
First Characterization of ADAMTS-4 in Kidney Tissue and Plasma of Patients with Chronic Kidney Disease—A Potential Novel Diagnostic Indicator

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
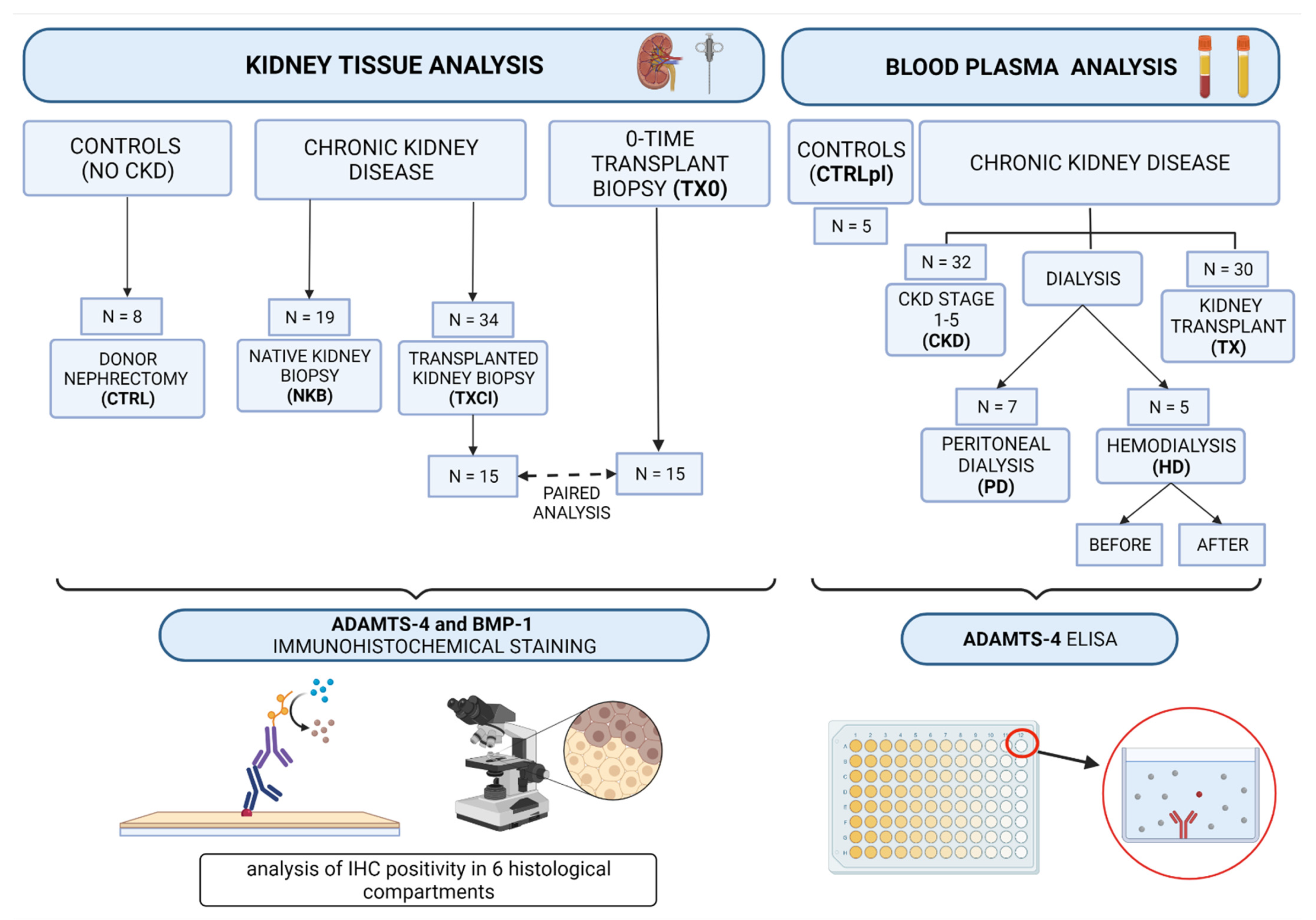
2.1. Sample Collection and Study Outline
2.2. Kidney Biopsy Sample Collection and Analysis
2.3. Immunohistochemistry Analysis (IHC)
2.4. Enzyme-Linked Immunosorbent Assay (ELISA)
2.5. Statistical Analysis
3. Results
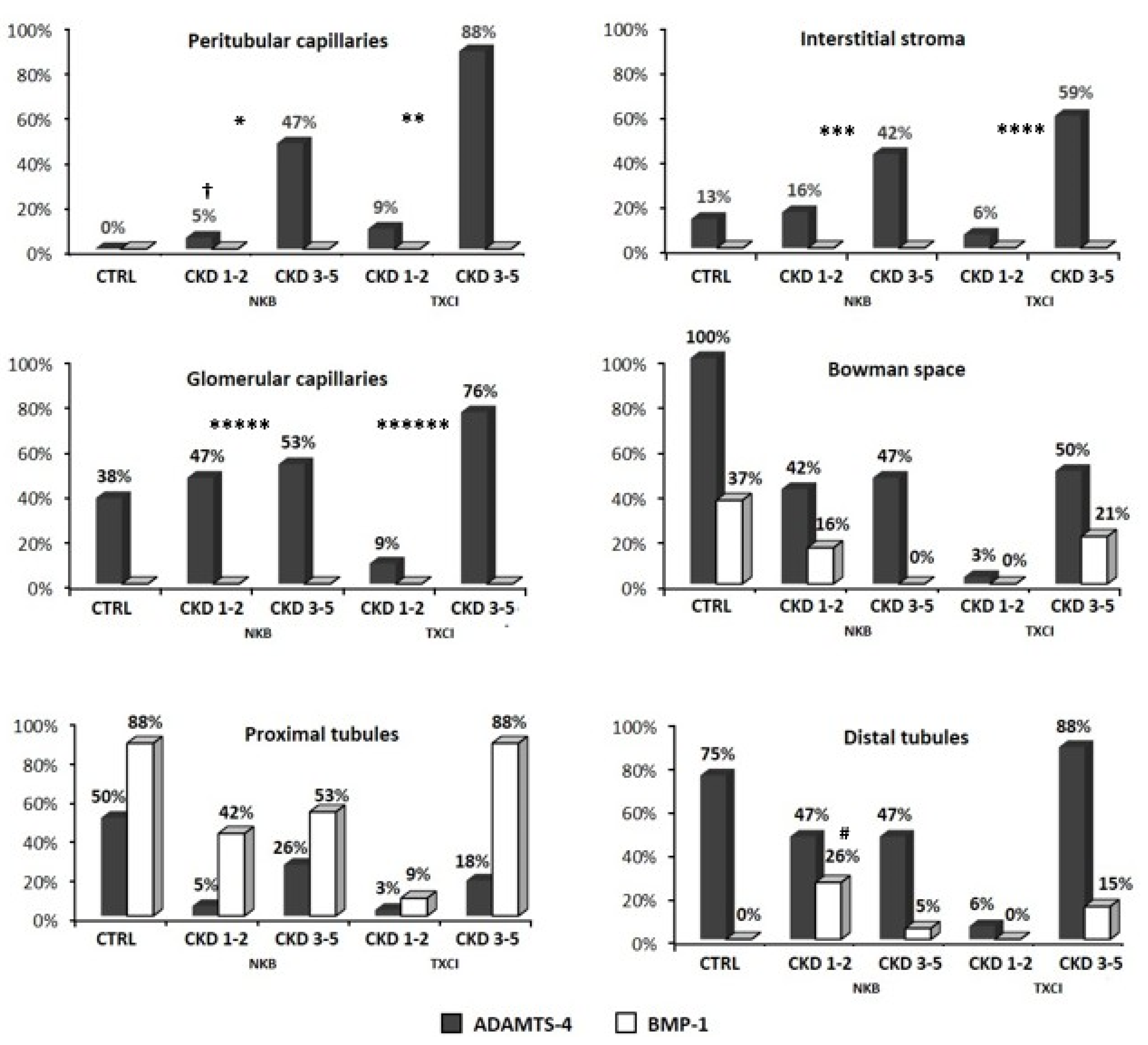
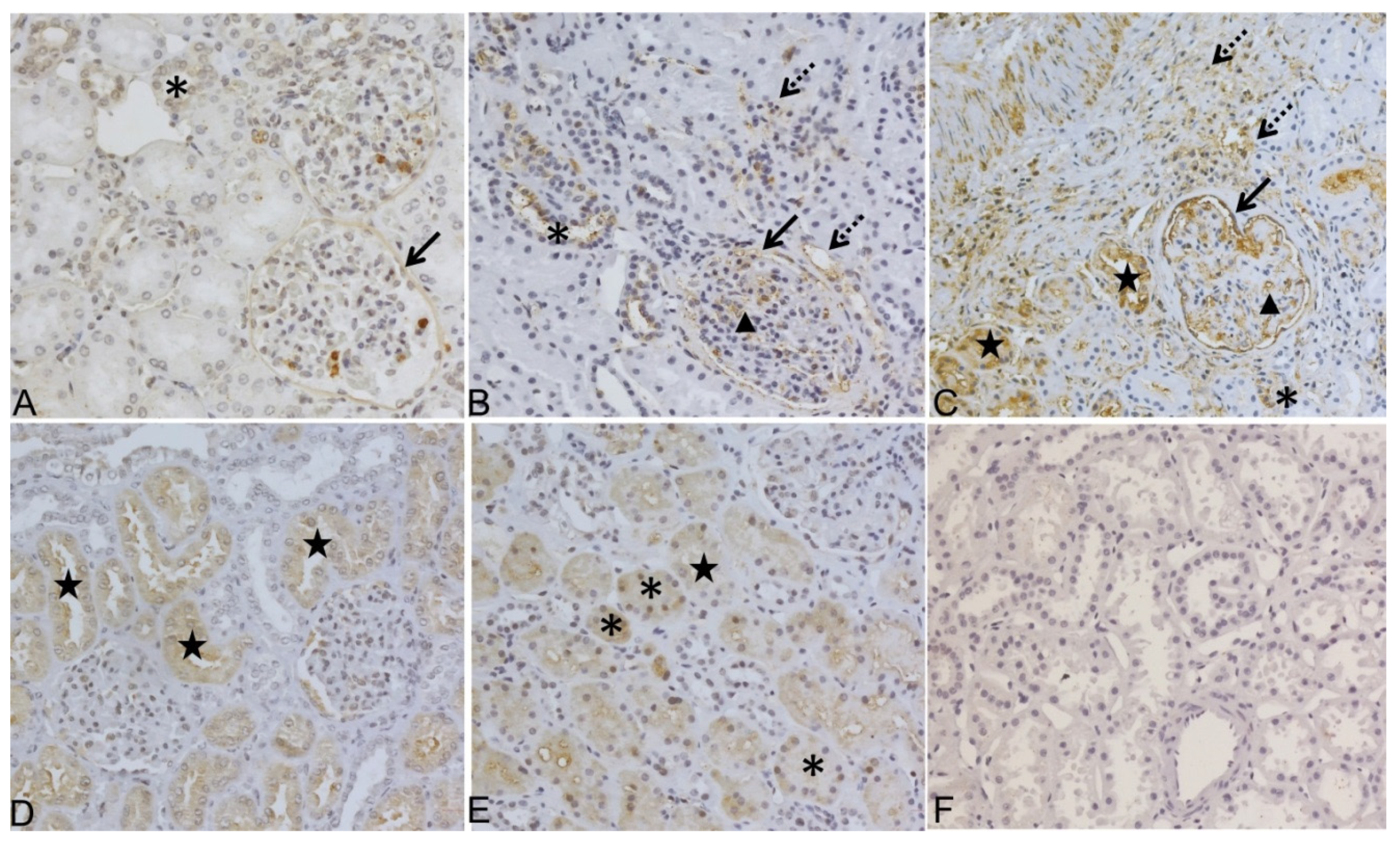
3.1. Immunohistochemistry Analysis of ADAMTS-4 and BMP-1 Molecules in Kidney Biopsy Samples of Patients with CKD
3.2. Distribution of ADAMTS-4 and BMP-1 in Kidney Tissue Samples of CTRL, NKB and TXCI Group
3.2.1. BMP-1 and ADAMTS-4 in Kidney Samples without CKD
3.2.2. BMP-1 and ADAMTS-4 in Kidney Samples with CKD
3.3. Association of ADAMTS-4 Expression in Interstitial Compartment with Chronic Kidney Histology Scores
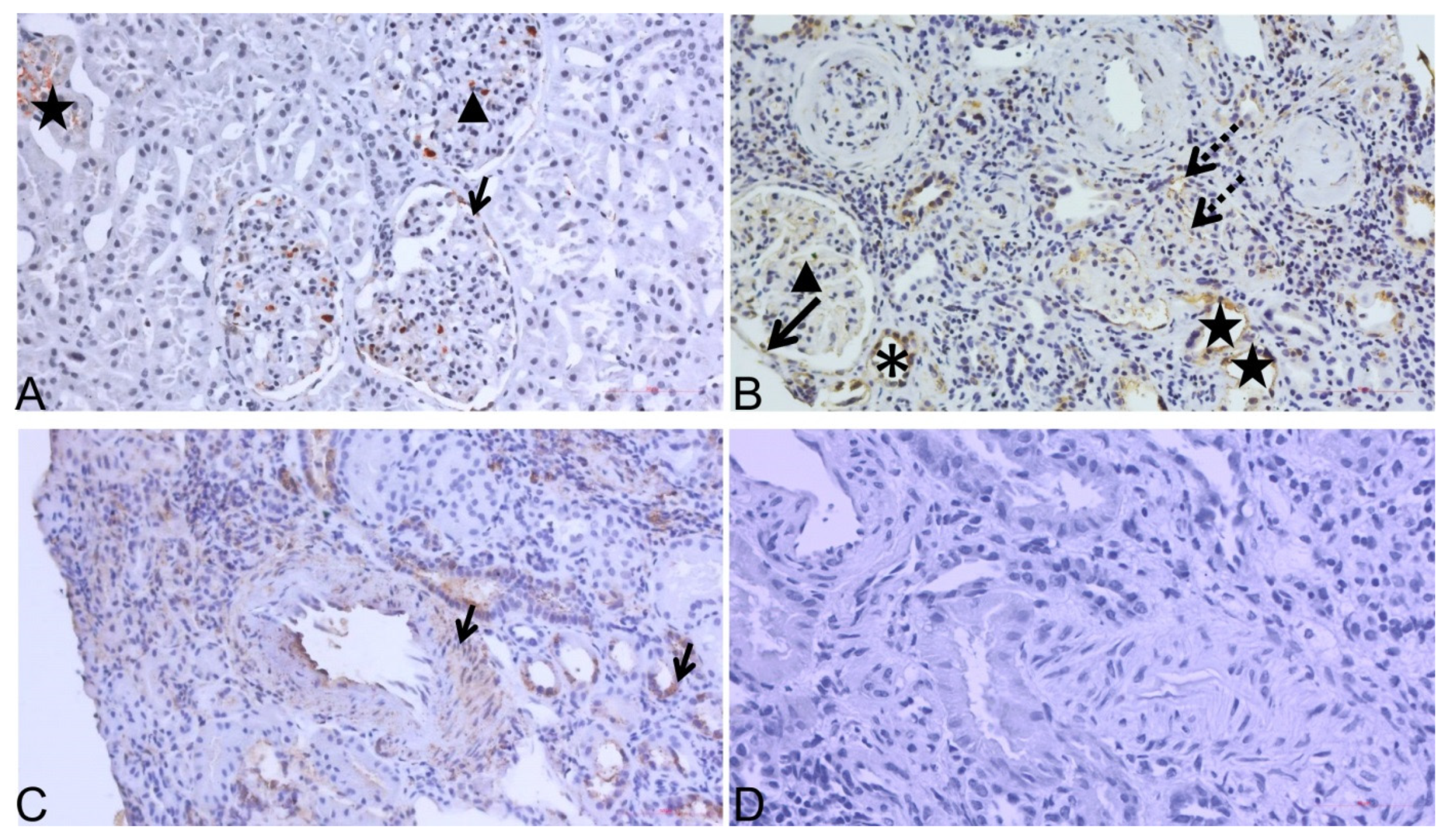
3.4. Analysis of ADAMTS-4 IHC Expression in 15 Transplant Kidney Biopsy Sample Pairs (TX0-TXCI)
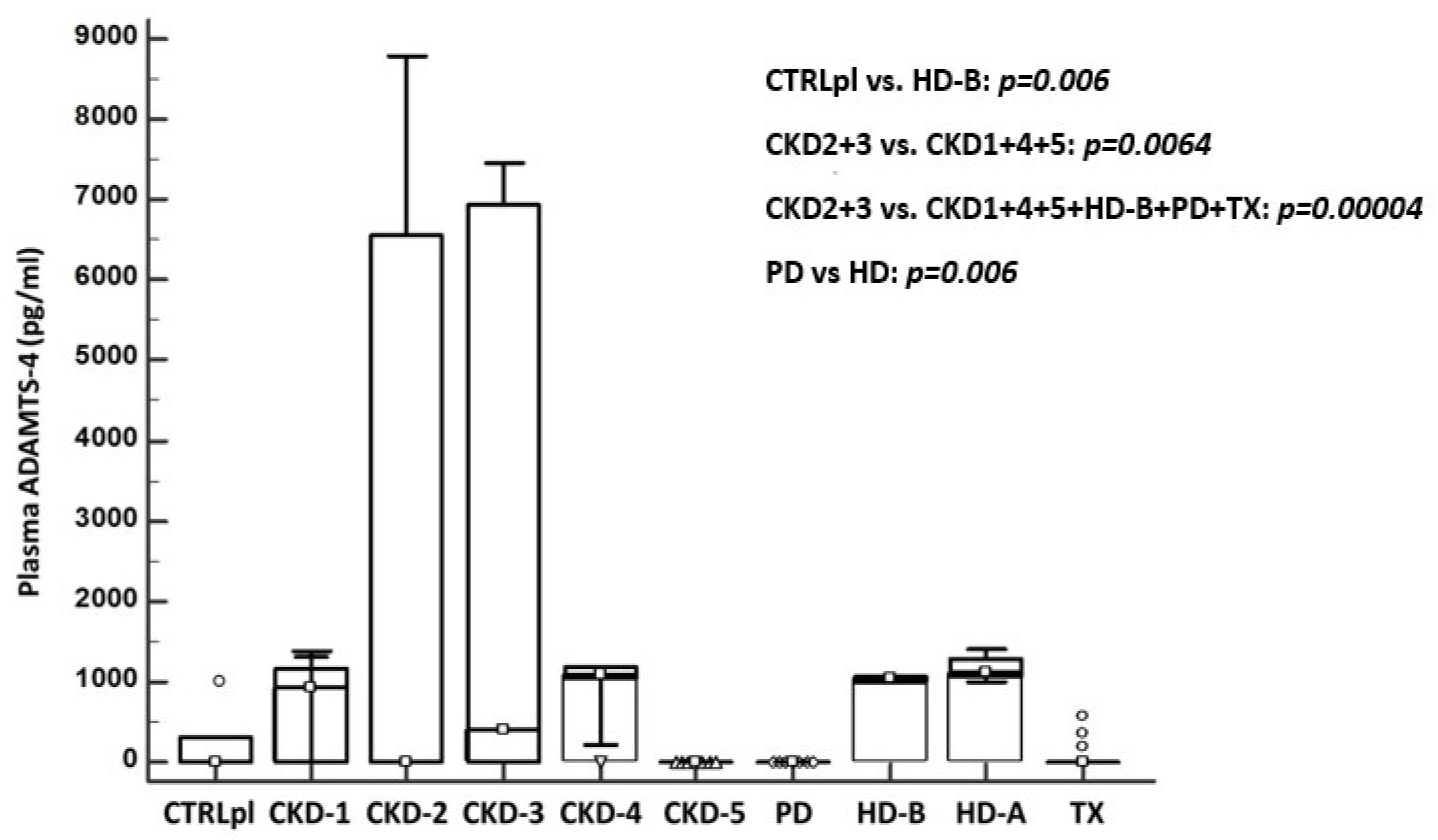
3.5. Detection of ADAMTS-4 in Plasma of Patients with CKD (Elisa Analysis)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef]
- Stenvinkel, P. Chronic kidney disease: A public health priority and harbinger of premature cardiovascular disease. J. Intern. Med. 2010, 268, 456–467. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Astor, B.C.; Stevens, L.A.; Coresh, J. Chronic kidney disease, diabetes, and hypertension: What’s in a name? Kidney Int. 2010, 78, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Gansevoort, R.T.; de Jong, P.E. Challenges for the present CKD classification system. Curr. Opin. Nephrol. Hypertens. 