
3D Automated Segmentation of Lower Leg Muscles Using Machine Learning on a Heterogeneous Dataset

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
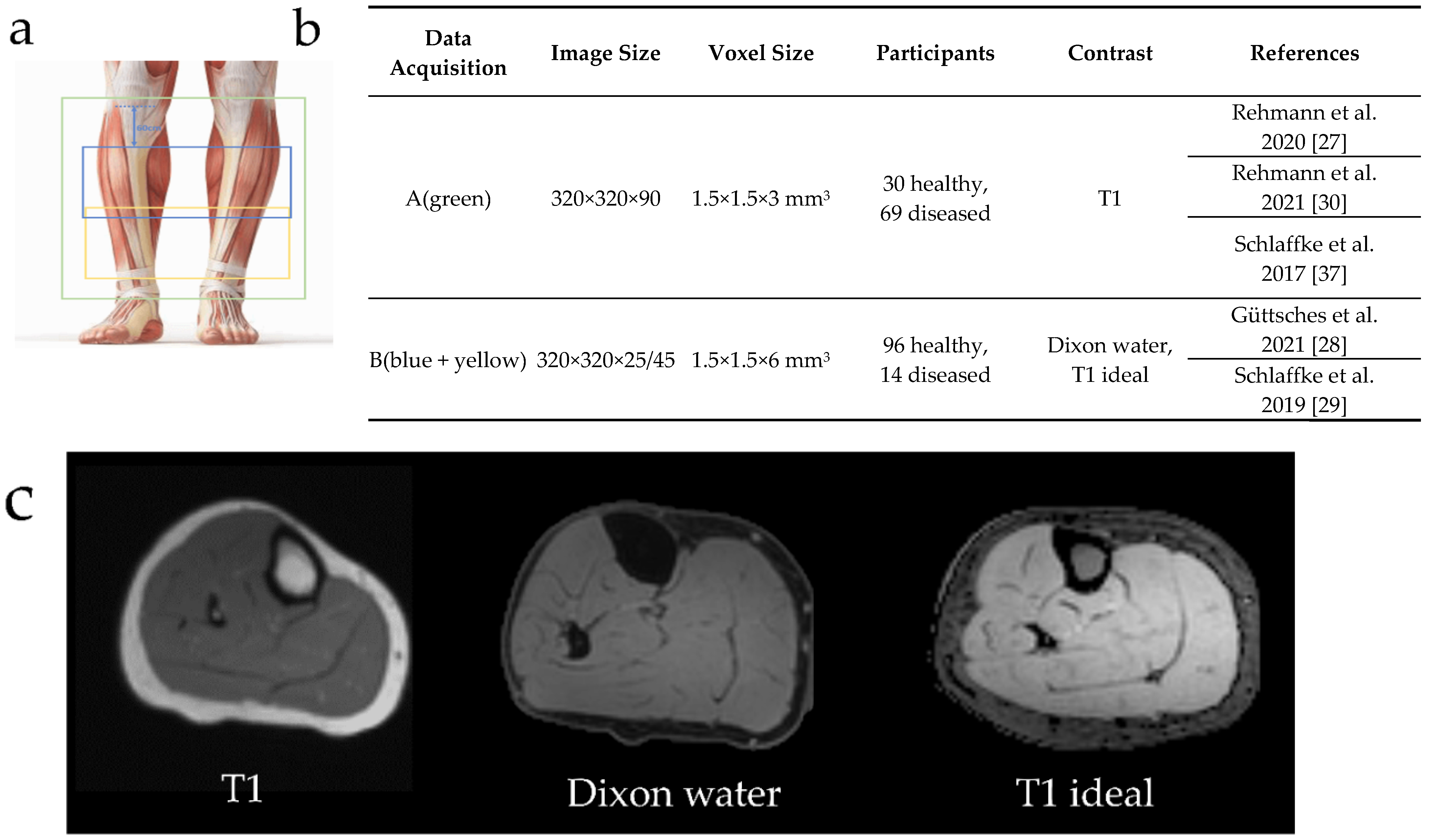
2.1. Datasets
2.2. Manual Segmentation
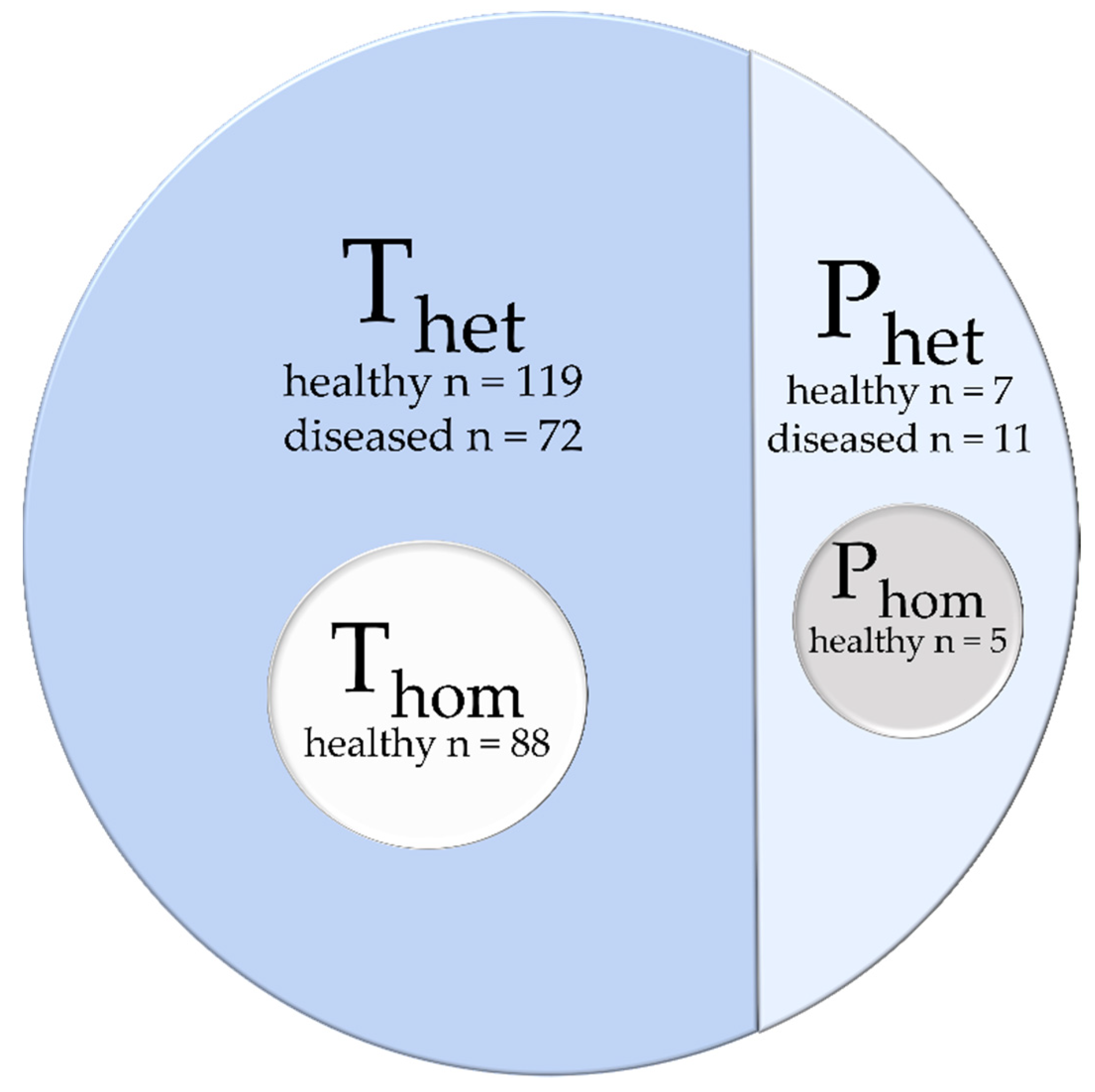
2.3. Data Selection and Composition
2.4. Preprocessing
2.5. Postprocessing
2.6. Convolutional Neuronal Networks
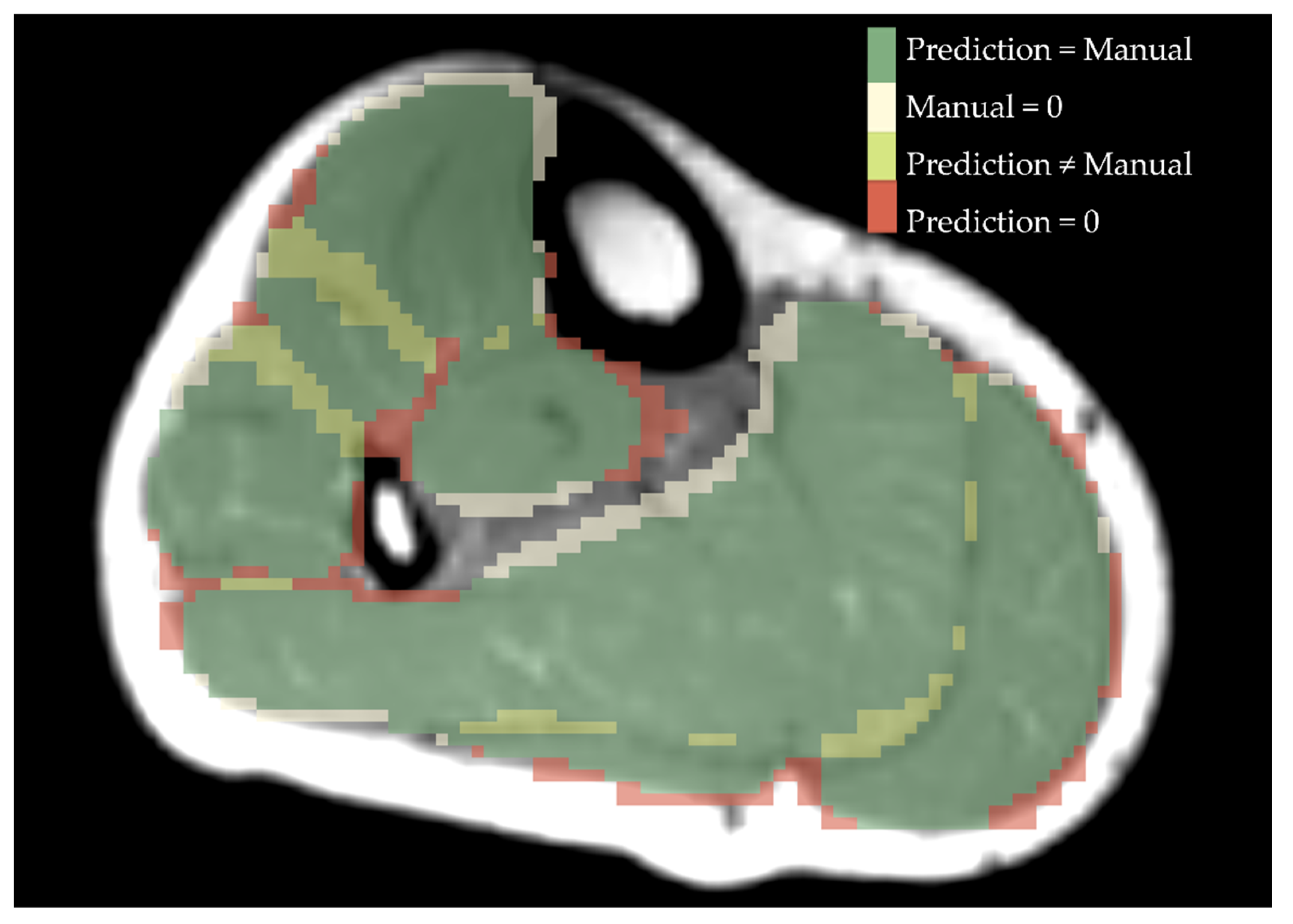
2.7. Evaluation
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Predicting Training | Dice Coefficient | Average Hausdorff Distance | ||||
|---|---|---|---|---|---|---|
| Homogeneous Phom Mean ± SD | Heterogeneous Phet Mean ± SD | Homogeneous Phom Mean ± SD | Heterogeneous Phet Mean ± SD | |||
| Homogeneous Thom | U-Net | GM | 0.92 ± 0.04 | 0.46 ± 0.36 | 0.14 ± 0.16 | 4.21 ± 4.21 |
| GL | 0.81 ± 0.15 | 0.34 ± 0.36 | 0.39 ± 0.49 | 5.26 ± 4.88 | ||
| SOL | 0.85 ± 0.12 | 0.48 ± 0.32 | 0.34 ± 0.44 | 3.47 ± 3.08 | ||
| TA | 0.90 ± 0.03 | 0.35 ± 0.41 | 0.15 ± 0.11 | 9.20 ± 8.03 | ||
| PER | 0.87 ± 0.06 | 0.38 ± 0.39 | 0.19 ± 0.14 | 8.69 ± 8.70 | ||
| EDL | 0.79 ± 0.04 | 0.31 ± 0.35 | 0.30 ± 0.11 | 8.96 ± 7.41 | ||
| TP | 0.85 ± 0.07 | 0.32 ± 0.41 | 0.31 ± 0.36 | 16.07 ± 13.89 | ||
| ResNet | GM | 0.91 ± 0.04 | 0.46 ± 0.34 | 0.13 ± 0.08 | 3.93 ± 3.10 | |
| GL | 0.77 ± 0.13 | 0.36 ± 0.33 | 0.66 ± 0.70 | 4.50 ± 3.99 | ||
| SOL | 0.84 ± 0.10 | 0.50 ± 0.30 | 0.39 ± 0.40 | 3.43 ± 3.25 | ||
| TA | 0.88 ± 0.05 | 0.34 ± 0.41 | 0.25 ± 0.27 | 10.68 ± 9.00 | ||
| PER | 0.84 ± 0.09 | 0.39 ± 0.35 | 0.31 ± 0.32 | 5.12 ± 4.09 | ||
| EDL | 0.77 ± 0.07 | 0.28 ± 0.36 | 0.36 ± 0.16 | 12.60 ± 10.56 | ||
| TP | 0.83 ± 0.05 | 0.33 ± 0.40 | 0.32 ± 0.30 | 10.39 ± 8.64 | ||
| DenseNet | GM | 0.77 ± 0.13 | 0.31 ± 0.34 | 0.75 ± 0.66 | 5.87 ± 4.27 | |
