
Low Lymphocyte-to-Monocyte Ratio Is the Potential Indicator of Worse Overall Survival in Patients with Renal Cell Carcinoma and Venous Tumor Thrombus


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Survival Analysis
3.3. Univariate and Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arda, E.; Yuksel, I.; Cakiroglu, B.; Akdeniz, E.; Cilesiz, N. Valuation of Neutrophil/Lymphocyte Ratio in Renal Cell Carcinoma Grading and Progression. Cureus 2018, 10, e2051. [Google Scholar] [CrossRef] [Green Version]
- Casamassima, A.; Picciariello, M.; Quaranta, M.; Berardino, R.; Ranieri, C.; Paradiso, A.; Lorusso, V.; Guida, M. C-reactive protein: A biomarker of survival in patients with metastatic renal cell carcinoma treated with subcutaneous interleukin-2 based immunotherapy. J. Urol. 2005, 173, 52–55. [Google Scholar] [CrossRef]
- Pichler, M.; Hutterer, G.C.; Stoeckigt, C.; Chromecki, T.F.; Stojakovic, T.; Golbeck, S.; Eberhard, K.; Gerger, A.; Mannweiler, S.; Pummer, K.; et al. Validation of the pre-treatment neutrophil-lymphocyte ratio as a prognostic factor in a large European cohort of renal cell carcinoma patients. Br. J. Cancer 2013, 108, 901–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Li, S.; Xu, Z.; Wang, K.; Fu, D.; Liu, Q.; Wang, X.; Wu, B. Clinical and oncological outcomes in Chinese patients with renal cell carcinoma and venous tumor thrombus extension: Single-center experience. World J. Surg. Oncol. 2015, 13, 14. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.; Fu, Q.; Xu, L.; Zhou, L.; Liu, Z.; Yang, Y.; Lin, Z.; Xu, J. Prognostic value of preoperative lymphocyte to monocyte ratio in patients with nonmetastatic clear cell renal cell carcinoma. Tumour Biol. 2016, 37, 4613–4620. [Google Scholar] [CrossRef] [PubMed]
- Colotta, F.; Allavena, P.; Sica, A.; Garlanda, C.; Mantovani, A. Cancer-related inflammation, the seventh hallmark of cancer: Links to genetic instability. Carcinogenesis 2009, 30, 1073–1081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.; Wang, K.; Lu, H.; Xue, D.; Fan, M.; Zhuang, Q.; Yin, S.; He, X.; Xu, R. Systemic inflammation response index predicts prognosis in patients with clear cell renal cell carcinoma: A propensity score-matched analysis. Cancer Manag. Res. 2019, 11, 909–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elghiaty, A.; Kim, J.; Jang, W.S.; Park, J.S.; Heo, J.E.; Rha, K.H.; Choi, Y.D.; Ham, W.S. Predictive value of preoperative monocyte–lymphocyte ratio among patients with localized clear renal cell carcinoma of ≤7 cm on preoperative imaging. Medicine 2018, 97, e13433. [Google Scholar] [CrossRef] [PubMed]
- Ravindranathan, D.; Master, V.A.; Bilen, M.A. Inflammatory Markers in Cancer Immunotherapy. Biology 2021, 10, 325. [Google Scholar] [CrossRef]
- Kunc, M.; Gabrych, A.; Dulak, D.; Karolina, H.; Styczewska, M.; Szmyd, D.; Nilsson, K.; Iwinski, M.; Sobocińska-Mirska, A.; Sawicka-Zukowska, M.; et al. Systemic inflammatory markers and serum lactate dehydrogenase predict survival in patients with Wilms tumour. Arch. Med Sci. 2021. [Google Scholar] [CrossRef]