2010, 19, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Tampe, D.; Zeisberg, M. Potential approaches to reverse or repair renal fibrosis. Nat. Rev. Nephrol. 2014, 10, 226–237. [Google Scholar] [CrossRef] [PubMed]
- Weiner, D.E.; Tighiouart, H.; Amin, M.G.; Stark, P.C.; MacLeod, B.; Griffith, J.L.; Salem, D.N.; Levey, A.S.; Sarnak, M.J. Chronic Kidney Disease as a Risk Factor for Cardiovascular Disease and All-Cause Mortality: A Pooled Analysis of Community-Based Studies. J. Am. Soc. Nephrol. 2004, 15, 1307–1315. [Google Scholar] [CrossRef]
- Kalluri, R.; Zeisberg, M. Fibroblasts in cancer. Nat. Rev. Cancer 2006, 6, 392–401. [Google Scholar] [CrossRef]
- Boor, P.; Ostendorf, T.; Floege, J. Renal fibrosis: Novel insights into mechanisms and therapeutic targets. Nat. Rev. Nephrol. 2010, 6, 643–656. [Google Scholar] [CrossRef]
- Strutz, F.; Zeisberg, M. Renal Fibroblasts and Myofibroblasts in Chronic Kidney Disease. J. Am. Soc. Nephrol. 2006, 17, 2992–2998. [Google Scholar] [CrossRef]
- Wolfe, R.A.; Ashby, V.B.; Milford, E.L.; Ojo, A.O.; Ettenger, R.E.; Agodoa, L.Y.C.; Held, P.J.; Port, F.K. Comparison of Mortality in All Patients on Dialysis, Patients on Dialysis Awaiting Transplantation, and Recipients of a First Cadaveric Transplant. N. Engl. J. Med. 1999, 341, 1725–1730. [Google Scholar] [CrossRef]
- Little, M.H.; Bertram, J.F. Is There Such a Thing as a Renal Stem Cell?: Figure 1. J. Am. Soc. Nephrol. 2009, 20, 2112–2117. [Google Scholar] [CrossRef] [PubMed]
