
Hysteroscopy as a Primary Tool in Exploration and Treatment of Infertility: Single Center Experience in Western Romania


 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Settings and Participants
2.2. Procedure
2.3. Variables
2.4. Data Sources
2.5. Bias
2.6. Statistical Methods
3. Results
3.1. Participants Characteristics
3.2. Hysteroscopic Finding among Infertile Women
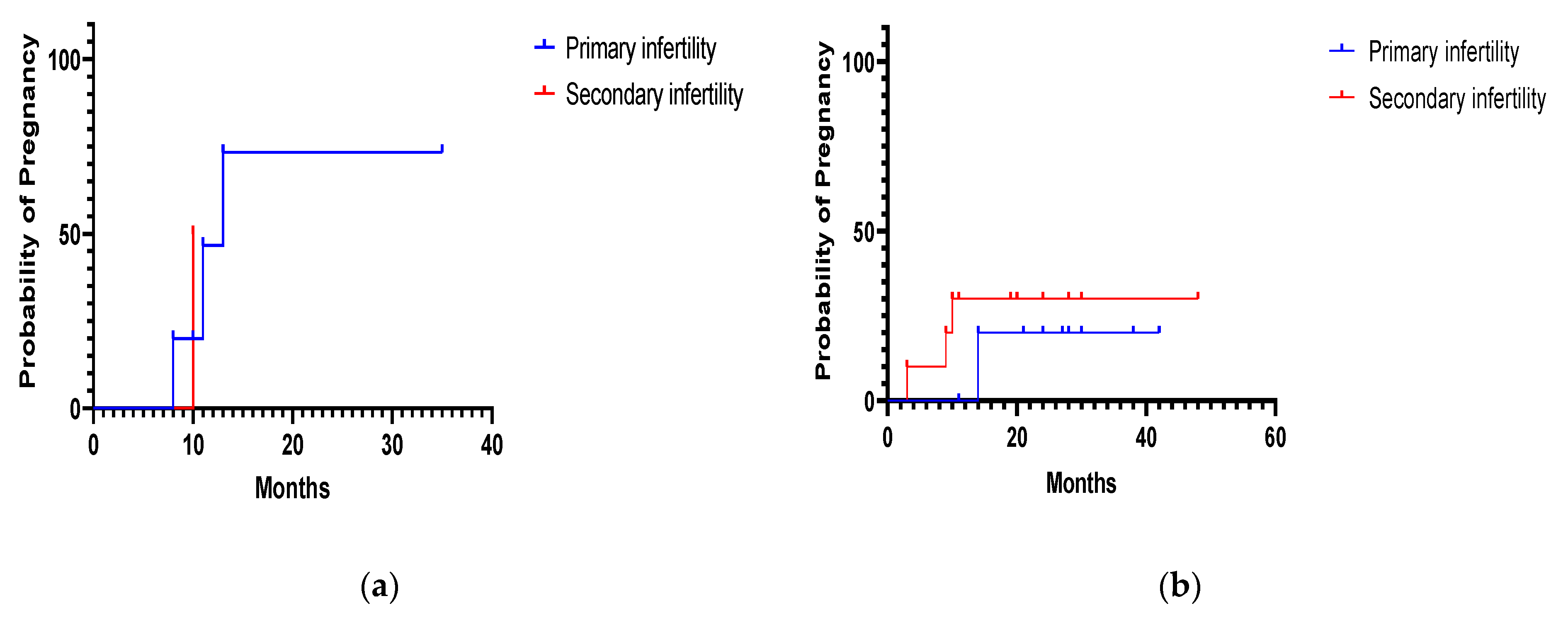
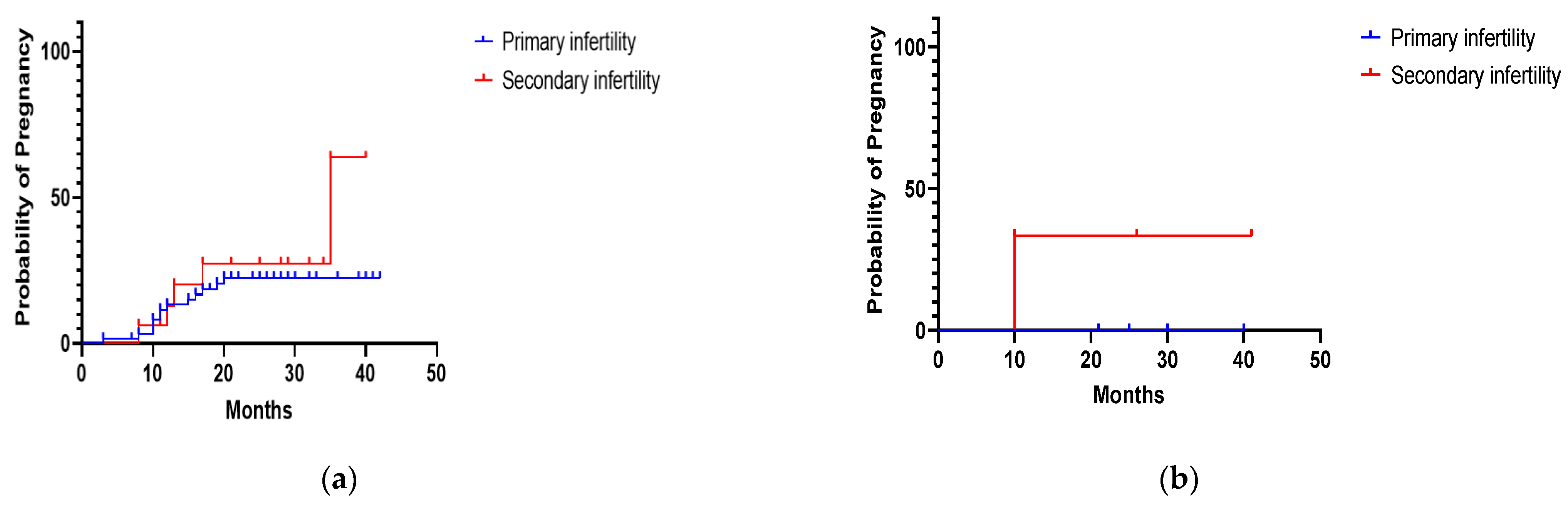
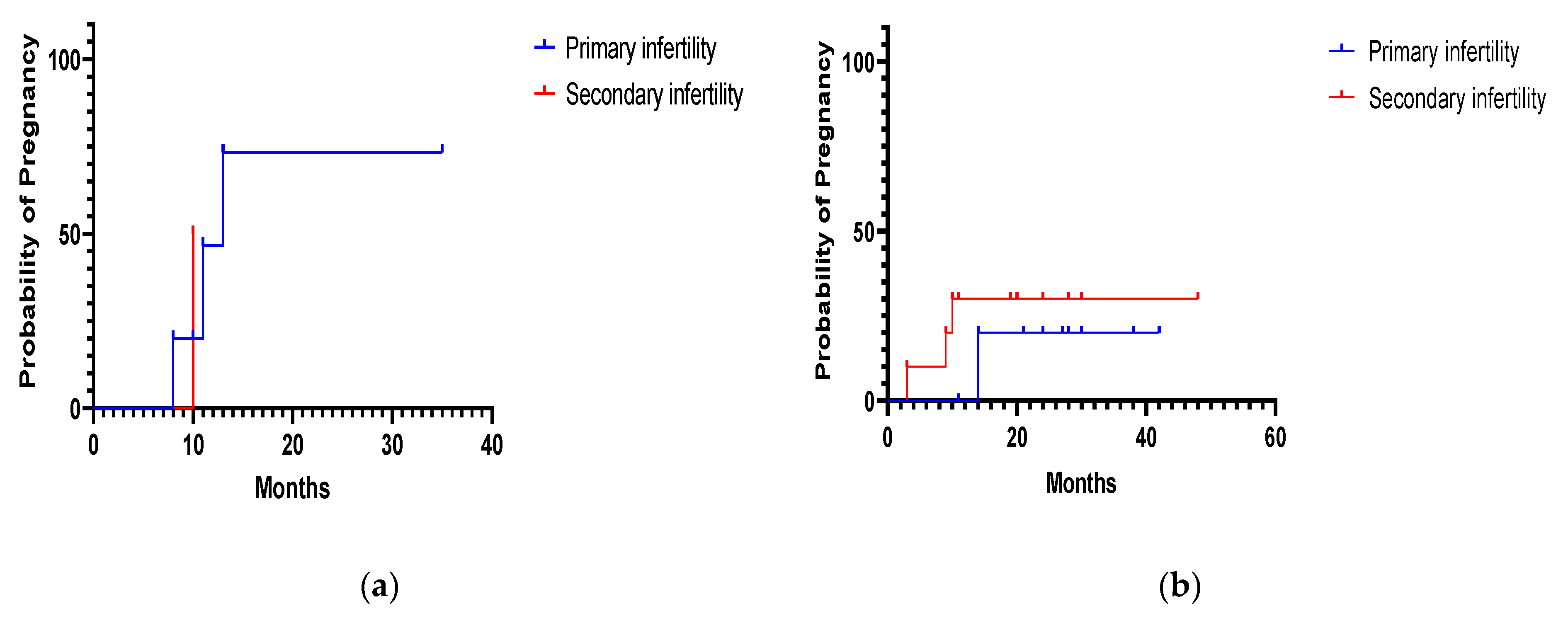
3.3. Fertility Outcomes after Operative Hysteroscopy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Infertility. Available online: https://www.who.int/news-room/fact-sheets/detail/infertility (accessed on 15 July 2021).
