
Nomogram Predicting the Survival of Young-Onset Patients with Colorectal Cancer Liver Metastases


Abstract
:1. Introduction
2. Materials and Methods
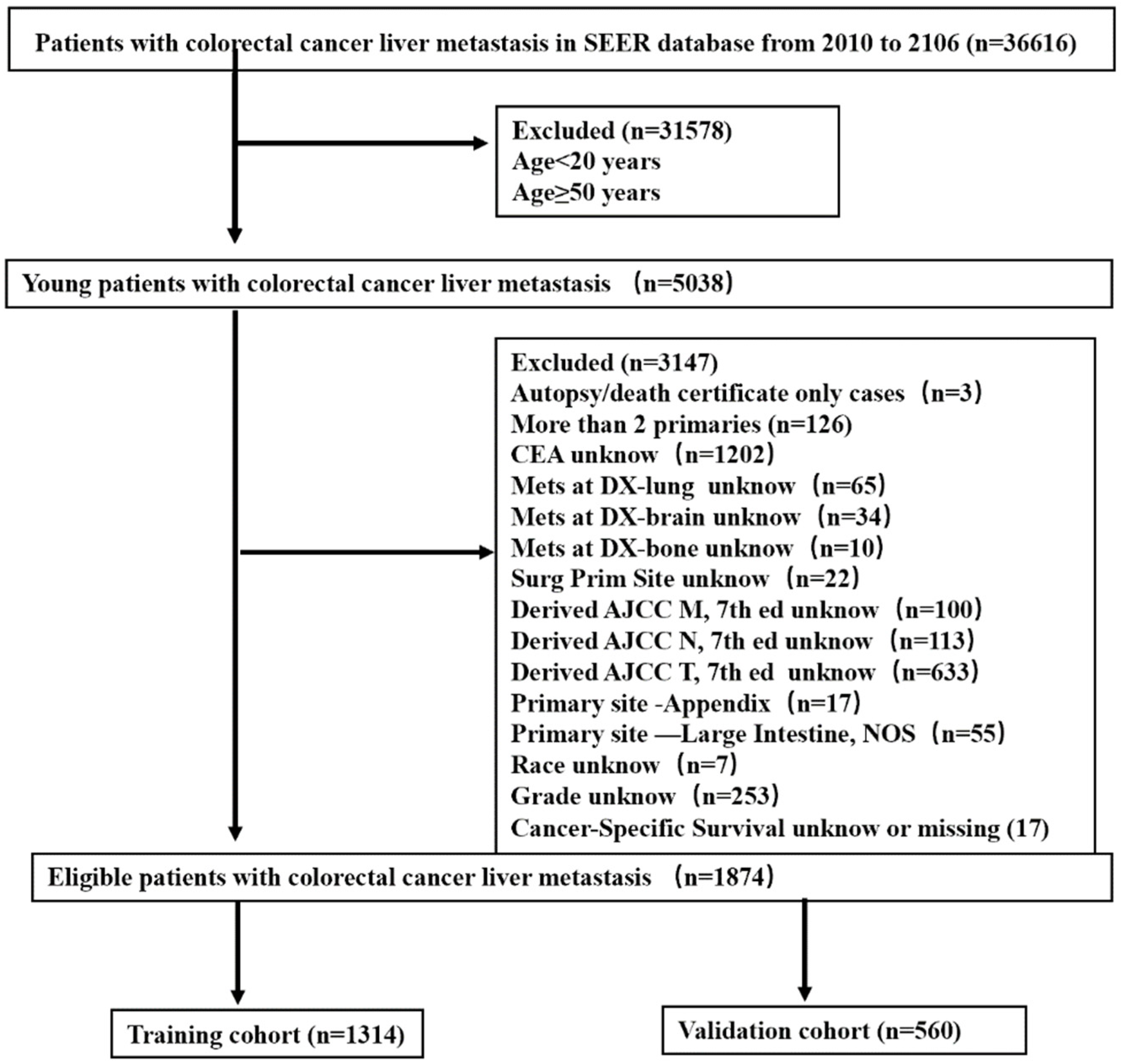
2.1. Patients
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Basic Patient Characteristics
3.2. Independent Features Predictive of Prognosis in Young-Onset Patients with CRLM
3.3. Construction of the Nomogram
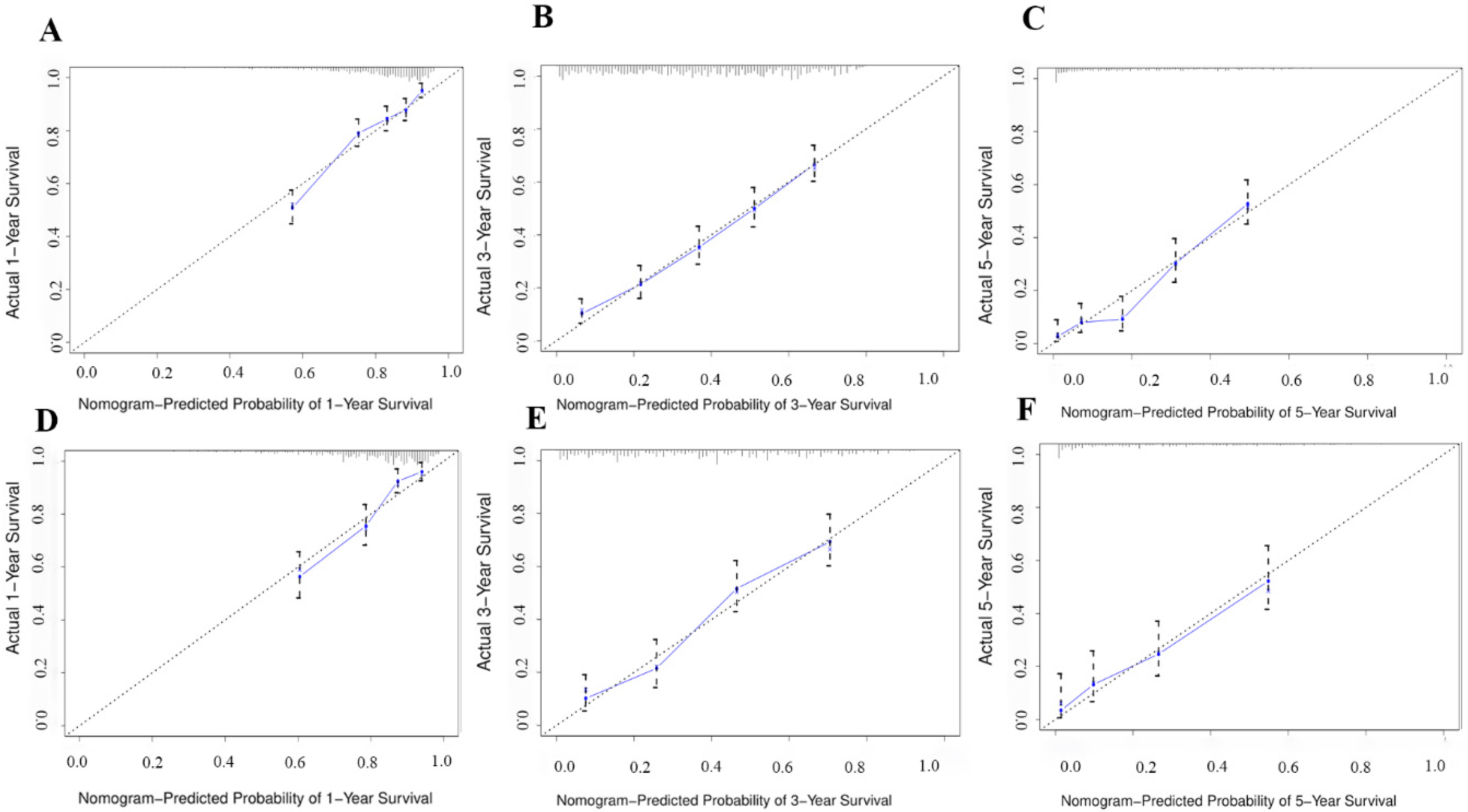
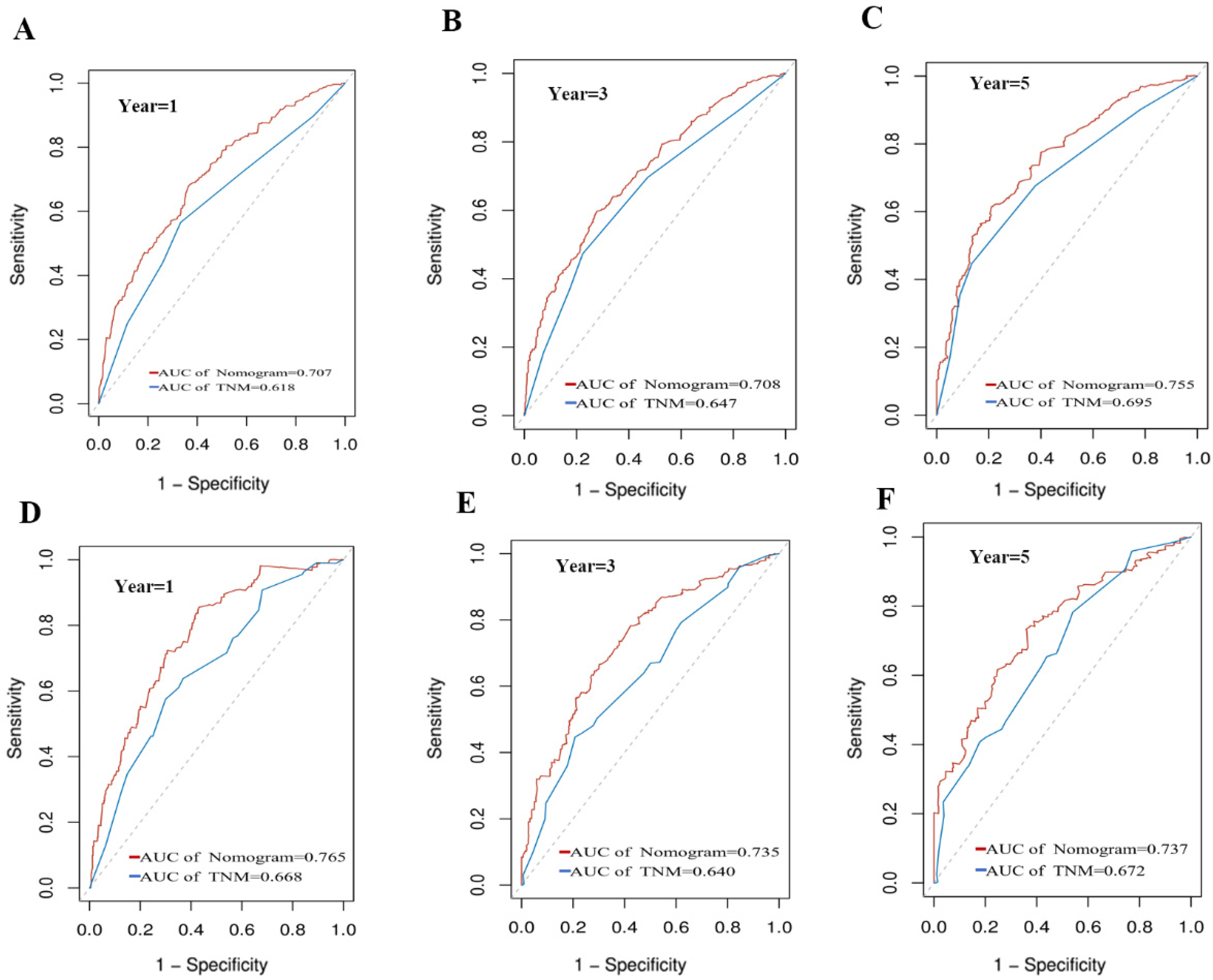
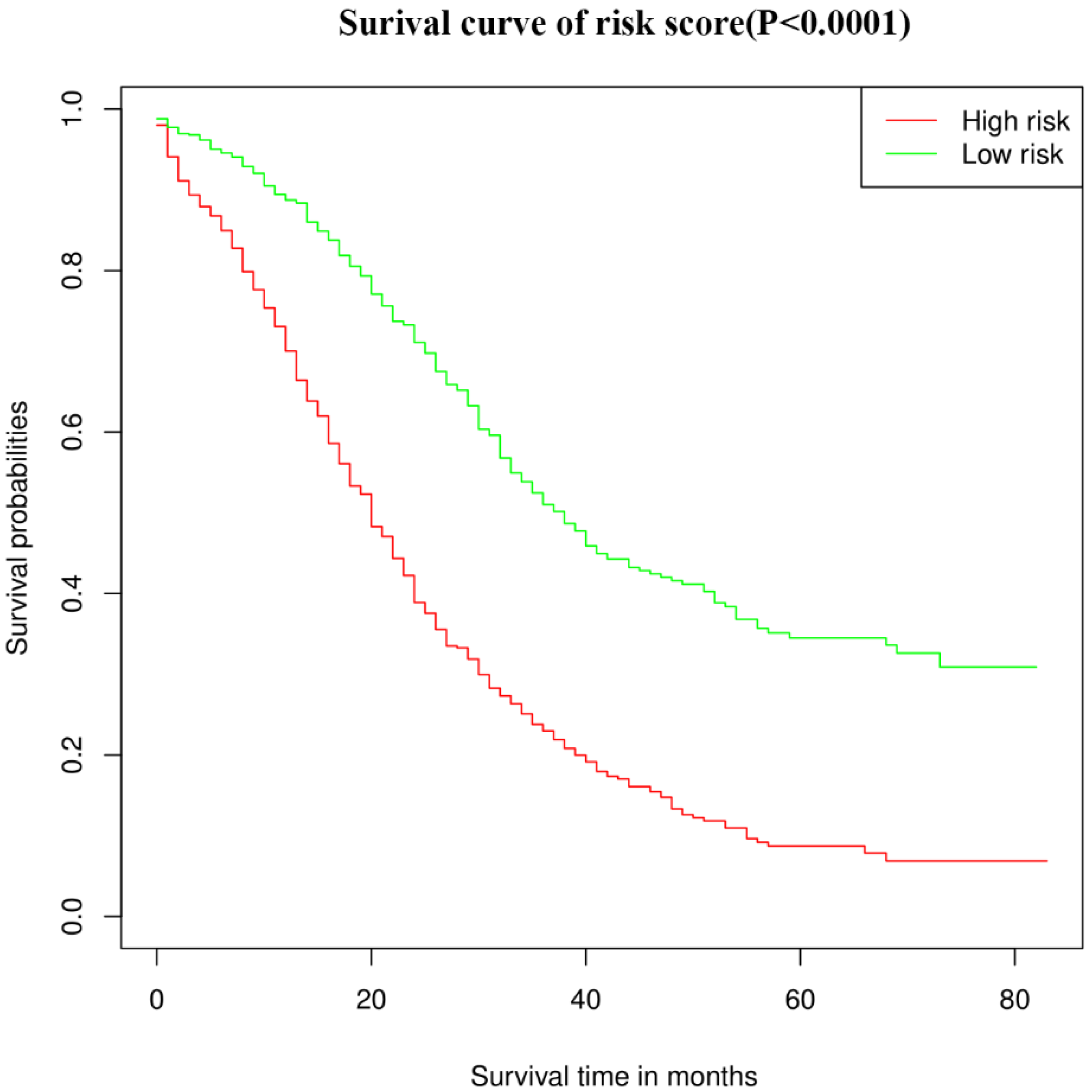
3.4. Validation of the Nomogram
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welch, H.G.; Robertson, D.J. Colorectal Cancer on the Decline--Why Screening Can’t Explain It All. N. Engl. J. Med. 2016, 374, 1605–1607. [Google Scholar] [CrossRef] [PubMed]
- Chambers, A.C.; Dixon, S.W.; White, P.; Williams, A.C.; Thomas, M.G.; Messenger, D.E. Demographic trends in the incidence of young-onset colorectal cancer: A population-based study. Br. J. Surg. 2020, 107, 595–605. [Google Scholar] [CrossRef] [PubMed]
- Sultan, I.; Rodriguez-Galindo, C.; El-Taani, H.; Pastore, G.; Casanova, M.; Gallino, G.; Ferrari, A. Distinct features of colorectal cancer in children and adolescents: A population-based study of 159 cases. Cancer 2010, 116, 758–765. [Google Scholar] [CrossRef]
- Lipsyc-Sharf, M.; Zhang, S.; Ou, F.S.; Ma, C.; McCleary, N.J.; Niedzwiecki, D.; Chang, I.W.; Lenz, H.J.; Blanke, C.D.; Piawah, S.; et al. Survival in Young-Onset Metastatic Colorectal Cancer: Findings from Cancer and Leukemia Group B (Alliance)/SWOG 80405. J. Natl. Cancer Inst. 2022, 114, 427–435. [Google Scholar] [CrossRef]