- Grgurevic, L.; Macek, B.; Healy, D.R.; Brault, A.L.; Erjavec, I.; Cipcic, A.; Grgurevic, I.; Rogic, D.; Galesic, K.; Brkljacic, J.; et al. Circulating Bone Morphogenetic Protein 1–3 Isoform Increases Renal Fibrosis. J. Am. Soc. Nephrol. 2011, 22, 681–692. [Google Scholar] [CrossRef]
- Grgurevic, L.; Vukicevic, S. ADAMTS4 as a Blood Biomarker and Therapeutic Target for Chronic Renal Failure. U.S. Patent 8,263,072 B2, 11 September 2012. [Google Scholar]
- Rudnicki, M.; Perco, P.; Neuwirt, H.; Noppert, S.-J.; Leierer, J.; Sunzenauer, J.; Eder, S.; Zoja, C.; Eller, K.; Rosenkranz, A.R.; et al. Increased Renal Versican Expression Is Associated with Progression of Chronic Kidney Disease. PLoS ONE 2012, 7, e44891. [Google Scholar] [CrossRef] [PubMed]
- Novak, R.; Hrkac, S.; Salai, G.; Bilandzic, J.; Mitar, L.; Grgurevic, L. The Role of ADAMTS-4 in Atherosclerosis and Vessel Wall Abnormalities. J. Vasc. Res. 2022, 1–9. [Google Scholar] [CrossRef]
- Engel, J.E.; Chade, A.R. Macrophage polarization in chronic kidney disease: A balancing act between renal recovery and decline? Am. J. Physiol. Physiol. 2019, 317, F1409–F1413. [Google Scholar] [CrossRef]
- Wågsäter, D.; Björk, H.; Zhu, C.; Björkegren, J.; Valen, G.; Hamsten, A.; Eriksson, P. ADAMTS-4 and -8 are inflammatory regulated enzymes expressed in macrophage-rich areas of human atherosclerotic plaques. Atherosclerosis 2008, 196, 514–522. [Google Scholar] [CrossRef]
- Walker, P.D. The Renal Biopsy. Arch. Pathol. Lab. Med. 2009, 133, 181–188. [Google Scholar] [CrossRef]
- Roufosse, C.; Simmonds, N.; Groningen, M.C.-V.; Haas, M.; Henriksen, K.J.; Horsfield, C.; Loupy, A.; Mengel, M.; Perkowska-Ptasińska, A.; Rabant, M.; et al. A 2018 Reference Guide to the Banff Classification of Renal Allograft Pathology. Transplantation 2018, 102, 1795–1814. [Google Scholar] [CrossRef]