- Rebuzzi, S.E.; Signori, A.; Banna, G.L.; Maruzzo, M.; De Giorgi, U.; Pedrazzoli, P.; Sbrana, A.; Zucali, P.A.; Masini, C.; Naglieri, E.; et al. Inflammatory indices and clinical factors in metastatic renal cell carcinoma patients treated with nivolumab: The development of a novel prognostic score (Meet-URO 15 study). Ther. Adv. Med. Oncol. 2021, 13, 17588359211019642. [Google Scholar] [CrossRef]
- Ramsey, S.; Lamb, G.W.; Aitchison, M.; Graham, J.; McMillan, D.C. Evaluation of an inflammation-based prognostic score in patients with metastatic renal cancer. Cancer 2007, 109, 205–212. [Google Scholar] [CrossRef]
- Fox, P.; Hudson, M.; Brown, C.; Lord, S.; Gebski, V.; De Souza, P.; Lee, C.K. Markers of systemic inflammation predict survival in patients with advanced renal cell cancer. Br. J. Cancer 2013, 109, 147–153. [Google Scholar] [CrossRef] [Green Version]
- Rajwa, P.; Zyczkowski, M.; Paradysz, A.; Slabon-Turska, M.; Suliga, K.; Bujak, K.; Bryniarski, P. Novel hematological biomarkers predict survival in renal cell carcinoma patients treated with nephrectomy. Arch. Med. Sci. 2020, 16, 1062–1071. [Google Scholar] [CrossRef]
- Qi, J.; Gu, Z.; Chen, F.; Shen, H.; Chen, J.; Zhang, L.; Wang, W. Management of renal cell carcinoma with tumor thrombus in renal vein and the inferior vena cava. Ann. Vasc. Surg. 2010, 24, 1089–1093. [Google Scholar] [CrossRef]
- Antonelli, A.; Sodano, M.; Sandri, M.; Tardanico, R.; Yarigina, M.; Furlan, M.; Galvagni, G.; Zanotelli, T.; Cozzoli, A.; Simeone, C. Venous tumor thrombus consistency is not predictive of survival in patients with renal cell carcinoma: A retrospective study of 147 patients. Int. J. Urol. 2015, 22, 534–539. [Google Scholar] [CrossRef] [Green Version]
- Boissier, R.; Campagna, J.; Branger, N.; Karsenty, G.; Lechevallier, E. The prognostic value of the neutrophil-lymphocyte ratio in renal oncology: A review. Urol. Oncol. 2017, 35, 135–141. [Google Scholar] [CrossRef]
- Sobin, L.H.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumors, ed. U.I.U.A.; Wiley-Blackwell: Hoboken, NJ, USA, 2009; p. 7. [Google Scholar]
- Mastoraki, A.; Mastoraki, S.; Tsikala-Vafea, M.; Papanikolaou, I.S.; Lazaris, A.; Smyrniotis, V.; Arkadopoulos, N. Prognostic Benefit of Surgical Management of Renal Cell Carcinoma Invading the Inferior Vena Cava. Indian J. Surg. Oncol. 2017, 8, 14–18. [Google Scholar] [CrossRef] [Green Version]
- Neves, R.J.; Zincke, H. Surgical treatment of renal cancer with vena cava extension. Br. J. Urol. 1987, 59, 390–395. [Google Scholar] [CrossRef]
- R Core Team: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020.
- Kassambara, A.; Kosinski, M.; Biecek, P.; Survminer. Drawing Survival Curves Using “ggplot2”. R Package Version 0.4.8. 2020. Available online: https://CRAN.R-project.org/package=survminer (accessed on 1 July 2021).
