
Risk Assessment of the Progression of Early Knee Osteoarthritis by Collagen Neoepitope C2C: A Longitudinal Study of an Estonian Middle-Aged Cohort

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Radiographic Evaluation
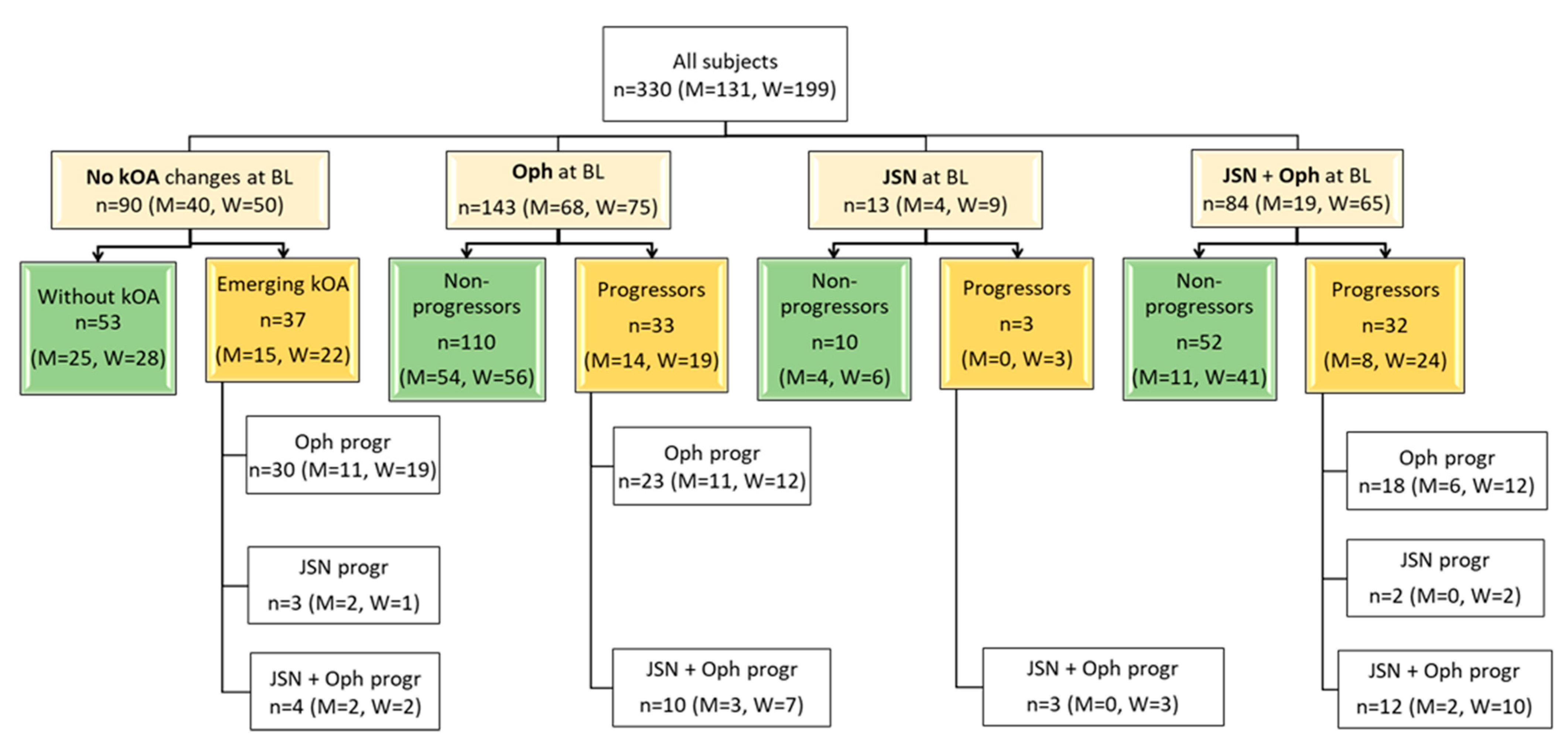
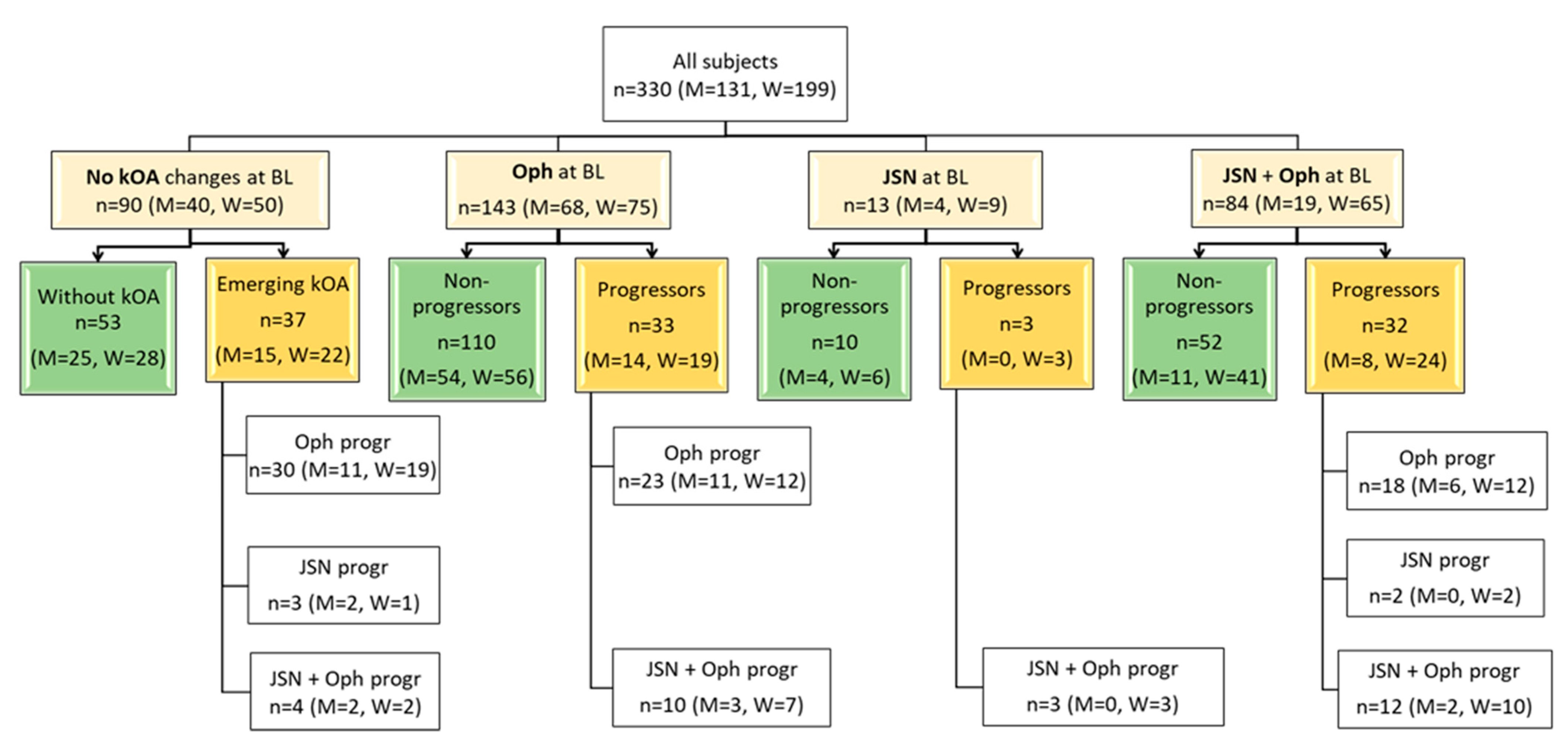
2.3. Definitions of Progression and Distribution of the Radiographic Groups
2.4. uC2C Measurement
2.5. Statistical Analysis
3. Results
3.1. Distribution of the Radiographic Groups
3.2. Baseline Characteristics of the Study Group
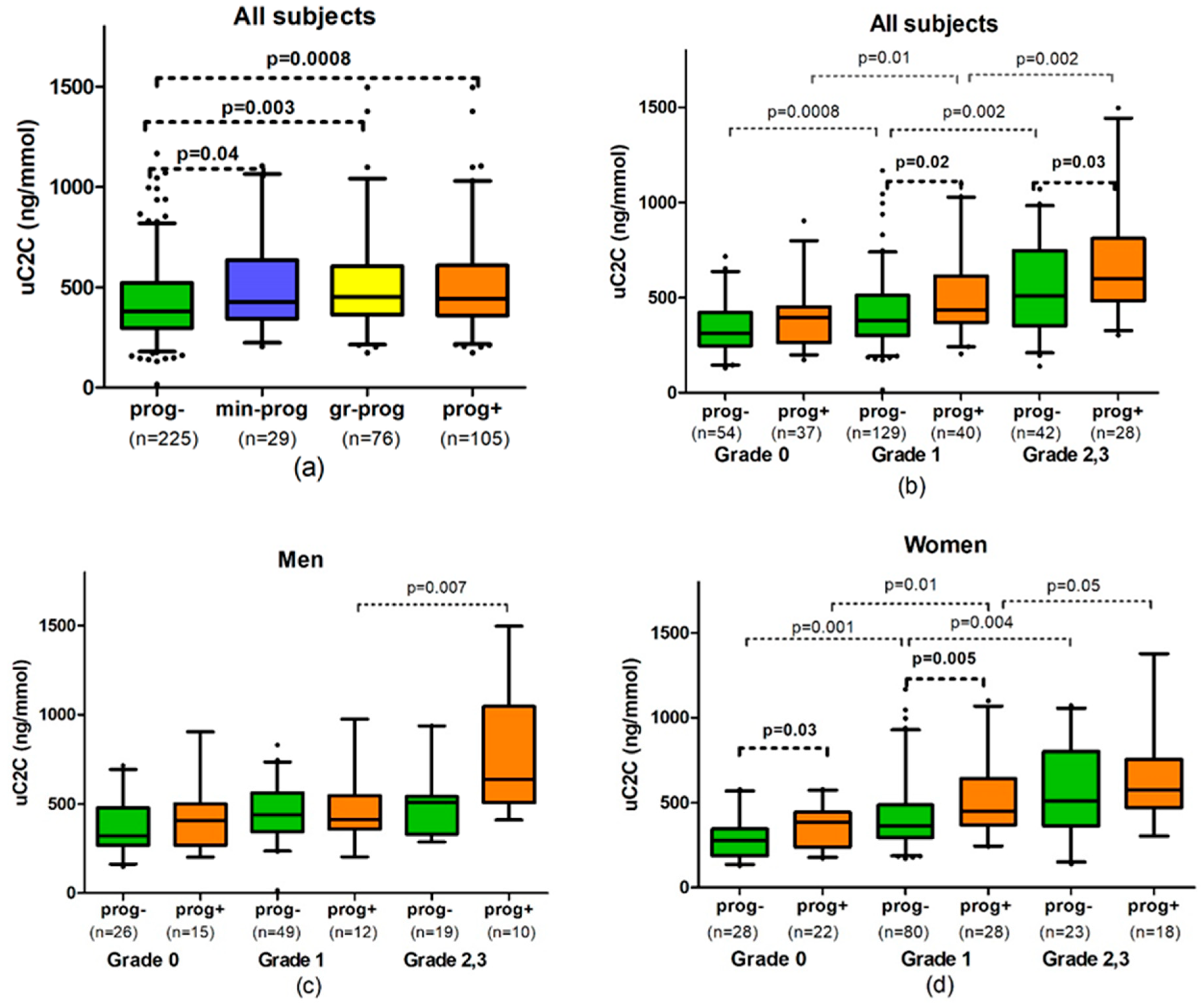
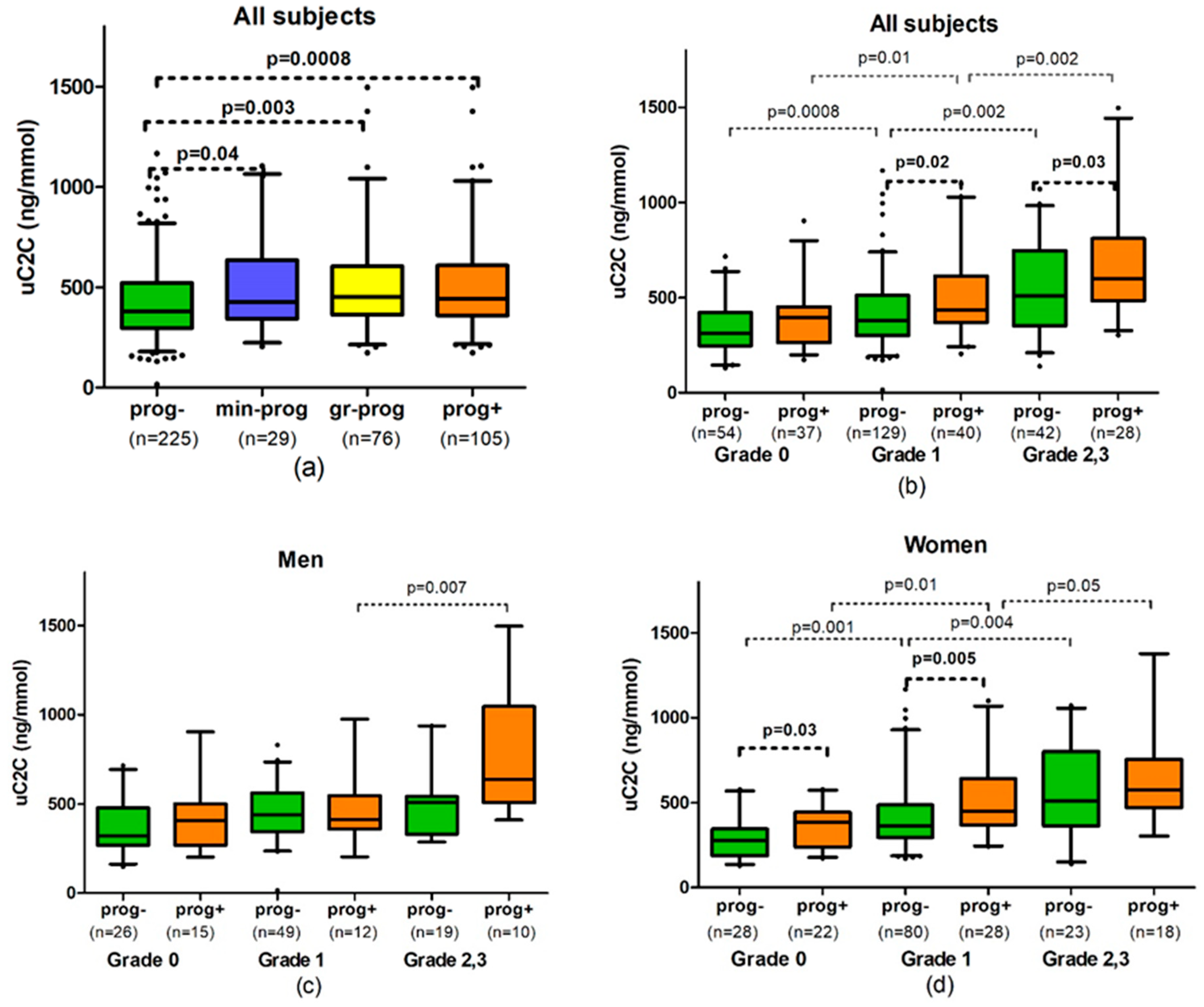
3.3. Association of uC2C Baseline Level with Three-Year kOA Progression
3.4. uC2C Prognostic Value for kOA Progressors in Distinct gOA
3.5. The Sex-Related Differences in Associations with uC2C at Baseline Level and kOA Progression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Baseline gOA Grade | Comparison Group | uC2C in All Subjects ng/mmol Medians (Q1–Q3) | p-Value between Groups | uC2C in Men ng/mmol Medians (Q1-Q3) | p-Value between Groups | uC2C in Women ng/mmol Medians (Q1–Q3) | p-Value between Groups | p-Value between Genders in the Group |
|---|---|---|---|---|---|---|---|---|
| All grades | Progressors (n = 105; M = 37) | 442.0 (361.0–604.0) | 0.0008 * | 426.0 (361.0–614.0) | 0.16 * | 445.5 (364.5–586.8) | 0.0009 * | 0.8 |
| gr-progressors (n = 76; M = 26) | 451.0 (365.5–589.2) | 0.003 ** | 418.5 (354.2–534.2) | 0.54 ** | 469.0 (370.8–642.2) | 0.001 ** | 0.5 | |
| min-progressors (n = 29; M = 11) | 426.0 (356.0–604.0) | 0.04 *** | 586.0 (413.5–987.5) | 0.06 *** | 410.5 (337.2–534.2) | 0.16 *** | 0.13 | |
| Non-progressors (n = 225; M = 94) | 380.0 (296.0–520.0) | 414.5 (318.2–539.2) | 360.0 (282.0–496.5) | 0.03 | ||||
| Grade 0 | Emerging kOA (n = 37; M = 15) | 395.0 (269.0–449.0) | 0.08 * | 407.0 (289.0–477.5) | 0.57 * | 387.0 (253.2–439.5) | 0.03 * | 0.6 |
| Without kOA (n = 54; M = 26) | 310.5 (249.8–414.8) | 322.0 (277.2–474.0) | 279.5 (200.8–338.2) | 0.03 | ||||
| Long term control group (n = 24; M = 14) | 290.5 (204.2–406.2) | 0.09 **** | 360.5 (261.0–468.5) | 0.65 **** | 225.0 (176.8–296.0) | 0.009 **** | 0.02 | |
| Grade 1 | Progressors (n = 40; M = 12) | 434.5 (374.0–607.0) | 0.02 * | 413.5 (374.5–517.0) | 0.83 * | 449.0 (374.0–624.8) | 0.005 * | 0.6 |
| gr-progressors (n = 24; M = 7) | 504.5 (400.0–660.2) | 0.001 ** | 484.0 (391.0–532.0) | 0.45 ** | 527.0 (430.0–688.0) | 0.0007 ** | 0.4 | |
| min-progressors (n = 16; M = 5) | 394.5 (304.5–443.5) | 0.95 *** | 409.0 (282.0–418.0) | 0.59 *** | 381.0 (321.5–449.0) | 0.57 *** | 1.0 | |