- Willauer, A.N.; Liu, Y.; Pereira, A.A.L.; Lam, M.; Morris, J.S.; Raghav, K.P.S.; Morris, V.K.; Menter, D.; Broaddus, R.; Meric-Bernstam, F.; et al. Clinical and molecular characterization of early-onset colorectal cancer. Cancer 2019, 125, 2002–2010. [Google Scholar] [CrossRef] [PubMed]
- Kuipers, E.J.; Grady, W.M.; Lieberman, D.; Seufferlein, T.; Sung, J.J.; Boelens, P.G.; van de Velde, C.J.; Watanabe, T. Colorectal cancer. Nat. Rev. Dis. Primers 2015, 1, 15065. [Google Scholar] [CrossRef] [Green Version]
- Done, J.Z.; Fang, S.H. Young-onset colorectal cancer: A review. World J. Gastrointest. Oncol. 2021, 13, 856–866. [Google Scholar] [CrossRef]
- Trivedi, P.D.; Mohapatra, A.; Morris, M.K.; Thorne, S.A.; Smith, S.C.; Ward, A.M.; Schroy, P.; Hampel, H.; Jandorf, L.; Popp, J.W., Jr.; et al. Prevalence and Predictors of Young-Onset Colorectal Neoplasia: Insights from a Nationally Representative Colonoscopy Registry. Gastroenterology 2022, 162, 1136–1146 e1135. [Google Scholar] [CrossRef]
- Guo, X.; Liu, Y.; Liu, L.J.; Li, J.; Zhao, L.; Jin, X.R.; Yan, W.; Lin, B.Q.; Shi, S.; Li, Z.Y.; et al. Development and validation of survival nomograms in colorectal cancer patients with synchronous liver metastases underwent simultaneous surgical treatment of primary and metastatic lesions. Am. J. Cancer Res. 2021, 11, 2654–2669. [Google Scholar]
- Kasi, P.M.; Shahjehan, F.; Cochuyt, J.J.; Li, Z.; Colibaseanu, D.T.; Merchea, A. Rising Proportion of Young Individuals with Rectal and Colon Cancer. Clin. Colorectal Cancer 2019, 18, e87–e95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rees, M.; Tekkis, P.P.; Welsh, F.K.; O’Rourke, T.; John, T.G. Evaluation of long-term survival after hepatic resection for metastatic colorectal cancer: A multifactorial model of 929 