| GL | 0.71 ± 0.16 | 0.27 ± 0.33 | 0.89 ± 0.58 | 11.17 ± 11.47 | ||
| SOL | 0.78 ± 0.12 | 0.33 ± 0.36 | 0.70 ± 0.45 | 8.42 ± 7.78 | ||
| TA | 0.84 ± 0.07 | 0.30 ± 0.39 | 0.24 ± 0.12 | 19.01 ± 15.56 | ||
| PER | 0.72 ± 0.14 | 0.29 ± 0.31 | 1.11 ± 1.22 | 7.97 ± 5.50 | ||
| EDL | 0.68 ± 0.10 | 0.23 ± 0.32 | 0.69 ± 0.38 | 15.24 ± 12.65 | ||
| TP | 0.80 ± 0.08 | 0.29 ± 0.38 | 0.26 ± 0.11 | 17.75 ± 15.53 | ||
| Heterogeneous Thet | U-Net | GM | 0.92 ± 0.04 | 0.83 ± 0.12 | 0.11 ± 0.08 | 0.42 ± 0.60 |
| GL | 0.78 ± 0.18 | 0.73 ± 0.14 | 0.41 ± 0.45 | 0.60 ± 0.40 | ||
| SOL | 0.84 ± 0.13 | 0.83 ± 0.08 | 0.40 ± 0.52 | 0.40 ± 0.35 | ||
| TA | 0.90 ± 0.04 | 0.85 ± 0.06 | 0.15 ± 0.10 | 0.25 ± 0.17 | ||
| PER | 0.87 ± 0.08 | 0.82 ± 0.08 | 0.21 ± 0.20 | 0.34 ± 0.30 | ||
| EDL | 0.77 ± 0.08 | 0.75 ± 0.10 | 0.36 ± 0.08 | 0.45 ± 0.35 | ||
| TP | 0.86 ± 0.05 | 0.80 ± 0.06 | 0.19 ± 0.10 | 0.31 ± 0.41 | ||
| ResNet | GM | 0.92 ± 0.04 | 0.83 ± 0.10 | 0.16 ± 0.17 | 0.49 ± 0.44 | |
| GL | 0.83 ± 0.10 | 0.73 ± 0.12 | 0.32 ± 0.28 | 0.66 ± 0.44 | ||
| SOL | 0.85 ± 0.10 | 0.83 ± 0.07 | 0.33 ± 0.39 | 0.36 ± 0.25 | ||
| TA | 0.90 ± 0.03 | 0.84 ± 0.05 | 0.16 ± 0.13 | 0.26 ± 0.15 | ||
| PER | 0.86 ± 0.08 | 0.80 ± 0.09 | 0.30 ± 0.33 | 0.41 ± 0.35 | ||
| EDL | 0.79 ± 0.06 | 0.73 ± 0.10 | 0.38 ± 0.24 | 0.52 ± 0.38 | ||
| TP | 0.85 ± 0.03 | 0.79 ± 0.08 | 0.18 ± 0.06 | 0.34 ± 0.25 | ||
| DenseNet | GM | 0.91 ± 0.03 | 0.83 ± 0.10 | 0.16 ± 0.14 | 0.44 ± 0.44 | |
| GL | 0.87 ± 0.06 | 0.78 ± 0.11 | 0.22 ± 0.15 | 0.59 ± 0.55 | ||
| SOL | 0.86 ± 0.08 | 0.85 ± 0.07 | 0.35 ± 0.42 | 0.36 ± 0.32 | ||
| TA | 0.89 ± 0.05 | 0.85 ± 0.07 | 0.22 ± 0.30 | 0.30 ± 0.25 | ||
| PER | 0.87 ± 0.07 | 0.82 ± 0.07 | 0.26 ± 0.32 | 0.33 ± 0.25 | ||
| EDL | 0.78 ± 0.06 | 0.75 ± 0.10 | 0.40 ± 0.27 | 0.55 ± 0.53 | ||
