
Gold Nanoparticle Approach to the Selective Delivery of Gene Silencing in Cancer—The Case for Combined Delivery?




Abstract
:1. Gene Therapy in Cancer Therapeutics
Cancer-Related Targets for Gene Silencing
2. Addressing Current Drawbacks in Gene Silencing Therapy—Focus on Nanomedicine
2.1. Nanomedicine Applied to Gene Therapy
2.2. Gold Nanoparticles Applied to Gene-Silencing Therapeutics
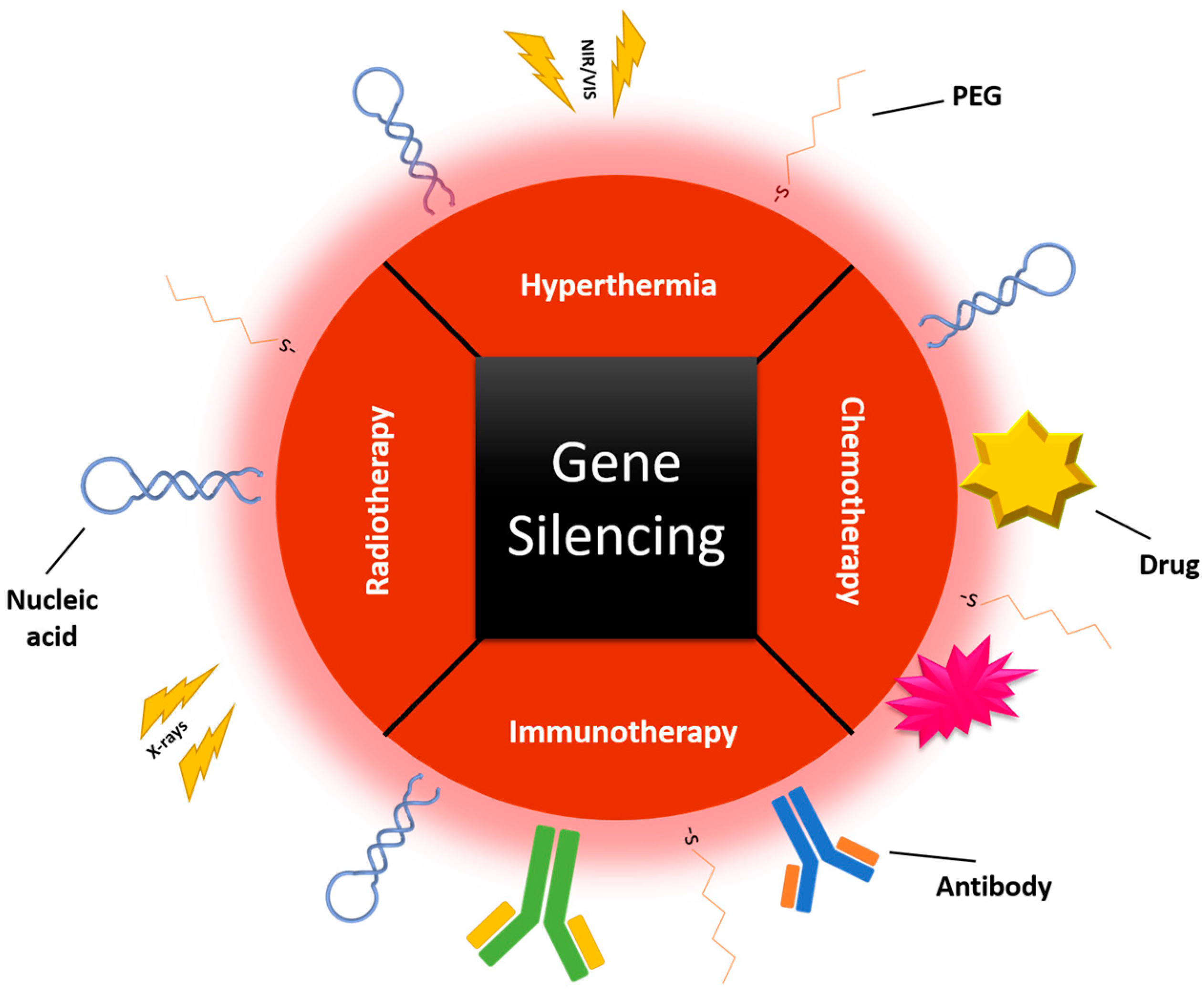
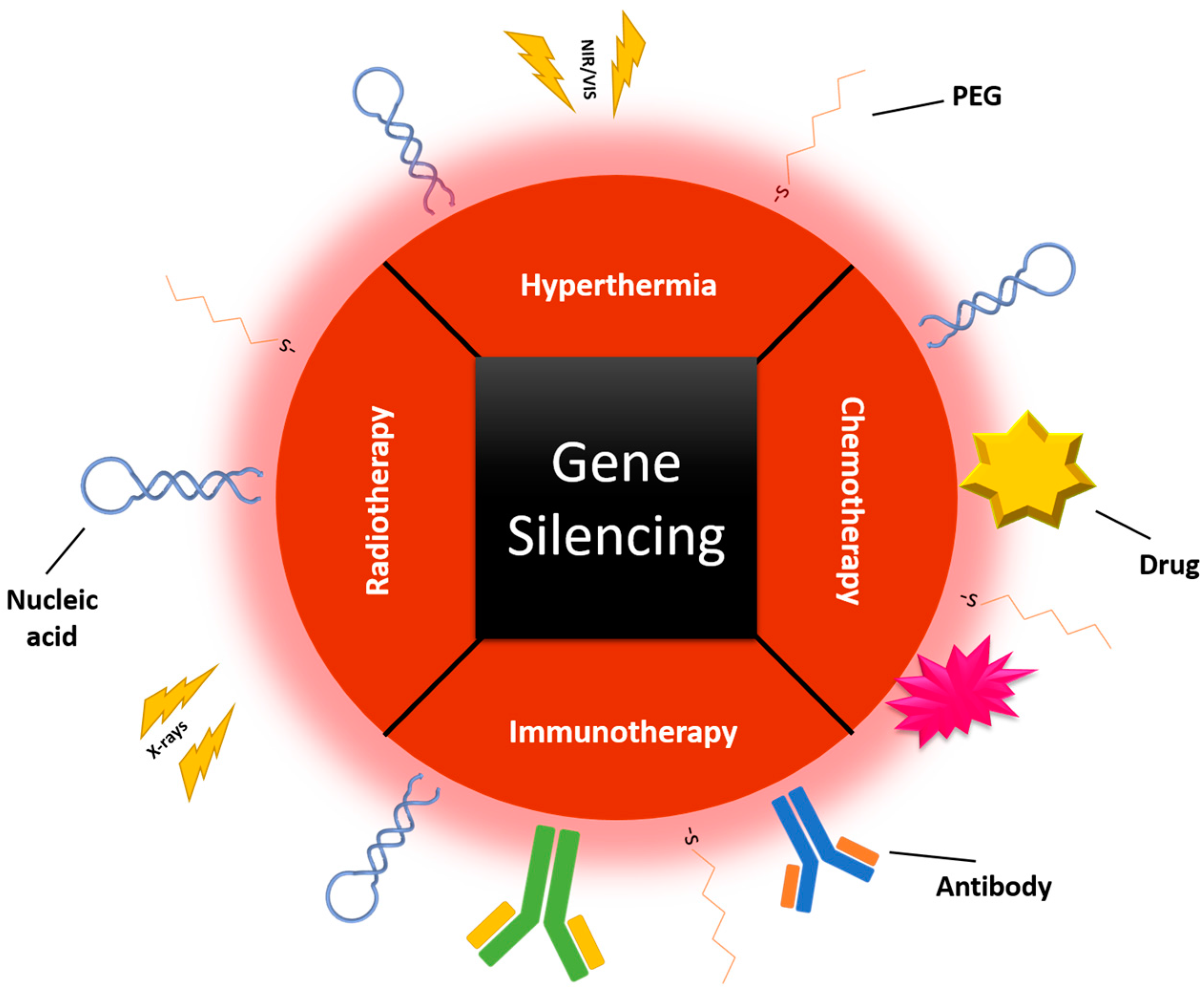
3. Combinatory Approaches
3.1. Gene Silencing–Gene Silencing
3.2. Gene Silencing–Chemotherapy
3.3. Gene Silencing–Light Induced Therapeutics
3.4. Gene Silencing–Radiotherapy
3.5. Gene Silencing–Immunotherapy
4. Translation to the Clinics
Acknowledgments
Conflicts of Interest
References
- Deng, Y.; Wang, C.C.; Choy, K.W.; Du, Q.; Chen, J.; Wang, Q.; Li, L.; Chung, T.K.H.; Tang, T. Therapeutic potentials of gene silencing by RNA interference: Principles, challenges, and new strategies. Gene 2014, 538, 217–227. [Google Scholar] [CrossRef] [PubMed]
- WHO: World Health Organization. Available online: http://www.who.int/en/ (accessed on 23 August 2016).