patients. Ann. Surg. 2008, 247, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Ueno, H.; Mochizuki, H.; Hashiguchi, Y.; Hatsuse, K.; Fujimoto, H.; Hase, K. Predictors of extrahepatic recurrence after resection of colorectal liver metastases. Br. J. Surg. 2004, 91, 327–333. [Google Scholar] [CrossRef]
- Cao, Y.; Ke, S.; Deng, S.; Yan, L.; Gu, J.; Mao, F.; Xue, Y.; Zheng, C.; Cai, W.; Liu, H.; et al. Development and Validation of a Predictive Scoring System for Colorectal Cancer Patients with Liver Metastasis: A Population-Based Study. Front. Oncol. 2021, 11, 719638. [Google Scholar] [CrossRef]
- Mauri, G.; Sartore-Bianchi, A.; Russo, A.G.; Marsoni, S.; Bardelli, A.; Siena, S. Early-onset colorectal cancer in young individuals. Mol. Oncol. 2019, 13, 109–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Creasy, J.M.; Sadot, E.; Koerkamp, B.G.; Chou, J.F.; Gonen, M.; Kemeny, N.E.; Saltz, L.B.; Balachandran, V.P.; Peter Kingham, T.; DeMatteo, R.P.; et al. The Impact of Primary Tumor Location on Long-Term Survival in Patients Undergoing Hepatic Resection for Metastatic Colon Cancer. Ann. Surg. Oncol. 2018, 25, 431–438. [Google Scholar] [CrossRef] [PubMed]
- De Renzi, G.; Gaballo, G.; Gazzaniga, P.; Nicolazzo, C. Molecular Biomarkers according to Primary Tumor Location in Colorectal Cancer: Current Standard and New Insights. Oncology 2021, 99, 135–143. [Google Scholar] [CrossRef]
- Benedix, F.; Schmidt, U.; Mroczkowski, P.; Gastinger, I.; Lippert, H.; Kube, R.; Study Group Colon/Rectum C. Colon carcinoma-classification into right and left sided cancer or according to colonic subsite?—Analysis of 29,568 patients. Eur. J. Surg. Oncol. 2011, 37, 134–139. