
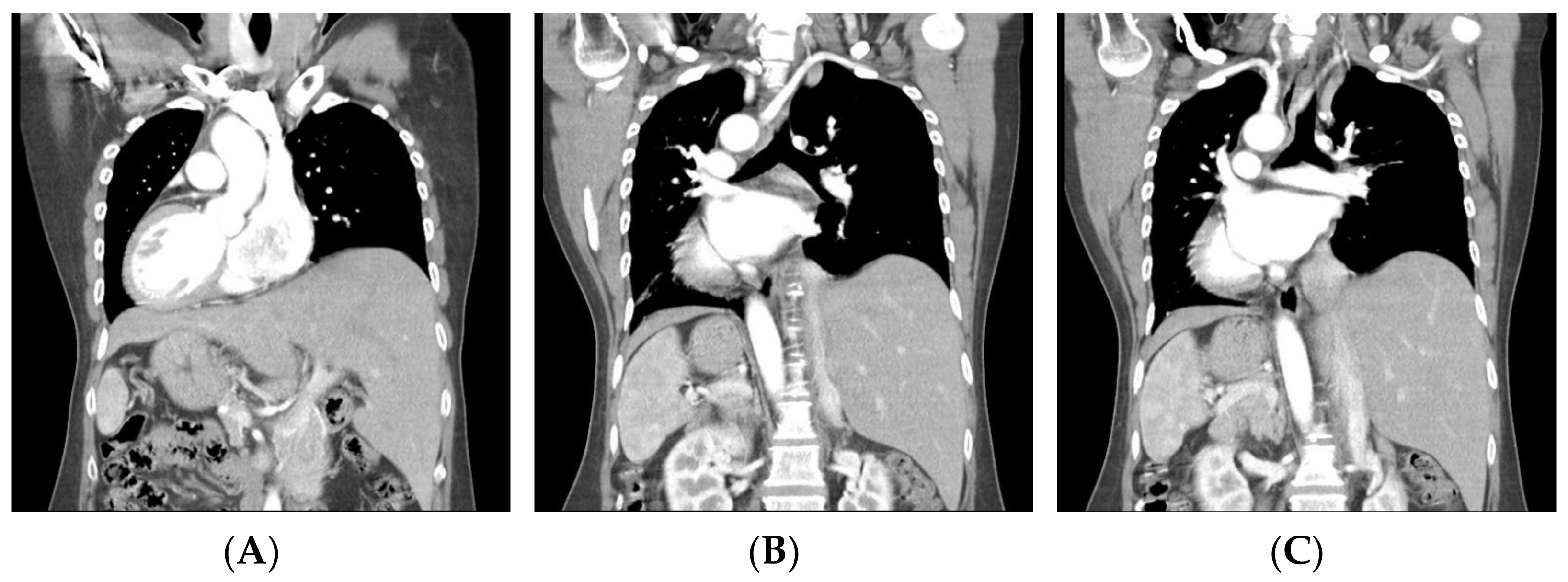
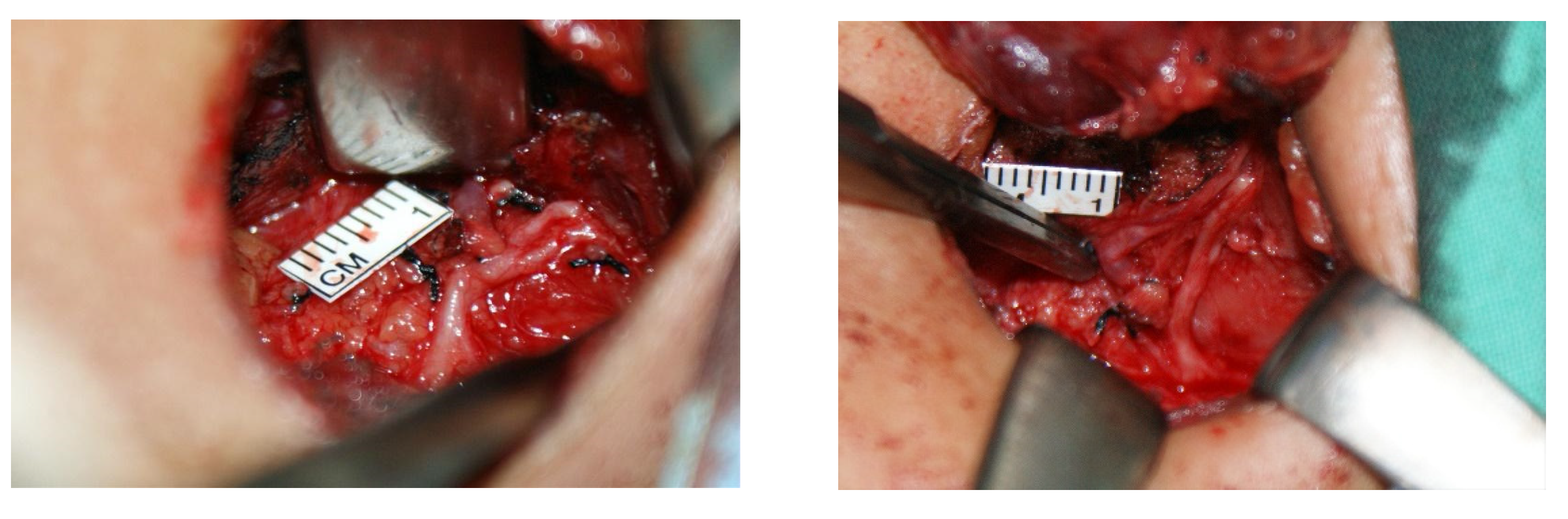
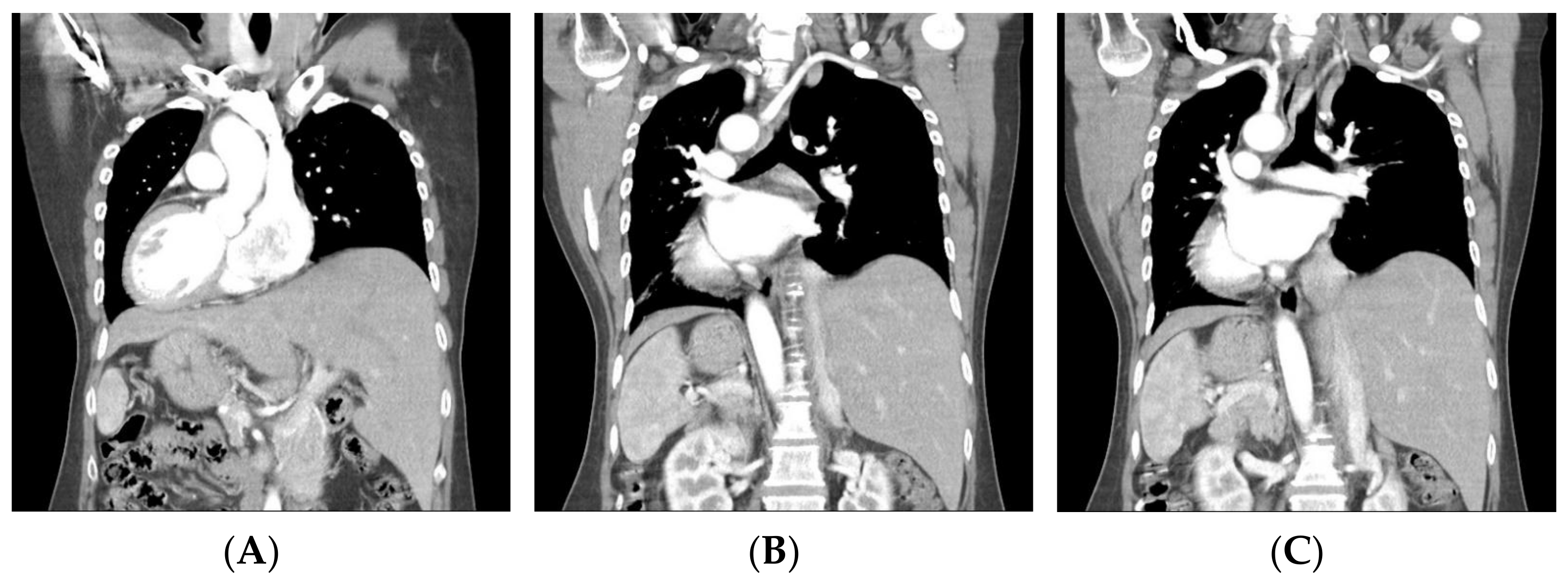
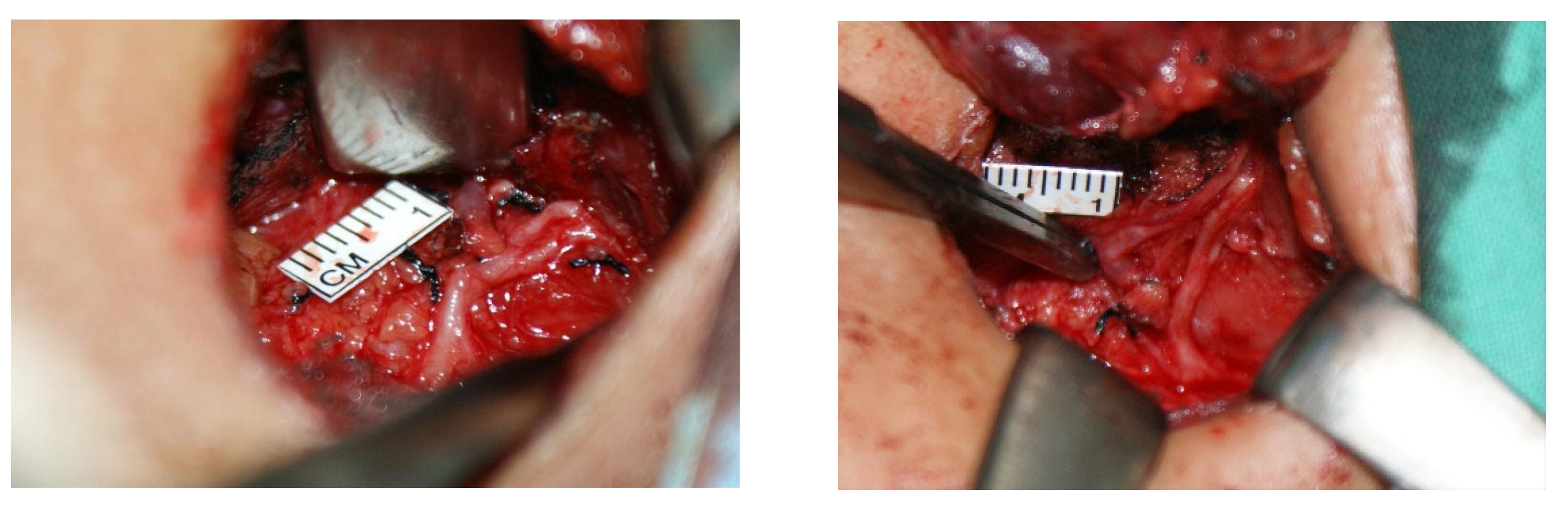
Left Nonrecurrent Laryngeal Nerve with Situs Inversus Totalis


{kind=link}
{kind=link}
Abstract
:
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Zambudio, A.R.; Rodríguez, J.; Riquelme, J.; Soria, T.; Canteras, M.; Parrilla, P. Prospective study of postoperative complications after total thyroidectomy for multinodular goiters by surgeons with experience in endocrine surgery. Ann. Surg. 2004, 240, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Henry, J.F.; Audiffret, J.; Plan, M. The nonrecurrent inferior laryngeal nerve. Apropos of 19 cases including 2 on the left side. J. Chir. 1985, 122, 391–397. (In French) [Google Scholar]
- Iacobone, M.; Viel, G.; Zanella, S.; Bottussi, M.; Frego, M.; Favia, G. The usefulness of preoperative ultrasonographic identification of nonrecurrent inferior laryngeal nerve in neck surgery. Langenbecks Arch. Surg. 2008, 393, 633–638. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-Y.; Liao, C.-Y.; Yao, C.-C. Left Nonrecurrent Laryngeal Nerve with Situs Inversus Totalis. Diagnostics 2022, 12, 730. https://doi.org/10.3390/diagnostics12030730
Chen Y-Y, Liao C-Y, Yao C-C. Left Nonrecurrent Laryngeal Nerve with Situs Inversus Totalis. Diagnostics. 2022; 12(3):730. https://doi.org/10.3390/diagnostics12030730
Chicago/Turabian StyleChen, Yin-Yang, Chi-You Liao, and Chung-Chin Yao. 2022. "Left Nonrecurrent Laryngeal Nerve with Situs Inversus Totalis" Diagnostics 12, no. 3: 730. https://doi.org/10.3390/diagnostics12030730
APA StyleChen, Y.-Y., Liao, C.-Y., & Yao, C.-C. (2022). Left Nonrecurrent Laryngeal Nerve with Situs Inversus Totalis. Diagnostics, 12(3), 730. https://doi.org/10.3390/diagnostics12030730