| Non-progressors (n = 129; M = 49) | 380.0 (302–512) | 440.0 (346.0–562.0) | 362.0 (296.8–473.2) | 0.04 | ||||
| Grade 2,3 | Progressors (n = 28: M = 10) | 600.0 (504.0–808.2) | 0.03 * | 640.0 (547.8–1019.5) | 0.11 * | 576.5 (484.0–732.0) | 0.59 * | 0.3 |
| gr-progressors (n = 15; M = 4) | 653.0 (547.5–773.0) | 0.03 ** | 574.5 (504.0–834.8) | 0.22 ** | 686.0 (570.5–773.0) | 0.18 ** | 0.6 | |
| min-progressors (n = 13; M = 6) | 572.0 (426.0–980.0) | 0.21 *** | 833.0 (606.0–1019.5) | 0.02 *** | 454.0 (384.5–565.5) | 0.67 *** | 0.03 | |
| Non-progressors (n = 42; M = 19) | 509.0 (360.0–743.5) | 507.0 (345.0–541.5) | 511.0 (371.5–776.0) | 0.5 |
References
- Loeser, R.F.; Goldring, S.R.; Scanzello, C.R.; Goldring, M.B. Osteoarthritis: A disease of the joint as an organ. Arthritis Rheum. 2012, 64, 1697–1707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldring, M.; Goldring, S.R. Articular cartilage and subchondral bone in the pathogenesis of osteoarthritis. Ann. N. Y. Acad. Sci. 2010, 1192, 230–237. [Google Scholar] [CrossRef]
- Wallace, I.J.; Worthington, S.; Felson, D.; Jurmain, R.D.; Wren, K.T.; Maijanen, H.; Woods, R.J.; Lieberman, D.E. Knee osteoarthritis has doubled in prevalence since the mid-20th century. Proc. Natl. Acad. Sci. USA 2017, 114, 9332–9336. [Google Scholar] [CrossRef] [Green Version]
- Kloppenburg, M.; Berenbaum, F. Osteoarthritis year in review 2019: Epidemiology and therapy. Osteoarthr. Cartil. 2020, 28, 242–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wyatt, L.; Moreton, B.; Mapp, P.; Wilson, D.; Hill, R.; Ferguson, E.; Scammell, B.; Walsh, D. Histopathological subgroups in knee osteoarthritis. Osteoarthr. Cartil. 2017, 25, 14–22. [Google Scholar] [CrossRef] [Green Version]
- Harkey, M.S.; Davis, J.E.; Lu, B.; Price, L.L.; Ward, R.J.; Mackay, J.W.; Eaton, C.B.; Lo, G.H.; Barbe, M.F.; Zhang, M.; et al. Early pre-radiographic structural pathology precedes the onset of accelerated knee osteoarthritis. BMC Musculoskelet. Disord. 2019, 20, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Karsdal, M.; Bihlet, A.; Byrjalsen, I.; Alexandersen, P.; Ladel, C.; Michaels, M.; Andersen, J.; Riis, B.; Kraus, V.; Bay-Jensen, A.; et al. OA phenotypes, rather than disease stage, drive structural progression—Identification of structural progressors from 2 phase III randomized clinical studies with symptomatic knee OA. Osteoarthr. Cartil. 2015, 23, 550–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraus, V.B.; Collins, J.E.; Hargrove, D.; Losina, E.; Nevitt, M.; Katz, J.N.; Wang, S.X.; Sandell, L.J.; Hoffmann, S.C.; Hunter, D.J. Predictive validity of biochemical biomarkers in knee osteoarthritis: Data from the FNIH OA Biomarkers Consortium. Ann. Rheum. Dis. 2016, 76, 186–195. [Google Scholar] [CrossRef]