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.; Wang, H.W.; Wang, K.; Xing, B.C. The primary tumor location impacts survival outcome of colorectal liver metastases after hepatic resection: A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2019, 45, 1349–1356. [Google Scholar] [CrossRef]
- Buisman, F.E.; Giardiello, D.; Kemeny, N.E.; Steyerberg, E.W.; Höppener, D.J.; Galjart, B.; Nierop, P.M.H.; Balachandran, V.P.; Cercek, A.; Drebin, J.A.; et al. Predicting 10-year survival after resection of colorectal liver metastases; an international study including biomarkers and perioperative treatment. Eur. J. Cancer 2022, 168, 25–33. [Google Scholar] [CrossRef]
- Snyder, R.A.; Hu, C.Y.; Cuddy, A.; Francescatti, A.B.; Schumacher, J.R.; Van Loon, K.; You, Y.N.; Kozower, B.D.; Greenberg, C.C.; Schrag, D.; et al. Association Between Intensity of Posttreatment Surveillance Testing and Detection of Recurrence in Patients with Colorectal Cancer. JAMA 2018, 319, 2104–2115. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Fu, J.; Chen, Y.; Wang, L.; Zheng, S. Early T Stage Is Associated with Poor Prognosis in Patients with Metastatic Liver Colorectal Cancer. Front. Oncol. 2020, 10, 716. [Google Scholar] [CrossRef] [PubMed]
- Ecker, B.L.; Shin, P.; Saadat, L.V.; Court, C.M.; Balachandran, V.P.; Chandwani, R.; Drebin, J.A.; Jarnagin, W.R.; Kingham, T.P.; Soares, K.C.; et al. Genomic Stratification of Resectable Colorectal Liver Metastasis Patients and Implications for Adjuvant Therapy and Survival. Ann. Surg. 2022, 275, 371–381. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; Van Krieken, J.H.; Aderka, D.; Aranda Aguilar, E.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef] [PubMed]