- Sun, H.; Gong, T.-T.; Jiang, Y.-T.; Zhang, S.; Zhao, Y.-H.; Wu, Q.-J. Global, Regional, and National Prevalence and Disability-Adjusted Life-Years for Infertility in 195 Countries and Territories, 1990–2017: Results from a Global Burden of Disease Study, 2017. Aging 2019, 11, 10952–10991. [Google Scholar] [CrossRef] [PubMed]
- Asociația pentru Reproducere Umană. Primul studiu de analiză a problemelor de infertilitate din România. Available online: https://www.arur.ro/2018/06/18/855/ (accessed on 31 August 2021).
- Ait Benkaddour, Y.; Gervaise, A.; Fernandez, H. Exploration de la cavité utérine dans le bilan d’infertilité: Quel examen choisir? J. Gynécologie Obs. Biol. Reprod. 2010, 39, 606–613. [Google Scholar] [CrossRef]
- The American College of Obstetricians and Gynecologists. Infertility Workup for the Women’s Health Specialist: ACOG Committee Opinion, Number 781. Obs. Gynecol. 2019, 133, e377–e384.
- Gupta, A.S.; Deshpande, P.S. Causes and prevalence of factors causing infertility in a public health facility. J. Hum. Reprod. Sci. 2019, 12, 287. [Google Scholar] [CrossRef] [PubMed]
- Farhi, J.; Ben-Haroush, A. Distribution of causes of infertility in patients attending primary fertility clinics in Israel. Isr. Med Assoc. J. 2011, 13, 51–54. [Google Scholar] [PubMed]
- Masoumi, S.Z.; Parsa, P.; Darvish, N.; Mokhtari, S.; Yavangi, M.; Roshanaei, G. An epidemiologic survey on the causes of infertility in patients referred to infertility center in Fatemieh Hospital in Hamadan. Iran. J. Reprod. Med. 2015, 13, 513–516. [Google Scholar] [PubMed]
- Allow, A.K. Distribution of Infertility Factors among Infertile Couples in Yemen. J. Clin. Dev. Biol. 2016, 1. [Google Scholar] [CrossRef] [Green Version]
- Pansky, M.; Feingold, M.; Sagi, R.; Herman, A.; Schneider, D.; Halperin, R. Diagnostic Hysteroscopy as a Primary Tool in a Basic Infertility Workup. JSLS J. Soc. Laparoendosc. Surg. 2006, 10, 231–235. [Google Scholar]
- Salim, S.; Won, H.; Nesbitt-Hawes, E.; Campbell, N.; Abbott, J. Diagnosis and Management of Endometrial Polyps: A Critical Review of the Literature. J. Minim. Invasive Gynecol. 2011, 18, 569–581. [Google Scholar] [CrossRef]
- Al Chami, A.; Saridogan, E. Endometrial Polyps and Subfertility. J. Obstet. Gynecol. India 2016, 67, 9–14. [Google Scholar] [CrossRef] [Green Version]
- Guo, X.C.; Segars, J.H. The Impact and Management of Fibroids for Fertility. Obstet. Gynecol. Clin. N. Am. 2012, 39, 521–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cook, H.; Ezzati, M.; Segars, J.H.; McCarthy, D. The impact of uterine leiomyomas on reproductive outcomes. Minerva Ginecol. 2010, 62, 225–236. [Google Scholar]
- Selvaraj, P.; Selvaraj, K. Reproductive outcome of septate uterus following hysteroscopic septum resection. J. Hum. Reprod. Sci. 2010, 3, 143–145. [Google Scholar] [CrossRef]
- Abuzeid, O.; LaChance, J.; Zaghmout, O.; Corrado, J.; Hebert, J.; Ashraf, M.; Abuzeid, M.I. The Role of Diagnostic Hysteroscopy in Diagnosis of Incomplete Uterine Septum/Significant Arcuate Uterine Anomaly in Infertile Patients in the Era of Trans-vaginal 3D Ultrasound Scan. Middle East Fertil. Soc. J. 2020, 25, 1. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, F.M.; Aguiar, F.N.; Tomioka, R.; de Oliveira, R.M.; Frantz, N.; Ueno, J. Functional endometrial polyps in infertile asymptomatic patients: A possible evolution of vascular changes secondary to endometritis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 170, 152–156. [Google Scholar] [CrossRef]