- Dong, H.; Du, T.; Premaratne, S.; Zhao, C.X.; Tian, Q.; Li, Y.; Yan, S.; Zhang, W.W. Relationship between ADAMTS4 and carotid atherosclerotic plaque vulnerability in humans. J. Vasc. Surg. 2018, 67, 1120–1126. [Google Scholar] [CrossRef]
- Yuan, C.; Liu, Z.; Yu, Q.; Wang, X.; Bian, M.; Yu, Z.; Yu, J. Expression of PD-1/PD-L1 in primary breast tumours and metastatic axillary lymph nodes and its correlation with clinicopathological parameters. Sci. Rep. 2019, 9, 14356. [Google Scholar] [CrossRef]
- Wang, S.; Lu, Y.; Hong, Q.; Geng, X.; Wang, X.; Zheng, W.; Song, C.; Liu, C.; Fan, M.; Xi, Y.; et al. Protein Array-Based Detection of Proteins in Kidney Tissues from Patients with Membranous Nephropathy. BioMed Res. Int. 2017, 2017, 7843584. [Google Scholar] [CrossRef] [PubMed]
- Boerboom, D.; Lafond, J.-F.; Zheng, X.; Lapointe, E.; Mittaz, L.; Boyer, A.; Pritchard, M.A.; DeMayo, F.J.; Mort, J.S.; Drolet, R.; et al. Partially redundant functions of Adamts1 and Adamts4 in the perinatal development of the renal medulla. Dev. Dyn. 2011, 240, 1806–1814. [Google Scholar] [CrossRef] [PubMed]
- Bábíčková, J.; Klinkhammer, B.M.; Buhl, E.M.; Djudjaj, S.; Hoss, M.; Heymann, F.; Tacke, F.; Floege, J.; Becker, J.U.; Boor, P. Regardless of etiology, progressive renal disease causes ultrastructural and functional alterations of peritubular capillaries. Kidney Int. 2017, 91, 70–85. [Google Scholar] [CrossRef] [PubMed]
- Schrimpf, C.; Xin, C.; Campanholle, G.; Gill, S.E.; Stallcup, W.; Lin, S.L.; Duffield, J.S. Pericyte TIMP3 and ADAMTS1 Modulate Vascular Stability after Kidney Injury. J. Am. Soc. Nephrol. 2012, 23, 868–883. [Google Scholar] [CrossRef]