- Di Nicolantonio, F.; Vitiello, P.P.; Marsoni, S.; Siena, S.; Tabernero, J.; Trusolino, L.; Bernards, R.; Bardelli, A. Precision oncology in metastatic colorectal cancer—from biology to medicine. Nat. Rev. Clin. Oncol. 2021, 18, 506–525. [Google Scholar] [CrossRef]
- Balachandran, V.P.; Arora, A.; Gonen, M.; Ito, H.; Turcotte, S.; Shia, J.; Viale, A.; Snoeren, N.; van Hooff, S.R.; Rinkes, I.H.; et al. A Validated Prognostic Multigene Expression Assay for Overall Survival in Resected Colorectal Cancer Liver Metastases. Clin. Cancer Res. 2016, 22, 2575–2582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruo, L.; Gougoutas, C.; Paty, P.B.; Guillem, J.G.; Cohen, A.M.; Wong, W.D. Elective bowel resection for incurable stage IV colorectal cancer: Prognostic variables for asymptomatic patients. J. Am. Coll. Surg. 2003, 196, 722–728. [Google Scholar] [CrossRef]
- Cummins, E.R.; Vick, K.D.; Poole, G.V. Incurable colorectal carcinoma: The role of surgical palliation. Am. Surg. 2004, 70, 433–437. [Google Scholar]
- Poultsides, G.A.; Servais, E.L.; Saltz, L.B.; Patil, S.; Kemeny, N.E.; Guillem, J.G.; Weiser, M.; Temple, L.K.; Wong, W.D.; Paty, P.B. Outcome of primary tumor in patients with synchronous stage IV colorectal cancer receiving combination chemotherapy without surgery as initial treatment. J. Clin. Oncol. 2009, 27, 3379–3384. [Google Scholar] [CrossRef] [Green Version]
- Kawamura, H.; Ogawa, Y.; Yamazaki, H.; Honda, M.; Kono, K.; Konno, S.; Fukuhara, S.; Yamamoto, Y. Impact of Primary Tumor Resection on Mortality in Patients with Stage IV Colorectal Cancer with Unresectable Metastases: A Multicenter Retrospective Cohort Study. World J. Surg. 2021, 45, 3230–3239. [Google Scholar] [CrossRef]