| TP | 0.86 ± 0.03 | 0.81 ± 0.84 | 0.17 ± 0.04 | 0.31 ± 0.18 | ||
References
- Díaz-Manera, J.; Llauger, J.; Gallardo, E.; Illa, I. Muscle MRI in muscular dystrophies. Acta Myol. 2015, 34, 95–108. [Google Scholar]
- Alic, L.; Griffin, J.F.; Eresen, A.; Kornegay, J.N.; Ji, J.X. Using MRI to quantify skeletal muscle pathology in Duchenne muscular dystrophy: A systematic mapping review. Muscle Nerve 2021, 64, 8–22. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Manera, J.; Walter, G.; Straub, V. Skeletal muscle magnetic resonance imaging in Pompe disease. Muscle Nerve 2021, 63, 640–650. [Google Scholar] [CrossRef] [PubMed]
- Wattjes, M.P.; Kley, R.A.; Fischer, D. Neuromuscular imaging in inherited muscle diseases. Eur. Radiol. 2010, 20, 2447–2460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bas, J.; Ogier, A.C.; Le Troter, A.; Delmont, E.; Leporq, B.; Pini, L.; Guye, M.; Parlanti, A.; Lefebvre, M.-N.; Bendahan, D.; et al. Fat fraction distribution in lower limb muscles of patients with CMT1A. Neurology 2020, 94, e1480–e1487. [Google Scholar] [CrossRef]
- Pons, C.; Borotikar, B.; Garetier, M.; Burdin, V.; BEN Salem, D.; Lempereur, M.; Brochard, S. Quantifying skeletal muscle volume and shape in humans using MRI: A systematic review of validity and reliability. PLoS ONE 2018, 13, e0207847. [Google Scholar] [CrossRef] [PubMed]
- Ogier, A.C.; Hostin, M.-A.; Bellemare, M.-E.; Bendahan, D. Overview of MR Image Segmentation Strategies in Neuromuscular Disorders. Front. Neurol. 2021, 12, 255. [Google Scholar] [CrossRef]
- Baudin, P.Y.; Azzabou, N.; Carlier, P.G.; Paragios, N. Prior knowledge, random walks and human skeletal muscle segmentation. Med. Image Comput. Comput. Assist. Interv. 2012, 7510, 569–576. [Google Scholar] [CrossRef] [Green Version]
