
Evaluation of Heterogeneous Nuclear Ribonucleoprotein D Expression as a Diagnostic Marker for Oral Squamous Cell Carcinoma

 , ,
, ,
Abstract
1. Introduction
2. Material and Methods
2.1. Tissue Specimens
2.2. Immunohistochemical Staining
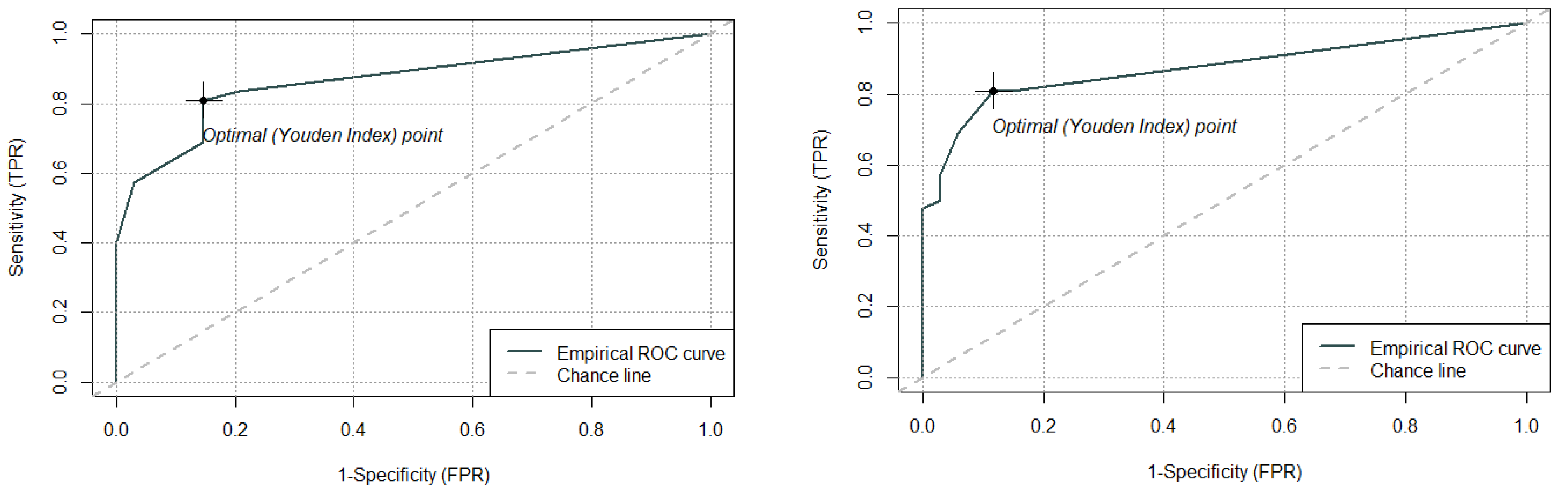
2.3. Statistical Analysis
3. Results
3.1. Clinicopathological Features
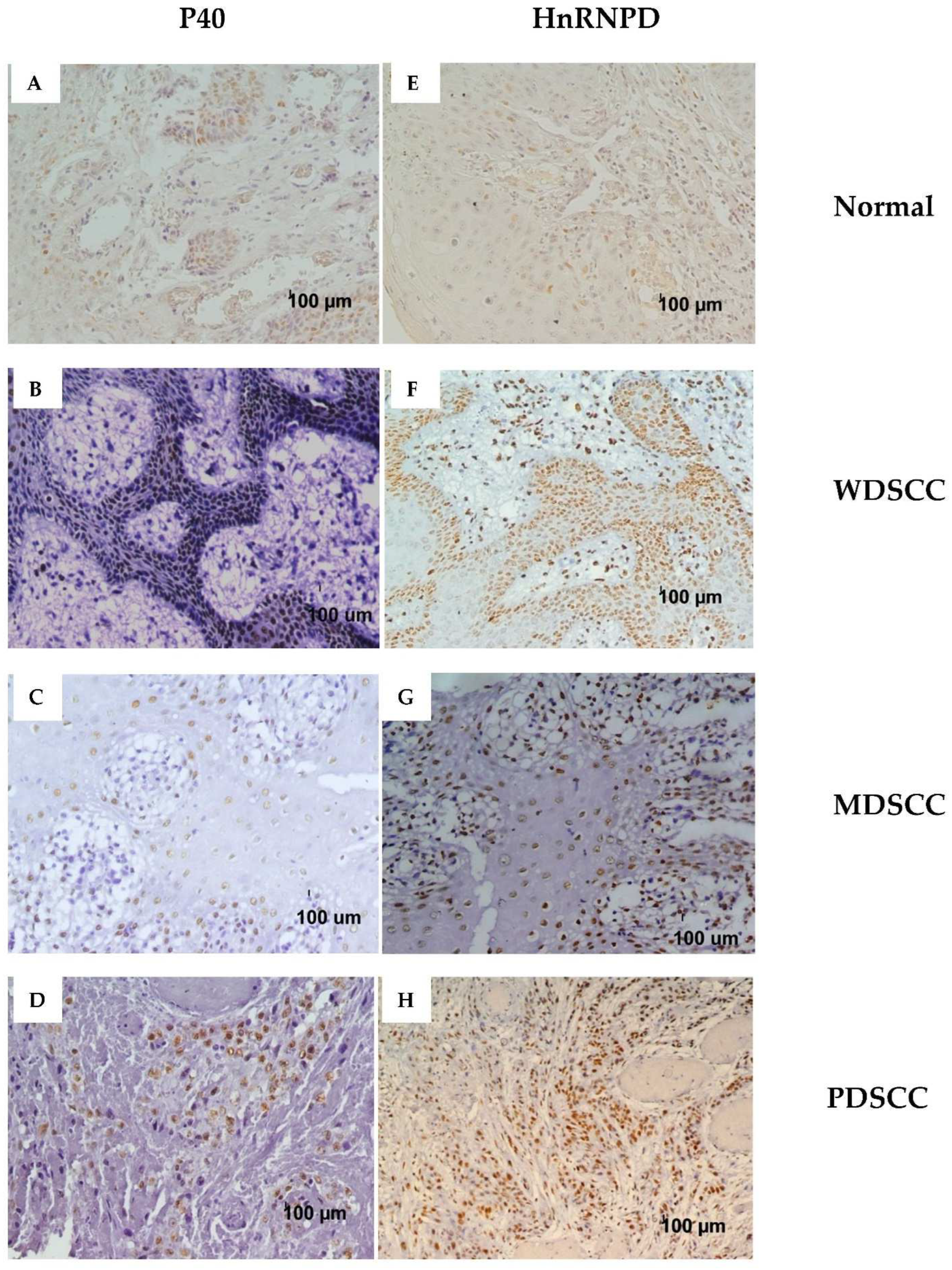
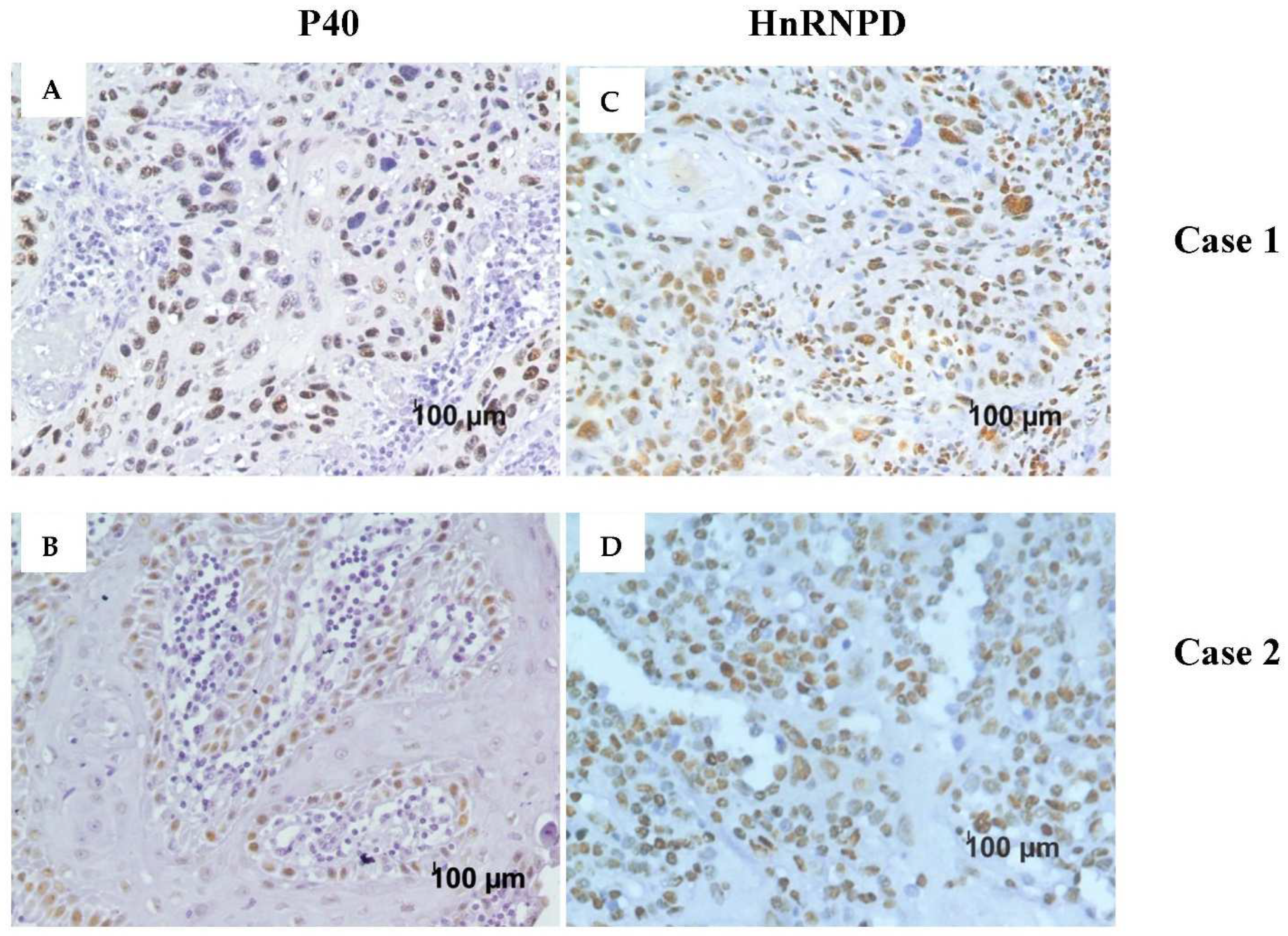
3.2. Immunohistochemical Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Rivera, C. Essentials of Oral Cancer. Int. J. Clin. Exp. Pathol. 2015, 8, 11884–11894. [Google Scholar] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, D.; Natarajan, C.; Mukherjee, A. Advances in Oral Cancer Detection. Adv. Clin. Chem. 2019, 91, 181–200. [Google Scholar] [CrossRef] [PubMed]
- Fedele, S. Diagnostic Aids in the Screening of Oral Cancer. Head Neck Oncol. 2009, 1, 5. [Google Scholar] [CrossRef]
- Abdulmajeed, A.A.; Farah, C.S. Can Immunohistochemistry Serve as an Alternative to Subjective Histopathological Diagnosis of Oral Epithelial Dysplasia? Biomark Cancer 2013, 5, 49–60. [Google Scholar] [CrossRef]
- Fanaras, N.; Warnakulasuriya, S. Oral Cancer Diagnosis in Primary Care. Prim. Dent. J. 2016, 5, 64–68. [Google Scholar] [CrossRef]
- Economopoulou, P.; de Bree, R.; Kotsantis, I.; Psyrri, A. Diagnostic Tumor Markers in Head and Neck Squamous Cell Carcinoma (HNSCC) in the Clinical Setting. Front. Oncol. 2019, 9, 827. [Google Scholar] [CrossRef]