- Karoui, M.; Roudot-Thoraval, F.; Mesli, F.; Mitry, E.; Aparicio, T.; Des Guetz, G.; Louvet, C.; Landi, B.; Tiret, E.; Sobhani, I. Primary colectomy in patients with stage IV colon cancer and unresectable distant metastases improves overall survival: Results of a multicentric study. Dis. Colon Rectum 2011, 54, 930–938. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients (n = 1874) | Training Cohort (n = 1314) | Validation Cohort (n = 560) | p Value | |||
|---|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | ||
| Race | 0.678 | ||||||
| Black | 290 | 15.5 | 204 | 15.5 | 86 | 15.4 | |
| White | 1372 | 73.2 | 956 | 72.8 | 416 | 74.3 | |
| Other | 212 | 11.3 | 154 | 11.7 | 58 | 11.3 | |
| Sex | 0.269 | ||||||
| Female | 853 | 45.5 | 609 | 46.3 | 244 | 43.6 | |
| Male | 1021 | 54.5 | 705 | 53.7 | 316 | 56.4 | |
| Primary site | 0.369 | ||||||
| RCC | 537 | 28.7 | 384 | 29.2 | 153 | 28.7 | |
| LCC | 708 | 37.8 | 502 | 38.2 | 206 | 37.7 | |
| RC | 629 | 33.5 | 428 | 32.6 | 201 | 33.6 | |
| Histology | 0.513 | ||||||
| Adenocarcinoma (Ad) | 1744 | 93.1 | 1218 | 92.7 | 526 | 93.9 | |
| Mucinous adenocarcinoma (Mu) | 90 | 4.8 | 68 | 5.2 | 22 | 3.9 | |
| Other | 40 | 2.1 | 28 | 2.1 | 12 | 2.1 | |
| Grade | 0.975 | ||||||
| Well + moderately (w + m) | 1418 | 75.7 | 994 | 75.6 | 424 | 75.7 | |
| Poorly + undifferentiated (p + u) | 456 | 24.3 | 320 | 24.4 | 136 | 24.3 | |
| Stage_T | 0.137 | ||||||
| T0-1 | 182 | 9.7 | 131 | 10.0 | 51 | 9.1 | |
| T2 | 63 | 3.4 | 36 | 2.7 | 27 | 4.8 | |
| T3 | 1020 | 54.4 | 721 | 54.9 | 299 | 53.4 | |
| T4 | 609 | 32.5 | 426 | 32.4 | 183 | 32.7 | |
| Stage_N | 0.690 | ||||||
| N0 | 393 | 21.0 | 274 | 20.9 | 119 | 21.3 | |
| N1 | 767 | 40.9 | 546 | 41.6 | 221 | 39.5 | |
