | <0.001 | 0.06 | 363 (8.8%) | 357 (8.7%) | 0.815 | 0.005 | |
| Asian | 61 (1.5%) | 1365 (2.1%) | 0.010 | 0.044 | 61 (1.5%) | 55 (1.3%) | 0.575 | 0.012 | |
| Ethnicity | Hispanic or Latino | 210 (5.1%) | 3864 (5.8%) | 0.049 | 0.033 | 210 (5.1%) | 208 (5.1%) | 0.920 | 0.002 |
| Not Hispanic or Latino | 3457 (84.0%) | 49,528 (74.9%) | <0.001 | 0.227 | 3457 (84.0%) | 3464 (84.2%) | 0.833 | 0.005 | |
| Unknown | 448 (10.9%) | 12,737 (19.3%) | <0.001 | 0.236 | 448 (10.9%) | 443 (10.8%) | 0.859 | 0.004 | |
| A | ||||||||
| CD + IBS | CD without IBS | CD + IBS vs. CD without IBS | ||||||
| N | Risk | N | Risk | Risk Difference | OR | p | ||
| Symptoms | Diarrhea | 958 | 44.8% | 695 | 21.2% | 23.58% (21.05–26.11%) | 3.02 (2.68–3.40) | <0.0001 |
| Constipation | 924 | 24.1% | 482 | 10.6% | 13.54% (11.91–15.16%) | 2.68 (2.38–3.03) | <0.0001 | |
| Abdominal bloating | 976 | 22.9% | 413 | 8.5% | 14.42% (12.93–15.90%) | 3.20 (2.83–3.62) | <0.0001 | |
| Abdominal pain | 789 | 53.7% | 717 | 29.1% | 24.59% (21.47–27.70%) | 2.83 (2.47–3.23) | <0.0001 | |
| Chronic pain | 928 | 20.9% | 442 | 9.1% | 11.82% (10.38–13.27%) | 2.65 (2.34–2.99) | <0.0001 | |
| Abnormal weight loss | 693 | 16.5% | 329 | 7.1% | 9.36% (8.01–10.70%) | 2.57 (2.24–2.95) | <0.0001 | |
| Complications | Perforation of intestine | 80 | 1.5% | 47 | 0.9% | 0.62% (0.21–1.03%) | 1.71 (1.19–2.46) | 0.0032 |
| GI bleeding | 271 | 5.5% | 133 | 2.6% | 2.91% (2.13–3.68%) | 2.18 (1.77–2.70) | <0.0001 | |
| Colon cancer | 106 | 2.0% | 65 | 1.2% | 0.79% (0.30–1.27%) | 1.65 (1.21–2.26) | 0.0014 | |
| GI fistula | 178 | 3.4% | 125 | 2.4% | 1.02% (0.38–1.66%) | 1.44 (1.14–1.82) | 0.0019 | |
| Abdominal abscess | 156 | 3.0% | 91 | 1.7% | 1.26% (0.68–1.84%) | 1.75 (1.35–2.28) | <0.0001 | |
| Surgeries | Small bowel resection | 80 | 1.5% | 31 | 0.6% | 0.92% (0.54–1.30%) | 2.61 (1.72–3.96) | <0.0001 |
| Colectomy | 190 | 3.6% | 137 | 2.6% | 1.01% (0.35–1.67%) | 1.41 (1.13–1.76) | 0.0026 | |
| Appendectomy | 51 | 1.0% | 25 | 0.5% | 0.49% (0.17–0.81%) | 2.06 (1.27–3.32) | 0.0026 | |
| Cholecystectomy | 93 | 1.8% | 52 | 1.0% | 0.80% (0.35–1.24%) | 1.83 (1.30–2.58) | 0.0004 | |
| Exploratory laparotomy | 45 | 0.8% | 24 | 0.4% | 0.39% (0.09–0.70%) | 1.89 (1.15–3.10) | 0.011 | |
| Hysterectomy | 54 | 1.0% | 24 | 0.4% | 0.57% (0.24–0.89%) | 2.27 (1.40–3.68) | 0.0006 | |
| B | ||||||||
| UC + IBS | UC without IBS | UC + IBS vs. UC without IBS | ||||||
| N | Risk | N | Risk | Risk Difference | OR | p | ||
| Symptoms | Diarrhea | 743 | 46.80% | 469 | 18.90% | 27.86% (24.96–30.76%) | 3.77 (3.27–4.34) | <0.0001 |