- Lewis, J.S.; Chernock, R.D.; Bishop, J.A. Squamous and Neuroendocrine Specific Immunohistochemical Markers in Head and Neck Squamous Cell Carcinoma: A Tissue Microarray Study. Head Neck Pathol. 2017, 12, 62–70. [Google Scholar] [CrossRef]
- Bishop, J.A.; Montgomery, E.A.; Westra, W.H. Use of P40 and P63 Immunohistochemistry and Human Papillomavirus Testing as Ancillary Tools for the Recognition of Head and Neck Sarcomatoid Carcinoma and Its Distinction From Benign and Malignant Mesenchymal Processes. Am. J. Surg. Pathol. 2014, 38, 257–264. [Google Scholar] [CrossRef]
- Moses, M.A.; George, A.L.; Sakakibara, N.; Mahmood, K.; Ponnamperuma, R.M.; King, K.E.; Weinberg, W.C. Molecular Mechanisms of P63-Mediated Squamous Cancer Pathogenesis. Int. J. Mol. Sci. 2019, 20, 3590. [Google Scholar] [CrossRef]
- Saintigny, P.; El-Naggar, A.K.; Papadimitrakopoulou, V.; Ren, H.; Fan, Y.-H.; Feng, L.; Lee, J.J.; Kim, E.S.; Hong, W.K.; Lippman, S.M.; et al. DeltaNp63 Overexpression, Alone and in Combination with Other Biomarkers, Predicts the Development of Oral Cancer in Patients with Leukoplakia. Clin. Cancer Res. 2009, 15, 6284–6291. [Google Scholar] [CrossRef] [PubMed]
- Tacha, D.; Bremer, R.; Haas, T.; Qi, W. An Immunohistochemical Analysis of a Newly Developed, Mouse Monoclonal P40 (BC28) Antibody in Lung, Bladder, Skin, Breast, Prostate, and Head and Neck Cancers. Arch. Pathol. Lab. Med. 2014, 138, 1358–1364. [Google Scholar] [CrossRef] [PubMed]