- Grgic, I.; Krautzberger, A.M.; Hofmeister, A.; Lalli, M.; DiRocco, D.P.; Fleig, S.V.; Humphreys, B.D. Translational Profiles of Medullary Myofibroblasts during Kidney Fibrosis. J. Am. Soc. Nephrol. 2014, 25, 1979–1990. [Google Scholar] [CrossRef]
- Armutcu, F.; Demircan, K.; Yildirim, U.; Namuslu, M.; Yagmurca, M.; Celik, H.T. Hypoxia causes important changes of extracellular matrix biomarkers and ADAMTS proteinases in the adriamycin-induced renal fibrosis model. Nephrology 2019, 24, 863–875. [Google Scholar] [CrossRef]
- Boyd, D.F.; Allen, E.K.; Randolph, A.G.; Guo, X.Z.J.; Weng, Y.; Sanders, C.J.; Thomas, P.G. Exuberant fibroblast activity compromises lung function via ADAMTS4. Nature 2020, 587, 466–471. [Google Scholar] [CrossRef]
- Bülow, R.D.; Boor, P. Extracellular Matrix in Kidney Fibrosis: More Than Just a Scaffold. J. Histochem. Cytochem. 2019, 67, 643–661. [Google Scholar] [CrossRef]
- Bode-Lesniewska, B.; Dours-Zimmermann, M.T.; Odermatt, B.F.; Briner, J.; Heitz, P.U.; Zimmermann, D.R. Distribution of the large aggregating proteoglycan versican in adult human tissues. J. Histochem. Cytochem. 1996, 44, 303–312. [Google Scholar] [CrossRef]
- Islam, S.; Watanabe, H. Versican: A Dynamic Regulator of the Extracellular Matrix. J. Histochem. Cytochem. 2020, 68, 763–775. [Google Scholar] [CrossRef]
- Tang, P.M.-K.; Nikolic-Paterson, D.J.; Lan, H.-Y. Macrophages: Versatile players in renal inflammation and fibrosis. Nat. Rev. Nephrol. 2019, 15, 144–158. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.Y.; Jiang, H.; Pan, J.; Huang, X.R.; Wang, Y.C.; Huang, H.F.; Chen, J.H. Macrophage-to-Myofibroblast Transition Contributes to Interstitial Fibrosis in Chronic Renal Allograft Injury. J. Am. Soc. Nephrol. 2017, 28, 2053–2067. [Google Scholar] [CrossRef] [PubMed]