- Andrews, S.; Hamarneh, G. The Generalized Log-Ratio Transformation: Learning Shape and Adjacency Priors for Simultaneous Thigh Muscle Segmentation. IEEE Trans. Med. Imaging 2015, 34, 1773–1787. [Google Scholar] [CrossRef] [Green Version]
- Shakya, S.R.; Zhang, C.; Zhou, Z. Comparative study of machine learning and deep learning architecture for human activity recognition using accelerometer data. Int. J. Mach. Learn. Comput. 2018, 8, 577–582. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Cham, Switzerland, 2015; pp. 234–241. [Google Scholar] [CrossRef] [Green Version]
- Oukil, S.; Kasmi, R.; Mokrani, K. U-Net and K-Means for Dermoscopic Skin Lesion Images: Segmentation and Comparison. In Soft Computing and Electrical Engineering; Springer: Cham, Switzerland, 2020; Volume 2. [Google Scholar]
- Hänsch, A.; Schwier, M.; Gass, T.; Morgas, T.; Haas, B.; Dicken, V.; Meine, H.; Klein, J.; Hahn, H.K. Evaluation of deep learning methods for parotid gland segmentation from CT images. J. Med. Imaging 2018, 6, 011005. [Google Scholar] [CrossRef] [PubMed]
- Tong, G.; Li, Y.; Chen, H.; Zhang, Q.; Jiang, H. Improved U-NET network for pulmonary nodules segmentation. Optik 2018, 174, 460–469. [Google Scholar] [CrossRef]
- Qamar, S.; Jin, H.; Zheng, R.; Ahmad, P.; Usama, M. A variant form of 3D-UNet for infant brain segmentation. Futur. Gener. Comput. Syst. 2020, 108, 613–623. [Google Scholar] [CrossRef]
- Zhuang, X.; Xu, J.; Luo, X.; Chen, C.; Ouyang, C.; Rueckert, D.; Campello, V.M.; Lekadir, K.; Vesal, S.; RaviKumar, N.; et al. Cardiac Segmentation on Late Gadolinium Enhancement MRI: A Benchmark Study from Multi-Sequence Cardiac MR Seg-mentation Challenge. arXiv 2020, arXiv:2006.12434. [Google Scholar]