- Revel, M.; Groner, Y. Post-Transcriptional and Translational Controls of Gene Expression in Eukaryotes. Annu. Rev. Biochem. 1978, 47, 1079–1126. [Google Scholar] [CrossRef] [PubMed]
- Bakheet, T.; Hitti, E.; Khabar, K.S.A. ARED-Plus: An Updated and Expanded Database of AU-Rich Element-Containing MRNAs and Pre-MRNAs. Nucleic Acids Res. 2018, 46, D218–D220. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Wagner, B.J.; Ehrenman, K.; Schaefer, A.W.; DeMaria, C.T.; Crater, D.; DeHaven, K.; Long, L.; Brewer, G. Purification, Characterization, and CDNA Cloning of an AU-Rich Element RNA-Binding Protein, AUF1. Mol. Cell. Biol. 1993, 13, 7652–7665. [Google Scholar] [CrossRef]
- Wagner, B.J.; Long, L.; Rao, P.N.; Pettenati, M.J.; Brewer, G. Localization and Physical Mapping of Genes Encoding the A+U-Rich Element RNA-Binding Protein AUF1 to Human Chromosomes 4 and X. Genomics 1996, 34, 219–222. [Google Scholar] [CrossRef]
- Wagner, B.J.; DeMaria, C.T.; Sun, Y.; Wilson, G.M.; Brewer, G. Structure and Genomic Organization of the Human AUF1 Gene: Alternative Pre-MRNA Splicing Generates Four Protein Isoforms. Genomics 1998, 48, 195–202. [Google Scholar] [CrossRef]