| N2 | 714 | 38.1 | 494 | 37.6 | 220 | 39.3 | |
| Stage_M | 0.170 | ||||||
| M1a | 1142 | 60.9 | 814 | 61.9 | 328 | 58.6 | |
| M1b | 732 | 39.1 | 500 | 38.1 | 232 | 41.4 | |
| Surgery (PTMR) | |||||||
| Neither (none) | 424 | 22.6 | 286 | 21.8 | 138 | 24.6 | 0.201 |
| Primary+ metastatic (yes) | 483 | 25.8 | 345 | 26.3 | 138 | 24.6 | |
| Only primary (p) | 936 | 49.9 | 657 | 50.0 | 279 | 49.8 | |
| Only metastatic (m) | 31 | 1.7 | 26 | 2.0 | 5 | 0.9 | |
| Extrahepatic metastasis (met) | 0.290 | ||||||
| No | 1520 | 81.1 | 1074 | 81.7 | 446 | 79.6 | |
| Yes | 354 | 18.9 | 240 | 18.3 | 114 | 20.4 | |
| CEA | 0.175 | ||||||
| Positive | 1507 | 80.4 | 1046 | 79.6 | 461 | 82.3 | |
| Negative | 367 | 19.6 | 268 | 20.4 | 99 | 17.7 | |
| Variable | Multivariate Analysis | ||
|---|---|---|---|
| HR | 95% CI | p Value | |
| Race | |||
| Black | Reference | ||
| White | 0.859 | 0.703–1.049 | 0.135 |
| Other | 0.985 | 0.746–1.300 | 0.914 |
| Sex | |||
| Female | Reference | ||
| Male | 1.065 | 0.917–1.238 | 0.407 |
| Primary site | |||
| RCC | Reference | ||
| LCC | 0.574 | 0.476–0.691 | <0.0001 |
| RC | 0.614 | 0.504–0.748 | <0.0001 |
| Histology | |||
| Adenocarcinoma (Ad) | Reference | ||
| Mucinous adenocarcinoma (Mu) | 0.938 | 0.672–1.309 | 0.704 |
| Other | 1.578 | 1.008–2.471 | 0.046 |
| Grade | |||
| Well + moderately (w + m) | Reference | ||
| Poorly + undifferentiated (p + u) | 1.938 | 1.637–2.294 | <0.0001 |
| Stage_T | |||
| T0-1 | Reference | ||
| T2 | 0.793 | 0.452–1.392 | 0.419 |
| T3 | 0.781 | 0.596–1.023 | 0.073 |
| T4 | 1.042 | 0.794–1.368 | 0.766 |
| Stage_N | |||
| N0 | Reference | ||
| N1 | 1.019 | 0.829–1.254 | 0.856 |
| N2 | 1.405 | 1.120–1.763 | 0.003 |
| Stage_M | |||