- Duarte, S.; Carle, G.; Faneca, H.; de Lima, M.C.P.; Pierrefite-Carle, V. Suicide gene therapy in cancer: Where do we stand now? Cancer Lett. 2012, 324, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Bertram, J.S. The molecular biology of cancer. Mol. Asp. Med. 2001, 21, 167–223. [Google Scholar] [CrossRef]
- Song, C.-Z. Gene Silencing Therapy Against Cancer. In Cancer Drug Discovery and Development: Gene Therapy for Cancer; Hunt, K.K., Vorburger, S.A., Swisher, S.G., Eds.; Humana Press: Totowa, NJ, USA, 2007; pp. 185–196. [Google Scholar]
- Guo, W.; Chen, W.; Yu, W.; Huang, W.; Deng, W. Small interfering RNA-based molecular therapy of cancers. Chin. J. Cancer 2013, 32, 488–493. [Google Scholar] [CrossRef] [PubMed]
- Li, S.-D.; Chono, S.; Huang, L. Efficient oncogene silencing and metastasis inhibition via systemic delivery of siRNA. Mol. Ther. 2008, 16, 942–946. [Google Scholar] [CrossRef] [PubMed]
- Fujita, Y.; Kuwano, K.; Ochiya, T. Development of small RNA delivery systems for lung cancer therapy. Int. J. Mol. Sci. 2015, 16, 5254–5270. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Wang, J. Delivery systems for siRNA drug development in cancer therapy. Asian J. Pharm. Sci. 2015, 10, 1–12. [Google Scholar] [CrossRef]
- Mendes, R.; Carreira, B.; Baptista, P.V.; Fernandes, A.R. Non-small cell lung cancer biomarkers and targeted therapy—Two faces of the same coin fostered by nanotechnology. Expert Rev. Precis. Med. Drug Dev. 2016, 1, 155–168. [Google Scholar] [CrossRef]
- Jonas, S.; Izaurralde, E. Towards a molecular understanding of microRNA-mediated gene silencing. Nat. Rev. Genet. 2015, 16, 421–433. [Google Scholar] [CrossRef] [PubMed]
- Song, N.; Wang, Y.; Gu, X.; Chen, Z.; Shi, L. Effect of siRNA-mediated knockdown of EIF3C gene on the survival of colon cancer cells. J. Zhejiang Univ. Sci. B 2013, 14, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Zeng, L.; Li, J.; Wang, Y.; Qian, C.; Chen, Y.; Zhang, Q.; Wu, W.; Lin, Z.; Liang, J.; Shuai, X.; et al. Combination of siRNA-directed Kras oncogene silencing and arsenic-induced apoptosis using a nanomedicine strategy for the effective treatment of pancreatic cancer. Nanomed. Nanotechnol. Biol. Med. 2014, 10, 463–472. [Google Scholar] [CrossRef] [PubMed]
- Verreault, M.; Webb, M.S.; Ramsay, E.C.; Bally, M.B. Gene silencing in the development of personalized cancer treatment: The targets, the agents and the delivery systems. Curr. Gene Ther. 2006, 6, 505–533. [Google Scholar] [CrossRef] [PubMed]
- Conde, J.; Rosa, J.; de la Fuente, J.M.; Baptista, P.V. Gold-nanobeacons for simultaneous gene specific silencing and intracellular tracking of the silencing events. Biomaterials 2013, 34, 2516–2523. [Google Scholar] [CrossRef] [PubMed]
- Moghimi, S.M.; Farhangrazi, Z.S. Nanomedicine and the complement paradigm. Nanomed. Nanotechnol. Biol. Med. 2013, 9, 458–460. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Ho, W.; Zhang, X.; Bertrand, N.; Farokhzad, O. Cancer nanomedicine: From targeted delivery to combination therapy. Trends Mol. Med. 2015, 21, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Hirst, D.G.; O’Sullivan, J.M. Gold nanoparticles as novel agents for cancer therapy. Br. J. Radiol. 2012, 85, 101–113. [Google Scholar] [CrossRef] [PubMed]
- Conde, J. The Golden Age in Cancer Nanobiotechnology: Quo Vadis? Front. Bioeng. Biotechnol. 2015, 3, 142. [Google Scholar] [CrossRef] [PubMed]
- Parveen, S.; Misra, R.; Sahoo, S.K. Nanoparticles: A boon to drug delivery, therapeutics, diagnostics and imaging. Nanomed. Nanotechnol. Biol. Med. 2012, 8, 147–166. [Google Scholar] [CrossRef] [PubMed]
- Pedrosa, P.; Vinhas, R.; Fernandes, A.; Baptista, P. Gold Nanotheranostics: Proof-of-Concept or Clinical Tool? Nanomaterials 2015, 5, 1853–1879. [Google Scholar] [CrossRef]
- Kong, L.; Wu, Y.; Alves, C.S.; Shi, X. Efficient delivery of therapeutic siRNA into glioblastoma cells using multifunctional dendrimer-entrapped gold nanoparticles. Nanomedicine 2016, 11, 3103–3115. [Google Scholar] [CrossRef] [PubMed]