- Hunter, D.J.; Nevitt, M.; Losina, E.; Kraus, V. Biomarkers for osteoarthritis: Current position and steps towards further validation. Best Pr. Res. Clin. Rheumatol. 2014, 28, 61–71. [Google Scholar] [CrossRef] [Green Version]
- Lotz, M.; Martel-Pelletier, J.; Christiansen, C.; Brandi, M.-L.; Bruyere, O.; Chapurlat, R.; Collette, J.; Cooper, C.; Giacovelli, G.; Kanis, J.A.; et al. Value of biomarkers in osteoarthritis: Current status and perspectives. Ann. Rheum. Dis. 2013, 72, 1756–1763. [Google Scholar] [CrossRef] [PubMed]
- Kraus, V.; Blanco, F.; Englund, M.; Henrotin, Y.; Lohmander, S.; Losina, E.; Önnerfjord, P.; Persiani, S. OARSI Clinical Trials Recommendations: Soluble biomarker assessments in clinical trials in osteoarthritis. Osteoarthr. Cartil. 2015, 23, 686–697. [Google Scholar] [CrossRef] [Green Version]
- Tamm, A.; Tamm, A.; Kumm, J.; Vija, M.; Lintrop, M. U-C2C in Estonian Early Knee OA Cohort: Progressive and Non-Progressive Cases. In Bone Abstracts; Bioscientifica: Bristol, UK, 2013; Volume 1. [Google Scholar] [CrossRef]
- Poole, A.R.; Ha, N.; Bourdon, S.; Sayre, E.C.; Guermazi, A.; Cibere, J. Ability of a Urine Assay of Type II Collagen Cleavage by Collagenases to Detect Early Onset and Progression of Articular Cartilage Degeneration: Results from a Population-based Cohort Study. J. Rheumatol. 2016, 43, 1864–1870. [Google Scholar] [CrossRef]
- Chu, C.R.; Williams, A.A.; Coyle, C.H.; Bowers, M.E. Early diagnosis to enable early treatment of pre-osteoarthritis. Arthritis Res. Ther. 2012, 14, 212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Favero, M.; Ramonda, R.; Goldring, M.B.; Goldring, S.R.; Punzi, L. Early knee osteoarthritis: Figure 1. RMD Open 2015, 1 (Suppl. 1), e000062. [Google Scholar] [CrossRef]
- Kisand, K.; Tamm, A.; Lintrop, M. New insights into the natural course of knee osteoarthritis: Early regulation of cytokines and growth factors, with emphasis on sex-dependent angiogenesis and tissue remodeling. A pilot study. Osteoarthr. Cartil. 