| Constipation | 627 | 21.30% | 299 | 8.60% | 12.69% (10.93–14.44%) | 2.86 (2.47–3.32) | <0.0001 | |
| Abdominal bloating | 672 | 20.40% | 269 | 7.10% | 13.22% (11.62–14.82%) | 3.32 (2.86–3.86) | <0.0001 | |
| Abdominal pain | 656 | 49.50% | 497 | 22.90% | 26.68% (23.46–29.90%) | 3.31 (2.86–3.84) | <0.0001 | |
| Chronic pain | 667 | 19.60% | 300 | 8.10% | 11.48% (9.89–13.07%) | 2.77 (2.39–3.20) | <0.0001 | |
| Abnormal weight loss | 515 | 15.70% | 223 | 6.20% | 9.56% (8.09–11.03%) | 2.84 (2.41–3.35) | <0.0001 | |
| Complications | Perforation of intestine | 52 | 1.30% | 14 | 0.30% | 0.94% (0.55–1.32%) | 3.77 (2.09–6.81) | <0.0001 |
| GI bleeding | 265 | 7.30% | 105 | 2.80% | 4.54% (3.54–5.53%) | 2.77 (2.20–3.49) | <0.0001 | |
| Colon cancer | 68 | 1.70% | 37 | 0.90% | 0.78% (0.28–1.27%) | 1.86 (1.24–2.78) | 0.0022 | |
| Abdominal abscess | 79 | 2.00% | 32 | 0.80% | 1.17% (0.66–1.67%) | 2.52 (1.66–3.80) | <0.0001 | |
| Surgeries | Colectomy | 158 | 3.90% | 88 | 2.20% | 1.74% (0.99–2.48%) | 1.84 (1.41–2.39) | <0.0001 |
| Appendectomy | 43 | 1.10% | 24 | 0.60% | 0.47% (0.08–0.86%) | 1.80 (1.09–2.98) | 0.0195 | |
| Cholecystectomy | 66 | 1.60% | 34 | 0.80% | 0.81% (0.32–1.29%) | 1.98 (1.31–3.00) | 0.0011 | |
| Exploratory laparotomy | 32 | 0.80% | 10 | 0.20% | 0.54% (0.23–0.85%) | 3.22 (1.58–6.56) | 0.0007 | |
| Hysterectomy | 34 | 0.80% | 16 | 0.40% | 0.44% (0.11–0.78%) | 2.14 (1.18–3.89) | 0.0103 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, Y.; Waghray, N.; Fass, R.; Song, G. Diagnostic Implications of Irritable Bowel Syndrome Is an Independent Risk Factor for Undergoing Surgical Interventions in Patients with Inflammatory Bowel Disease. Diagnostics 2023, 13, 1901. https://doi.org/10.3390/diagnostics13111901
Fu Y, Waghray N, Fass R, Song G. Diagnostic Implications of Irritable Bowel Syndrome Is an Independent Risk Factor for Undergoing Surgical Interventions in Patients with Inflammatory Bowel Disease. Diagnostics. 2023; 13(11):1901. https://doi.org/10.3390/diagnostics13111901
Chicago/Turabian StyleFu, Yuhan, Nisheet Waghray, Ronnie Fass, and Gengqing Song. 2023. "Diagnostic Implications of Irritable Bowel Syndrome Is an Independent Risk Factor for Undergoing Surgical Interventions in Patients with Inflammatory Bowel Disease" Diagnostics 13, no. 11: 1901. https://doi.org/10.3390/diagnostics13111901
APA StyleFu, Y., Waghray, N., Fass, R., & Song, G. (2023). Diagnostic Implications of Irritable Bowel Syndrome Is an Independent Risk Factor for Undergoing Surgical Interventions in Patients with Inflammatory Bowel Disease. Diagnostics, 13(11), 1901. https://doi.org/10.3390/diagnostics13111901