- Hou, W.; Wei, P.; Kong, L.; Guo, R.; Wang, S.; Shi, X. Partially PEGylated dendrimer-entrapped gold nanoparticles: A promising nanoplatform for highly efficient DNA and siRNA delivery. J. Mater. Chem. B 2016, 4, 2933–2943. [Google Scholar] [CrossRef]
- Egusquiaguirre, S.P.; Igartua, M.; Hernández, R.M.; Pedraz, J.L. Nanoparticle delivery systems for cancer therapy: Advances in clinical and preclinical research. Clin. Transl. Oncol. 2012, 14, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Ajnai, G.; Chiu, A.; Kan, T.; Cheng, C.; Tsai, T.-H.; Chang, J. Trends of Gold Nanoparticle-based Drug Delivery System in Cancer Therapy Trends of Gold Nanoparticle-based Drug Delivery System in Cancer Therapy. J. Exp. Clin. Med. 2014, 6, 172–178. [Google Scholar] [CrossRef]
- Cabral, R.M.; Baptista, P.V. Anti-cancer precision theranostics: A focus on multifunctional gold nanoparticles. Expert Rev. Mol. Diagn. 2014, 14, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Jiang, Z.; Saha, K.; Kim, C.S.; Kim, S.T.; Landis, R.F.; Rotello, V.M. Gold nanoparticles for nucleic acid delivery. Mol. Ther. 2014, 22, 1075–1083. [Google Scholar] [CrossRef] [PubMed]
- Keles, E.; Song, Y.; Du, D.; Dong, W.-J.; Lin, Y. Recent progress in nanomaterials for gene delivery applications. Biomater. Sci. 2016, 4, 1291–1309. [Google Scholar] [CrossRef] [PubMed]
- Draz, M.S.; Fang, B.A.; Zhang, P.; Hu, Z.; Gu, S.; Weng, K.C.; Gray, J.W.; Chen, F.F. Nanoparticle-mediated systemic delivery of siRNA for treatment of cancers and viral infections. Theranostics 2014, 4, 872–892. [Google Scholar] [CrossRef] [PubMed]
- Tabernero, J.; Shapiro, G.I.; Lorusso, P.M.; Cervantes, A.; Schwartz, G.K.; Weiss, G.J.; Paz-ares, L.; Cho, D.C.; Infante, J.R.; Alsina, M.; et al. First-in-Humans Trial of an RNA Interference Therapeutic Targeting VEGF and KSP in Cancer Patients with Liver Involvement. Cancer Discov. 2013, 3, 406–417. [Google Scholar] [CrossRef] [PubMed]
- Kanasty, R.; Dorkin, J.R.; Vegas, A.; Anderson, D. Delivery materials for siRNA therapeutics. Nat. Mater. 2013, 12, 967–977. [Google Scholar] [CrossRef] [PubMed]
- Williford, J.M.; Wu, J.; Ren, Y.; Archang, M.M.; Leong, K.W.; Mao, H.Q. Recent Advances in Nanoparticle-Mediated siRNA Delivery. Annu. Rev. Biomed. Eng. 2014, 16, 347–370. [Google Scholar] [CrossRef] [PubMed]
- Wan, C.; Allen, T.M.; Cullis, P.R. Lipid nanoparticle delivery systems for siRNA-based therapeutics. Drug Deliv. Transl. Res. 2014, 4, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Martins, P.; Rosa, D.; Fernandes, A.R.; Baptista, P.V. Nanoparticle Drug Delivery Systems: Recent Patents and Applications in Nanomedicine. Recent Pat. Nanomed. 2013, 3, 1–14. [Google Scholar] [CrossRef]
- Huang, X.; El-Sayed, M.A. Gold nanoparticles: Optical properties and implementations in cancer diagnosis and photothermal therapy. J. Adv. Res. 2010, 1, 13–28. [Google Scholar] [CrossRef]
- Sharma, H.; Mishra, P.K.; Talegaonkar, S.; Vaidya, B. Metal nanoparticles: A theranostic nanotool against cancer. Drug Discov. Today 2015, 20, 1143–1151. [Google Scholar] [CrossRef] [PubMed]
- Arvizo, R.; Bhattacharya, R.; Mukherjee, P. Gold nanoparticles: Opportunities and challenges in nanomedicine. Expert Opin. Drug Deliv. 2010, 7, 753–763. [Google Scholar] [CrossRef] [PubMed]
- Muddineti, O.S.; Ghosh, B.; Biswas, S. Current trends in using polymer coated gold nanoparticles for cancer therapy. Int. J. Pharm. 2015, 484, 252–267. [Google Scholar] [CrossRef] [PubMed]
- Cabral, R.M.; Baptista, P.V. The Chemistry and Biology of Gold Nanoparticle-Mediated Photothermal Therapy: Promises and Challenges. Nano Life 2013, 3, 1330001. [Google Scholar] [CrossRef]
- Abadeer, N.S.; Murphy, C.J. Recent Progress in Cancer Thermal Therapy using Gold Nanoparticles. J. Phys. Chem. C 2016, 120, 4691–4718. [Google Scholar] [CrossRef]
- Conde, J.; Ambrosone, A.; Hernandez, Y.; Tian, F.; McCully, M.; Berry, C.C.; Baptista, P.V.; Tortiglione, C.; De La Fuente, J.M. 15 years on siRNA delivery: Beyond the State-of-the-Art on inorganic nanoparticles for RNAi therapeutics. Nano Today 2015, 10, 421–450. [Google Scholar] [CrossRef]