2018, 26, 1045–1054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerna, I.; Kisand, K.; Tamm, A.E.; Kumm, J.; Tamm, A.O. Two Single-Nucleotide Polymorphisms in ADAM12 Gene Are Associated with Early and Late Radiographic Knee Osteoarthritis in Estonian Population. Arthritis 2013, 2013, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Kerna, I.; Kisand, K.; Suutre, S.; Murde, M.; Tamm, A.; Kumm, J.; Tamm, A. The ADAM12 is upregulated in synovitis and postinflammatory fibrosis of the synovial membrane in patients with early radiographic osteoarthritis. Jt. Bone Spine 2014, 81, 51–56. [Google Scholar] [CrossRef]
- Roos, E.; Roos, H.P.; Lohmander, S.; Ekdahl, C.; Beynnon, B.D. Knee Injury and Osteoarthritis Outcome Score (KOOS)—Development of a Self-Administered Outcome Measure. J. Orthop. Sports Phys. Ther. 1998, 28, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Kumm, J.; Tamm, A.; Lintrop, M.; Tamm, A. The prevalence and progression of radiographic knee osteoarthritis over 6 years in a population-based cohort of middle-aged subjects. Rheumatol. Int. 2011, 32, 3545–3550. [Google Scholar] [CrossRef] [PubMed]
- Nagaosa, Y.; Mateus, M.; Hassan, B.; Lanyon, P.; Doherty, M. Development of a logically devised line drawing atlas for grading of knee osteoarthritis. Ann. Rheum. Dis. 2000, 59, 587–595. [Google Scholar] [CrossRef] [Green Version]
- Kuhi, L.; Tamm, A.E.; Tamm, A.O.; Kisand, K. Cartilage collagen neoepitope C2C in urine as an integrative diagnostic marker for early knee osteoarthritis. Osteoarthr. Cartil. Open 2020, 2, 100096. [Google Scholar] [CrossRef]
- Hosnijeh, F.S.; Runhaar, J.; van Meurs, J.B.; Bierma-Zeinstra, S.M. Biomarkers for osteoarthritis: Can they be used for risk assessment? A systematic review. Maturitas 2015, 82, 36–49. [Google Scholar] [CrossRef]
- Dam, E.B.; Loog, M.; Christiansen, C.; Byrjalsen, I.; Folkesson, J.; Nielsen, M.; Qazi, A.A.; Pettersen, P.C.; Garnero, P.; Karsdal, M.A. Identification of progressors in osteoarthritis by combining biochemical and MRI-based markers. Arthritis Res. Ther. 2009, 11, R115. [Google Scholar] [CrossRef] [Green Version]
- Wirth, W.; Hunter, D.; Nevitt, M.C.; Sharma, L.; Kwoh, C.; Ladel, C.; Eckstein, F. Predictive and concurrent validity of cartilage thickness change as a marker of knee osteoarthritis progression: Data from the Osteoarthritis Initiative. Osteoarthr. Cartil. 2017, 25, 2063–2071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sobue, Y.; Kojima, T.; Kurokouchi, K.; Takahashi, S.; Yoshida, H.; Poole, R.; Ishiguro, N. Prediction of progression of damage to articular cartilage 2 years after anterior cruciate ligament reconstruction: Use of aggrecan and type II collagen biomarkers in a retrospective observational study. Arthritis Res. 2017, 19, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Boegård, T.; Rudling, O.; Petersson, I.F.; Jonsson, K. Correlation between radiographically diagnosed osteophytes and magnetic resonance detected cartilage defects in the tibiofemoral joint. Ann. Rheum. Dis. 1998, 57, 401–407. [Google Scholar] [CrossRef] [Green Version]