- Gouble, A.; Grazide, S.; Meggetto, F.; Mercier, P.; Delsol, G.; Morello, D. A New Player in Oncogenesis: AUF1/HnRNPD Overexpression Leads to Tumorigenesis in Transgenic Mice. Cancer Res. 2002, 62, 1489–1495. [Google Scholar]
- White, E.J.F.; Brewer, G.; Wilson, G.M. Post-Transcriptional Control of Gene Expression by AUF1: Mechanisms, Physiological Targets, and Regulation. Biochim. Biophys. Acta 2013, 1829, 680–688. [Google Scholar] [CrossRef]
- Moore, A.E.; Chenette, D.M.; Larkin, L.C.; Schneider, R.J. Physiological Networks and Disease Functions of RNA-Binding Protein AUF1. Wiley Interdiscip. Rev. RNA 2014, 5, 549–564. [Google Scholar] [CrossRef]
- Gratacós, F.M.; Brewer, G. The Role of AUF1 in Regulated MRNA Decay. Wiley Interdiscip. Rev. RNA 2010, 1, 457–473. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Matta, A.; Masui, O.; Srivastava, G.; Kaur, J.; Thakar, A.; Shukla, N.K.; RoyChoudhury, A.; Sharma, M.; Walfish, P.G.; et al. Nuclear Heterogeneous Nuclear Ribonucleoprotein D Is Associated with Poor Prognosis and Interactome Analysis Reveals Its Novel Binding Partners in Oral Cancer. J. Transl. Med. 2015, 13, 285. [Google Scholar] [CrossRef] [PubMed]
- Pereira, B.; Billaud, M.; Almeida, R. RNA-Binding Proteins in Cancer: Old Players and New Actors. Trends Cancer 2017, 3, 506–528. [Google Scholar] [CrossRef] [PubMed]
- Tumor Markers in Common Oral and Maxillofacial Lesions | IntechOpen. Available online: https://www.intechopen.com/chapters/48237 (accessed on 11 August 2021).