- Sardo, A.D.S.; Di Carlo, C.; Minozzi, S.; Spinelli, M.; Pistotti, V.; Alviggi, C.; DE Placido, G.; Nappi, C.; Bifulco, G. Efficacy of hysteroscopy in improving reproductive outcomes of infertile couples: A systematic review and meta-analysis. Hum. Reprod. Update 2016, 22, 479–496. [Google Scholar] [CrossRef]
- Shokeir, T.A.; Shalan, H.M.; El-Shafei, M.M. Significance of endometrial polyps detected hysteroscopically in eumenorrheic infertile women. J. Obstet. Gynaecol. Res. 2004, 30, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Varasteh, N.N.; Neuwirth, R.S.; Levin, B.; Keltz, M.D. Pregnancy Rates After Hysteroscopic Polypectomy and Myomectomy in Infertile Women. Obstet. Gynecol. 1999, 94, 168–171. [Google Scholar] [PubMed]
- Jee, B.C.; Jeong, H.G. Management of endometrial polyps in infertile women: A mini-review. Clin. Exp. Reprod. Med. 2021, 48, 198–202. [Google Scholar] [CrossRef]
- Donnez, J.; Jadoul, P. What are the implications of myomas on fertility? Hum. Reprod. 2002, 17, 1424–1430. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Hou, H.; Yu, Q. Fertility and Pregnancy Outcomes Following Hysteroscopic Metroplasty of Different Sized Uterine Septa: A Retrospective Cohort Study Protocol. Medicine 2019, 98, e16623. [Google Scholar] [CrossRef] [PubMed]
- Chua, S.J.; Danhof, N.A.; Mochtar, M.H.; Van Wely, M.; McLernon, D.; Custers, I.; Lee, E.; Dreyer, K.; Cahill, D.J.; Gillett, W.R.; et al. Age-related natural fertility outcomes in women over 35 years: A systematic review and individual participant data meta-analysis. Hum. Reprod. 2020, 35, 1808–1820. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.A.; Healy, D.; Black, D.; Sullivan, E.A. Age-Specific Success Rate for Women Undertaking Their First Assisted Re-production Technology Treatment Using Their Own Oocytes in Australia, 2002–2005. Hum. Reprod. 2008, 23, 1633–1638. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Primary Infertility (No. of Patients = 134) | Secondary Infertility (No. of Patients = 64) | |
|---|---|---|
| Median Age (Range) | 34 (23–47) | 34.5 (25–47) |
| Urban Area N/total (%; 95%CI) | 94/134 (70.1%; 61.9–77.2) | 42/64 (65.6%; 53.4–76.1) |
| Rural Area N/total (%; 95%CI) | 40/134 (29.9%; 22.8–38.1) | 22/64 (34.4%; 23.9–46.6) |
| Hysteroscopic Finding | Total No. (%; 95%CI) | Primary Infertility No. (%; 95%CI) | Secondary Infertility No. (%; 95%CI) | p Value OR (95%CI) |
|---|---|---|---|---|
| Normal uterine cavity | 73 (36.9%; 30.5–43.8) | 44 (22.2%; 17.0–28.5) | 29 (14.6%; 10.4–20.2) | p = 0.06 1.66 (1.00–2.77) |
| Endometrial Polyp | 78 (39.4%; 32.9–46.3) | 62 (31.3%; 25.3–38.1) | 16 (8.1%; 5.0–12.7) | p < 0.001 5.18 (2.92–9.26) |
| Uterine Septum | 7 (3.5%; 1.7–7.1) | 5 (2.5%; 1.1–5.8) | 2 (1.0%; 0.2–3.6) | p = 0.44 2.53 (0.53–12.87) |
| Uterine Synechiae | 21 (10.6%; 7.0–15.7) | 11 (5.6%; 3.1–9.7) | 10 (5.1%; 2.8–9.0) | p > 0.99 1.10 (0.47–2.65) |