- Zhu, D.; Song, P.; Shen, J.; Su, S.; Chao, J.; Aldalbahi, A.; Zhou, Z.; Song, S.; Fan, C.; Zuo, X.; et al. PolyA-Mediated DNA Assembly on Gold Nanoparticles for Thermodynamically Favorable and Rapid Hybridization Analysis. Anal. Chem. 2016, 88, 4949–4954. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.K.L.; Mohseni, R.; Hamidieh, A.A.; Maclaren, R.E.; Habib, N.; Seifalian, A.M. Will Nanotechnology Bring New Hope for Gene Delivery? Trends Biotechnol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Mieszawska, A.J.; Mulder, W.J.M.; Fayad, Z.A.; Cormode, D.P. Multifunctional Gold Nanoparticles for Diagnosis and Therapy of Disease. Mol. Pharm. 2013, 10, 831–847. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; O’Driscoll, C.M.; Holmes, J.D.; Rahme, K. Bioconjugated Gold Nanoparticles Enhance Cellular Uptake: A Proof of Concept Study for siRNA Delivery in Prostate Cancer Cells. Int. J. Pharm. 2016, 509, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Conde, J.; Ambrosone, A.; Sanz, V.; Hernandez, Y.; Marchesano, V.; Tian, F.; Child, H.; Berry, C.C.; Ibarra, M.R.; Baptista, P.V.; et al. Design of multifunctional gold nanoparticles for in vitro and in vivo gene silencing. ACS Nano 2012, 6, 8316–8324. [Google Scholar] [CrossRef] [PubMed]
- Shaat, H.; Mostafa, A.; Moustafa, M.; Gamal-Eldeen, A.; Emam, A.; El-Hussieny, E.; Elhefnawi, M. Modified gold nanoparticles for intracellular delivery of anti-liver cancer siRNA. Int. J. Pharm. 2016, 504, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Cordeiro, M.; Carvalho, L.; Silva, J.; Saúde, L.; Fernandes, A.R.; Baptista, P.V. Gold Nanobeacons for Tracking Gene Silencing in Zebrafish. Nanomaterials 2017, 7, 1–8. [Google Scholar] [CrossRef]
- Groenendijk, F.H.; Bernards, R. Drug resistance to targeted therapies: Déjà vu all over again. Mol. Oncol. 2014, 8, 1067–1083. [Google Scholar] [CrossRef] [PubMed]
- Komarova, N.L.; Roland, R. Calculated treatment. Nature 2013, 499, 291–292. [Google Scholar] [CrossRef] [PubMed]
- Lu, D.-Y.; Lu, T.-R.; Cao, S. Drug Combinations in Cancer Treatments. Clin. Exp. Pharmacol. 2013, 3, 134. [Google Scholar] [CrossRef]
- Patil, Y.; Swaminathan, S.; Sadhukha, T.; Ma, L.; Panyam, J. The use of Nanoparticle-mediated targeted gene silencing and drug delivery to overcome tumor drug resistance. Biomaterials 2010, 31, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Conde, J.; Artzi, N. Are RNAi and miRNA therapeutics truly dead? Trends Biotechnol. 2015, 33, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.K.W.; Chow, M.Y.T.; Zhang, Y.; Leung, S.W.S. siRNA Versus miRNA as Therapeutics for Gene Silencing. Mol. Ther. Nucleic Acids 2015, 4, e252. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhu, X.; Zhang, X.; Liu, B.; Huang, L. Nanoparticles Modified With Tumor-targeting scFv Deliver siRNA and miRNA for Cancer Therapy. Mol. Ther. J. Am. Soc. Gene Ther. 2010, 18, 1650–1656. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, M.; Jung, E.; Shah, M.Y.; Lu, C.; Shimizu, M.; Han, H.D.; Ivan, C.; Rossi, S.; Nicoloso, M.S.; Wu, S.Y.; et al. Therapeutic synergy between microRNA and siRNA in ovarian cancer treatment. Cancer Discov. 2013, 3, 1302–1315. [Google Scholar] [CrossRef] [PubMed]
- Werner, K.; Lademann, F.; Thepkaysone, M.; Jahnke, B.; Aust, D.E.; Kahlert, C.; Weber, G.; Weitz, J.; Pilarsky, C. Simultaneous gene silencing of KRAS and anti-apoptotic genes as a multitarget therapy. Oncotarget 2016, 7, 3984–3992. [Google Scholar] [PubMed]
- Tacar, O.; Sriamornsak, P.; Dass, C.R. Doxorubicin: An update on anticancer molecular action, toxicity and novel drug delivery systems. J. Pharm. Pharmacol. 2013, 65, 157–170. [Google Scholar] [CrossRef] [PubMed]
- Silva, J.; Fernandes, A.R.; Baptista, P.V. Application of Nanotechnology in Drug Delivery. In Application of Nanotechnology in Drug Delivery; Sezer, A., Ed.; InTech: Rijeka, Croatia, 2014; pp. 127–154. [Google Scholar]