- Cervino, G.; Fiorillo, L.; Herford, A.S.; Romeo, U.; Bianchi, A.; Crimi, S.; D’Amico, C.; De Stefano, R.; Troiano, G.; Santoro, R.; et al. Molecular Biomarkers Related to Oral Carcinoma: Clinical Trial Outcome Evaluation in a Literature Review. Dis. Markers 2019, 2019, 8040361. [Google Scholar] [CrossRef] [PubMed]
- Ralhan, R.; DeSouza, L.V.; Matta, A.; Chandra Tripathi, S.; Ghanny, S.; Datta Gupta, S.; Bahadur, S.; Siu, K.W.M. Discovery and Verification of Head-and-Neck Cancer Biomarkers by Differential Protein Expression Analysis Using ITRAQ Labeling, Multidimensional Liquid Chromatography, and Tandem Mass Spectrometry. Mol. Cell. Proteom. 2008, 7, 1162–1173. [Google Scholar] [CrossRef] [PubMed]
- Ralhan, R.; Desouza, L.V.; Matta, A.; Tripathi, S.C.; Ghanny, S.; Dattagupta, S.; Thakar, A.; Chauhan, S.S.; Siu, K.W.M. ITRAQ-Multidimensional Liquid Chromatography and Tandem Mass Spectrometry-Based Identification of Potential Biomarkers of Oral Epithelial Dysplasia and Novel Networks between Inflammation and Premalignancy. J. Proteome Res. 2009, 8, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.; Kaghad, M.; Wang, Y.; Gillett, E.; Fleming, M.D.; Dötsch, V.; Andrews, N.C.; Caput, D.; McKeon, F. P63, a P53 Homolog at 3q27–29, Encodes Multiple Products with Transactivating, Death-Inducing, and Dominant-Negative Activities. Mol. Cell 1998, 2, 305–316. [Google Scholar] [CrossRef]
- Crum, C.P.; McKeon, F.D. P63 in Epithelial Survival, Germ Cell Surveillance, and Neoplasia. Annu. Rev. Pathol. 2010, 5, 349–371. [Google Scholar] [CrossRef]
- Saghravanian, N.; Anvari, K.; Ghazi, N.; Memar, B.; Shahsavari, M.; Aghaee, M.A. Expression of P63 and CD44 in Oral Squamous Cell Carcinoma and Correlation with Clinicopathological Parameters. Arch. Oral Biol. 2017, 82, 160–165. [Google Scholar] [CrossRef]
- Lin, N.-C.; Hsu, J.-T.; Tsai, K.-Y. Survival and Clinicopathological Characteristics of Different Histological Grades of Oral Cavity Squamous Cell Carcinoma: A Single-Center Retrospective Study. PLoS ONE 2020, 15, e0238103. [Google Scholar] [CrossRef]
- Ha, J.; Yang, M. The Use of P40 Helps to Differentiate Squamous Cell Carcinoma From Adenocarcinoma. Am. J. Clin. Pathol. 2012, 138, A150. [Google Scholar] [CrossRef][Green Version]
- Sailer, V.; Stephan, C.; Wernert, N.; Perner, S.; Jung, K.; Dietel, M.; Kristiansen, G. Comparison of P40 (ΔNp63) and P63 Expression in Prostate Tissues--Which One Is the Superior Diagnostic Marker for Basal Cells? Histopathology 2013, 63, 50–56. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Normal Mucosa (n = 32) | Oral Squamous Cell Carcinoma (OSCC) (n = 46) | |