- Roemer, F.W.; Guermazi, A.; Niu, J.; Zhang, Y.; Mohr, A.; Felson, D. Prevalence of magnetic resonance imaging-defined atrophic and hypertrophic phenotypes of knee osteoarthritis in a population-based cohort. Arthritis Rheum. 2012, 64, 429–437. [Google Scholar] [CrossRef]
- Zhu, Z.; Ding, C.; Han, W.; Zheng, S.; Winzenberg, T.; Cicuttini, F.; Jones, G. MRI-detected osteophytes of the knee: Natural history and structural correlates of change. Arthritis Res. 2018, 20, 237. [Google Scholar] [CrossRef] [Green Version]
- Van Spil, W.; Welsing, P.; Bierma-Zeinstra, S.; Bijlsma, J.; Roorda, L.; Cats, H.; Lafeber, F. The ability of systemic biochemical markers to reflect presence, incidence, and progression of early-stage radiographic knee and hip osteoarthritis: Data from CHECK. Osteoarthr. Cartil. 2015, 23, 1388–1397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boeth, H.; MacMahon, A.; Poole, A.R.; Buttgereit, F.; Önnerfjord, P.; Lorenzo, P.; Klint, C.; Pramhed, A.; Duda, G.N. Differences in biomarkers of cartilage matrix turnover and their changes over 2 years in adolescent and adult volleyball athletes. J. Exp. Orthop. 2017, 4, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cibere, J.; Zhang, H.; Garnero, P.; Poole, A.R.; Lobanok, T.; Saxne, T.; Kraus, V.B.; Way, A.; Thorne, A.; Wong, H.; et al. Association of biomarkers with pre-radiographically defined and radiographically defined knee osteoarthritis in a population-based study. Arthritis Rheum. 2009, 60, 1372–1380. [Google Scholar] [CrossRef] [PubMed]
- Kraus, V.B.; Hargrove, D.E.; Hunter, D.J.; Renner, J.B.; Jordan, J.M. Establishment of reference intervals for osteoarthritis-related soluble biomarkers: The FNIH/OARSI OA Biomarkers Consortium. Ann. Rheum. Dis. 2016, 76, 179–185. [Google Scholar] [CrossRef]
- Deveza, L.A.; Nelson, A.E.; Loeser, R.F. Phenotypes of osteoarthritis: Current state and future implications. Clin. Exp. Rheumatol. 2019, 37, 64–72. [Google Scholar]
- Van Spil, W.E.; Kubassova, O.; Boesen, M.; Bay-Jensen, A.-C.; Mobasheri, A. Osteoarthritis phenotypes and novel therapeutic targets. Biochem. Pharmacol. 2019, 165, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Gardiner, B.S.; Woodhouse, F.G.; Besier, T.; Grodzinsky, A.J.; Lloyd, D.; Zhang, L.; Smith, D. Predicting Knee Osteoarthritis. Ann. Biomed. Eng. 2016, 44, 222–233. [Google Scholar] [CrossRef] [Green Version]