| Uterine Fibroids | 9 (4.5%; 2.4–8.4) | 6 (3.0%; 1.4–6.5) | 3 (1.5%; 0.4–4.4) | p = 0.50 2.03 (0.51–7.48) |
| Endometrial Hyperplasia | 8 (4.0%; 2.1–7.8) | 6 (3.0%; 1.4–6.5) | 2 (1.0%; 0.2–3.6) | p = 0.28 3.06 (0.73–15.05) |
| Endometritis | 1 (0.5%; 0.02–2.8) | — | 1 (0.5%; 0.02–2.8) | NA |
| Retained placental tissue | 1 (0.5%; 0.02–2.8) | — | 1 (0.5%; 0.02–2.8) | NA |
| Total n/total (%; 95%CI) | Primary Infertility n/total (%; 95%CI) | Secondary Infertility n/total (%; 95%CI) | |
|---|---|---|---|
| After hysteroscopic polypectomy | |||
| Pregnancies | 18/78 (23.1%; 15.1–33.6) | 13/62 (21.0%; 12.7–32.6) | 5/16 (31.3%; 14.2–55.6) |
| Births | 17/78 (21.8%; 14.1–32.2) | 13/62 (21.0%; 12.7–32.6) | 4/16 (25.0%; 10.2–49.5) |
| Miscarriages | 1/78 (1.3%; 0.1–6.9) | — | 1/16 (6.3%; 0.3–28.3) |
| After hysteroscopic myomectomy | |||
| Pregnancies | 1/9 (11.1%; 0.6–43.5) | — | 1/3 (33.3%; 1.7–88.2) |
| Births | 1/9 (11.1%; 0.6–43.5) | — | — |
| Miscarriages | — | — | — |
| After metroplasty | |||
| Pregnancies | 3/7 (42.9%; 15.8–75.0) | 2/5 (40.0%; 7.1–76.9) | 1/2 (50.0%; 2.6–96.4) |
| Births | 2/7 (28.6%; 5.1–64.1) | 1/5 (20.0%; 1.0–62.4) | 1/2 (50.0%; 2.6–96.4) |
| Miscarriages | 1/7 (14.3%; 0.7–51.3) | 1/5 (20.0%; 1.0–62.4) | — |
| After synechiae resection | |||
| Pregnancies | 5/21 (23.8%; 10.6–45.1) | 2/11 (18.2%; 3.2–47.7) | 3/10 (30.0%; 10.8–60.3) |
| Births | 3/21 (14.3%; 5.0–34.6) | 2/11 (18.2%; 3.2–47.7) | 1/10 (10.0%; 0.5–40.4) |
| Miscarriages | 2/21 (9.5%; 1.7–28.9) | — | 2/10 (20.0%; 3.6–51.0) |
| After endometrial resection | |||
| Pregnancies | 4/8 (50.0%; 21.5–78.5) | 2/6 (33.3%; 5.9–70.0) | 2/2 (100%; 17.8–100) |
| Births | 2/8 (25.0%; 4.4–59.1) | 2/6 (33.3%; 5.9–70.0) | — |
| Miscarriages | 1/8 (12.5%; 0.6–47.1) | — | 1/2 (50.0; 2.6–97.4) |
| Ectopic pregnancy | 1/8 (12.5%; 0.6–47.1) | — | 1/2 (50.0; 2.6–97.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Citu, C.; Gorun, F.; Motoc, A.; Sas, I.; Gorun, O.M.; Burlea, B.; Serban, D.M.; Neamtu, R.; Citu, I.M. Hysteroscopy as a Primary Tool in Exploration and Treatment of Infertility: Single Center Experience in Western Romania. Diagnostics 2021, 11, 1917. https://doi.org/10.3390/diagnostics11101917
Citu C, Gorun F, Motoc A, Sas I, Gorun OM, Burlea B, Serban DM, Neamtu R, Citu IM. Hysteroscopy as a Primary Tool in Exploration and Treatment of Infertility: Single Center Experience in Western Romania. Diagnostics. 2021; 11(10):1917. https://doi.org/10.3390/diagnostics11101917
Chicago/Turabian StyleCitu, Cosmin, Florin Gorun, Andrei Motoc, Ioan Sas, Oana Maria Gorun, Bogdan Burlea, Denis Mihai Serban, Radu Neamtu, and Ioana Mihaela Citu. 2021. "Hysteroscopy as a Primary Tool in Exploration and Treatment of Infertility: Single Center Experience in Western Romania" Diagnostics 11, no. 10: 1917. https://doi.org/10.3390/diagnostics11101917
APA StyleCitu, C., Gorun, F., Motoc, A., Sas, I., Gorun, O. M., Burlea, B., Serban, D. M., Neamtu, R., & Citu, I. M. (2021). Hysteroscopy as a Primary Tool in Exploration and Treatment of Infertility: Single Center Experience in Western Romania. Diagnostics, 11(10), 1917. https://doi.org/10.3390/diagnostics11101917