- Sandy, J.D.; Westling, J.; Kenagy, R.D.; Iruela-Arispe, M.L.; Verscharen, C.; Rodriguez-Mazaneque, J.C.; Clowes, A.W. Versican V1 Proteolysis in Human Aorta in Vivo Occurs at the Glu441-Ala442 Bond, a Site That Is Cleaved by Recombinant ADAMTS-1 and ADAMTS-4. J. Biol. Chem. 2001, 276, 13372–13378. [Google Scholar] [CrossRef] [PubMed]
- Koch, C.D.; Lee, C.M.; Apte, S.S. Aggrecan in Cardiovascular Development and Disease. J. Histochem. Cytochem. 2020, 68, 777–795. [Google Scholar] [CrossRef] [PubMed]
- Vadon-Le Goff, S.; Hulmes, D.J.S.; Moali, C. BMP-1/tolloid-like proteinases synchronize matrix assembly with growth factor activation to promote morphogenesis and tissue remodeling. Matrix Biol. 2015, 44–46, 14–23. [Google Scholar] [CrossRef]
- Bai, M.; Lei, J.; Wang, S.; Ding, D.; Yu, X.; Guo, Y.; Zhang, A. BMP1 inhibitor UK383,367 attenuates renal fibrosis and inflammation in CKD. Am. J. Physiol. Physiol. 2019, 317, F1430–F1438. [Google Scholar] [CrossRef]
- Yong, K.; Dogra, G.; Boudville, N.; Lim, W. Increased Inflammatory Response in Association with the Initiation of Hemodialysis Compared with Peritoneal Dialysis in a Prospective Study of End-Stage Kidney Disease Patients. Perit. Dial. Int. 2018, 38, 18–23. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CTRL N = 8 | NKB N = 19 | TXCI N = 34 | TXCI-TX0 PAIRS N = 15 | ||
|---|---|---|---|---|---|
| TXCI (N = 15) | TX0 (N = 15) | ||||
| AGE (YEARS) | 53 ± 13 | 43 ± 17 | 50 ± 16 | 51 ± 44 | 51 ± 7 |
| SEX (% MALE) | 2 (25%) | 7 (37%) | 28 (82%) | 14 (93%) | 6 (40%) |
| BMI | 24.3 ± 4.6 | 26.1 ± 5.7 | 27.1 ± 5.4 | 27.9 ± 18.5 | 25.6 ± 2.2 |