- Atkinson, A.; Colburn, W.; Degruttola, V.; Demets, D.; Downing, G.; Hoth, D.; Oates, J.; Peck, C.; Schooley, R.; Spilker, B.; et al. Biomarkers and Surrogate Endpoints: Preferred Definitions and Conceptual Framework. Clin. Pharmacol. Ther. 2001, 69, 89–95. [Google Scholar]
| Grade 0 | Grade 1 | Grade 2 | Grade 3 | Overall | |
|---|---|---|---|---|---|
| Subjects, n, (% all subjects) | 91 (27.6) | 169 (51.2) | 55 (16.7) | 15 (4.5) | 330 |
| Progressors, n, (%, subjects in the grade) | 37 (41) | 40 (24) | 23 (42) | 5 (33) | 105 |
| A. gr-progressors, n, (%, subjects in the grade) | 37 (41) | 24 (14) | 15 (27) | - | 76 |
| B. min-progressors, n (%, subjects in the grade) | - | 16 (10) | 8 (15) | 5 (33) | 29 |
| Non-progressors, n (%, subjects in the grade) | 54 (59) | 129 (76) | 32 (58) | 10 (67) | 225 |
| Men, n, (% in the grade) | 41 (45) | 61 (36) | 21 (38) | 8 (53) | 131 |
| Male progressors, n | 15 | 12 | 7 | 3 | 37 |
| Male gr-progressors, n | 15 | 7 | 4 | - | 26 |
| Male min-progressors, n | - | 5 | 3 | 3 | 11 |
| Male non-progressors, n | 26 | 49 | 14 | 5 | 94 |
| Women, n, (% in the grade) | 50 (55) | 108 (64) | 34 (62) | 7 (47) | 199 |
| Female progressors, n | 22 | 28 | 16 | 2 | 68 |
| Female gr-progressors, n | 22 | 17 | 11 | - | 50 |
| Female min-progressors, n | - | 11 | 5 | 2 | 18 |
| Female non-progressors, n | 28 | 80 | 18 | 5 | 131 |
| Grade 0 | Grade 1 | Grade 2 | Grade 3 | p-Value, Difference between Grades | Overall | |
|---|---|---|---|---|---|---|
| Mean age in all subjects, years, ± SD | 46.1 ±6.5 | 47.7 ±6.2 | 49.5 ±6.8 | 48.6 ±6.6 | 0.02 * | 47.6 ±6.5 |
| Mean age in progressors, years ± SD | 46.4 ±6.2 | 47.8 ±6.2 | 50.1 ±6.3 | 52.2 ±3.4 | 0.007 * | 48.0 ±6.2 |
| Mean age in gr-progressors, years ± SD | 46.4 ±6.2 | 49.5 ±5.5 | 49.4 ±7.0 | - | 0.06 * | 48.0 ±6.3 |
| Mean age in min-progressors, years ± SD | - | 45.3 ±6.3 | 51.4 ±4.9 | 52.2 ±3.4 | 0.008 * | 48.1 ±6.3 |
| Mean age in non-progressors, years ± SD | 45.8 ±6.7 | 47.6 ±6.2 | 49.1 ±7.1 | 46.8 ±7.2 | 0.09 * | 47.4 ±6.5 |
| p-value, age difference between the investigated progression groups | 0.7 ** | 0.3 * | 0.8 * | 0.07 ** | 0.8 * | |
| BMI, kg/m2 ± SD | 26.2 ±5.1 | 28.0 ±4.8 | 30.5 ±5.8 | 29.5 ±6.1 | 1.5 × 10−5 * | 28.0 ± 5.3 |
| BMI in progressors, kg/m2 ± SD | 26.8 ±5.2 | 29.0 ±4.6 | 33.0 ±6.2 | 34.2 ±6.2 | 4.2 × 10−6 * | 29.3 ±5.8 |