- Long, F. Microscopy cell nuclei segmentation with enhanced U-Net. BMC Bioinform. 2020, 21, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Veit, A.; Wilber, M.; Belongie, S. Residual Networks Behave Like Ensembles of Relatively Shallow Networks. arXiv 2016, arXiv:1605.06431. [Google Scholar]
- He, F.; Liu, T.; Tao, D. Why ResNet Works? Residuals Generalize. IEEE Trans. Neural Netw. Learn. Syst. 2020, 31, 5349–5362. [Google Scholar] [CrossRef] [Green Version]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition; IEEE Computer Society: Tapei, Taiwan, 2015; pp. 770–778. [Google Scholar] [CrossRef] [Green Version]
- Drozdzal, M.; Vorontsov, E.; Chartrand, G.; Kadoury, S.; Pal, C. The Importance of Skip Connections in Biomedical Image Segmentation. In Proceedings of the Lecture Notes in Computer Science (Including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); Springer: Cham, Switzerland, 2016; Volume 10008, pp. 179–187. [Google Scholar]
- Lin, B.; Xle, J.; Li, C.; Qu, Y. Deeptongue: Tongue Segmentation Via Resnet. In Proceedings of the 2018 IEEE International Conference on Acoustics, Speech and Signal Processing—Proceedings, Calgary, AB, Canada, 15 April 2018; Institute of Electrical and Electronics Engineers, 2018; pp. 1035–1039. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely Connected Convolutional Networks. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2016; IEEE: New York, NY, USA, 2016; pp. 2261–2269. [Google Scholar] [CrossRef] [Green Version]
- Jegou, S.; Drozdzal, M.; Vazquez, D.; Romero, A.; Bengio, Y. The one hundred layers tiramisu: Fully convolutional DenseNets for semantic segmentation. In Proceedings of the IEEE Computer Society Conference on Computer Vision and Pattern Recognition Workshops, Honolulu, HI, USA, 21–26 July 2017; pp. 1175–1183. [Google Scholar]