- Xiao, N. ggplot2Scientific Journal and Sci-Fi ThemedColor Palettes for “ggplot2”; R Package Version 2.7; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- de Martino, M.; Pantuck, A.J.; Hofbauer, S.; Waldert, M.; Shariat, S.F.; Belldegrun, A.S.; Klatte, T. Prognostic impact of preoperative neutrophil-to-lymphocyte ratio in localized nonclear cell renal cell carcinoma. J. Urol. 2013, 190, 1999–2004. [Google Scholar] [CrossRef]
- Peyton, C.C.; Abel, E.J.; Chipollini, J.; Boulware, D.C.; Azizi, M.; Karam, J.A.; Margulis, V.; Master, V.A.; Matin, S.F.; Raman, J.D.; et al. The Value of Neutrophil to Lymphocyte Ratio in Patients Undergoing Cytoreductive Nephrectomy with Thrombectomy. Eur. Urol. Focus 2020, 6, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Otunctemur, A.; Dursun, M.; Besiroglu, H.; Ozer, K.; Horsanali, O.; Ozbek, E. Clinical Significance of Preoperative Neutrophil-to-Lymphocyte Ratio in Renal Cell Carcinoma. Int. Braz. J. Urol. 2016, 42, 678–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutterer, G.C.; Stoeckigt, C.; Stojakovic, T.; Jesche, J.; Eberhard, K.; Pummer, K.; Zigeuner, R.; Pichler, M. Low preoperative lymphocyte-monocyte ratio (LMR) represents a potentially poor prognostic factor in nonmetastatic clear cell renal cell carcinoma. Urol. Oncol. 2014, 32, 1041–1048. [Google Scholar] [CrossRef]
- Wang, Z.; Peng, S.; Wang, A.; Xie, H.; Guo, L.; Jiang, N.; Niu, Y. Platelet-lymphocyte ratio acts as an independent predictor of prognosis in patients with renal cell carcinoma. Clin. Chim. Acta 2018, 480, 166–172. [Google Scholar] [CrossRef]