| BMI in gr-progressors, kg/m2 ± SD | 26.8 ±5.2 | 30.8 ±3.8 | 32.9 ±6.2 | - | 5.0 × 10−5 * | 29.2 ±5.6 |
| BMI in min-progressors, kg/m2 ± SD | - | 26.3 ±4.5 | 33.2 ±6.7 | 34.2 ±6.2 | 0.002 * | 29.6 ±6.4 |
| BMI in non-progressors, kg/m2 ± SD | 25.8 ±5.0 | 27.7 ±4.8 | 28.7 ±4.8 | 27.2 ±4.8 | 0.6 * | 27.4 ±4.9 |
| p-value, BMI difference between the investigated progression groups | 0.4 ** | 0.02 * | 0.01 * | 0.06 ** | 0.02 * | |
| Mean age in men, years ± SD | 46.3 ±6.4 | 46.6 ±7.1 | 47.2 ±7.5 | 47.3 ±6.7 | 0.6 * | 46.6 ± 6.9 |
| Mean age in women years ± SD | 45.9 ±6.6 | 48.2 ±5.5 | 50.9 ±5.9 | 50.0 ±6.8 | 0.0003 * | 48.2 ± 6.1 |
| p-value, age difference between sexes | 0.8 ** | 0.1 ** | 0.06 ** | 0.5 ** | 0.04 ** | |
| BMI in men, kg/m2 ± SD | 27.5 ±5.6 | 28.1 ±3.8 | 28.5 ±4.4 | 30.1 ±6.9 | 0.1 * | 28.1 ± 4.7 |
| BMI in women, kg/m2 ± SD | 25.2 ±4.4 | 28.0 ±5.3 | 31.7 ±6.2 | 28.8 ±5.5 | 1.2 × 10−6 * | 27.9 ± 5.6 |
| p-value, BMI difference between sexes | 0.03 ** | 0.8 ** | 0.03 ** | 0.7 ** | 0.7 ** | |
| BMI in female progressors, kg/m2 ± SD | 26.5 ±4.8 | 29.2 ±5.2 | 33.8 ±6.8 | 31.4 ±7.8 | 0.0004 * | 29.5 ±6.1 |
| BMI in female non-progressors, kg/m2 ± SD | 24.0 ±3.9 | 27.5 ±5.2 | 29.9 ±5.1 | 27.8 ±5.0 | 5.0 × 10−5 * | 27.1 ±5.2 |
| p-value, BMI difference between female progression groups | 0.06 ** | 0.2 ** | 0.08 ** | 0.6 ** | 0.008 ** | |
| Mean knee VAS score (0–10) | 1.0 ±2.0 | 2.3 ±2.5 | 3.2 ±2.9 | 3.6 ±3.3 | 2.2 × 10−7 * | 2.2 ±2.6 |
| Models | Independent Variables in the Model | All Subjects | Men | Women | ||||
|---|---|---|---|---|---|---|---|---|
| Baseline gOA | Compared Groups | OR (CI 95%) | AUC (CI 95%) | OR (CI 95%) | AUC (CI 95%) | OR (CI 95%) | AUC (CI 95%) | |
| All grades | Progressor, n = 105 (M = 37) Non-progressors, n = 225 (M = 94) | log2(C2C) Age BMI Sex gOA | 2.34 (1.48–3.68) *** 0.99 (0.95–1.03) 1.07 (1.02–1.12) ** 1.54 (0.92–2.59) 0.67 (0.47–0.96) * | 0.67 (0.61–0.73) | 2.59 (1.18–5.70) * 0.96 (0.90–1.02) 1.05 (0.97–1.15) – 0.78 (0.47–1.31) | 0.65 (0.55–0.75) | 2.22 (1.26–3.92) ** 1.01 (0.96–1.07) 1.07 (1.01–1.14) * – 0.57 (0.35–0.93) * | 0.68 (0.60–0.76) |
| All grades | gr-progressors, n = 76 (M = 26) Non-progressors, n = 225 (M = 94) | log2(C2C) Age BMI Sex gOA | 2.80 (1.66–4.72) *** 0.99 (0.95–1.04) 1.08 (1.02–1.14) ** 1.72 (0.95–3.13) 0.34 (0.21–0.55) *** | 0.73 (0.67–0.79) | 2.23 (0.93–5.35) 0.96 (0.90–1.03) 1.01 (0.92–1.11) – 0.40 (0.20–0.81)* | 0.68 (0.57–0.8) | 3.27 (1.66–6.46) *** 1.01 (0.95–1.08) 1.11 (1.04–1.20)** – 0.26 (0.13–0.51)*** | 0.76 (0.68–0.84) |