|---|---|---|
| Sex | ||
| Male | 26 (81.25) | 38 (83.60) |
| Female | 6 (18.75) | 8 (17.39) |
| Age | 46.31 ± 13.10 | 45 ± 13.18 |
| Histological grade | ||
| Well-differentiated | - | 17 |
| Moderately differentiated | - | 21 |
| Poorly differentiated | - | 8 |
| Patients No. | Age/Gender | Tumor Site | Pathological Stage | Histological Stage | P40 Total Score * | HnRNPD Total Score * |
|---|---|---|---|---|---|---|
| 1 | 75/M | Tongue | T3N0M0 | PDSCC | 4 | 2 |
| 2 | 55/M | Buccal mucosa | T4N1M0 | MDSCC | 0 | 0 |
| 3 | 40/F | Hard palate | T2N2M0 | WDSCC | 3 | 3 |
| 4 | 52/F | Tongue | T2N1M0 | MDSCC | 7 | 7 |
| 5 | 45/M | Tongue | T2N2M0 | MDSCC | 4 | 7 |
| 6 | 15/M | Buccal mucosa | T4N0M0 | WDSCC | 0 | 0 |
| 7 | 75/M | Buccal mucosa | T4N1M0 | WDSCC | 3 | 6 |
| 8 | 49/M | Tongue | T2N1M0 | WDSCC | 6 | 5 |
| 9 | 52/F | Buccal mucosa | T4N1M0 | WDSCC | 6 | 7 |
| 10 | 60/M | Retromolar trigone | T3N1M0 | WDSCC | 0 | 0 |
| 11 | 33/M | Buccal mucosa | T4N1M0 | MDSCC | 3 | 0 |
| 12 | 35/M | Retromolar trigone | T4N1M0 | MDSCC | 0 | 0 |
| 13 | 71/M | Tongue | T2N2M0 | WDSCC | 6 | 3 |
| 14 | 55/M | Tongue | T1N1M0 | MDSCC | 5 | 1 |
| 15 | 29/M | Buccal mucosa | T2N1M0 | MDSCC | 6 | 7 |
| 16 | 38/M | Buccal mucosa | T4N2M0 | PDSCC | 4 | 7 |
| 17 | 35/M | Retromolar trigone | T4N0M0 | MDSCC | 0 | 1 |
| 18 | 57/M | Buccal mucosa | T4N1M0 | MDSCC | 4 | 6 |
| 19 | 38/M | Buccal mucosa | T2N0M0 | MDSCC | 5 | 7 |
| 20 | 35/M | Buccal mucosa | T2N1M0 | MDSCC | 4 | 2 |
| 21 | 55/F | Alveolar | T4N1M0 | MDSCC | 0 | 0 |
| 22 | 45/M | Alveolar | T4N1M0 | WDSCC | 2 | 3 |
| 23 | 39/M | Buccal mucosa | T4N1M0 | WDSCC | 3 | 7 |
| 24 | 55M | Soft palate | T2N2M0 | WDSCC | 2 | 4 |
| 25 | 60/F | Buccal mucosa | T3N1M0 | WDSCC | 6 | 6 |
| 26 | 35/M | Retromolar trigone | T4N1M0 | MDSCC | 5 | 6 |
| 27 | 35/M | Retromolar trigone | T4N0M0 | MDSCC | 3 | 3 |
| 28 | 55/M | Alveolar | T4N2M0 | MDSCC | 6 | 2 |
| 29 | 48/M | Gingivobuccal sulci | T2N0M0 | WDSCC | 3 | 4 |
| 30 | 31/M | Tongue | T3N2M0 | WDSCC | 5 | 7 |
| 31 | 52/M | Tongue | T2N0M0 | MDSCC | 5 | 6 |
| 32 | 36/M | Buccal mucosa | T3N2M0 | MDSCC | 4 | 6 |
| 33 | 33/M | Tongue | T4N2M0 | WDSCC | 2 | 3 |
| 34 | 44/F | Tongue | T2N1M0 | WDSCC | 3 | 2 |
| 35 | 32/M | Alveolar | T4N2M0 | MDSCC | 6 | 6 |
| 36 | 35/M | Tongue | T1N0M0 | PDSCC | 1 | 4 |
| 37 | 31/M | Tongue | T4N0M0 | WDSCC | 6 | 7 |
| 38 | 55/M | Retromolar trigone | T4N1M0 | MDSCC | 3 | 5 |
| 39 | 48/M | Tongue | T4N1M0 | MDSCC | 4 | 6 |
| 40 | 53/M | Buccal mucosa | T3N1M0 | WDSCC | 6 | 6 |