- Hu, H.; Yao, X.; Xie, X.; Wu, X.; Zheng, C.; Xia, W.; Ma, S. Prognostic value of preoperative NLR, dNLR, PLR and CRP in surgical renal cell carcinoma patients. World J. Urol. 2017, 35, 261–270. [Google Scholar] [CrossRef]
- Saroha, S.; Uzzo, R.G.; Plimack, E.R.; Ruth, K.; Al-Saleem, T. Lymphopenia is an independent predictor of inferior outcome in clear cell renal carcinoma. J. Urol. 2013, 189, 454–461. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | N (%) | |
|---|---|---|
| Gender | Male | 50 (54.5) |
| Female | 41 (45.5) | |
| Age | Median: 66 (IQR 60–71 years) | |
| Histology | Clear cell | 88 (97) |
| other | 3 (3) | |
| Grade | Low (G1–2) | 28 (30) |
| High (G3–4) | 63 (70) | |
| T | 3a | 88 (97) |
| 3b | 1 (1) | |
| 3c | - | |
| 4 | 2 (2) | |
| N | 0 | 78 (86) |
| 1 | 13 (14) | |
| M | 0 | 67 (74) |
| 1 | 24 (26) | |
| R | 0 | 70 (77) |
| 1–2 | 21 (23) | |
| Tumor necrosis | Present | 41 (45.5) |
| absent | 50 (54.5) | |
| Mayo stage | Low (0–1) | 85 (93) |
| High (≥2) | 6 (7) | |
| LOH | Short (≤9 days) | 61 (67) |
| Long | 29 (33) | |
| Clavien-Dindo | Low (0–1) | 79 (87) |
| High ≥2 | 12 (13) | |
| Death during follow-up | No | 58 (64) |
| Yes | 33 (36) | |
| Preoperative values | Lymphocytes | median 1.55 IQR—1.18–2.12 |
| Monocytes | median 0.82 IQR—0.6–1.04 | |
| Neutrophils | median 4.91 IQR—3.8–6.26 | |