- Stawiaski, J. pretrained densenet encoder for brain tumor segmentation. In Proceedings of the Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); Springer: Cham, Switzerland, 2019; Volume 11384, pp. 105–115. [Google Scholar]
- Forsting, J.; Rehmann, R.; Froeling, M.; Vorgerd, M.; Tegenthoff, M.; Schlaffke, L. Diffusion tensor imaging of the human thigh: Consideration of DTI-based fiber tracking stop criteria. Magma Magn. Reson. Mater. Phys. Biol. Med. 2020, 33, 343–355. [Google Scholar] [CrossRef]
- Rehmann, R.; Froeling, M.; Rohm, M.; Forsting, J.; Kley, R.A.; Schmidt-Wilcke, T.; Karabul, N.; Meyer-Frießem, C.H.; Vollert, J.; Tegenthoff, M.; et al. Diffusion tensor imaging reveals changes in non-fat infiltrated muscles in late onset Pompe disease. Muscle Nerve 2020, 62, 541–549. [Google Scholar] [CrossRef]
- Güttsches, A.-K.; Rehmann, R.; Schreiner, A.; Rohm, M.; Forsting, J.; Froeling, M.; Tegenthoff, M.; Vorgerd, M.; Schlaffke, L. Quantitative Muscle-MRI Correlates with Histopathology in Skeletal Muscle Biopsies. J. Neuromuscul. Dis. 2021, 8, 669–678. [Google Scholar] [CrossRef]
- Schlaffke, L.; Rehmann, R.; Rohm, M.; Otto, L.A.; De Luca, A.; Burakiewicz, J.; Baligand, C.; Monte, J.; Harder, C.D.; Hooijmans, M.T.; et al. Multi-center evaluation of stability and reproducibility of quantitative MRI measures in healthy calf muscles. NMR Biomed. 2019, 32, e4119. [Google Scholar] [CrossRef] [PubMed]
- Rehmann, R.; Schneider-Gold, C.; Froeling, M.; Güttsches, A.; Rohm, M.; Forsting, J.; Vorgerd, M.; Schlaffke, L. Diffusion Tensor Imaging Shows Differences Between Myotonic Dystrophy Type 1 and Type 2. J. Neuromuscul. Dis. 2021, Pre-press, 1–14. [Google Scholar] [CrossRef]