- Gerber, D.E. Targeted therapies: A new generation of cancer treatments. Am. Fam. Physician 2008, 77, 311–319. [Google Scholar] [PubMed]
- Liu, F.-S. Mechanisms of Chemotherapeutic Drug Resistance in Cancer Therapy—A Quick Review. Taiwan. J. Obstet. Gynecol. 2009, 48, 239–244. [Google Scholar] [CrossRef]
- Conde, J.; de la Fuente, J.M.; Baptista, P.V. Nanomaterials for reversion of multidrug resistance in cancer: A new hope for an old idea? Front. Pharmacol. 2013, 4, 134. [Google Scholar] [CrossRef] [PubMed]
- Ganesh, S.; Iyer, A.K.; Weiler, J.; Morrissey, D.V.; Amiji, M.M. Combination of siRNA-directed Gene Silencing With Cisplatin Reverses Drug Resistance in Human Non-small Cell Lung Cancer. Mol. Ther. Nucleic Acids 2013, 2, e110. [Google Scholar] [CrossRef] [PubMed]
- Shen, H.; Mittal, V.; Ferrari, M.; Chang, J. Delivery of gene silencing agents for breast cancer therapy. Breast Cancer Res. 2013, 15, 205. [Google Scholar] [CrossRef] [PubMed]
- Creagh, E.; Sheehan, D.; Cotter, T. Heat shock proteins—Modulators of apoptosis in tumour cells. Leukemia 2000, 14, 1161–1173. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; El-Sayed, M.A. Plasmonic photo-thermal therapy (PPTT). Alexandria J. Med. 2011, 47, 1–9. [Google Scholar] [CrossRef]
- Chicheł, A.; Skowronek, J.; Kubaszewska, M.; Kanikowski, M. Hyperthermia—Description of a method and a review of clinical applications. Rep. Pract. Oncol. Radiother. 2007, 12, 267–275. [Google Scholar] [CrossRef]
- Tabuchi, Y.; Kondo, T. Targeting heat shock transcription factor 1 for novel hyperthermia therapy (Review). Int. J. Mol. Med. 2013, 32, 3–8. [Google Scholar] [CrossRef] [PubMed]
- De Billy, E.; Clarke, P.A.; Workman, P. HSF1 in translation. Cancer Cell 2013, 24, 147–149. [Google Scholar] [CrossRef] [PubMed]
- Scherz-Shouval, R.; Santagata, S.; Mendillo, M.L.; Sholl, L.M.; Ben-Ahron, I.; Beck, A.H.; Dias-Santagata, D.; Koeva, M.; Stemmer, S.M.; Whitesell, L.; et al. The reprogramming of tumor stroma by HSF1 is a potent enabler of malignancy. Cell 2014, 158, 564–578. [Google Scholar] [CrossRef] [PubMed]
- Hwang, G.; Ryoke, K.; Lee, J.; Takahashi, T. siRNA-mediated silencing of the gene for heat shock transcription factor 1 causes hypersensitivity to methylmercury in HEK293 cells. J. Toxicol. Sci. 2011, 36, 851–853. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Fujimoto, M.; Hayashida, N.; Takii, R. Silencing HSF1 by short hairpin RNA decreases cell proliferation and enhances sensitivity to hyperthermia in human melanoma cell lines. J. Dermatol. Sci. 2010, 60, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.; Ciafrè, S.; Balsamo, M.; Pierimarchi, P.; Santoro, M.G. Targeting the heat shock factor 1 by RNA interference: A potent tool to enhance hyperthermochemotherapy efficacy in cervical cancer. Cancer Res. 2006, 66, 7678–7685. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, J.; Jeong, C.; Kim, W.J. Synergistic nanomedicine by combined gene and photothermal therapy. Adv. Drug Deliv. Rev. 2016, 98, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Lin, Y.; Wang, C.; Tzeng, H.; Chen, Y.; Chen, C.; Chen, L.; Wu, Y.; Chen, C.; Lin, Y.; et al. Article DNA—Gold Nanorod Conjugates for Remote Control of Localized Gene Expression by near Infrared Irradiation. J. Am. Chem. Soc. 2006, 128, 3709–3715. [Google Scholar] [CrossRef] [PubMed]
- Vijayaraghavan, P.; Vankayala, R.; Chiang, C.; Sung, H. Biomaterials Complete destruction of deep-tissue buried tumors via combination of gene silencing and gold nanoechinus-mediated photodynamic therapy. Biomaterials 2015, 62, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Teh, B.S. Combining Radiotherapy with Gene Therapy (From the Bench to the Bedside): A Novel Treatment Strategy for Prostate Cancer. Oncologist 2002, 7, 458–466. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Jiang, T.; Wen, Z.; Gao, R.; Cui, M.; Wang, F. Silencing of Heat Shock Protein 70 Expression Enhances Radiotherapy Efficacy and Inhibits Cell Invasion in Endometrial Cancer Cell Line. Croat. Med. J. 2009, 50, 143–450. [Google Scholar] [CrossRef] [PubMed]