| Platelets | median 262.5 IQR—220–334 | |
| LMR | median—1.96 IQR—1.41–3.05 | |
| NLR | median—3.18 IQR—2.04–4.79 | |
| PLR | median—166 IQR—119–234 | |
| Feature | NLR | p (q) | PLR | p (q) | LMR | p (q) |
|---|---|---|---|---|---|---|
| Sex | ||||||
| Male | 3.47 (2.32–4.79) | 0.16 (0.28) | 172 (127–226) | 0.8 (0.9) | 1.67 (1.26–2.53) | 0.008 * (0.07) |
| Female | 2.86 (1.88–4.26) | 160 (116–233) | 2.64 (1.57–3.49) | |||
| Nodal status | ||||||
| N0 | 3.12 (2.04–4.78) | 0.86 (0.9) | 160 (117–249) | 0.66 (0.85) | 2.01 (1.46–3.10) | 0.15 (0.34) |
| N1 | 3.34 (2.30–4.26) | 188 (157–229) | 1.60 (0.97–2.20) | |||
| Distant metastases | ||||||
| M0 | 2.95 (1.90–4.57) | 0.15 (0.31) | 156 (113–222) | 0.021 * (0.126) | 2.06 (1.47–3.44) | 0.02 * (0.11) |
| M1 | 3.63 (2.76–5.21) | 217 (151–260) | 1.66 (1.18–2.15) | |||
| Grade | ||||||
| Low (1–2) | 3.39 (1.74–4.59) | 0.63 (0.88) | 155 (104–230) | 0.32 (0.47) | 1.82 (1.49–2.93) | 0.76 (0.9) |
| High (3–4) | 3.07 (2.04–5.16) | 178 (120–249) | 2.03 (1.39–3.05) | |||
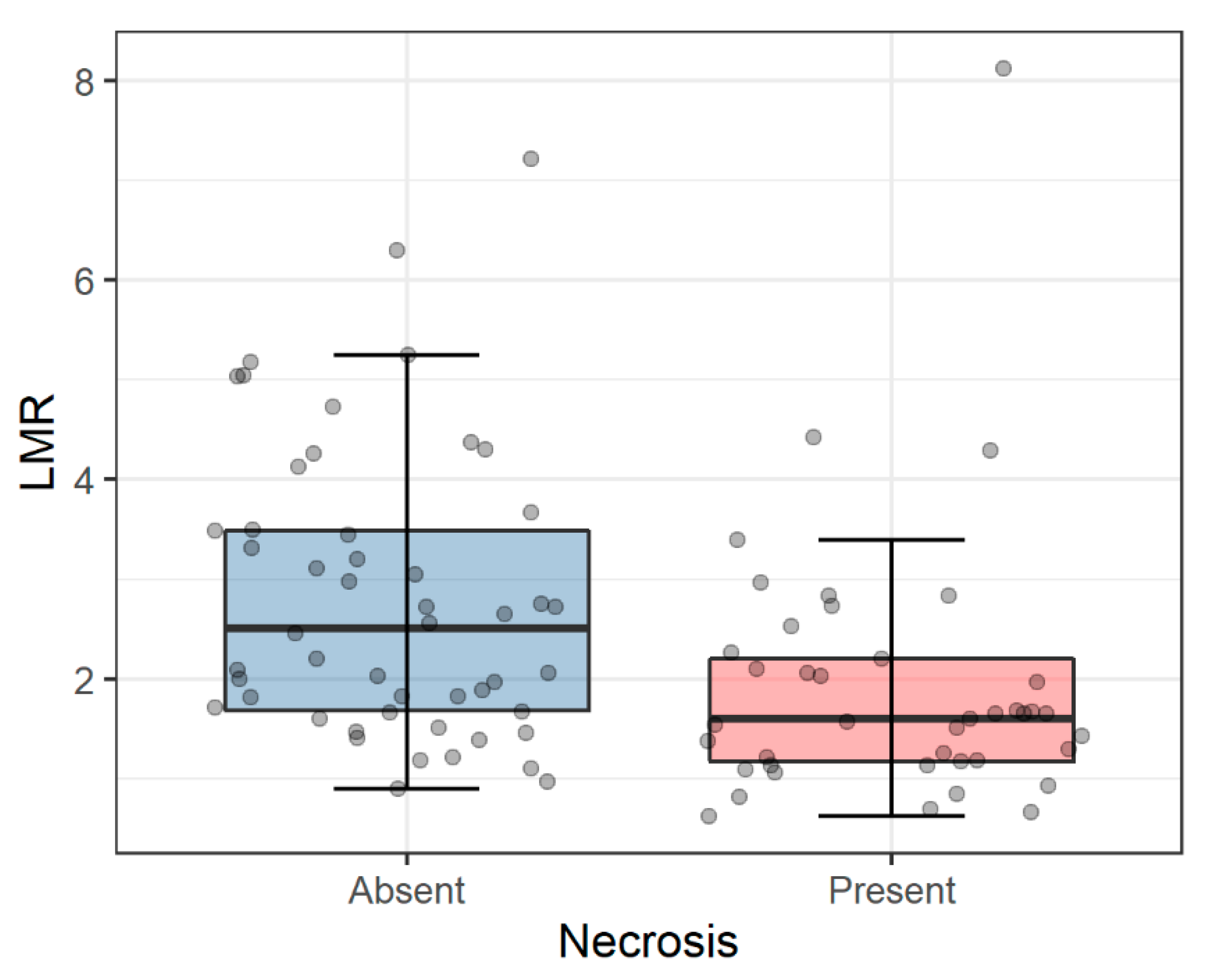
| Necrosis | ||||||
| No | 2.82 (2.00–4.25) | 0.03 * (0.11) | 163 (116–217) | 0.24 (0.39) | 2.51 (1.67–3.49) | 0.0004 * (0.007) * |
| Yes | 3.73 (2.77–5.56) | 181 (128–258) | 1.60 (1.17–2.21) | |||
| Mayo stage | ||||||
| Low | 3.18 (2.05–4.74) | 0.1 (0.3) | 166 (119–249 | 0.9 (0.9) | 2.00 (1.46–3.10) | 0.1 (0.26) |
| High | 2.93 (1.67–5.73) | 176 (128–226) | 1.46 (1.09–2.10) |
| Feature | HR (95% CI) | p |