| Grade 0 | Emerging kOA, n = 37 (M = 15) Without kOA, n = 54 (M = 26) | log2(C2C) Age BMI Sex | 2.58 (1.08–6.16) * 0.98 (0.91–1.05) 1.03 (0.94–1.13) 2.09 (0.81–5.37) | 0.64 (0.53–0.76) | 2.44 (0.63–9.48) 0.95 (0.85–1.07) 0.96 (0.85–1.09) – | 0.58 (0.39–0.77) | 2.86 (0.85–9.58) 0.99 (0.89–1.09) 1.11 (0.96–1.29) – | 0.72 (0.57–0.87) |
| Grade 0 | Emerging kOA, n = 37 (M = 15) Long-term control group, n = 24 (M = 14) | log2(C2C) Age BMI Sex | 5.87 (1.71–20.22) ** 0.86 (0.77–0.96) ** 1.00 (0.88–1.13) 4.01 (1.12–14.39) * | 0.79 (0.67–0.91) | 5.19 (0.79–34.15) 0.84 (0.71–0.99) * 0.90 (0.76–1.07) – | 0.7 (0.50–0.90) | 22.95 (2.15–245) ** 0.76 (0.60–0.97) * 1.32 (0.95–1.83) – | 0.91 (0.81–1) |
| Grade 1 | Progressors, n = 40 (M = 12) Non-progressors, n = 129 (M = 49) | log2(C2C) Age BMI Sex | 2.36 (1.19–4.67) * 0.98 (0.91–1.04) 1.06 (0.98–1.14) 1.56 (0.70–3.48) | 0.67 (0.57–0.76) | 1.59 (0.49–5.15) 0.96 (0.87–1.05) 1.05 (0.89–1.25) – | 0.60 (0.42–0.78) | 2.67 (1.18–6.04) * 0.99 (0.91–1.08) 1.05 (0.97–1.14) – | 0.68 (0.56–0.80) |
| Grade 2,3 | Progressors, n = 28 (M = 10) Non-progressors, (grade 2,3), n = 42 (M = 19) | log2(C2C) Age BMI Sex | 2.22 (0.89–5.55) 1.02 (0.93–1.13) 1.15 (1.03–1.29) * 1.06 (0.33–3.41) | 0.77 (0.66–0.88) | 11.41 (0.86–151) 0.91 (0.75–1.11) 1.30 (1.00–1.68) – | 0.85 (0.70–1) | 1.32 (0.45–3.82) 1.10 (0.95–1.26) 1.12 (0.99–1.27) – | 0.70 (0.53–0.86) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuhi, L.; Tamm, A.E.; Tamm, A.O.; Kisand, K. Risk Assessment of the Progression of Early Knee Osteoarthritis by Collagen Neoepitope C2C: A Longitudinal Study of an Estonian Middle-Aged Cohort. Diagnostics 2021, 11, 1236. https://doi.org/10.3390/diagnostics11071236
Kuhi L, Tamm AE, Tamm AO, Kisand K. Risk Assessment of the Progression of Early Knee Osteoarthritis by Collagen Neoepitope C2C: A Longitudinal Study of an Estonian Middle-Aged Cohort. Diagnostics. 2021; 11(7):1236. https://doi.org/10.3390/diagnostics11071236
Chicago/Turabian StyleKuhi, Liisa, Ann E. Tamm, Agu O. Tamm, and Kalle Kisand. 2021. "Risk Assessment of the Progression of Early Knee Osteoarthritis by Collagen Neoepitope C2C: A Longitudinal Study of an Estonian Middle-Aged Cohort" Diagnostics 11, no. 7: 1236. https://doi.org/10.3390/diagnostics11071236
APA StyleKuhi, L., Tamm, A. E., Tamm, A. O., & Kisand, K. (2021). Risk Assessment of the Progression of Early Knee Osteoarthritis by Collagen Neoepitope C2C: A Longitudinal Study of an Estonian Middle-Aged Cohort. Diagnostics, 11(7), 1236. https://doi.org/10.3390/diagnostics11071236