| 41 | 60/F | Buccal mucosa | T3N1M0 | MDSCC | 7 | 6 |
| 42 | 29/F | Buccal mucosa | T3N1M0 | PDSCC | 2 | 4 |
| 43 | 62/M | Alveolar | T4N1M0 | PDSCC | 3 | 4 |
| 44 | 31/M | Buccal mucosa | T4N1M0 | PDSCC | 5 | 7 |
| 45 | 67/M | Buccal mucosa | T2N1M0 | PDSCC | 5 | 7 |
| 46 | 38/M | Buccal mucosa | T4N2M0 | PDSCC | 2 | 3 |
| Normal Mucosa | Oral Squamous Cell Carcinoma (OSCC) | Histological Grade | |||
|---|---|---|---|---|---|
| WDSCC | MDSCC | PDSCC | |||
| p40 | |||||
| Positive | 3 (9.37) | 39 (84.78) | 15 (88.23) | 17 (80.95) | 7 (87.50) |
| Negative | 29 (90.62) | 7 (15.21) | 2 (11.76) | 4 (19.04) | 1 (12.50) |
| hnRNPD | |||||
| Positive | 2 (6.25) | 38 (82.60) | 15 (88.23) | 15 (71.42) | 8 (100) |
| Negative | 30 (93.75) | 8 (17.39) | 2 (11.76) | 6 (28.57) | 0 (0) |
| Immunostained Cells | Intensity Score | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No. | 0 | 1 | 2 | 3 | 0–10% | 10–30% | 30–50% | 50–70% | >70% | |
| p40 | 46 | 7 (15.21) | 8 (17.39) | 19 (41.30) | 12 (26.08) | 8 (17.39) | 12 (26.08) | 9 (19.56) | 14 (30.43) | 3 (6.52) |
| hnRNPD | 46 | 8 (17.39) | 7 (15.21) | 8 (17.39) | 23 (50) | 8 (17.39) | 12 (26.08) | 4 (8.69) | 10 (21.73) | 12 (26.08) |
| Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | |
|---|---|---|---|---|
| p40 | 80.95 | 85.29 | 87.17 | 78.37 |
| hnRNPD | 80.95 | 88.23 | 89.47 | 78.94 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumar, V.; Lone, M.R.; Kumar, A.; Vincent, V.; Thakkar, H.; Mishra, D.; Chauhan, S.S. Evaluation of Heterogeneous Nuclear Ribonucleoprotein D Expression as a Diagnostic Marker for Oral Squamous Cell Carcinoma. Diagnostics 2022, 12, 1332. https://doi.org/10.3390/diagnostics12061332
Kumar V, Lone MR, Kumar A, Vincent V, Thakkar H, Mishra D, Chauhan SS. Evaluation of Heterogeneous Nuclear Ribonucleoprotein D Expression as a Diagnostic Marker for Oral Squamous Cell Carcinoma. Diagnostics. 2022; 12(6):1332. https://doi.org/10.3390/diagnostics12061332
Chicago/Turabian StyleKumar, Vikas, Moien Rasheed Lone, Anurag Kumar, Vinnyfred Vincent, Himani Thakkar, Deepika Mishra, and Shyam S. Chauhan. 2022. "Evaluation of Heterogeneous Nuclear Ribonucleoprotein D Expression as a Diagnostic Marker for Oral Squamous Cell Carcinoma" Diagnostics 12, no. 6: 1332. https://doi.org/10.3390/diagnostics12061332
APA StyleKumar, V., Lone, M. R., Kumar, A., Vincent, V., Thakkar, H., Mishra, D., & Chauhan, S. S. (2022). Evaluation of Heterogeneous Nuclear Ribonucleoprotein D Expression as a Diagnostic Marker for Oral Squamous Cell Carcinoma. Diagnostics, 12(6), 1332. https://doi.org/10.3390/diagnostics12061332