|---|---|---|
| Nodal status (N0 vs. N1) | 0.19 (0.07–0.47) | 0.0003 * |
| Grade (High vs. Low) | 3.92 (1.56–9.86) | 0.004 * |
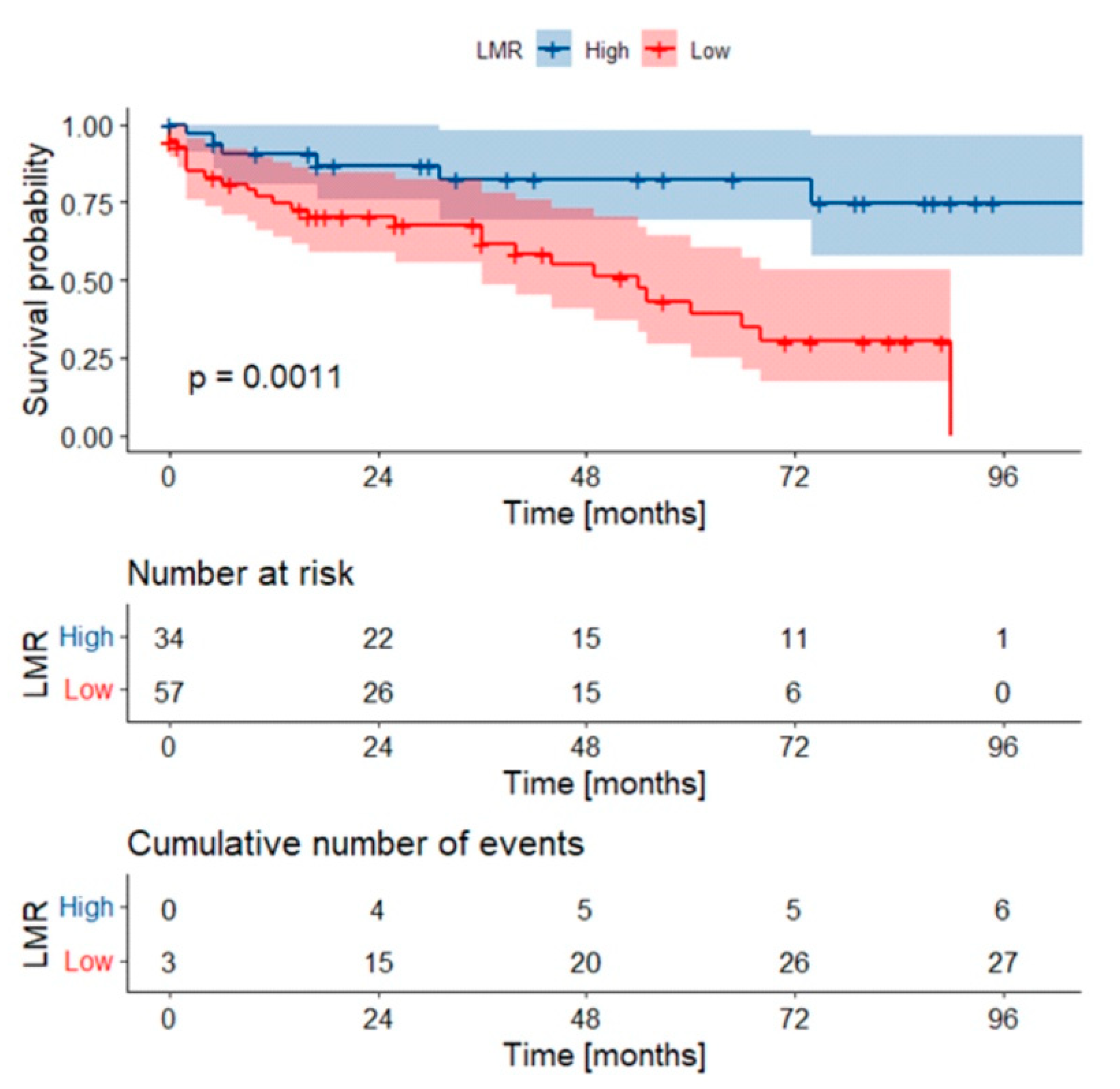
| LMR (High vs. low) | 0.20 (0.07–0.55) | 0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zapała, Ł.; Kunc, M.; Sharma, S.; Biernat, W.; Radziszewski, P. Low Lymphocyte-to-Monocyte Ratio Is the Potential Indicator of Worse Overall Survival in Patients with Renal Cell Carcinoma and Venous Tumor Thrombus. Diagnostics 2021, 11, 2159. https://doi.org/10.3390/diagnostics11112159
Zapała Ł, Kunc M, Sharma S, Biernat W, Radziszewski P. Low Lymphocyte-to-Monocyte Ratio Is the Potential Indicator of Worse Overall Survival in Patients with Renal Cell Carcinoma and Venous Tumor Thrombus. Diagnostics. 2021; 11(11):2159. https://doi.org/10.3390/diagnostics11112159
Chicago/Turabian StyleZapała, Łukasz, Michał Kunc, Sumit Sharma, Wojciech Biernat, and Piotr Radziszewski. 2021. "Low Lymphocyte-to-Monocyte Ratio Is the Potential Indicator of Worse Overall Survival in Patients with Renal Cell Carcinoma and Venous Tumor Thrombus" Diagnostics 11, no. 11: 2159. https://doi.org/10.3390/diagnostics11112159
APA StyleZapała, Ł., Kunc, M., Sharma, S., Biernat, W., & Radziszewski, P. (2021). Low Lymphocyte-to-Monocyte Ratio Is the Potential Indicator of Worse Overall Survival in Patients with Renal Cell Carcinoma and Venous Tumor Thrombus. Diagnostics, 11(11), 2159. https://doi.org/10.3390/diagnostics11112159