| M1a | Reference | ||
| M1b | 1.624 | 1.352–1.952 | <0.0001 |
| Surgery (PTMR) | |||
| Neither (none) | Reference | ||
| Primary+ metastatic (yes) | 0.378 | 0.291–0.490 | <0.0001 |
| Only primary | 0.567 | 0.452–0.712 | <0.0001 |
| Only metastatic | 0.642 | 0.363–1.133 | 0.126 |
| Extrahepatic metastasis (met) | |||
| No | Reference | ||
| Yes | 1.222 | 0.982–1.521 | 0.072 |
| CEA | |||
| Positive | Reference | ||
| Negative | 0.773 | 0.633–0.943 | 0.011 |
| Survival | Training Cohort | Validation Cohort | ||||
|---|---|---|---|---|---|---|
| C-Index | 95% CI | C-Index | 95% CI | |||
| Nomogram | 0.709 | 0.689 | 0.729 | 0.735 | 0.708 | 0.762 |
| TNM stage | 0.635 | 0.613 | 0.657 | 0.663 | 0.629 | 0.696 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, X.; Li, Y.; Chen, D.; Xu, X.; Liu, F.; Zhao, F. Nomogram Predicting the Survival of Young-Onset Patients with Colorectal Cancer Liver Metastases. Diagnostics 2022, 12, 1395. https://doi.org/10.3390/diagnostics12061395
Cheng X, Li Y, Chen D, Xu X, Liu F, Zhao F. Nomogram Predicting the Survival of Young-Onset Patients with Colorectal Cancer Liver Metastases. Diagnostics. 2022; 12(6):1395. https://doi.org/10.3390/diagnostics12061395
Chicago/Turabian StyleCheng, Xiaofei, Yanqing Li, Dong Chen, Xiangming Xu, Fanlong Liu, and Feng Zhao. 2022. "Nomogram Predicting the Survival of Young-Onset Patients with Colorectal Cancer Liver Metastases" Diagnostics 12, no. 6: 1395. https://doi.org/10.3390/diagnostics12061395
APA StyleCheng, X., Li, Y., Chen, D., Xu, X., Liu, F., & Zhao, F. (2022). Nomogram Predicting the Survival of Young-Onset Patients with Colorectal Cancer Liver Metastases. Diagnostics, 12(6), 1395. https://doi.org/10.3390/diagnostics12061395