- Ghafouri-Fard, S.; Ghafouri-Fard, S. siRNA and cancer immunotherapy. Immunotherapy 2012, 4, 907–917. [Google Scholar] [CrossRef] [PubMed]
- Conde, J.; Arnold, C.E.; Tian, F.; Artzi, N. RNAi nanomaterials targeting immune cells as an anti-tumor therapy: The missing link in cancer treatment? Mater. Today 2016, 19, 29–43. [Google Scholar] [CrossRef]
- Mao, C.-P.; Wu, T.-C. Inhibitory RNA Molecules in Immunotherapy for Cancer. Methods Mol. Biol. 2010, 623, 325–339. [Google Scholar] [PubMed]
- Sioud, M. Engineering better immunotherapies via RNA interference. Hum. Vaccines Immunother. 2014, 10, 3165–3174. [Google Scholar] [CrossRef] [PubMed]
- Pillai, G. Nanomedicines for Cancer Therapy: An Update of FDA Approved and Those under Various Stages of Development. SOJ Pharm. Pharm. Sci. 2014, 1, 13. [Google Scholar]
- Yoo, B.; Medarova, Z. Nanoformulations for Pharmacological siRNA Delivery in Cancer. In Design and Applications of Nanoparticles in Biomedical Imaging; Bulte, J.W.M., Modo, M.M.J., Eds.; Springer: Cham, Switzerland, 2017; pp. 171–186. [Google Scholar]
- Anselmo, A.C.; Mitragotri, S. Nanoparticles in the Clinic. Bioeng. Transl. Med. 2016, 55, 10–29. [Google Scholar] [CrossRef]
- Zuckerman, J.E.; Davis, M.E. Clinical experiences with systemically administered siRNA-based therapeutics in cancer. Nat. Rev. Drug Discov. 2015, 14, 843–856. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.K.; Han, M.S.; Asokan, S.; Tung, C.-H. Effective Gene Silencing by Multilayered siRNA-Coated Gold Nanoparticles. Small 2011, 7, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Sanna, V.; Sechi, M. Targeted therapy using nanotechnology: Focus on cancer. Int. J. Nanomed. 2014, 9, 467–483. [Google Scholar]
- Wang, K.; Kievit, F.M.; Zhang, M. Nanoparticles for cancer gene therapy: Recent advances, challenges, and strategies. Pharmacol. Res. 2016, 114, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Conde, J.; Doria, G.; Baptista, P. Noble Metal Nanoparticles Applications in Cancer. J. Drug Deliv. 2012, 2012, 751075. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M.; Foote, M.; Prow, T.W. Therapeutic gold, silver, and platinum nanoparticles. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2015, 7, 428–445. [Google Scholar] [CrossRef] [PubMed]
- Dreaden, E.C.; Austin, L.A.; Mackey, M.A.; El-Sayed, M.A. Size matters: Gold nanoparticles in targeted cancer drug delivery. Ther. Deliv. 2012, 3, 457–478. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Gene | RNAi Technology | Effect on Tumor Cells | Reference |
|---|---|---|---|
| B-cell lymphoma/leukemia 2 protein (BCL-2) (oncogene) | siRNA | Induced apoptosis in vitro | [1] |
| BCL-2 (oncogene) | shRNA | Suppressed tumor growth in mice with xenograft tumor | [1] |
| Clusterin (CLU) (heterodimeric glycoprotein) | siRNA | Decrease in cancer cell proliferation and an increase in apoptosis rate in vitro | [1] |
| CLU (heterodimeric glycoprotein) | siRNA | CLU siRNA treated MDA-MB-231 cells grew significantly slower in vivo | [1] |
| N-acetylglucosaminyltransferase V (GNT-V) (overexpression in malignant tumors) | siRNA | Decreased proliferation of BGC823 cells | [1] |
| Peptidyl-prolyl cis/trans isomerase (PIN1) (overexpression in prostate and breast cancers) | shRNA | Inhibited tumor growth, metastasis and angiogenesis | [1] |
| Vascular Endothelial Growth Factor (VEGF) | shRNA | Inhibited cancer cell proliferation and tumor growth, and reduced tumor microvessel density (MVD) and microlymphatic vessel density (MLVD) | [1] |
| Eukaryotic Initiation Factor 3 c (eIF3c) (oncogene) | siRNA | The survival rate of RKO colon cancer cells drastically, the cell cycle was arrested as the number of cells entering the S phase was significantly reduced, and the induction of apoptosis was prominent | [12] |
| M-BCR/ABL fusion (constitutively activated) | siRNA | Killed leukemic cells with this arrangement | [5] |