| EGFR (ML/MIN) | 108 ± 28 | 56 ± 36 | 37 ± 16 | 38 ± 64 | 91 ± 22 |
| 24-PROT G/L | - | 3.27 ± 2.74 | 1.53 ± 1.50 | 1.22 ± 5.46 | - |
| CKD | N (%) | N (%) | N (%) | N (%) | N (%) |
| NO CKD | 8 (100) | 0 | 0 | 0 | 14 (93) |
| CKD-1 | 5 (26.3) | 0 | 0 | 1 (6.7) | |
| CKD-2 | 4 (21.1) | 3 (8.8) | 1 (6.7) | 0 | |
| CKD-3 | 2 (10.5) | 20 (58.8) | 9 (60) | 0 | |
| CKD-4 | 6 (31.6) | 10 (29.4) | 5 (33.3) | 0 | |
| CKD-5 | 2 (10.5) | 1 (2.9) | 0 | 0 | |
| COMORBIDITIES | N (%) | N (%) | N (%) | N (%) | N (%) |
| AH | 4 (50) | 12 (63.2) | 31 (91.2) | 13 (86.6) | 6 (40) |
| DM | 0 | 0 | 9 (26.5) | 5 (33.3) | 0 |
| SMOK | 0 | 6 (31.6) | 5 (14.7) | 1 (6.7) | 1 (6.7) |
| HLP | 0 | 9 (47.4) | 13 (38.2) | 5 (33.3) | 0 |
| CAD | 0 | 0 | 4 (11.8) | 1 (6.7) | 0 |
| ATH | 0 | 2 (10.5) | 4 (11.8) | 13 (86.6) | 0 |
| KIDNEY DISEASE | N (%) | N (%) | N (%) | N (%) | N (%) |
| NB | 8 (100) | 0 | 2 (5.8) | 2 (13.3) | 13 (86.6) |
| GN | - | 17 (89.5) | 4 (11.7) | 1 (6.6) | - |
| HTN | - | 1 (5.3) | - | - | - |
| ANCA VS | - | 1 (5.3) | - | - | - |
| TCR | - | - | 2 (5.8) | 1 (6.6) | - |
| ABMR | - | - | 5 (14.7) | 1 (6.6) | - |
| TCR + ABMR | - | - | 4 (11.7) | 1 (6.6) | - |
| BKVAN | - | - | 3 (8.8) | 3 (20) | - |
| NC | - | 0 | 14 (41.1) | 6 (40) | 2 (13.3) |
| ATI | 6 (75) | 5 (26.3) | 8 (23.5) | 3 (20) | 8 (53.3) |
| TX0 (N = 15) | TXCI (N = 15) | p | |
|---|---|---|---|
| eGFR (mean) | 91.47 | 37.93 | <0.00001 |
| CKD STAGE (median) | 0 (0–3) | 3 (2–4) | <0.00001 |
| CI SCORE (mean) | 0.07 | 1.27 | 0.000157 |
| ADAMTS-4 INT (n/N) | 1/15 | 10/15 | 0.00169 |
| ADAMTS-4 PTC (n/N) | 0/15 | 15/15 | <0.0001 |
| ADAMTS-4 PXT (n/N) | 6/15 | 2/15 | NS |
| ADAMTS-4 DT (n/N) | 11/15 | 15/15 | NS |