- Çiçek, Ö. 3D U-Net: Learning Dense Volumetric Segmentation from Sparse Annotation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Cambridge, UK, 19–22 September 1999; Springer: Cham, Switzerland, 2016; pp. 424–432. [Google Scholar]
- Taha, A.A.; Hanbury, A. Metrics for evaluating 3D medical image segmentation: Analysis, selection, and tool. BMC Med. Imaging 2015, 15, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, Z.; Zhang, H.; Chen, Z.; van der Plas, E.; Gutmann, L.; Thedens, D.; Nopoulos, P.; Sonka, M. Fully automated 3D segmentation of MR-imaged calf muscle compartments: Neighborhood relationship enhanced fully convolutional network. Comput. Med. Imaging Graph. 2021, 87, 101835. [Google Scholar] [CrossRef] [PubMed]
- Dam, L.T.; Van Der Kooi, A.J.; Verhamme, C.; Wattjes, M.P.; De Visser, M. Muscle imaging in inherited and acquired muscle diseases. Eur. J. Neurol. 2016, 23, 688–703. [Google Scholar] [CrossRef]
- Degardin, A.; Morillon, D.; Lacour, A.; Cotten, A.; Vermersch, P.; Stojkovic, T. Morphologic imaging in muscular dystrophies and inflammatory myopathies. Skelet. Radiol. 2010, 39, 1219–1227. [Google Scholar] [CrossRef]
- Secondulfo, L.; Ogier, A.C.; Monte, J.R.; Aengevaeren, V.L.; Bendahan, D.; Nederveen, A.J.; Strijkers, G.J.; Hooijmans, M.T. Supervised segmentation framework for evaluation of diffusion tensor imaging indices in skeletal muscle. NMR Biomed. 2021, 34, e4406. [Google Scholar] [CrossRef]
- Schlaffke, L.; Rehmann, R.; Froeling, M.; Kley, R.; Tegenthoff, M.; Vorgerd, M.; Schmidt-Wilcke, T. Diffusion tensor imaging of the human calf: Variation of inter- and intramuscle-specific diffusion parameters. J. Magn. Reson. Imaging 2017, 46, 1137–1148. [Google Scholar] [CrossRef] [PubMed]



| Predicting Training | Dice Score | Average Hausdorff Distance | |||||||||||