| K-RASv12 allele (oncogene) | siRNA | Specifically and stably inhibited the expression of the oncogenic K-RASv12 allele while leaving the wild type K-RAS intact in human tumor cells | [5,13] |
| Name (Company) | Particle Type/Drug | Application/Indication | Clinical Trials. Gov (Phase) |
|---|---|---|---|
| TKM-080301 (Arbutus Biopharma) | Lipid particle targeting Polo-Like Kinase 1 (PLK1) for delivery of siRNA | Hepatocellular carcinoma | NCT02191878 (Ph I/II) |
| siRNA-EphA2-DOPC (M.D. Anderson Cancer Center) | siRNA liposome for EPHA2 knockdown | Solid tumors | NCT01591356 (Ph I) |
| PNT2258 (ProNAi Therapeutics) | Proprietary single-stranded DNAi (PNT100) encapsulated in lipid nanoparticles | Lymphomas | NCT02378038 (Ph II) NCT02226965 (Ph II) NCT01733238 (Ph II) |
| BP1001 (Bio-Path Holdings) oligonucleotide | Growth Factor Receptor Bound Protein-2 (GRB-2) antisense encapsulated in neutral liposomes | Leukemia | NCT01159028 (Ph I) |
| DCR-MYC (Dicerna Pharmaceuticals) | DsiRNA lipid nanoparticle for MYC oncogene silencing | Solid tumors, multiple myeloma, lymphoma, or hepatocellular carcinoma | NCT02110563 (Ph I) NCT02314052 (Ph I/II) |
| Atu027 (Silence Therapeutics GmbH) | AtuRNAi® liposomal formulation for Protein Kinase N3 (PKN3) knockdown in vascular endothelium | Pancreatic cancer | NCT01808638 (Ph I/II) |
| SGT-53 (SynerGene Therapeutics) | Cationic liposome with anti-transferrin receptor antibody, encapsulating Wildtype p53 sequence | Glioblastoma, solid tumors, or pancreatic cancer | NCT02354547 (Ph I) NCT00470613 (Ph I) NCT02354547 (Ph I) NCT02340156 (Ph II) |
| SGT-94 (SynerGene Therapeutics) | RB94 plasmid DNA in a liposome with anti-transferrin receptor antibody | Solid tumors | NCT01517464 (Ph I) |
| MRX34 (Mirna Therapeutics) | Double-stranded RNA mimic of miR-34 encapsulated in liposomes | Liver cancer | NCT01829971 (Ph I) |
| TargomiRs (EnGeneIC) | Anti-EGFR bispecific antibody minicells (bacteria derived nanoparticles) with a miR-16 based microRNA payload | Mesothelioma and Non-small cell lung cancer | NCT02369198 (Ph I) |
| CALAA-01 (Calando Pharmaceuticals) | Polymer (targeted)/siRNA targeting Ribonucleotide Reductase Regulatory Subunit M2 (RRM2) | Melanoma | NCT00689065 (Ph I) |
| ALN-VSP (Alnylam Pharmaceuticals) | Lipid (non-targeted)/siRNA targeting VEGFA and KSP | Solid Tumors | NCT00882180 (Ph I) NCT01158079 (Ph I) |
| Atu027 PKN3 (Silence Therapeutics) | Lipid (non-targeted)/siRNA targeting PKN3 | Advanced solid tumors and metastatic pancreatic adenocarcinoma | NCT00938574 (Ph I) NCT01808638 (Ph I/II) |
| TKM-PLK1 (Tekmira Pharmaceuticals) | Lipid (non-targeted)/siRNA targeting PLK1 | solid tumors, hepatocellular carcinoma, gastrointestinal neuroendocrine tumors and adrenocortical carcinoma | NCT01262235 (Ph I/II) NCT01437007 (Ph I) NCT02191878 (Ph I/II) |
| siG12D LODER (Silenseed) | Biodegradable polymer matrix/siRNA targeting K-RAS | Pancreatic Ductal Adenocarcinoma and Pancreatic cancer | NCT01188785 Ph I) NCT01676259 (Ph II) |
| SNS01-T (Senesco Technologies) | Polyethylenimine (non-targeted)/eIF5AK50R plasmid eIF5A siRNA | NR | NCT01435720 (Ph II) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendes, R.; Fernandes, A.R.; Baptista, P.V. Gold Nanoparticle Approach to the Selective Delivery of Gene Silencing in Cancer—The Case for Combined Delivery? Genes 2017, 8, 94. https://doi.org/10.3390/genes8030094
Mendes R, Fernandes AR, Baptista PV. Gold Nanoparticle Approach to the Selective Delivery of Gene Silencing in Cancer—The Case for Combined Delivery? Genes. 2017; 8(3):94. https://doi.org/10.3390/genes8030094
Chicago/Turabian StyleMendes, Rita, Alexandra R. Fernandes, and Pedro V. Baptista. 2017. "Gold Nanoparticle Approach to the Selective Delivery of Gene Silencing in Cancer—The Case for Combined Delivery?" Genes 8, no. 3: 94. https://doi.org/10.3390/genes8030094
APA StyleMendes, R., Fernandes, A. R., & Baptista, P. V. (2017). Gold Nanoparticle Approach to the Selective Delivery of Gene Silencing in Cancer—The Case for Combined Delivery? Genes, 8(3), 94. https://doi.org/10.3390/genes8030094