| ADAMTS-4 GC (n/N) | 5/15 | 13/15 | 0.00778 |
| ADAMTS-4 BW (n/N) | 14/15 | 10/15 | NS |
| TIMEPOINT OF BIOPSY (days) | 0 | 690 (28–2340) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vojtusek, I.K.; Laganovic, M.; Burek Kamenaric, M.; Bulimbasic, S.; Hrkac, S.; Salai, G.; Ivkovic, V.; Coric, M.; Novak, R.; Grgurevic, L. First Characterization of ADAMTS-4 in Kidney Tissue and Plasma of Patients with Chronic Kidney Disease—A Potential Novel Diagnostic Indicator. Diagnostics 2022, 12, 648. https://doi.org/10.3390/diagnostics12030648
Vojtusek IK, Laganovic M, Burek Kamenaric M, Bulimbasic S, Hrkac S, Salai G, Ivkovic V, Coric M, Novak R, Grgurevic L. First Characterization of ADAMTS-4 in Kidney Tissue and Plasma of Patients with Chronic Kidney Disease—A Potential Novel Diagnostic Indicator. Diagnostics. 2022; 12(3):648. https://doi.org/10.3390/diagnostics12030648
Chicago/Turabian StyleVojtusek, Ivana Kovacevic, Mario Laganovic, Marija Burek Kamenaric, Stela Bulimbasic, Stela Hrkac, Grgur Salai, Vanja Ivkovic, Marijana Coric, Rudjer Novak, and Lovorka Grgurevic. 2022. "First Characterization of ADAMTS-4 in Kidney Tissue and Plasma of Patients with Chronic Kidney Disease—A Potential Novel Diagnostic Indicator" Diagnostics 12, no. 3: 648. https://doi.org/10.3390/diagnostics12030648
APA StyleVojtusek, I. K., Laganovic, M., Burek Kamenaric, M., Bulimbasic, S., Hrkac, S., Salai, G., Ivkovic, V., Coric, M., Novak, R., & Grgurevic, L. (2022). First Characterization of ADAMTS-4 in Kidney Tissue and Plasma of Patients with Chronic Kidney Disease—A Potential Novel Diagnostic Indicator. Diagnostics, 12(3), 648. https://doi.org/10.3390/diagnostics12030648