| Homogeneous Phom | Heterogeneous Phet | Homogeneous Phom | Heterogeneous Phet | ||||||||||
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | ||||||||||
| Homogeneous Thom | U-Net | 0.86 | ± | 0.07 | 0.38 | ± | 0.36 | 0.26 | ± | 0.25 | 7.98 | ± | 6.57 |
| ResNet | 0.83 | ± | 0.07 | 0.38 | ± | 0.35 | 0.35 | ± | 0.29 | 7.24 | ± | 5.67 | |
| DenseNet | 0.76 | ± | 0.09 | 0.29 | ± | 0.34 | 0.66 | ± | 0.39 | 12.2 | ± | 9.60 | |
| Heterogeneous Thet | U-Net | 0.85 | ± | 0.08 | 0.80 | ± | 0.10 | 0.26 | ± | 0.23 | 0.39 | ± | 0.37 |
| ResNet | 0.86 | ± | 0.06 | 0.79 | ± | 0.10 | 0.26 | ± | 0.22 | 0.43 | ± | 0.35 | |
| DenseNet | 0.86 | ± | 0.05 | 0.81 | ± | 0.09 | 0.25 | ± | 0.21 | 0.41 | ± | 0.40 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rohm, M.; Markmann, M.; Forsting, J.; Rehmann, R.; Froeling, M.; Schlaffke, L. 3D Automated Segmentation of Lower Leg Muscles Using Machine Learning on a Heterogeneous Dataset. Diagnostics 2021, 11, 1747. https://doi.org/10.3390/diagnostics11101747
Rohm M, Markmann M, Forsting J, Rehmann R, Froeling M, Schlaffke L. 3D Automated Segmentation of Lower Leg Muscles Using Machine Learning on a Heterogeneous Dataset. Diagnostics. 2021; 11(10):1747. https://doi.org/10.3390/diagnostics11101747
Chicago/Turabian StyleRohm, Marlena, Marius Markmann, Johannes Forsting, Robert Rehmann, Martijn Froeling, and Lara Schlaffke. 2021. "3D Automated Segmentation of Lower Leg Muscles Using Machine Learning on a Heterogeneous Dataset" Diagnostics 11, no. 10: 1747. https://doi.org/10.3390/diagnostics11101747
APA StyleRohm, M., Markmann, M., Forsting, J., Rehmann, R., Froeling, M., & Schlaffke, L. (2021). 3D Automated Segmentation of Lower Leg Muscles Using Machine Learning on a Heterogeneous Dataset. Diagnostics, 11(10), 1747. https://doi.org/10.3390/diagnostics11101747